
Abstract
This study was to examine the effects of support interventions on anxiety, depression, and quality of life in women hospitalized with preterm labor. A randomized, single-blind experimental design was used. Participants were recruited from maternity wards of one medical center in Taiwan. The control group (n = 103) received routine nursing care, and intervention group (n = 140) received interventional support during hospitalization. The Beck Anxiety Inventory, Edinburgh Postnatal Depression Scale, and Quality of Life Enjoyment and Satisfaction Questionnaire were used at admission and 2 weeks of hospitalization. For the control group, anxiety and depression scores increased significantly and quality of life decreased 2 weeks after hospitalization. Participants who received 2 weeks of support intervention had significantly lower anxiety and depression scores than controls. Thus, clinical nurses can offer support interventions to improve anxiety and depression for women with preterm labor during hospitalization.
Introduction
Preterm labor (PTL), which occurs in approximately 5% to 10% of all births, is the most important factor in neonatal morbidity and mortality (Challis, 2000; Goldenberg, Culhane, Iams, & Romero, 2008; Lumley, 2003). Approximately 40% to 45% of preterm deliveries are caused by spontaneous PTL, 25% to 30% are due to preterm premature rupture of membranes (PPROM), and 30% to 35% are medically indicated preterm births resulting from preeclampsia, intrauterine growth restriction, fetal distress, or placental abruption, and so on (Ananth & Vintzileos, 2006; MacDorman, 2011). Obstetric therapeutic strategies for treating PTL include hospitalization, bed rest, hydration, sedation, uterine activity monitoring, and tocolytic agents (Goldenberg, 2002).
For more than 30 years, the foundation for treating PTL has relied almost exclusively on antepartum bed rest (ABR) and activity restriction (AR), which requires confinement to bed and limits activities to toileting needs (Maloni, 2010). Bed rest is designed to prevent preterm birth and reduce stress levels for women in PTL; however, there are no data supporting an improvement in outcomes, and these restrictions often result in higher stress levels than seen in typical pregnant women (Alder, Fink, Bitzer, Hösli, & Holzgreve, 2007; MacKinnon, 2006). Rather than benefit the mother or baby, ABR/AR is perceived as a negative experience for the mother, and it can have an adverse impact on the fetus (Lederman et al., 2013; Maloni, BrezinskiTomasi, & Johnson, 2001). The physiological and psychosocial changes of ABR and AR can be accompanied by maternal feelings of fear, lack of control, powerlessness, and anxiety (Lederman et al., 2013; May, 2001).
Symptoms of depression and anxiety are high during ABR and AR (Maloni, Park, Anthony, & Musil, 2005), and a positive association between PTL and maternal anxiety and depression has been demonstrated (Dayan et al., 2002; Martini, Knappe, Beesdo-Baum, Lieb, & Wittchen, 2010). Hospitalization can also introduce additional sources of stress by removing women from the comfort and security of their home environment (Heaman & Gupton, 1998), which can add an additional component to anxiety and depression. The coincidence of anxiety and depression during pregnancy is associated with a higher risk of preterm birth (Grote et al., 2010; Li, Liu, & Odouli, 2009).
Maternal quality of life (QoL) during the prenatal period may also be affected by the occurrence of preterm birth. Women in pregnancy who experience depressive symptoms and anxiety have poor QoL (Nicholson et al., 2006; Setse et al., 2009). Women in PTL have significantly higher depression scores and lower QoL scores than those without complications (Mautner et al., 2009). Primary sources of maternal stress during hospitalization to prevent PTL include anxiety about the baby’s outcome, separation from and concern for the family at home, negative emotions, self-image, and personal health status (Giurgesco, Penckofer, Maurer, & Bryant, 2006; MacDonald & Jonas-Simpson, 2009; Maloni, Margevicius, & Damato, 2006). Psychological support for women with PTL may alleviate or reduce their feelings of stress. Mind–body interventions, which constitute a major portion of the overall use of complementary and alternative medicine (CAM), can also provide support. These techniques are designed to enhance the mind’s capacity to affect bodily function and symptoms (National Center for Complementary and Integrative Health [NCCIH], 2015).
