
Abstract
This systematic review was to identify and synthesize literature that described the cultural appropriateness and effectiveness of interventions aimed at cardiovascular risk reduction in Korean Americans. We searched multiple electronic databases for studies published between January 2000 and August 2017 and identified 14 eligible research reports. All reviewed studies targeted first-generation Korean American adults. Most of the reviewed studies incorporated components of surface structure, and leveraged deep structure in those interventions. Significant changes in cardiovascular health outcomes were reported in most of the reviewed studies; however, the role of cultural factors in the outcomes was rarely evaluated, and few reported long-term effects. Future research needs to consider long-term effects. Deploying cultural factors and evaluating their contributions to the target outcomes will enhance the research on cardiovascular health disparities.
Introduction
Cardiovascular disease (CVD) is the leading cause of death in the United States and worldwide, while racial/ethnic disparities in CVD and CVD risks have persisted (Benjamin et al., 2017). Despite considerable efforts to eliminate these disparities through CVD risk reduction interventions, few review studies comprehensively investigated the cultural appropriateness, effectiveness, and theoretical frameworks of those interventions designed specifically for Korean Americans (KAs). KAs are at high risk for CVD, including high rates of unhealthy behaviors (consumption of a high-sodium diet, physical inactivity, smoking) as well as hypertension and diabetes (Shin, Keller, An, & Sim, 2018), while they are one of the fastest growing ethnic groups in the United States and the fifth largest group among Asian Americans (Hoeffel, Rastogi, Kim, & Shahid, 2012; Pew Research Center, 2013). Findings from this review may help clinicians and researchers design and implement CVD risk reduction interventions for KAs who are underrepresented in cardiovascular (CV) health research.
Background
Despite the recommendations of Healthy People 2020 and other nation-wide health programs that prioritize the reduction of health disparities among ethnic minority populations, CV health disparities have little improved over the last two decades (Benjamin et al., 2017; U.S. Department of Health and Human Services, 2014). In an effort to close the gap of CV health disparities among ethnic minority populations and with growing recognition of the effectiveness of culturally relevant and age- and gender-appropriate interventions, investigators have attempted to integrate cultural aspects in health promotion interventions in a variety of ethnic populations, including Koreans in the United States (Joseph, Keller, Affuso, & Ainsworth, 2017; Keller, Coe, & Moore, 2014; S. S. Kim, 2017).
Replicating a well-tested intervention in the general U.S. population, or in a specific ethnic group, for implementation in another ethnic group is perhaps more efficient than designing a new intervention. However, a successful intervention in one ethnic group does not guarantee equal success in other ethnic groups. This is primarily related to the unique needs, preferences, and cultural values of each ethnic group (Song et al., 2010). Therefore, it is critical to understand how those cultural factors of the target ethnic group were incorporated in health interventions. In recent systematic reviews targeting Korean Americans (KAs), investigators have reported culturally relevant facilitators and barriers to breast and cervical cancer screening (Lee, 2015; Oh, Taylor, & Jacobsen, 2017). Another systematic review on culturally tailored interventions for chronic disease in KAs included 21 articles published from 1980 to 2011, including seven interventions related to CVD risks (Heo & Braun, 2014). Four of the seven were the primary study, while the rest included a pilot study or subsequent publications in addition to the primary study.
This review has international relevance because CVD is not only a national but also a global burden because of its high mortality and prevalence across countries in the world. According to a study on the burden of CVD worldwide, 17.9 million died from CVD (one-third of all deaths) and 422 million cases of CVD in 2015 (Roth et al., 2017). Also, there are potential unfavorable effects of immigration on CVD risks worldwide, such as increase hypertension and other CVD risks (Rosenthal, 2014). These findings highlight the importance of identifying potential strategies to reduce CVD risks for all regions of the world.
Purpose of This Review
The purpose of this article was to update and extend prior reviews and synthesize the available literature regarding culturally appropriate interventions designed to reduce CVD risks in KAs. We specifically examined existing interventions to identify (a) how cultural factors (e.g., needs, preference, values) of KAs were incorporated in study design and delivery, (b) how successfully the interventions improved CV health and engaged participants, and (c) the usefulness of theory in guiding interventions if reported in reviewed studies.
Method
This systematic review was conducted following the 5-stage process recommended by Whittemore and Knafl (2005): problem identification, literature search, data evaluation, data analysis, and presentation.
Problem Identification
For this review, we included studies that met the following eligibility criteria. Inclusion criteria were that the studies (a) were conducted in KA adults (⩾18 years) who resided in the United States, (b) reported the intervention effects on CVD risk reduction, (c) addressed culture in study design and delivery elements, and (d) were published in English between January 2000 and August 2017. The exclusion criteria were that studies (a) published only aggregate data of the multiethnic groups, (b) were preliminary findings or a pilot study for a larger study, or (c) were not the primary study (i.e., if more than one publication resulted from a study, we included only the primary study and not any subsequent publications in which the same investigators were discussing the same sample). Two authors (C.S. and J.S.) conducted search procedures and the full-text review to determine the eligibility. If the research reports were not clear whether they met the eligibility criteria, the third author (C.K.) reviewed, and selection of eligible studies was determined by all authors reaching a consensus.
