
Abstract
Variability and factors influencing quality of life (QOL) in breast cancer patients having chemotherapy were examined in a longitudinal prospective cohort study in two teaching hospitals in China. Physical, mental, social/family, and functional QOL changed significantly over time with varying patterns. In addition, various factors influenced the QOL of breast cancer patients at each chemotherapy cycle. Health professionals should focus on critical time periods during chemotherapy, particularly at baseline and during the fourth and fifth cycles when the QOL in our sample was at the lowest point, and they should provide additional support to patients to ensure that chemotherapy is delivered in an optimal fashion.
Introduction
Breast cancer is the most common malignancy in women worldwide, with nearly 1.7 million new cases diagnosed in 2012 (Salem et al., 2017). From 1980 to 2011, the incidence of breast cancer rose from 6.4/100,000 to 31.93/100,000 in China (Fang, Wu, Zhang, & Ma, 2012). Breast cancer is characterized by high disease incidence, long survival time, and special lesion sites. Therefore, breast cancer patients face the fear of cancer recurrence and various treatment side-effects after surgery, as well as a damaged body. All of these factors severely affect the quality of life (QOL) of breast cancer patients. To our knowledge, this was the first study in China to examine the variability and factors influencing QOL in breast cancer patients over chemotherapy cycles to help health professionals provide additional support to patients aiming to ensure that chemotherapy is delivered in an optimal fashion.
Background
Chemotherapy is able to reduce the risk of breast cancer recurrence by 30% to 50% (Moulder & Hortobagyi, 2008). When the tumor is removed, residual tumor cells are easily killed by anticancer drugs. Various combinations of drugs are often used to strengthen the anticancer effects and reduce side-effects, including the TAC regimen (docetaxel, doxorubicin, and cyclophosphamide). TAC has been shown to outperform as other adjuvant treatments in node-positive and node-negative breast cancer patients, providing longer term disease-free survival and overall survival benefits (Early Breast Cancer Trialists’ Collaborative Group, 2012; Mackey et al., 2013). The 10-year survival of breast cancer patients using the TAC regimen was 63.4% (Matikas et al., 2018).
Nevertheless, approximately three fourths of patients reported at least one problem, and three fifths reported two or more problems, including fatigue, sleep disruption, dry/itchy skin, pain, and feeling swollen; these were the most common side-effects reported by patients receiving chemotherapy (McFarland, Shaffer, Tiersten, & Holland, 2018); there was an association between QOL and chemotherapy and its adverse effects, as well as with anxiety and depressive symptoms (Daldoul et al., 2018; da Mata Tiezzi et al., 2017; Hamer et al., 2017; Jacob, Kalder, & Kostev, 2017).
Currently, QOL is believed to be the most sensitive and powerful indicator of breast cancer outcomes. Over the past decades, considerable breast cancer QOL research resources has been devoted to evaluation scales, as well as the effects of demographic and clinical characteristics on QOL. By contrast, the variability of QOL with breast cancer patients over chemotherapy cycles has received less attention.
Therefore, the purpose of this study was to examine the variability of physical, mental, social/family, and functional QOL and their influencing factors at every treatment cycle. Specifically, the authors sought to
describe the variability in physical, mental, social/family, and functional QOL over chemotherapy cycles.
examine the factors influencing physical, mental, social/family, and functional QOL at each chemotherapy cycle.
Making such information available could help health care professionals to take appropriate intervention measures at various treatment times to prevent or alleviate the factors that will affect the QOL of breast cancer patients. In addition, effective interventions aiming to prevent the development of influencing factors need to be identified to save health care costs, reduce patient morbidity, and improve QOL.
Method
Design and Setting
This was a two-center, longitudinal prospective cohort study of patients with breast cancer receiving chemotherapy. Both hospitals were university-affiliated teaching hospitals located in southwest China. From July 2016 to February 2017, a total of 270 breast cancer patients were eligible according to the inclusion criteria, and 76 were excluded according to exclusion criteria. Therefore, 194 participants were included in this study. A total of 20 participants were lost through the six cycles of chemotherapy. Finally, only 174 patients completed the investigation. The final response rate was 89.69%.
The inclusion criteria were as follows: females who were older than 18 years; initial diagnosis of unilateral breast cancer received surgical treatment and were prescribed six cycles of TAC (docetaxel, adriamycin, and cyclophosphamide) after surgical treatment; first chemotherapy treatment was introduced 3 to 5 days after the initial surgery; willingness to receive and sign informed consent for this study; and ability to accurately complete the scales. The exclusion criteria were as follows: patients who died or terminated treatment for various reasons during the treatments; refusal to participate in or continuously receive this survey; or used other treatment methods or drugs for any reason.