Mind–body interventions cover a broad range of techniques and practices, such as autogenic training, hypnotherapy, imagery, prayer, auto-suggestion, tai-chi, and yoga (Marc et al., 2011). These complementary therapies can have physiological as well as psychological benefits, which may consequently reduce the physio-pathological impact of stress (Beddoe & Lee, 2008; Tiran & Chummun, 2004). Mind–body interventions can facilitate a state of relaxation to treat stress and anxiety-related psychological and physical disorders (Astin, Shapiro, Eisenberg, & Forys, 2003) and have the potential to improve psycho-physiological states during pregnancy (Beddoe & Lee, 2008). For example, Saisto, Toivanen, Salmela-Aro, and Halmesmaki (2006) found that support interventions for pregnant women, which included discussions of concerns and feelings about birth, taught positive birth imagery and relaxation exercises were beneficial at reducing fears surrounding childbirth. Unstructured support groups have been used as important antepartum nursing interventions for women on hospital bed rest; sharing feelings with others in similar situations may provide women with PTL the ability to cope with the stress of bed rest (Maloni & Kutil, 2000). Additional efforts to minimize the adverse effects of long-term bed rest and prolonged hospitalization include provision of privacy in a family unit and more organized activities to relieve boredom (Richter, Parkes, & Chaw-Kant, 2007) by recreation activities such as scrapbooking, blanket making, and knitting supplies during hospitalization (Thorman & McLean, 2006).
Few studies evaluated the efficacy of support interventions for women in PTL who have been treated with tocolytic therapy during hospitalization. Hospitalization of women in PTL treated with tocolytic medications may result in additional stress due to the separation from home and family, lack of privacy, hospital discomfort environment, restricted activities, and the anxiety about preterm birth and the baby’s outcome (Heaman & Gupton, 1998). We developed a support intervention and applied it to this population of women. We then tested the hypothesis that a support intervention would reduce anxiety and depression, and promote QoL during hospitalization. Thus, the purpose of this study was to examine the effects of support interventions on anxiety, depression, and QoL in women with PTL at admission and at admission 2 weeks.
Method
Study Design and Samples
We used a pretest/posttest design to examine the effects of support interventions. For this study, we recruited Taiwanese women admitted to the maternity wards of obstetrics and gynecology at a medical center in northern Taiwan. The inclusion criteria were as follows: (a) a diagnosis of PTL; (b) pregnancy stage between 20 and 36 weeks of gestation; (c) receiving tocolytic therapy, such as ritodrine, magnesium sulfate (MgSO4), or Nifedipine; (d) no significant medical history of thyroid, adrenal, cardiac, or chronic renal disease or other medical complications; (e) no mental health concerns; and (f) the ability to read, write, and understand Chinese. Exclusion criteria were infection, hypertension, preeclampsia, gestational diabetes mellitus, immunological disease, fetal distress, or placental abruption. Women who cannot complete the pre- or posttest, or who were discharged within 2 weeks or who cannot read and communicate in Chinese were also excluded. Specific hospital bed number was designed as intervention or control group before the study. The participants were randomly admitted to the ward assigned to either group according to the bed number during hospital stay. The allocation of the bed number was independently conducted by the admission office which was blind to the study, and the medical staff could not purposely assign women to specific bed number.
G*Power 3.1.5 (Faul, Erdfelder, Lang, & Buchner, 2007) was used for our power analysis to determine sample size for the analysis of anxiety, depression, and QoL scores in this study. Based on the study design, we applied a t test to estimate the appropriate number of participants. The alpha was set to .05, power .80, and effect size as .5. The estimated sample size was 64 participants for each group.
Measures
Baseline characteristics
Demographics (e.g., age, marital status, work status, educational level, socioeconomic status) and obstetric characteristics on admission (gestational weeks, multiple gestation, abortion history, preterm uterine contraction, vaginal bleeding, PPROM, placenta previa, and admission diagnosis) as well as number of weeks of gestation at hospital discharge were collected from the patient’s medical record.
Beck Anxiety Inventory (BAI)
The BAI is a 21-item self-report inventory that measures severity of anxiety, which rates symptoms and attitudes toward anxiety for the previous week (Beck, Epstein, Brown, & Steer, 1988). The severity of each individual item is scored from 0 to 3 (0 = no anxiety, 3 = severe anxiety). Total scores range from 0 to 63 with higher scores indicating more severe anxiety. The BAI has been shown to be a valid measure of anxiety for perinatal depression (American College of Obstetricians and Gynecologists, 2015). We used the Chinese version of the BAI (Che, Lu, Chen, Chang, & Lee, 2006), which showed high internal consistency (Cronbach’s α = .95, Guttman split-half coefficient = 0.91) and good convergent validity (Pearson’s correlation = .72). The optimal cutoff point for discriminating between anxious and nonanxious individuals was 13/14 (Che et al., 2006).