Literature Search
We searched the electronic databases of PubMed, Cumulative Index for Nursing and Allied Health Literature (CINAHL), PsycInfo, and Web of Science, between January 2000 and August 2017. The keywords related to interventions (health education, program, evaluation, intervention) and the target population (Korean, Korean immigrant, Korean American) were combined and used to search relevant articles. Of 1,887 articles identified initially, 23 duplicates were removed, and then 1,818 studies were excluded after screening a title and abstract. An additional 32 studies were excluded after full-text screening. This article presents a review of 14 eligible articles, and the flowchart of the selection process is illustrated in Figure 1.
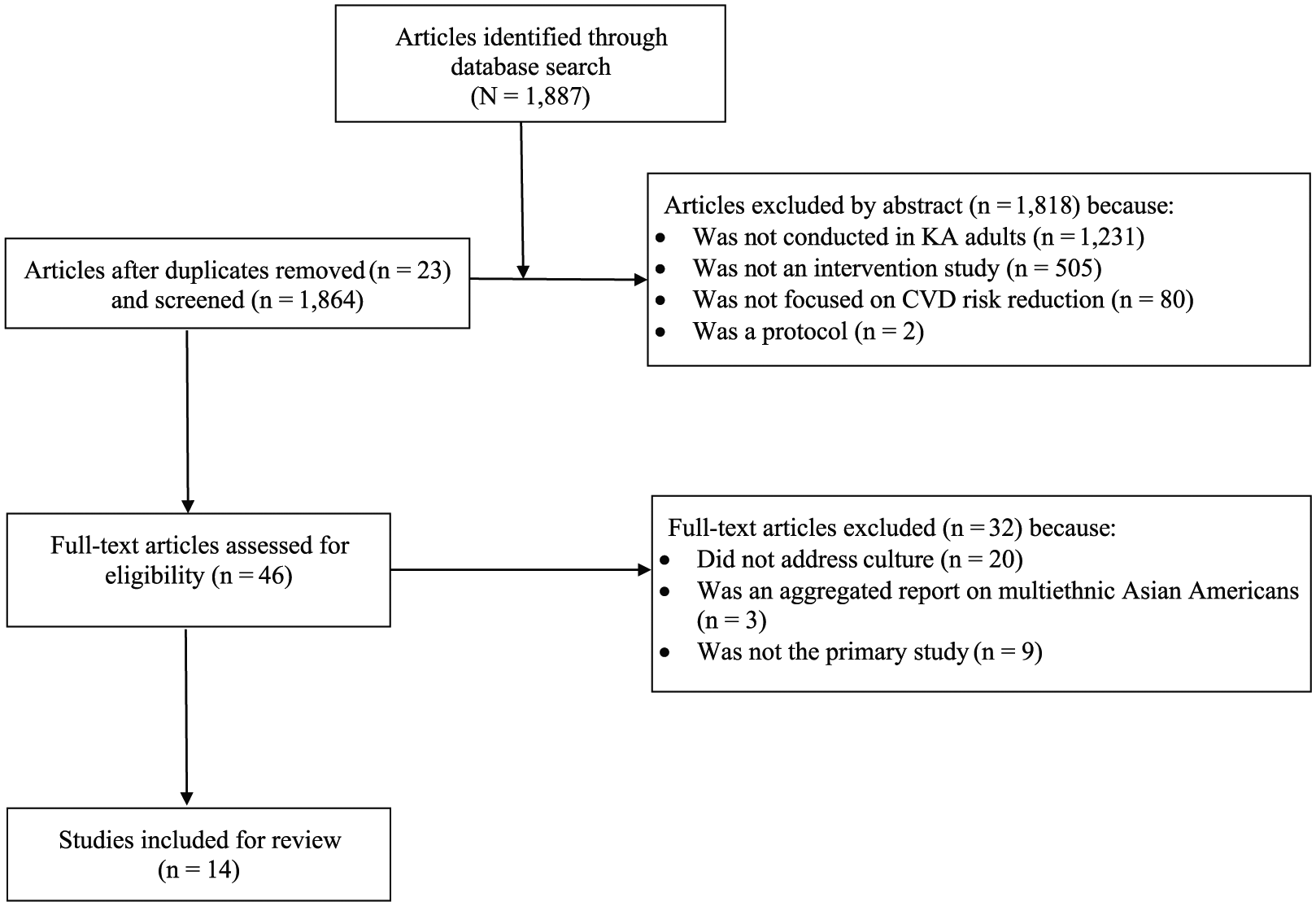
Flow diagram for study selection process.
Data Evaluation
Two authors (C.S. and J.S.) reviewed each study, performed data extraction independently, and then verified the results together. We extracted the following information: (a) characteristics of the reviewed studies (the authors and publication year, study design, sample and study location, intervention, data collection method and time points, and theoretical framework); (b) cultural appropriateness of interventions; and (c) effectiveness of interventions.
Data Analysis and Presentation
First, we examined the reviewed research articles to determine how interventions incorporated unique cultural factors (e.g., needs, preference, values) of KAs according to the two dimensions of cultural appropriateness of interventions (i.e., surface structure and deep structure) characterized by Resnicow, Baranowski, Ahluwalia, and Braithwaite (1999). More specifically, surface structure involves external intervention components (i.e., materials, communication channels, settings, staff, and recruitment strategies) reflecting the characteristics of a target population and can influence the appeal, salience, and acceptance of the intervention, whereas deep structure refers to recognizing and leveraging culturally normative practices and beliefs embedded in the target population and can influence health behaviors (Heo & Braun, 2014; Joseph et al., 2017; Resnicow et al., 1999). We examined each intervention study for five components of surface structure: (a) intervention materials, (b) communication channel for delivering intervention, (c) settings for delivering intervention, (d) culturally relevant staff (recruiters and educators), and (e) methods for recruiting participants. We then examined deep structure to evaluate whether cultural factors (e.g., norms and values) of KAs were recognized and leveraged in delivering interventions.