Instruments
A General Information Questionnaire designed by the research group was used to collect sociodemographic and disease information including age, marital status, education level, medical insurance status, and surgical methods.
The MD Anderson Symptom Inventory (Cleeland et al., 2000) was used to measure the symptoms at each measurement point. This scale is composed of two parts: The first part contains 13 items to measure the severity and degrees of pain, fatigue, nausea, sleep disturbed, distress, shortness of breath, amnesia, lack of appetite, drowsiness, dry mouth, sadness, vomiting, and numbness. Zero points are given if symptoms are not present; higher scores represent more serious symptoms and the highest score is 10 points; the second part contains 10 items to measure how the relevant symptoms affected patient’s life. This study mainly used the first part of the scale to measure the relevant symptoms and side-effects at each time point. A study by Cleeland et al. (2000) previously confirmed that this scale included most of the discomfort symptoms patients experience during and after chemotherapy. It can be used to investigate symptoms for clinical research. Internal consistency reliability of the scale was established, with the alpha coefficients ranging from .730 to .950 in this study.
The Hospital Anxiety and Depression Scale (HADS; Zheng, Wang, & Li, 2003) was used to measure the degree of anxiety and depression at each time point in this study. This scale includes two parts: the anxiety subscale (HADS-a) and the depression subscale (HADS-d). Each subscale contains seven items. The sum of the measured scores of all items is the score of the subscale. The higher the score is, the more serious the anxiety and depression are. A study by Zheng et al. (2003) classified a score of 9 points as the screening standard for anxiety and depression. Internal consistency reliability of the scale was established with alpha coefficients ranging from .769 to .931 in this study. Discriminant validity for this instrument has been established.
Functional Assessment of Cancer Therapy—Breast Cancer (FACT-B) Chinese version (Wan et al., 2007) was used to measure the level of QOL in breast cancer patients at each time point in this study. There were three reasons to choose FACT-B scale to measure QOL in this study: First, the FACT-B is a special scale used for QOL of breast cancer patients; second, this scale has been applied extensively in breast cancer patients in China with good reliability and validity; and third, this scale is composed of five dimensions with 36 items that primarily measure the physical, social/family, mental, and functional QOL of breast cancer patients, in accordance with the definition of QOL from the World Health Organization (1997). The alpha coefficients ranged from .636 to .788 in this sample. Discriminant validity for this instrument has been established. It required 15 to 20 min to complete all three scales.
Data Collection
For patients meeting the eligibility criteria, general demographic information, and disease information were collected with the Homemade General Information Questionnaire by one of our researchers according to the medical records. Then, the patients completed the scales independently postoperatively and 24 hr before chemotherapy. This information was considered to be the baseline information. Subsequently, the patients were instructed to complete the scales within 24 hr after finishing each treatment.
Data Analysis
Data from 194 participants were parallel double entered from the raw survey data to avoid errors during data entry using SPSS 17.0 statistical software. Once a participant was enrolled, the data were not excluded from any of the analyses to ensure consistency with intent-to-treat analysis. All inferential tests of statistical significance were two-sided with a criterion level of significance of 0.05. Descriptive data were expressed as the mean ± standard deviation. The Shapiro–Wilk test was used to check the normality of the data. Only when normality was established were one-way repeated measure ANOVA introduced to explore the variability of physical, mental, social/family, and functional QOL over time. When the sphericity test was not assumed, the Greenhouse-Geisser of Epsilon was used to adjust the degrees of freedom for the averaged test of significance. Multiple stepwise regression analysis was used to identify factors affecting physical, mental, social/family, and functional QOL at each treatment cycle. The cut-off for significance for all the statistical procedures was p ⩽ .05.
Ethical Considerations
This study was approved by the hospital ethics committee. All participants were informed of the purpose of the study that they would not suffer any harm as the result of the study and that they could withdraw from the study any time.
