
Abstract
Clinicians routinely perform bone marrow aspiration and biopsy (BMAB) to diagnose cancer and evaluate disease status; however, few studies address pain and distress with BMAB. A prospective descriptive–correlational design examined patients’ (N = 152) ratings of pain intensity (numeric rating scale, 0-10) and distress (distress thermometer) at baseline and 5 min and 1 hr postprocedure. Data were analyzed using descriptive statistics, chi-square, and linear regression models. Mean postprocedure pain intensity at 5 min was moderate, 5.56 (SD = 3.03), and opioid use was associated with decreased pain at 1 hr (p < .001). Preprocedure administration of anxiolytics had no significant effect on distress reduction (p = .88). Being female, first-time biopsy, and increased preprocedure pain were significant predictors of postprocedure distress (p < .001). Treating anxiety alone may not be sufficient to lessen pain and distress. Individualized plans of care should be based on patient risk and response to procedure.
Introduction
Hematologic malignancies account for approximately 8% of newly diagnosed cancer cases annually (American Cancer Society, 2017). Bone marrow aspiration and biopsy (BMAB) is a standard procedure for diagnosing, classifying, and staging hematologic malignancies (Bain & Bailey, 2011). Advances in immunophenotyping, cytogenetic, and molecular science further substantiate the clinical value of BMAB in gauging responses to therapy and guiding treatment decisions (Trewhitt, 2001). Chromosomal abnormalities identified through BMAB can yield potential targets for the development of novel treatment agents (Riley et al., 2009). Because of its clinical utility, patients with hematological malignancies undergo repeated BMAB procedures over the course of their disease trajectory to evaluate the effectiveness of treatment regimens and confirm a molecular remission.
Background
Despite the evolving role for BMAB in the diagnosis and treatment of hematological malignancies, the technical aspects of performing the procedure have remained relatively unchanged for decades (Hjortholm, Jaddini, Hałaburda, & Snarski, 2013). After infiltrating the skin, subcutaneous tissue, and bone periosteum with a local anesthetic, a needle is inserted through the boney cortex to obtain a bone marrow aspirate and a core of bone marrow tissue. The posterior superior spine of the ileac crest is the preferred site for procuring bone marrow specimens (Hjortholm et al., 2013; Trewhitt, 2001). This procedure is commonly performed by hematologists, oncologists, advanced practice registered nurses, and physician assistants (Naegele et al., 2015; Trewhitt, 2001). BMAB is a relatively safe procedure and rarely leads to serious complications; however, BMAB is a painful procedure often associated with anxiety (Degen, Christen, Rovo, & Gratwohl, 2010).
Few prospective observational studies address the prevalence and severity of pain and anxiety with BMAB. Vanhelleputte, Nijs, Delforge, Evers, and Vanderschueren (2003) evaluated 132 patients with hematological malignancies undergoing BMAB, and reported pain in 86%, with 36% experiencing moderate to severe pain. Higher estimates of pain, 91% of 184 patients, were found with bone marrow biopsy with 50% having moderate to severe pain for a median pain duration of 36 hr (Valebjørg et al., 2014). Pain ratings with BMAB were severe (defined as ⩾ 54 on a visual analog scale, 0 to 100) for 32% of 235 adult patients with hematological malignancies (Lidén, Olofsson, Landgren, & Johansson, 2012), and moderate to severe (⩾ 4, 0-10) for 44 of 69 patients (63.7%; Portnow, Lim, & Grossman, 2003). Findings from qualitative research likened the pain experience from BMAB to posttraumatic stress with some participants ranking the procedure as the worst part of their cancer experience (McGrath, Rawson-Huff, & Holewa, 2013). Conversely, a lower mean and median pain rating, 2.8 and 1.9 (range = 0-10), respectively, were obtained from 202 patients having BMAB, and 21% had no pain (Tanasale, Kits, Kluin, Trip, & Kluin-Nelemans, 2013). Pain is associated with higher levels of anxiety (Tanasale et al., 2013; Yuvalı Karacan, Demircioğlu, & Ali, 2017).