Second, we assessed the effectiveness of interventions by significant improvements in CV health and the engagement of participants. In this review, we defined CV health by following the American Heart Association (AHA)–defined seven CV health metrics (Benjamin et al., 2017): blood pressure (BP), physical activity (PA), total cholesterol (TC), diet, body mass index (BMI), smoking status, and fasting blood glucose (FBG). We assessed the engagement of participants in the intervention by retention and satisfaction rates. In addition, we evaluated the usefulness of theory/model if an intervention theory/model was reported in the reviewed studies: whether and how the core constructs of the intervention theory/model and cultural factors were linked to the intervention and CV health outcomes. Two authors (C.S. and J.S.) independently analyzed each reviewed study, and if consensus was not reached, the third author (C.K.) helped to resolve the discrepancies. The findings from the data analysis are displayed in three tables. Table 1 summarizes characteristics of the reviewed studies, and Table 2 presents cultural appropriateness. Table 3 reports effectiveness of interventions.
Summary of Included Studies.
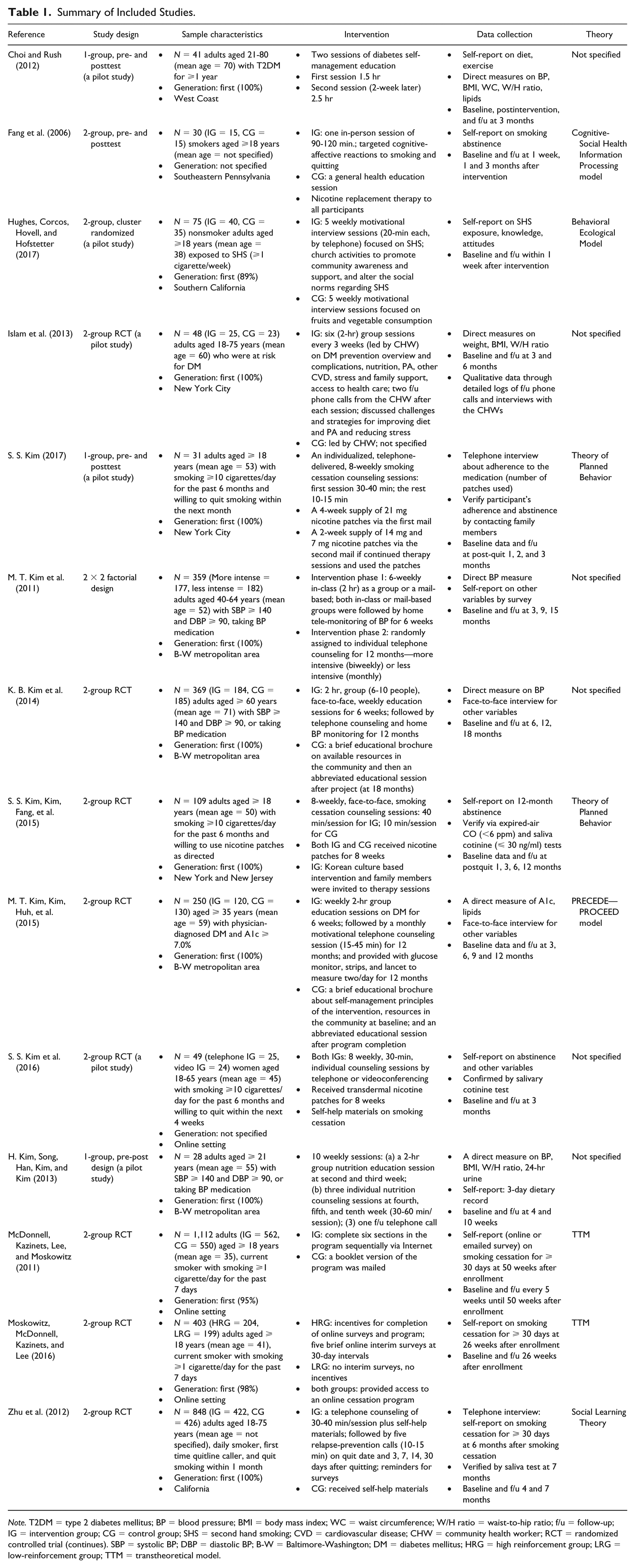
Note. T2DM = type 2 diabetes mellitus; BP = blood pressure; BMI = body mass index; WC = waist circumference; W/H ratio = waist-to-hip ratio; f/u = follow-up; IG = intervention group; CG = control group; SHS = second hand smoking; CVD = cardiovascular disease; CHW = community health worker; RCT = randomized controlled trial (continues). SBP = systolic BP; DBP = diastolic BP; B-W = Baltimore-Washington; DM = diabetes mellitus; HRG = high reinforcement group; LRG = low-reinforcement group; TTM = transtheoretical model.
Cultural Appropriateness of the Interventions.