Edinburgh Postnatal Depression Scale (EPDS)
The EPDS is a 10-item self-report scale, which is designed to screen women for symptoms of emotional distress in the past 7 days during pregnancy and the postnatal period. The 4-point scale generates scores ranging from 0 to 30. The EPDS has been translated into Chinese-EPDS for use in Hong Kong (Lee et al., 1998) and Taiwan (Heh, 2001; Huang & Mathers, 2001; Teng et al., 2005). The Chinese-EPDS and Taiwanese version of the EPDS recommended the cutoff point is 9/10 to indicate depressive symptoms for women (Heh, 2001; Lee et al., 1998). Higher scores indicate greater depression. We used the Taiwanese version of the EPDS (Heh, 2001; Huang & Mathers, 2001) to assess participants’ depressive symptoms during hospitalization.
The QoL Enjoyment and Satisfaction Questionnaire–Short Form (Q-LES-Q-SF)
The Q-LES-Q-SF is a self-rated scale designed to measure the degree of enjoyment and satisfaction experienced by persons in various activities of daily functioning (Endicott, Nee, Harrison, & Blumenthal, 1993). The Q-LES-Q-SF is comprised of 15 general activity items and one overall life satisfaction item. A summary score is calculated for the general activity items and for the overall life satisfaction item. Using a 5-point scale, scores for state of satisfaction range from 16 to 80. Higher scores indicate greater enjoyment or satisfaction. We used the Chinese version of the Q-LES-Q-SF (Lee et al., 2014) to measure participants’ QoL. The Chinese Q-LES-Q-SF was shown to have high 2-week test–retest reliability, adequate construct validity, and concurrent validity; internal consistency Cronbach’s alpha was .87; and the intraclass correlation coefficient (ICC) was .75.
Birth outcomes
Birth outcome data were collected from the participant’s obstetric record, which included number of weeks of gestation at delivery, birth weight, and Apgar scores at 1 min and 5 min.
Treatment for the Control and Intervention Group
The participants in the control group received an educational program and instruction on the prevention of preterm birth, which was part of the routine nursing care provided to women in PTL on the maternity wards of the medical center. The duration of the education program ranged from 5 to 10 min. Prevention of preterm birth was provided as a booklet, which included information and descriptions of various behaviors related to preterm birth.
First, the intervention group participants received individual instruction in relaxation techniques and support in addition to the above general educational instructions. Next, the intervention was divided into two sessions. The first part consisted of at least one interview/instructional session, which was conducted by a nurse educator within the first week after admission. The nurse educator has a bachelor’s degree of science in nursing and 3-year working experience in obstetric nursing. She received 2 weeks of interview and counseling training before starting the project. She discussed the work with the principal investigators at least once a week. During the interview, the nurse educator listened to participants’ talk about any emotional stress or complaints regarding their PTL and hospitalization. The nurse educator instructed the participants in techniques involving psycho-physiological relaxation (such as decentralized attention of participants and expressing their feelings), to help them reduce feelings of anxiety and depression. This form of complementary therapy as a support intervention has been demonstrated to have physiological as well as the psychological benefits (Beddoe & Lee, 2008). In addition, the nurse educator discussed forms of distraction methods for the participants, which involved focusing on and expressing feelings toward their unborn infant. These distractions can also result in relaxation. The intervention session takes 30 to 40 min for each participant. Then, the nurse educator visited the participant 3 to 5 times during hospitalization. The nurse educator used the techniques of distractions that included encouraging participants to prepare clothing for the unborn baby, teaching them to knit, recording fetal growth, or keeping a diary for talk with unborn baby. The second part of the intervention involved personal assistance from a hospital volunteer with high school or college education level 1 to 3 times a week depending on the needs of participants, which included communication; psychological support; shopping; massage, which can foster relaxation; and help with daily activities such as toiletry, bathing, and shampooing during hospitalization.
Ethical Considerations
This study was performed in accordance with the ethical standards and principles outlined in the Declaration of Helsinki and its amendments (World Medical Association, 2013). Prior to beginning this study and recruiting participants, ethics approval was obtained from the institutional review board of the study hospital. A research assistant made initial contact with the patients and explained the purpose and procedures of the study; the voluntary nature of participation; the right to withdraw at any time, for any reason, without any consequences regarding care; and that their data would be kept confidential. Informed consent was obtained from all study participants.