Results
General Information
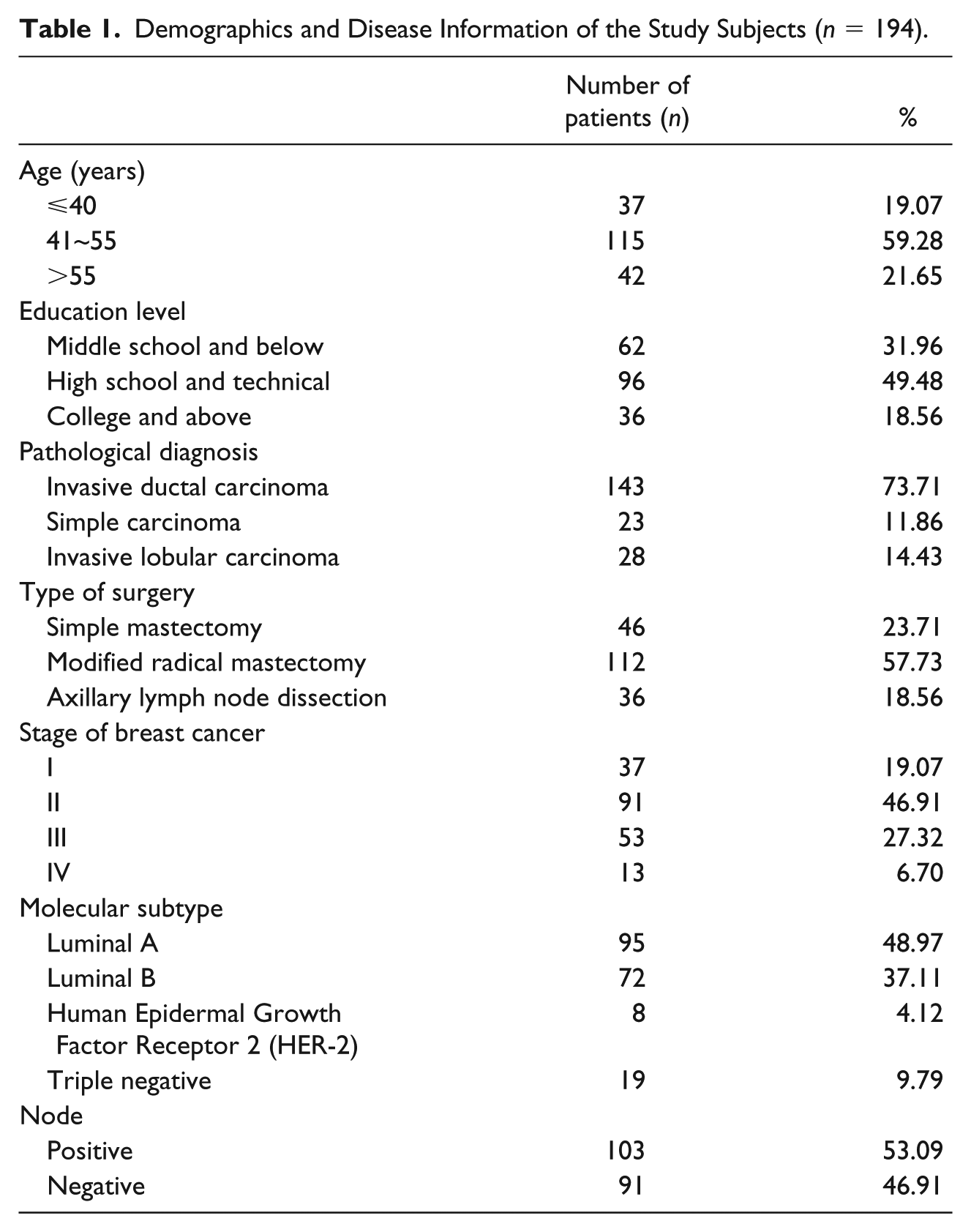
The general demographic information showed that the study subjects ranged in age from 25 to 68 years, with a mean age of 48.1 years; 59.28% of participants were aged 41 to 55 years. In terms of diagnosis, there were 143 cases of invasive ductal carcinoma, 23 cases of simple carcinoma, and 28 cases of invasive lobular carcinoma. In terms of surgical management, there were 46 cases of simple mastectomy, 112 cases of modified radical mastectomy, and 36 cases of axillary lymph node dissection (Table 1).
Demographics and Disease Information of the Study Subjects (n = 194).
Variability and Influencing Factors of QOL
The HADS scores and the physical, mental, social/family, and functional QOL scores are shown in Table 2. After all the variables in MD Anderson Symptom Inventory and HADS (anxiety and depression) were imputed to the stepwise regression analysis, significant relationships of these variables and physical, mental, social/family, and functional QOL were calculated (Table 4 and Supplemental Table 1).
Scores of HADS and Physical, Mental, Social/Family, and Functional QOL (M ± SD) at Each Time Point.