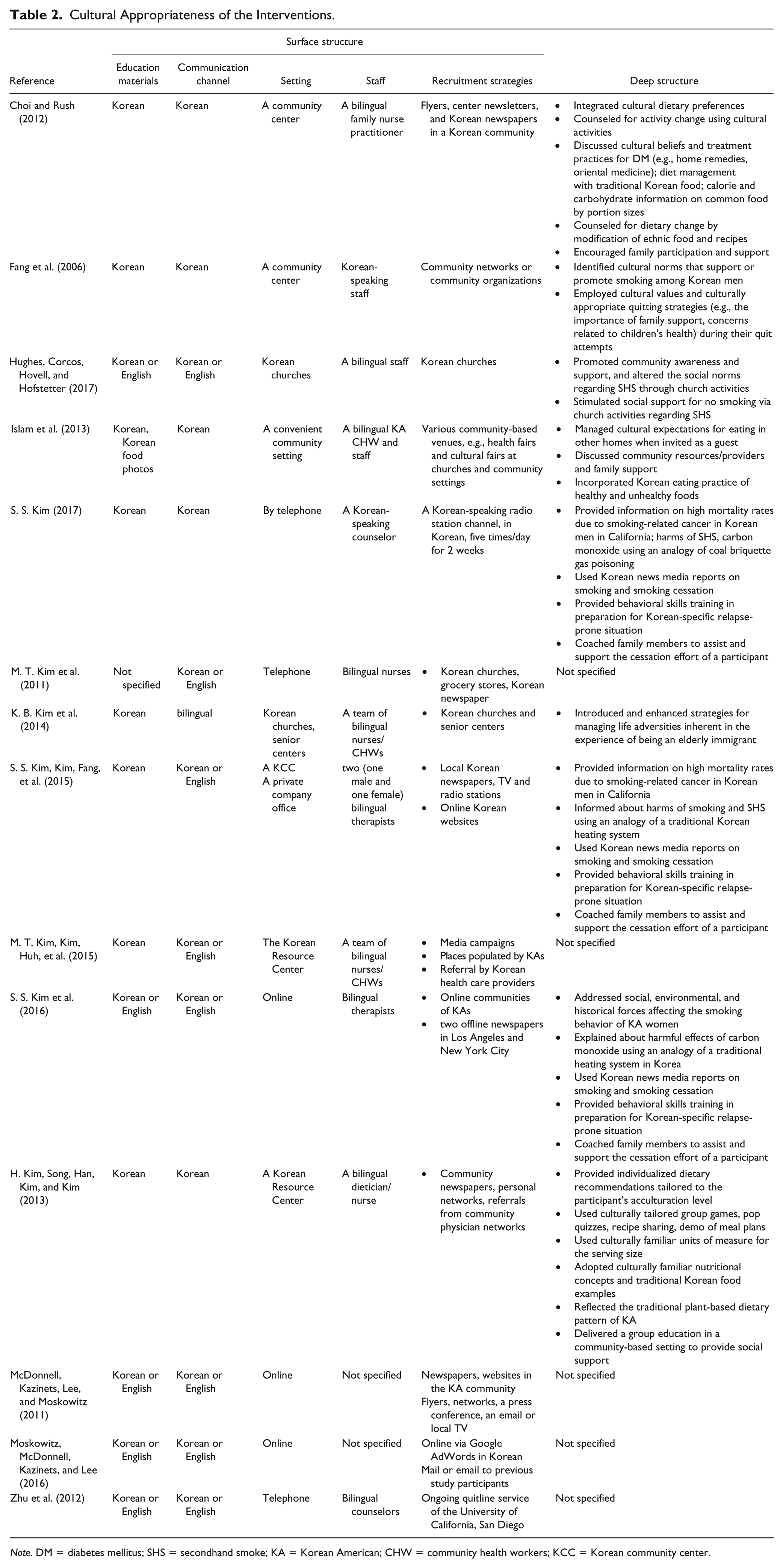
Note. DM = diabetes mellitus; SHS = secondhand smoke; KA = Korean American; CHW = community health workers; KCC = Korean community center.
Effectiveness of the Interventions.