Data Collection
Data were collected from January 2013 to April 2015. After obtaining written informed consent, the research assistant gave participants the questionnaires. Participant’s demographic and obstetric data were then collected. Admission data were collected before instructions or interventions were initiated. Participants completed the BAI, EPDS, and Q-LES-Q-SF while in the hospital ward. Two weeks after admission, participants completed the BAI, EPDS, and Q-LES-Q-SF again. Discharge and birth outcome data were collected after delivery.
Data Analyses
Data were analyzed using the Statistical Package for the Social Sciences Version 20.0 (SPSS Inc., Chicago, IL). Participants’ characteristics were analyzed by frequency, means, and standard deviation; t test and chi-square tests were used to evaluate differences in participants’ characteristics, anxiety, depression, QoL scores, gestation at delivery, birth weight, and Apgar scores at 1 min and 5 min; repeated-measures ANOVA and t test were used to evaluate the anxiety, depression, and QoL scores at admission and at 2 weeks following admission. A p value <.05 was considered significant.
Results
Characteristics of the Study Participants
The demographics and hospital records were obtained after participant gave informed consent, and this study was approved by the institutional review board of the hospital. Excluding 10 participants in the control group who did not complete posttest measurement of the study, a total of 243 participants were recruited in this study. There were 103 women in the control group and 140 women in the intervention group. The mean ages of participants were 33.10 (SD = 4.21) and 32.83 (SD = 4.07) years