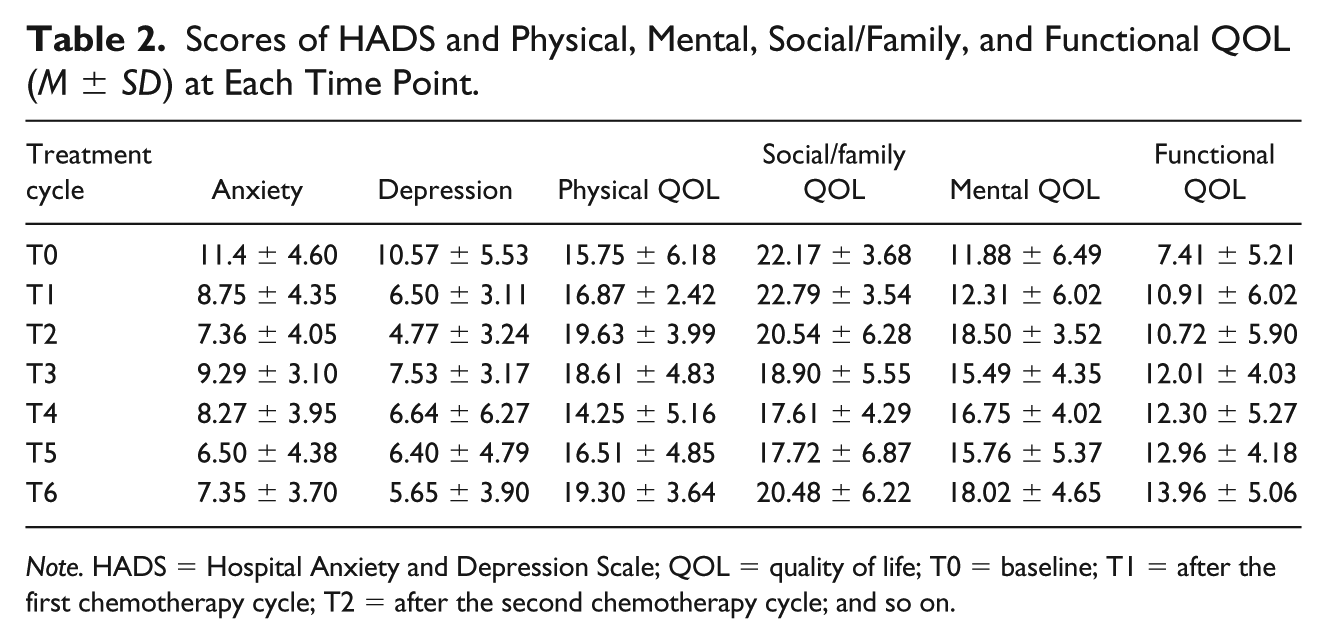
Note. HADS = Hospital Anxiety and Depression Scale; QOL = quality of life; T0 = baseline; T1 = after the first chemotherapy cycle; T2 = after the second chemotherapy cycle; and so on.
Physical QOL
Physical QOL scores changed significantly over time, F(4.264, 217.462) = 10.184, p < .005 (Table 3). Physical QOL scores were relatively low at baseline. Paired comparison analysis revealed that the physical QOL significantly increased from baseline to the highest level at Cycle 2 (p < .01) and decreased from Cycle 2 to the lowest at Cycle 4 (p < .005), then significantly increased from Cycle 4 to Cycle 6 (p < .005) (Table 2 and Figure 1).
Repeated Measures ANOVA.