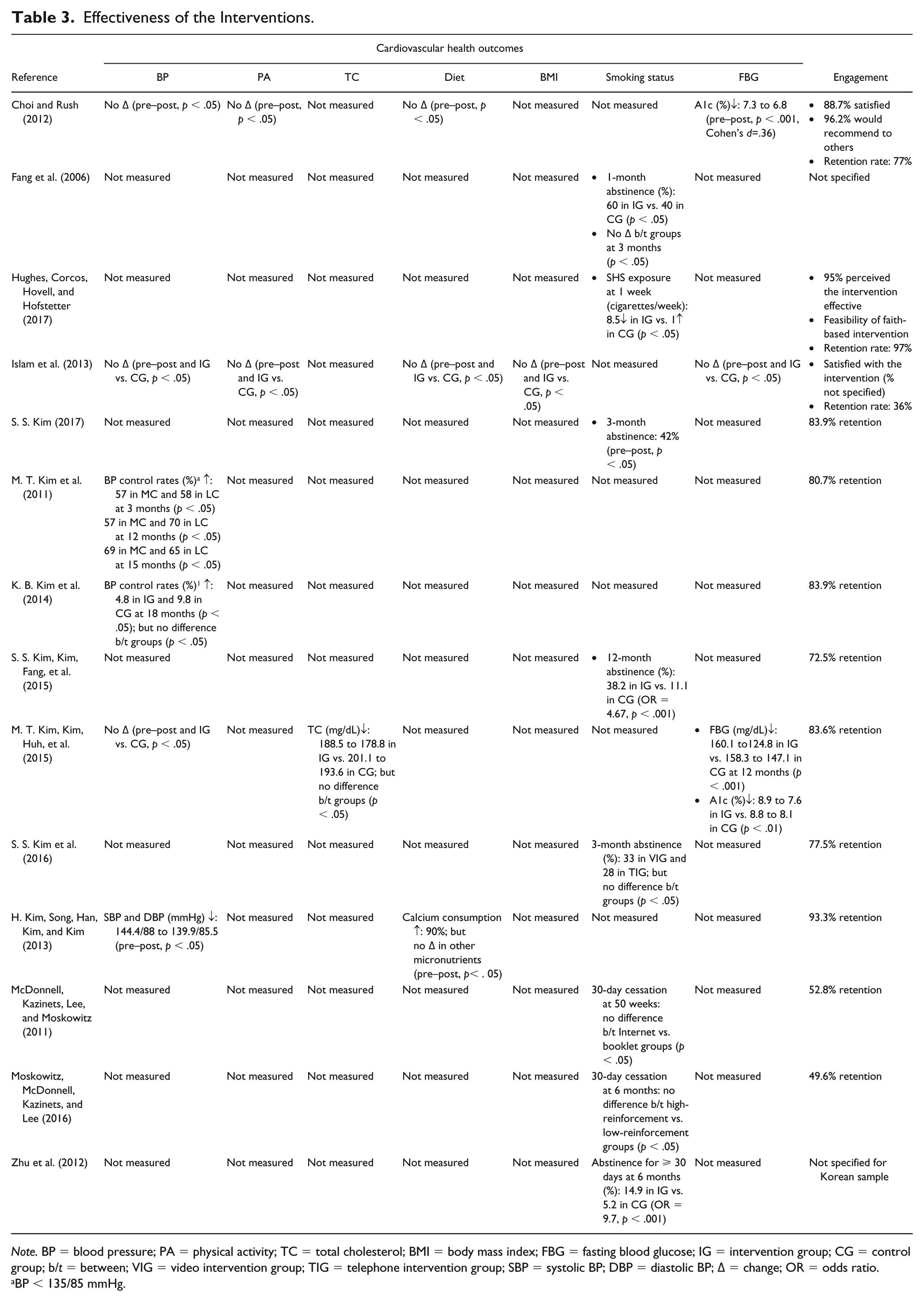
Note. BP = blood pressure; PA = physical activity; TC = total cholesterol; BMI = body mass index; FBG = fasting blood glucose; IG = intervention group; CG = control group; b/t = between; VIG = video intervention group; TIG = telephone intervention group; SBP = systolic BP; DBP = diastolic BP; ∆ = change; OR = odds ratio.
BP < 135/85 mmHg.
Results
Overview of Studies
All but two studies (Fang et al., 2006; S. S. Kim et al., 2016) specified recruitment of Korean-speaking KAs or indicated that their participants were predominantly (89%-98%) first-generation KAs. The samples were primarily adults aged 18 years and older (mean age ranged 35-70). Of 14 reviewed studies, 10 used a randomized controlled trial (RCT) with two groups (Hughes, Corcos, Hovell, & Hofstetter, 2017; Islam et al., 2013; K. B. Kim et al., 2014; M. T. Kim et al., 2011; S. S. Kim et al., 2016; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015; McDonnell, Kazinets, Lee, & Moskowitz, 2011; Moskowitz, McDonnell, Kazinets, & Lee, 2016; Zhu et al., 2012). The sample size ranged from 28 to 1,112, with the median of 92, and the power to detect changes before and after intervention and/or between groups was addressed in four studies (Choi & Rush, 2012; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015; Zhu et al., 2012).
Use and Usefulness of Theory
Of 14 reviewed studies, eight (Fang et al., 2006; Hughes et al., 2017; S. S. Kim, 2017; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015; McDonnell et al., 2011; Moskowitz et al., 2016; Zhu et al., 2012) reported a specific theory/model as the basis of interventions, and all of them were relevant to health behavior change, such as the Theory of Planned Behavior or the Transtheoretical Model (TTM). Five of them specified the cause of the problem being investigated (Hughes et al., 2017; S. S. Kim, 2017; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015; Zhu et al., 2012), four clearly indicated the core constructs and mechanism of the theory/model (Fang et al., 2006; S. S. Kim, 2017; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015), and five specifically explained how and what elements of the intervention linked to CV health outcomes (Hughes et al., 2017; S. S. Kim, 2017; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015; Zhu et al., 2012).
Despite the specification of the theory/model in eight of the 14 studies, only two of them (S. S. Kim, 2017; S. S. Kim, Kim, Fang, et al., 2015) clearly reported on all components necessary for a complete evaluation. For example, two studies (McDonnell et al., 2011; Moskowitz et al., 2016) indicated the use of the TTM as the theoretical basis for the intervention, but they provided very limited information about the cause of the problem (smoking behavior among KAs) and the mechanism of the model. They measured some constructs in the TTM (e.g., self-efficacy, social support); however, no specific information was provided about how the intervention targeted each stage of change and which elements of the intervention targeted self-efficacy or social support and smoking cessation.