Brunetti et al. (2011) who evaluated 152 patients undergoing BMAB documented a similar incidence for any level pain and anxiety, 78% and 71%, respectively. Anxiety should be routinely assessed with BMAB, as it can be an important predictor of pain (Kuball, Schuz, Gamm, & Weber, 2004). Other studies measuring anxiety with BMAB estimate that as many as 70% of patients experience some level of anxiety with BMAB, even when anxiolytic medications are administered (Lidén et al., 2012; Park et al., 2008). Patients who experience higher preprocedure anxiety tend to be less willing to have subsequent BMAB procedures and experience higher levels of pain (Kuivalainen, Ebeling, & Rosenberg, 2013; Liden, Landgren, Arnér, Sjölund, & Johansson, 2009).
Currently, there are a lack of predictive models to identify patients at risk of experiencing moderate to severe pain and/or anxiety with BMAB. The inability to stratify patients at greater risk for moderate to severe pain and anxiety jeopardizes patient responses and their willingness and ability to tolerate BMAB procedures. Studies identify that younger age (Tanasale et al., 2013), longer procedure times (Kuball et al., 2004; Vanhelleputte et al., 2003), inadequate patient preparation and education (Degen et al., 2010), procedure-related complications (Kuball et al., 2004; Vanhelleputte et al., 2003), having undergone a prior BMAB (Degen et al., 2010), and inexperience of provider performing the procedure (Kuball et al., 2004; Tanasale et al., 2013) place patients at risk of greater pain and/or anxiety. Additional evidence disputes that higher body mass index (BMI > 30) is associated with increased pain with BMAB (Tanasale et al., 2013; Vanhelleputte et al., 2003). Understanding risks for greater pain, anxiety, and distress levels with BMAB has important implications for individualizing patient plans of care and implementing effective interventions such as more aggressive management with pharmacological and nonpharmacological measures to minimize these symptoms.
The National Comprehensive Cancer Network (NCCN; 2018) defines distress as a “multifactorial unpleasant psychological (ie, cognitive, behavioral, emotional), social, spiritual and/or physical nature that may interfere with the ability to cope effectively with cancer, its physical symptoms, and its treatments” (pp. DIS-2). The continuum of distress begins with common feelings of vulnerability, sadness, and fears in response to a situation and can progress to disabling states such as depression, anxiety, panic, social isolation, and an existential and spiritual crisis (NCCN, 2018). Distress, rarely addressed with BMAB, encompasses a broader range of psychological experiences than anxiety alone, and therefore, may be more representative of a patient’s experience (Holland et al., 2010). Pain and distress are uniquely measureable experiences.
Study Aims
The aims of this investigation were to (a) report patterns of pain severity, pain quality, and distress levels and their associations during and 1 hr following BMAB procedures; (b) explore differences in pain severity and distress levels with and without premedication; and (c) examine relevant demographic, clinical, and procedure-related predictors of pain and distress with BMAB.
Method
Study Design
This study utilized a prospective, descriptive–correlational, repeated measures design to investigate pain and distress with BMAB. Authors adhered to STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for quality and transparency of reporting for observational studies (von Elm et al., 2007).
Participants
The final sample comprised 152 adult hospitalized patients recruited from one of the three oncology inpatient units at a single academic medical center over 16 months. Approximately 400 BMAB procedures are performed annually across these units. Recruitment commenced in March 2014 and ended in June 2015. The advanced practice provider service and physician fellows covering the oncology service identified potential patients scheduled for BMAB. Study staff screened all eligible patients meeting inclusion criteria for the study. Inclusion criteria were age greater than 18 years, no known cognitive deficits, and able to read, speak, and understand English. Patients were also eligible if there were plans to administer a preprocedure single agent (opioid or benzodiazepine) for minimal sedation rendering patients in a drug-induced state, but able to respond normally to verbal stimuli (No Authors Listed, 2018). Patients were excluded if the plan for pain and anxiety management was moderate sedation, defined by a drug-induced depression of consciousness, which would preclude the ability to recall the experience (No Authors Listed, 2018). An apriori sample size calculation for statistical power was based on the analyses for multivariate regression models. Anticipating that approximately seven predictors per dependent variable (i.e., pain and distress), we targeted 150 patients consistent with Nunnally’s and Bernstein’s (1994) suggested minimum of 20 participants per predictor.