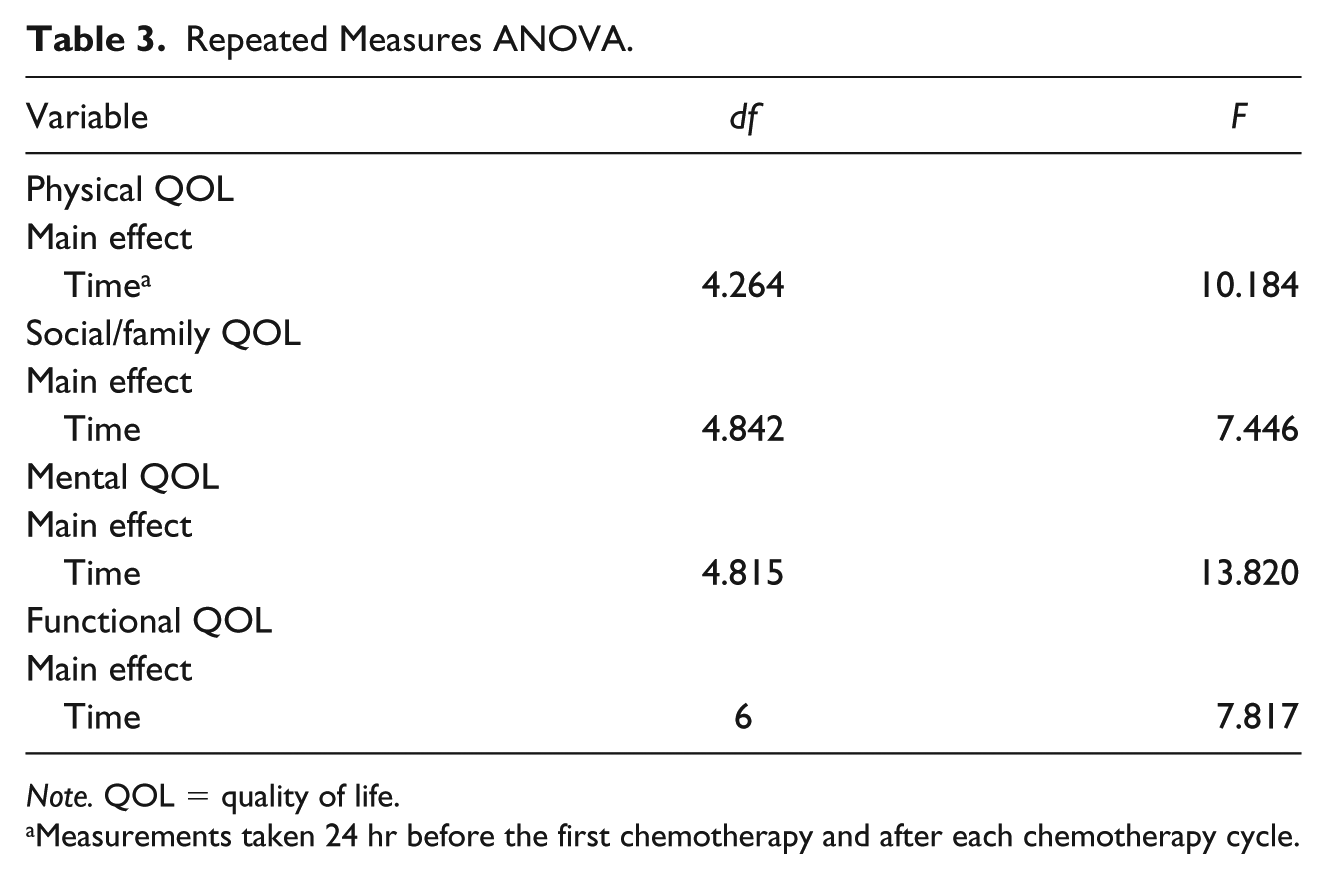
Note. QOL = quality of life.
Measurements taken 24 hr before the first chemotherapy and after each chemotherapy cycle.
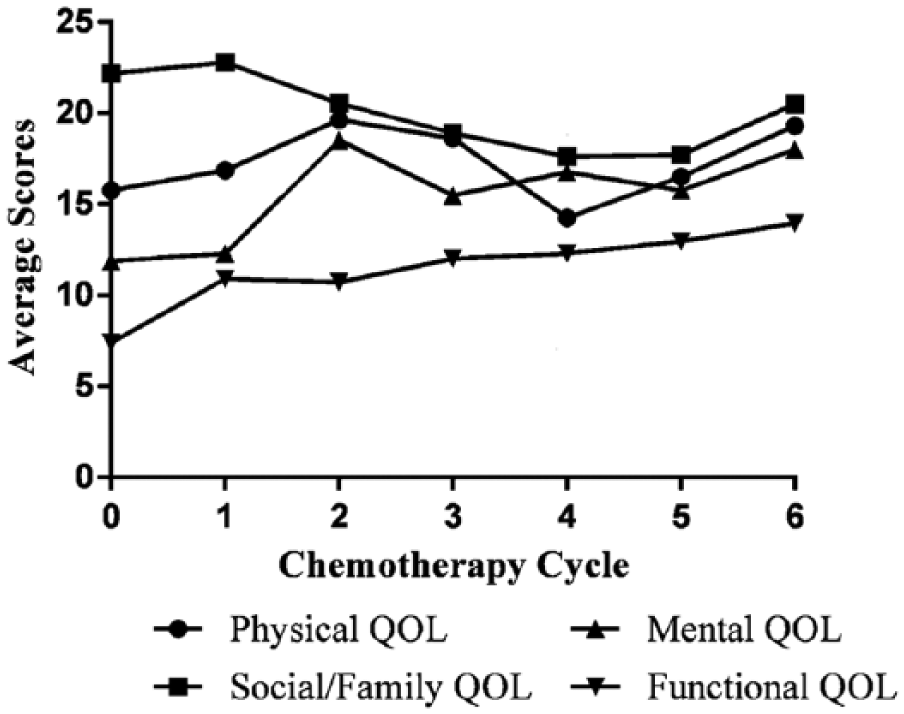
Patterns of physical, social/family, mental and functional QOL over the chemotherapy cycles.