In contrast, two other studies (S. S. Kim, 2017; S. S. Kim, Kim, Fang, et al., 2015) specified the cause of problem (smoking) and provided concise and sufficient information about the theory used (Theory of Planned Behavior). They also described relevant theoretical constructs and cultural factors (e.g., attitudes, self-efficacy, social norms), clearly linked them to each element of the intervention, and evaluated them associated with the primary CV health outcome (i.e., smoking abstinence).
Intervention Delivery
Individual sessions were provided in nine studies (Fang et al., 2006; Hughes et al., 2017; M. T. Kim et al., 2011; S. S Kim, 2017; S. S. Kim et al., 2016; S. S. Kim, Kim, Fang, et al., 2015; McDonnell et al., 2011; Moskowitz et al., 2016; Zhu et al., 2012), whereas five other interventions provided group sessions (Choi & Rush, 2012; Islam et al., 2013; H. Kim, Song, Han, Kim, & Kim, 2013; K. B. Kim et al., 2014; M. T. Kim, Kim, Huh, et al., 2015). The most common intervention approach was education/counseling sessions (Choi & Rush, 2012; Fang et al., 2006; Hughes et al., 2017; S. S. Kim, 2017; S. S. Kim et al., 2016; S. S. Kim, Kim, Fang, et al., 2015; McDonnell et al., 2011; Moskowitz et al., 2016), followed by education/counseling sessions combined with follow-up counseling sessions (Islam et al., 2013; H. Kim et al., 2013; K. B. Kim et al., 2014; M. T. Kim et al., 2011; M. T. Kim, Kim, Huh, et al., 2015; Zhu et al., 2012).
Half of the reviewed studies (Choi & Rush, 2012; Hughes et al., 2017; Islam et al., 2013; H. Kim et al., 2013; McDonnell et al., 2011; Moskowitz et al., 2016; Zhu et al., 2012) primarily emphasized cognitive strategies (e.g., knowledge, self-efficacy), while other half (Fang et al., 2006; K. B. Kim et al., 2014; M. T. Kim et al., 2011; S. S. Kim, 2017; S. S. Kim et al., 2016; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015) focused on both cognitive and behavioral strategies, such as self-monitoring of BP or glucose, developing dietary goals, and providing nicotine patches. Interventions were mostly (n = 7) provided by bilingual nurses or professional counselors (Choi & Rush, 2012; H. Kim et al., 2013; M. T. Kim et al., 2011; S. S. Kim, 2017; S. S. Kim et al., 2016; S. S. Kim, Kim, Fang, et al., 2015; Zhu et al., 2012). The duration and frequency of the interventions ranged from one time (90-120 min) to 10 weeks (weekly, 30 min to 2 hr per session), while a weekly intervention session was provided in eight studies (Hughes et al., 2017; H. Kim et al., 2013; K. B. Kim et al., 2014; M. T. Kim et al., 2011; S. S. Kim, 2017; S. S. Kim et al., 2016; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015).
Target Outcomes
Smoking behavior was the most common (n = 8) primary target outcome (Fang et al., 2006; Hughes et al., 2017; S. S. Kim, 2017; S. S. Kim et al., 2016; S. S. Kim, Kim, Fang, et al., 2015; McDonnell et al., 2011; Moskowitz et al., 2016; Zhu et al., 2012), while self-efficacy was the most often (n = 6) addressed among theoretically relevant constructs across studies (Fang et al., 2006; S. S. Kim, 2017; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015; McDonnell et al., 2011; Moskowitz et al., 2016). Other primary target outcomes include A1c/FBG (Choi & Rush, 2012; Islam et al., 2013; M. T. Kim, Kim, Huh, et al., 2015) or BP (H. Kim et al., 2013; K. B. Kim et al., 2014; M. T. Kim et al., 2011). The primary CV health outcomes were evaluated congruent with the theoretical basis in eight studies (Fang et al., 2006; Hughes et al., 2017; S. S. Kim, 2017; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015; McDonnell et al., 2011; Moskowitz et al., 2016; Zhu et al., 2012); however, only five of them evaluated theoretical outcomes (Fang et al., 2006; Hughes et al., 2017; S. S. Kim, 2017; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015). For example, Fang et al. (2006) evaluated and reported theoretical outcomes (e.g., risk perception, health beliefs, self-efficacy, pros, and cons) in addition to the primary CV health outcome (smoking abstinence), consistent with the theory they used (Cognitive-Social Health Processing Information model).
Objective measures (e.g., blood or salivary test) were used to assess the primary CV health outcomes in six studies (Choi & Rush, 2012; Islam et al., 2013; H. Kim et al., 2013; K. B. Kim et al., 2014; M. T. Kim et al., 2011; M. T. Kim, Kim, Huh, et al., 2015), while five studies used only self-report subjective data (Fang et al., 2006; Hughes et al., 2017; S. S. Kim, 2017; McDonnell et al., 2011; Moskowitz et al., 2016). Another three collected self-report data verified by objective data (S. S. Kim et al., 2016; S. S. Kim, Kim, Fang, et al., 2015; Zhu et al., 2012). Data were collected three or more times after the intervention in seven studies (Fang et al., 2006; K. B. Kim et al., 2014; M. T. Kim et al., 2011; S. S. Kim, 2017; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015; McDonnell et al., 2011).