Data Collection
Demographic data were collected on age, height, weight, BMI, gender, type of malignancy (if known), and whether or not this was the patient’s first BMAB. Researchers recorded procedure-specific variables including the indication for BMAB and whether or not the patient received premedication, which was not influenced by the researchers and was dependent on patient and health care provider preferences. Patient-reported outcomes for pain intensity and distress were completed at three time points: baseline within 1 hr prior to procedure (before anticipating a peak effect of premedications), 5 min immediately postprocedure with recall during the procedure, and 1 hr postprocedure. Pain quality was also measured during (recalled 5 min after the procedure) and 1 hr postprocedure. Table 1 provides a detailed description of the study variables and their operational definitions, timing sequence of data collection, and validated scales/questionnaires utilized to measure each variable.
Description of Patient-Reported Study Variables.
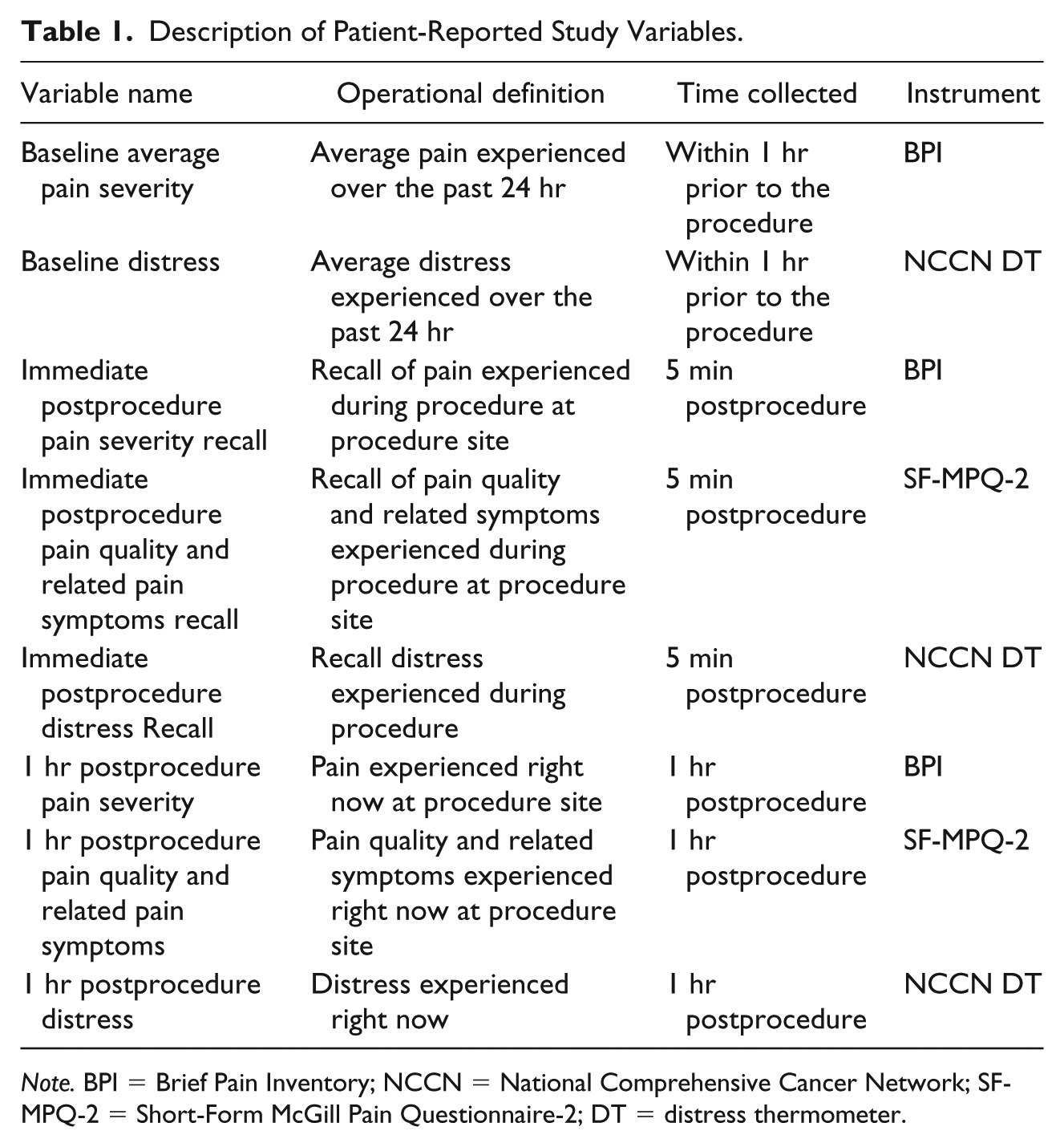
Note. BPI = Brief Pain Inventory; NCCN = National Comprehensive Cancer Network; SF-MPQ-2 = Short-Form McGill Pain Questionnaire-2; DT = distress thermometer.