in the control and intervention groups, respectively. There was no significant difference in the mean weeks of gestational age at admission: 27.06 (SD = 4.61) for the control group and 26.86 (SD = 4.8) for intervention group. There were no significant differences in any variables of demographics or obstetric characteristics between the two groups (Table 1). Most of participants received ritodrine for tocolytic therapy during hospitalization in the two groups (93.2% vs. 92.9%, p > .05). There was no significant difference in the mean weeks of gestation for the two groups at discharge (control = 31.12 [SD = 4.56]; intervention = 31.88 [SD = 4.03]; p > .05).
Demographic and Obstetric Characteristics at Admission of the Two Study Groups.
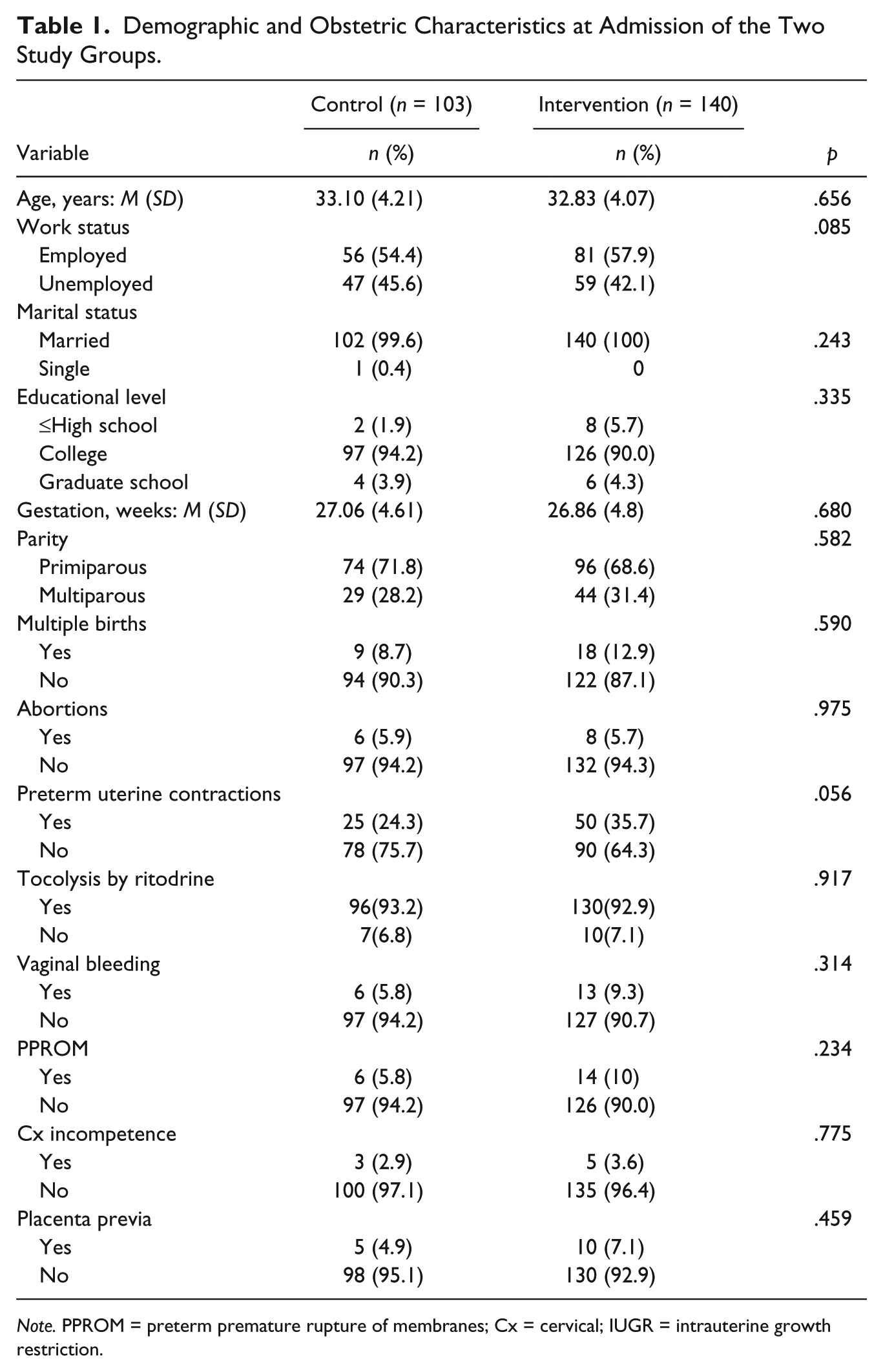
Note. PPROM = preterm premature rupture of membranes; Cx = cervical; IUGR = intrauterine growth restriction.
Effects of the Support Intervention on Anxiety, Depression, and QoL Scores for Study Groups After 2 Weeks
Scores for anxiety, depression, and QoL were measured with the BAI, EPDS, and Q-LES-Q-SF instruments, respectively, on admission and after 2 weeks of hospitalization for each group of participants (Table 2). In scores for anxiety and depression, neither control or intervention group exceeded the cutoff for depression before or after the intervention (Heh, 2001; Lee et al., 1998). The repeated-measures ANOVA demonstrated significant differences between control and intervention groups in scores for anxiety (p < .01), depression (p < .01), and QoL (p < .05) at post-admission (2 weeks; Table 2). After 2 weeks of hospitalization, the effect size for anxiety was 0.19, depression scores was 0.20, and