Special attention should be paid to those time points when the QOL was relatively low. At baseline and Cycle 4, when the physical QOL was lower than other cycles, there was a significant relationship between depression, distress, drowsiness, and poor physical QOL (R = .987, R2 = .974, F = 521.545, p < .01), and there were significant relationships between pain, sadness, nausea, shortness of breath, and physical QOL (R = .995, R2 = .990, F = 89.446, p < .01) (Table 4 and Supplemental Table 1).
Summary of Influencing Factors of Physical, Social/Family, Mental and Functional QOL at Each Chemotherapy Cycle.
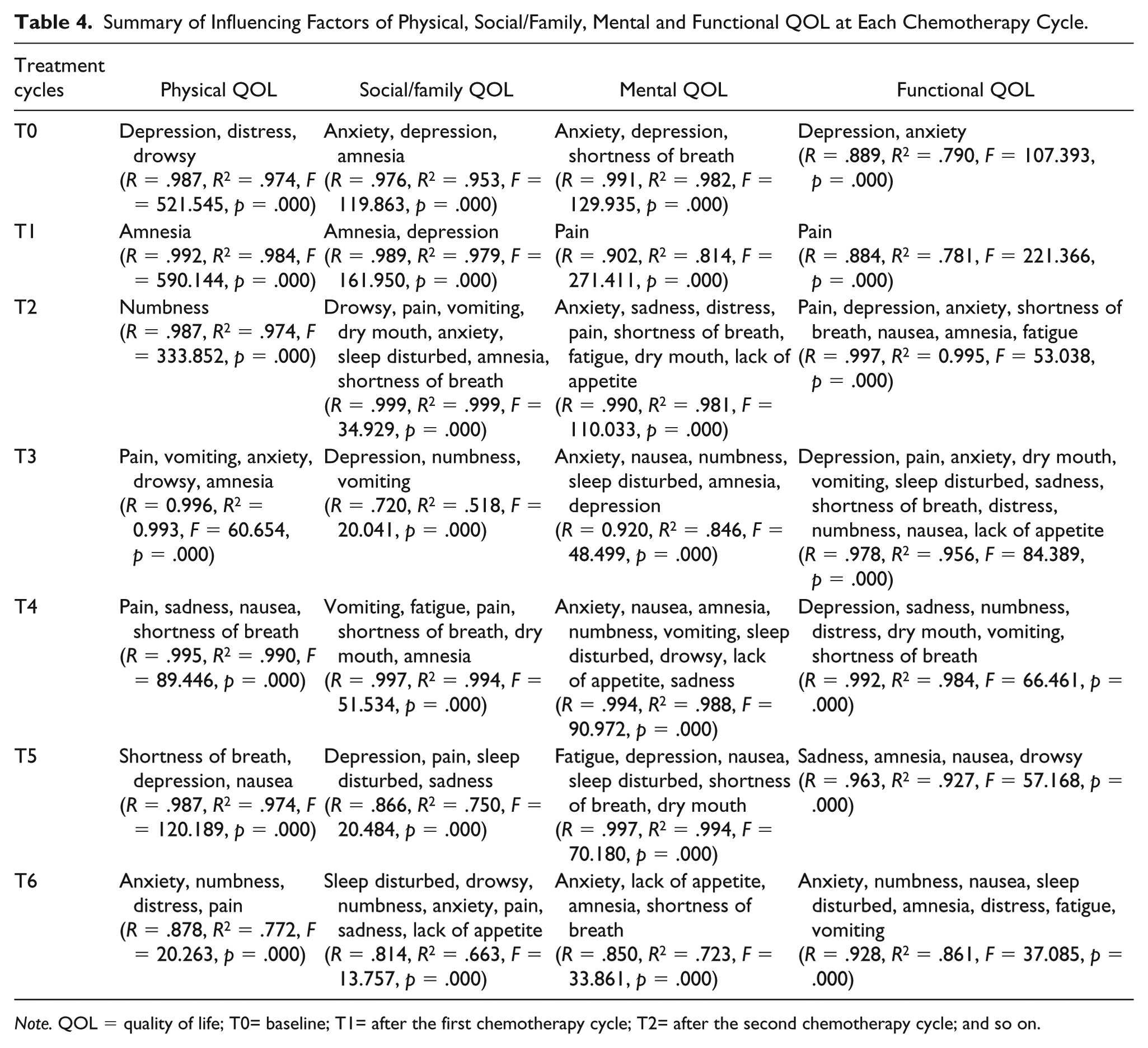
Note. QOL = quality of life; T0= baseline; T1= after the first chemotherapy cycle; T2= after the second chemotherapy cycle; and so on.