Cultural Appropriateness of Interventions
Most interventions incorporated all five components of surface structure of cultural appropriateness. For example, Korean-speaking or bilingual (Korean/English) educators and counselors delivered interventions in all interventions (n = 14), while all but two studies (Moskowitz et al., 2016; Zhu et al., 2012) recruited participants via Korean media (newspapers, TV channels) or events in Korean communities. The intervention setting was a place familiar to KAs (e.g., a Korean community center) in eight studies (Choi & Rush, 2012; Fang et al., 2006; Hughes et al., 2017; Islam et al., 2013; H. Kim et al., 2013; K. B. Kim et al., 2014; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015), whereas four studies delivered interventions by telephone (S. S. Kim, 2017; Zhu et al., 2012) or online (McDonnell et al., 2011; Moskowitz et al., 2016), one used telephone or videoconferencing (S. S. Kim et al., 2016), and the other delivered the intervention at a Korean community center or via mail at the first phase, and then by telephone at the second phase (M. T. Kim et al., 2011).
Eight interventions incorporated deep structure of cultural appropriateness by leveraging the unique needs, preference, and cultural values of KAs in delivery of interventions (Choi & Rush, 2012; Fang et al., 2006; Hughes et al., 2017; Islam et al., 2013; H. Kim et al., 2013; S. S. Kim, 2017; S. S. Kim et al., 2016; S. S. Kim, Kim, Fang, et al., 2015). For example, traditional Korean food with recipes and serving-size measures familiar to Koreans was utilized in diet education (Choi & Rush, 2012; Islam et al., 2013; H. Kim et al., 2013). Social norms that encourage smoking among Korean men and cultural values that highly value family were discussed in counseling sessions for smoking cessation (Fang et al., 2006; Hughes et al., 2017; S. S. Kim, 2017; S. S. Kim et al., 2016; S. S. Kim, Kim, Fang, et al., 2015). Social support was incorporated during the intervention and/or follow-up period in eight studies (Fang et al., 2006; Hughes et al., 2017; Islam et al., 2013; S. S. Kim, 2017; S. S. Kim et al., 2016; S. S. Kim, Kim, Fang, et al., 2015). None of them measured or reported social support linking with CV health outcomes. Two studies measured and evaluated social norms to determine whether and how they specifically contributed to changes in the primary CV health outcomes (S. S. Kim, 2017; S. S. Kim, Kim, Fang, et al., 2015).
Outcome Efficacy
Of 14 reviewed studies, eight reported improvements in the primary target outcomes with a significant difference pre- and postintervention or between the intervention and control groups (Choi & Rush, 2012; Hughes et al., 2017; H. Kim et al., 2013; M. T. Kim et al., 2011; S. S. Kim, 2017; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015; Zhu et al., 2012). Only three of them reported an effect size (ES), such as Cohen’s d or odds ratio (OR): Cohen’s d = .36 (Choi & Rush, 2012); OR = 4.67 (equivalent to d = .85; S. S. Kim, Kim, Fang, et al., 2015); and OR = 9.7 (equivalent to d = 1.25; Zhu et al., 2012). The ES in each of those three studies was moderate to large (Cohen, 1988).
Six of the reviewed studies showed a short-term effect (Choi & Rush, 2012; Hughes et al., 2017; H. Kim et al., 2013; M. T. Kim et al., 2011; S. S. Kim, 2017; M. T. Kim, Kim, Huh, et al., 2015), and other two reported a long-term effect (S. S. Kim, Kim, Fang, et al., 2015; Zhu et al., 2012). For example, BP control rates were significantly improved and maintained over time for 12 months while the participants received intervention, but not sustained after completion of the intervention (K. B. Kim et al., 2014). In contrast, one study (S. S. Kim, Kim, Fang, et al., 2015) reported that the smoking abstinence rate in the intervention group was improved and maintained for 12 months, beyond the intervention period (8 weeks).
Successful retention of participants was reported in 11 studies, indicating that participants were engaged in the intervention (Choi & Rush, 2012; Hughes et al., 2017; Islam et al., 2013; H. Kim et al., 2013; K. B. Kim et al., 2014; M. T. Kim et al., 2011; S. S. Kim, 2017; S. S. Kim, Kim, Fang, et al., 2015; M. T. Kim, Kim, Huh, et al., 2015; McDonnell et al., 2011; Moskowitz et al., 2016). Median retention rates across the reviewed studies were 79%, while the lowest retention (36%) was reported in a study that targeted A1c/glucose (Islam et al., 2013), and the highest (97%) was in a study of secondhand smoking (Hughes et al., 2017). Satisfaction about intervention programs (89%-95%) was reported in 2 studies (Choi & Rush, 2012; Hughes et al., 2017).
Discussion
We reviewed 14 intervention studies on CVD risk reduction among KAs and identified significant gaps that further research should fill. An RCT, the most rigorous design, was most frequently used, and smoking behavior was the most common among the AHA’s seven CV health metrics. As reported in earlier reviews on CV health interventions in KAs and multiple ethnic groups (Heo & Braun, 2014; Walton-Moss et al., 2014), a weekly, individual, in-class education or counseling provided by health care professionals (e.g., nurses, counselors) was the most common form of intervention. All reviewed studies reported a culturally tailored, adapted, acceptable, or sensitive intervention for KAs, while targeting first-generation KA adults. The use of Korean or Korean/English in education materials and communication channels was the most frequently incorporated component of surface structure, while deep structure (e.g., social norms, social support) was leveraged through content in education or counseling. However, few evaluated whether and how those cultural factors interacted with interventions and health outcomes, as those evaluation was scant in health literature of other racial/ethnic populations (Barrera, Castro, Strycker, & Toobert, 2013; Castro, Barrera, & Holleran Steiker, 2010).