QoL was 0.15 for the intervention. The effect size around 0.2 indicates the small magnitude (Page, 2014). However, it further demonstrates the statistically significant differences and provides information on the interventions that are potentially beneficial in clinical practice. Participants in the control group had significantly higher anxiety and depression scores after 2 weeks of hospitalization compared with scores at admission (p < .01; Table 2).
Comparison of Scores for Anxiety, Depression, and Quality of Life at Admission and Post-Admission (2 Weeks) for Study Groups.
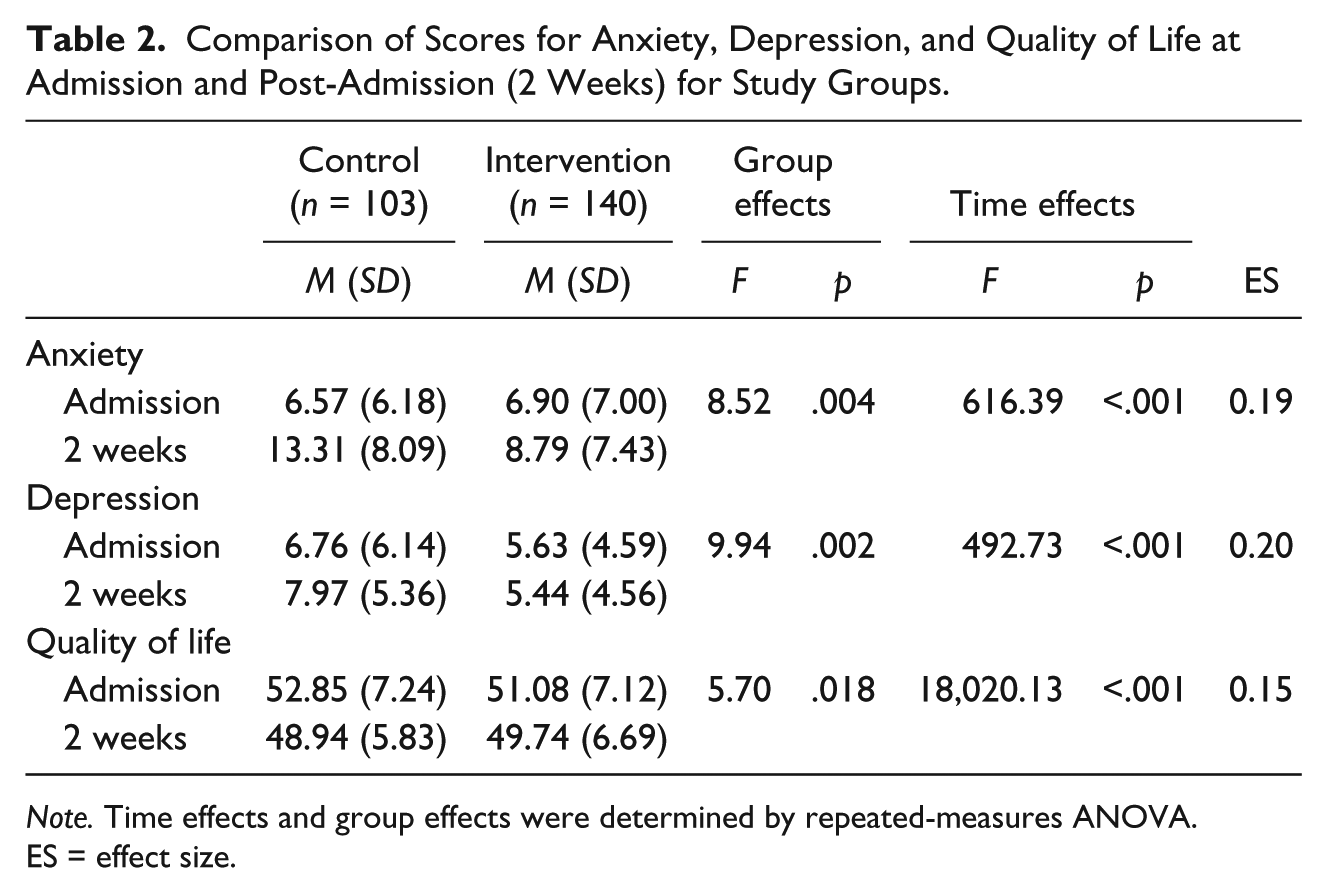
Note. Time effects and group effects were determined by repeated-measures ANOVA. ES = effect size.
Differences in Anxiety, Depression, and QoL Scores at Admission and 2 Weeks Post-Admission Between Study Groups
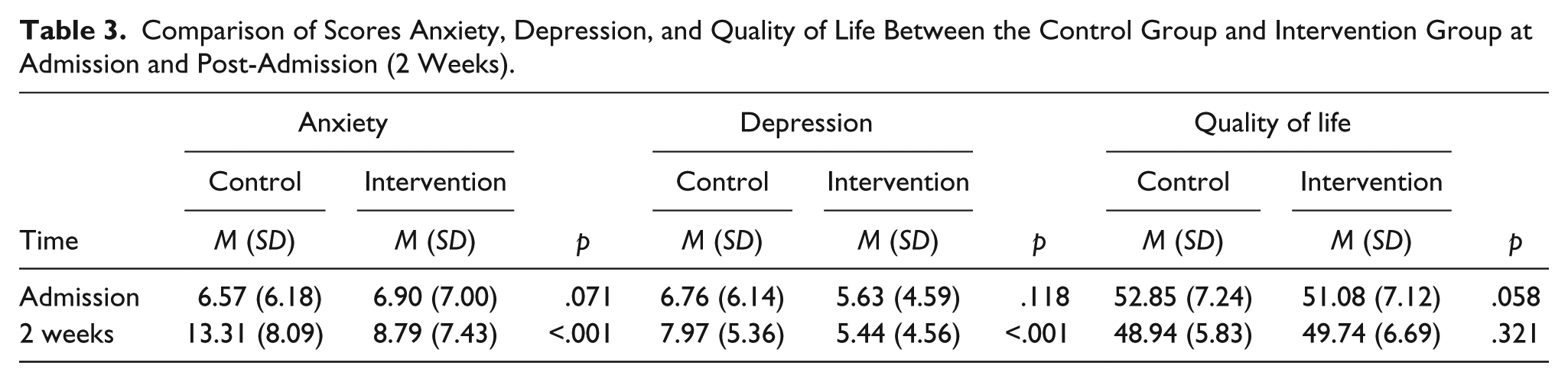
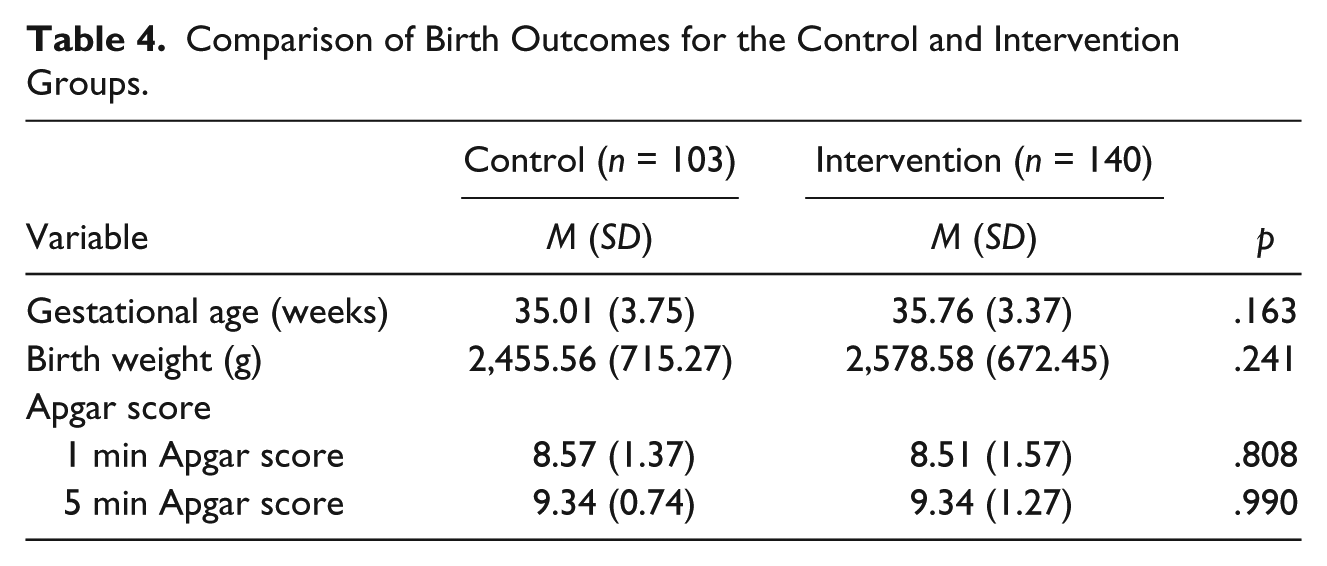
Scores for anxiety, depression, and QoL were compared between the control and intervention group at admission and 2 weeks after admission (Table 3). There was no significant difference in the three scores at admission between participants in the control or intervention group. Two weeks after admission, scores for both anxiety and depression were significantly lower for participants in the intervention group than the control group (p < .001 for both). There was no significant difference in scores for QoL between the two groups (p > .05). The birth outcomes were not different between control and intervention group (Table 4).
Comparison of Scores Anxiety, Depression, and Quality of Life Between the Control Group and Intervention Group at Admission and Post-Admission (2 Weeks).