Social/family QOL
Social/family QOL scores changed significantly over time, F(4.842, 246.918) = 7.446, p < .005 (Table 3). The social/family QOL scores were relatively high at baseline, increasing to the highest point at Cycle 1. Paired comparison analysis demonstrated that it significantly decreased from Cycle 1 to Cycle 2 (p < .05), continuously decreased from Cycle 2 to the lowest point at Cycle 4 (p = .005), then significantly increased from Cycle 4 to Cycle 6 (p < .05) (see Table 2 and Figure 1).
For social/family QOL, at Cycle 5 when the participant passed the lowest point, there were significant relationships with depression, sleep disturbed, sadness, and pain (R = .866, R2 = .750, F = 20.484, p < .01; Table 4 and Supplemental Table 2).
Mental QOL
Mental QOL scores changed significantly over time, F(4.815, 245.554) = 13.820, p < .005 (Table 3). The mental QOL scores were at the lowest point at baseline. Paired comparison analysis showed that mental QOL significantly increased from Cycle 1 to the highest point at Cycle 2 (p < .005) and then changed significantly between Cycle 2 and Cycle 4 (p < .05) and between Cycle 5 and Cycle 6 (p < .05) (Table 2 and Figure 1).
For mental QOL, at baseline and Cycle 1 when the score was lower than other time points, there were significant relationships with anxiety, depression, and shortness of breath (R = .991, R2 = .982, F = 129.935, p < .01) and with pain (R = .902, R2 = .814, F = 271.411, p < .01) (Table 4 and Supplemental Table 3).
Functional QOL
The functional QOL changed significantly over time, F(6, 270) = 7.82, p < .005 (Table 3). The scores of functional QOL were the lowest at the baseline, and then displayed a gradual upward trend with slight fluctuations (Table 3 and Figure 1). Paired comparison analysis revealed that the functional QOL scores significantly changed between baseline and cycle 1 (p = .005) and between Cycle 2 and Cycle 6 (p < .005) (Table 2 and Figure 1).
For functional QOL at baseline when the score was lowest over the chemotherapy, there was a significant relationship with depression and anxiety (R = .889, R2 = .790, F = 107.393, p < .01; see Table 4 and Supplemental Table 4).
Discussion
This study involved a large sample using reliable and valid instruments and longitudinal design to identify the variability of patterns and influencing factors on physical, mental, social/family, and functional QOL over chemotherapy cycles in Chinese breast cancer patients receiving TAC chemotherapy. Several important findings were made. First, the physical, social/family, mental, functional QOL changed significantly over time but with different patterns. Second, there were different symptoms affecting the physical, social/family, mental, and functional QOL at each treatment cycle.
The studies of Salonen, Kellokumpu-Lehtinen, Tarkka, Koivisto, and Kaunonen (2011) and Schmidt et al. (2012) showed that QOL changed over time. However, we found no study concerning how breast cancer patients’ physical, social/family, mental, and functional QOL changed over each chemotherapy cycle. Our results provided clear data regarding the changing patterns of the physical, mental, social/family, and functional QOL over a chemotherapy course.
In addition, we clearly showed when the physical, mental, social/family, and functional QOL were the highest and lowest during chemotherapy. The results tested and confirmed that participants who received TAC chemotherapy regimen reported significantly the lowest physical QOL and social/family QOL at the fourth chemotherapy cycle, a finding generally consistent with the literature reporting the variability of patterns in QOL (Berger, Lockhart, & Agrawal, 2009).