Most interventions reported improvements in CV health outcomes. However, few of them provided a theoretical rational when interpreting the results, such as how and which aspects of the theoretical constructs in the intervention brought success or failure. As noted by another review on health behavior interventions (Prestwich et al., 2014), the short-term effects of an intervention on target outcomes have often been reported in the reviewed studies; however, reports on long-term effects/sustainability have been rare. The interventions (K. B. Kim et al., 2014; M. T. Kim et al., 2011; M. T. Kim, Kim, Huh, et al., 2015) with a higher intensity and longer duration brought significant changes in health outcomes during intervention delivery but did not show long-term effects/sustainability.
Limitations and Strengths
Limitations of this review include representativeness and variability among reviewed studies. As most reviewed studies were conducted in large Northeastern cities in the United States and derived from sample-based data, caution should be taken in generalizing the results to a larger KA community or other racial/ethnic minority groups. The reviewed studies varied in study design (from a small-scale, one-group, pilot study to an RCT with two groups and a large sample size), measurement strategy (subjective or objective measures), and intervention and follow-up length. Due to this wide variability and lack of reports on ES in most of the reviewed studies, comparison between studies and pooling the results in a meta-analysis with an overall ES were not optimal.
Nevertheless, this review article has a number of strengths. We expanded the current literature regarding culturally appropriate interventions aimed CVD risk reduction among KAs by retrieving and reviewing the most up-to-date intervention studies relevant to the topic. To do that, we used a comprehensive search strategy with specified inclusion and exclusion criteria as well as multiple databases. We determined cultural appropriateness and effectiveness of the interventions by using well-defined criteria, such as surface and deep structures proposed by Resnicow et al. (1999) and significant changes in CV health based on the AHA’s seven metrics (Benjamin et al., 2017) and the engagement of participants.
Application
This review has shown that studies incorporated cultural factors (both surface and deep structure) of KAs into design and delivery of the intervention were more effective and brought significant improvements in CV health outcomes than nonculturally tailored approaches (e.g., a general health education delivered to the control group). This means not only delivery of interventions in the participant’s mother tongue, but also leverage of cultural values and norms of the target population should be considered when designing and implementing interventions (Heo & Braun, 2014; Joseph et al., 2017; Resnicow et al., 1999). We recommend future CV health interventions to extend the target to other areas of the seven CV health metrics (e.g., PA, diet) beyond the well-researched areas (e.g., smoking), as KAs have a great risk in those areas (Shin, Keller, An, & Sim, 2018).
As revealed in some successful interventions in this review, future interventions may consider incorporating behavioral strategies (e.g., self-monitoring of BP, providing nicotine patches) in addition to cognitive strategies (e.g., a lecture about harmful consequences of hypertension or smoking). This approach may help participants better learn how to link information provided by health education to their daily lives and lead to sustained lifestyle change, as a recent meta-analysis of PA interventions found that interventions emphasized behavioral strategies (e.g., self-monitoring of PA) than cognitive strategies (e.g., targeted knowledge about PA) were more effective (Conn, Hafdahi, & Mehr, 2011).
Sustainability of the intervention would be of great interests to not only clinicians but funding organizations and government agencies who work hard to promote public health, including CV health. Future researchers may include follow-up assessments beyond the intervention period so that the sustainability of the intervention can be determined.
Future research with a clear specification of the theoretical constructs relevant to the problem under investigation and clear links to specific inputs of interventions will provide meaningful guidelines for intervention development targeting these constructs and contribute to the empirical literature: how the intervention worked or failed as well as when to modify which aspects and how (Davis, Campbell, Hildon, Hobbs, & Michie, 2015; Keller, Fleury, Sidani, & Ainsworth, 2009). Given that social support was reported as the most salient cultural value in KAs (Heo & Braun, 2014; Shin, Keller, & Sim, 2018), investigators may adapt a theoretical framework that incorporate social support in CV health intervention for KAs. An in-depth exploration of social support may contribute to the specification of the critical components that may be deployed in “deep structure” of culturally relevant CV health interventions among KAs.
The validity of intervention outcomes may be improved by conducting rigorous RCTs with an optimal sample size for an adequate power, reliable and valid objective measures, and adequate follow-up lengths. Limitations related to generalizability could be overcome by conducting multisite or population-based studies in the future. Reports of ES in future research may enable systematic reviews to make statistically valid conclusions.
Conclusion
CVD risk reduction via successful interventions is critical in prevention and control of CVD events as well as the progression of disease. The CV health can be improved by achieving optimal levels of the AHA’s seven metrics (i.e., BP, PA, TC, diet, BMI, nonsmoking, FBG). However, designing an intervention to achieve meaningful clinical changes (e.g., BP < 120 mmHg) and sustain it to significantly impact population health is challenging. We conducted this review to synthesize the available literature regarding culturally appropriate and effective interventions designed to reduce CVD risks in KAs. Given the available evidence through this review and the heterogeneity of the interventions, it is difficult to state which interventions might work the best. Continued efforts for thoughtfully deploying and evaluating of cultural factors that are congruent with the problem under investigation, the theoretical framework, and the intervention will ensure a successful intervention during and beyond the intervention delivery, which will lead to closing the gap in CV health disparities among ethnic minority populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.