Comparison of Birth Outcomes for the Control and Intervention Groups.
Discussion
Previous reports have revealed the relationship between PTL and anxiety and depression (Heaman & Gupton, 1998; Maloni, 2010). In the present study, we examined women with PTL who were hospitalized and treated concomitantly with tocolytic therapy. The control and intervention groups of participants admitted to the hospital with PTL were not significantly different in demographics, obstetric characteristics, or scores for anxiety and depression. Two weeks of hospitalization resulted in increased scores for anxiety in both groups. However, in contrast to the control group, the intervention group did not exhibit an increase in depression scores. When the participants in the intervention group were compared with the control group, scores for both anxiety and depression were statistically significantly lower for the intervention group. There was no statistical difference in QoL between the two groups.
Treatment for PTL includes ABR and AR. This restricted our participants from conducting daily chores and activities, which can increase anxiety and depression for prenatal women hospitalized for PTL (Maloni, 2010). Tocolytic therapy added an additional need for ABR and AR. Although we did not evaluate the physiological effects of tocolytic therapy on the participants, this is the first study to specifically address the issue of reduction of anxiety and depression for women hospitalized for PTL and treated with tocolytic therapy. In addition, high proportion of women using the same drug for tocolysis in both groups should avoid the confounding effect of the drug in anxiety, depression, and QoL measurements.