However, in the present study, mental QOL was the lowest at baseline, followed by the second cycle, a finding that may reflect the changing trend of chemotherapy toxicity according to the studies of Gauthier et al. (2018). In addition, functional QOL was the lowest at baseline and highest at the sixth chemotherapy cycle, with an upward trend from baseline to final chemotherapy in the present study. These findings may reflect the changing trend of chemotherapy toxicity according to the studies of Byar, Berger, Bakken, and Cetak (2006) and Martin et al. (2006) that showed that there were symptoms of pain and anxiety related to functional and mental QOL at baseline, and other severe symptoms related to physical QOL and social/family QOL at Cycle 4.
Almost all studies found that QOL declined if the patient experienced serious side-effects (Liu et al., 2013; Sultan, Choudhary, & Parganiha, 2017). Sultan found that patients became more worried about the future outcomes of the disease with the progression of the treatment course (Sultan et al., 2017). If this continued to occur, it could lead to discontinuation of the treatment and subsequent worsening health.
Therefore, clinicians should screen for influencing factors according to various scales. Especially at the postoperative stage prior to chemotherapy and at Cycle 1 when the physical, mental, and functional QOL were relatively low. Clinicians should also provide more help to breast cancer patients at Cycles 4 and 5 when they experience rather low physical and social/family QOL to prevent the negative outcomes that result from side-effects. Effective management of common side-effects of adjuvant chemotherapy can assist in relieving their negative impact on QOL. Combined smartwatch and social media intervention were recommended to promote breast cancer patients’ QOL (Pope, Zeng, Zhang, Lee, & Gao, 2018).
Limitation of the Study
There are several limitations in the current study that have to be acknowledged. First, the participants were selected from only two hospitals in China, possibly affecting the generalized of the results to other countries and areas. Second, only breast cancer patients with TAC chemotherapy regimen were considered in our study. Therefore, the findings cannot be generalized to other chemotherapy regimens. Third, the variability of patterns of the QOL was assessed based only on chemotherapy cycle, without considering general information, possibly affecting the reliability of the results. Finally, another limitation of this study was that we did not consider other important factors such as type of surgery, disease stage, time since treatment, molecular subtype, diagnosis, radiotherapy treatment, family members, and partners or friends, all of which may influence the QOL of breast cancer patients. Nevertheless, this was the first study from China to investigate the variability and influencing factors of QOL in breast cancer patients having chemotherapy at each treatment cycle. The results of this study can help provide a baseline for future research so that strategies aiming at addressing the needs for better practice in improving the QOL of breast cancer patients can be formulated.
Conclusion
We found that physical, social/family, mental, functional QOL changed significantly with various patterns over chemotherapy cycles. There are various symptoms affecting varying areas of QOL in different chemotherapy cycles; health care professionals should pay more attention to breast cancer patients at baseline, Cycle 1, Cycle 4, and Cycle 5 when the QOL was relatively low and with various factors affecting the QOL at different treatment cycles. Understanding the changing trends of QOL and influencing factors in different chemotherapy cycles may help health care professionals intervene appropriately at different treatment cycles to prevent or alleviate factors precisely. Furthermore, effective interventions to prevent the development of severe side-effects need to be identified to save health care costs and reduce patient morbidity. Nevertheless, special attention should be paid to the fact that these findings should not be extrapolated to other chemotherapy regimens other than TAC chemotherapy.
Implications for Practice and Research
Symptom screening and management should be obligatory during the chemotherapy for clinicians. First, clinicians should identify individuals who report higher chemotherapy-related symptoms early to prevent negative outcomes. Second, clinicians should reassess symptoms and determine their impact on physical, social/family, mental, and functional QOL over time. Third, physical activity was shown to improve functional QOL (Fisher et al., 2017), and exercise-based interventions also may improve QOL (Carayol, Delpierre, Bernard, & Ninot, 2015) for women undergoing breast cancer treatment. Therefore, clinicians should make individualized activity plan for breast cancer patients to improve their QOL.
Finally, qualitative research can explore patients’ experiences and understanding of chemotherapy-related symptoms and decreased QOL. Use of advanced statistical prediction models of symptoms and lower QOL are also recommended.
Supplemental Material
Supplementary_Material_cnr – Supplemental material for Variability and Influencing Factors of QOL in Breast Cancer Patients Having Chemotherapy
Supplemental material, Supplementary_Material_cnr for Variability and Influencing Factors of QOL in Breast Cancer Patients Having Chemotherapy by Zhongping Ai, Xiaolan Gao, Silin Zheng and Changbi Lu in Clinical Nursing Research
Footnotes
Acknowledgements
Thanks for Professor Roger Watson who provided writing assistance for this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.