After 2 weeks of hospital stay, the anxiety and depression scores in the control group were significantly higher than those who received interventional treatment with relaxation and distraction techniques. This suggests that providing relaxation instruction, distractions, and assistance with personal activities can improve the overall emotional experience of women confined to bed rest for PTL. Holistic care provided by the nurse educator focused on facilitating the participants’ psychosocial well-being and helped them cope with the impact of physiological stress. Listening to the participants talk about their emotional stress or complaints during the interview may have provided emotional support; providing women on hospital bed rest an opportunity to talk in a confidential and supportive environment has been shown to help reduce anxiety and depression (Maloni & Kutil, 2000). The support intervention encouraged participants to discuss feelings about their pregnancy and hospitalization, which gave them an opportunity to discuss negative emotions. Instruction in applying relaxation techniques can improve the state of a person’s psycho-physiological well-being. This may have allowed participants to process emotions and decrease the anxiety and depression surrounding their PTL. Support interventions that include CAM can have physiological as well as psychological effects (Beddoe & Lee, 2008).
The distractions incorporated into the support intervention allowed participants to engage in activities involving care of their unborn infant and focused attention on the positive aspects of their pregnancy, rather than the restrictions in activities resulting from ABR. Some of the distractions were centered on activities surrounding their unborn infant. These distraction methods can also result in a physiological state of relaxation and reduced anxiety and depression. Preparing clothing for a newborn, recording fetal growth, and maintaining a diary about their feelings were distractions that assisted participants in recognizing they had a responsibility to their unborn child and were capable of performing well in the role of motherhood. In a qualitative study by Lederman et al. (2013), women hospitalized for PTL reported support and guidance from health care staff helped them to feel more secure in their ability to continue with their high-risk pregnancy, which may be one of the few positive components of hospitalization for PTL.
Although the support intervention reduced anxiety and depression, there were no significant differences in variables of birth outcomes in the two study groups. This is similar to results of Bastani, Hidarnia, Kazemnejad, Vafaei, and Kashanian (2005), who found that relaxation training reduced anxiety and perceived stress in pregnant women, but did not affect the rate of preterm birth (Bastani, Hidarnia, Montgomery, Aguilar-Vafaei, & Kazemnejad, 2006). Khianman, Pattanittum, Thinkhamrop, and Lumbiganon (2012) found similar results. They reviewed birth outcomes from studies investigating benefits of relaxation on maternal stress reduction for women in PTL; although relaxation reduced anxiety, there was no difference in birth outcomes between controls and those receiving relaxation therapy. However, the variation in the etiologies of the patients with PTL recruited in the present study may affect the birth outcome, which mitigated the effect of psychological support intervention. Study in a more homogeneous group (such as preterm uterine contraction) may help to elucidate the effect of psychological support intervention on birth outcome.
Conclusion
Our results indicate that providing support therapy, which includes mind–body interventions such as relaxation exercises, distraction techniques, and providing assistance with activities of daily living decreases anxiety and depression in women hospitalized for PTL. Clinical nurses and other maternity health care professionals can easily adapt these interventions for use in a hospital environment.
Limitations
There are some limitations to our study. The participants were recruited from only one hospital in northern Taiwan. Future studies should include other regions of Taiwan to enrich the data and identify regional differences. The intervention of this study consists of many elements. It is unclear which elements accounted for the significant changes realized by the intervention group. The effective ingredients of the intervention and the satisfaction of participants need further investigation in future. In the present study, we provided holistic care including relaxation instruction, distractions, and assistance with personal activities to improve overall emotional experience of the patients. Individualization of the management for the need of the participants after the first interview and provide individual support intervention focusing on special activities, such as distraction method focusing on unborn baby, or develop other stress management activities may have greater impact in reducing anxiety and depression. Furthermore, the difference between intervention and control may have been larger if only depressed or anxious women were included in the program in future.
Application to Clinical Practice
Our results showed that the support intervention reduced anxiety and depression for women hospitalized with PTL. There was no significant difference in QoL between participants of the two groups. This may be due to the fact that both groups were still hospitalized rather than in a home environment. The hospital is a stress-filled environment and women often have concerns regarding being away from home (Heaman & Gupton, 1998). This intervention study might be presented as a preventive program in clinical practice. All women with or without depression or anxiety were eligible to participate in future clinical work.
Footnotes
Acknowledgements
The authors would like to express sincere appreciation to the patients who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from Premature Baby Foundation of Taiwan.