Measures
Pain severity was measured using the Brief Pain Inventory (BPI) pain intensity scales, a numeric rating scale ranging from 0 (no pain) to 10 (pain as bad as you can imagine). Several investigators established reliability and validity for single-item use of pain intensity measures with oncology populations (Atkinson et al., 2011; Cleeland et al., 1994; Tittle, McMillan, & Hagan, 2003). Although cutoff points for pain severity categories are debated, pain severity for this study was classified as mild (1-4), moderate (5-6), and severe (7-10) according to Serlin, Mendoza, Nakamura, Edwards, and Cleeland (1995) and Li, Harris, Hadi, and Chow (2007) and moderate to severe pain (⩾ 5) as determined by Paul, Zelman, Smith, and Miaskowski (2005).
Distress levels were obtained using the NCCN distress thermometer (DT). Distress is conceptually defined as an unpleasant emotional state that includes unease, sadness, worry, anger, anxiety, and hopelessness. The DT is a validated scale that allows patients to rate their distress level on a single item scale from 0 (no distress) to 10 (extreme distress; Jacobsen et al., 2005). This measure is used extensively with cancer populations, and is recommended by the NCCN as a brief, easy to interpret, and meaningful measure to screen for procedure-associated distress (Holland et al., 2010). Scores ⩾ 4 are considered within the moderate to severe range (NCCN, 2018).
The Short-Form McGill Pain Questionnaire-2 (SF-MPQ-2) quantified pain quality and related symptoms. Comprised of 22 descriptors, each item is rated on a 0 (none) to 10 (worst possible) scale. The instrument is defined by four dimensions: intermittent pain, continuous pain, neuropathic pain, and affective pain. Although data were collected on all items, only the intermittent and affective pain dimensions were statistically analyzed in this study. Acceptable reliability and validity exists for the SF-MPQ-2 (Gauthier et al., 2014). Internal consistency reliability obtained from our study sample yielded acceptable Cronbach’s alphas (α) for both the intermittent and affective pain dimensions, (α = .79, α = .75), respectively.
Ethical Considerations
Prior to initiating the study, institutional review board approval was granted from the authors’ institution by the executive chair using the expedited procedure (IRB 819409). Written informed consent was obtained by all eligible and willing participants as a condition of participation in the study.
Data Analysis
Descriptive statistics were used to report all demographic, clinical, and procedure-related variables, and patient-reported outcomes. Bivariate associations were examined by Pearson’s correlation (r), and group differences were tested with chi-square tests (χ2), t tests, and ANOVA, as appropriate. Multivariate regression models were constructed to examine significant predictors of pain and distress as well as pain quality and related symptoms over time. To avoid overfitting, only significant bivariate associations (i.e., p ⩽ .05) were examined as predictor variables in the multivariate regression models. Interaction terms were also evaluated as predictors and baseline values were controlled when available to allow for prediction independent of initial values.
Results
Sample Characteristics
The study sample of 152 participants had a mean age of 56.08 years (SD = 14.72, range = 20-83) with 55.6% (n = 85) being male. Mean BMI was 27.34 (SD = 5.44, range = 17-48). Table 2 reports participant- and procedure-related information. For the majority (85.9%) of participants, the entire procedure time documented in the health record lasted up to 45 min with start times when patients were positioned and draped and end times when drape were removed and patients repositioned.
Sample Demographic and Clinical Characteristics (N = 152).
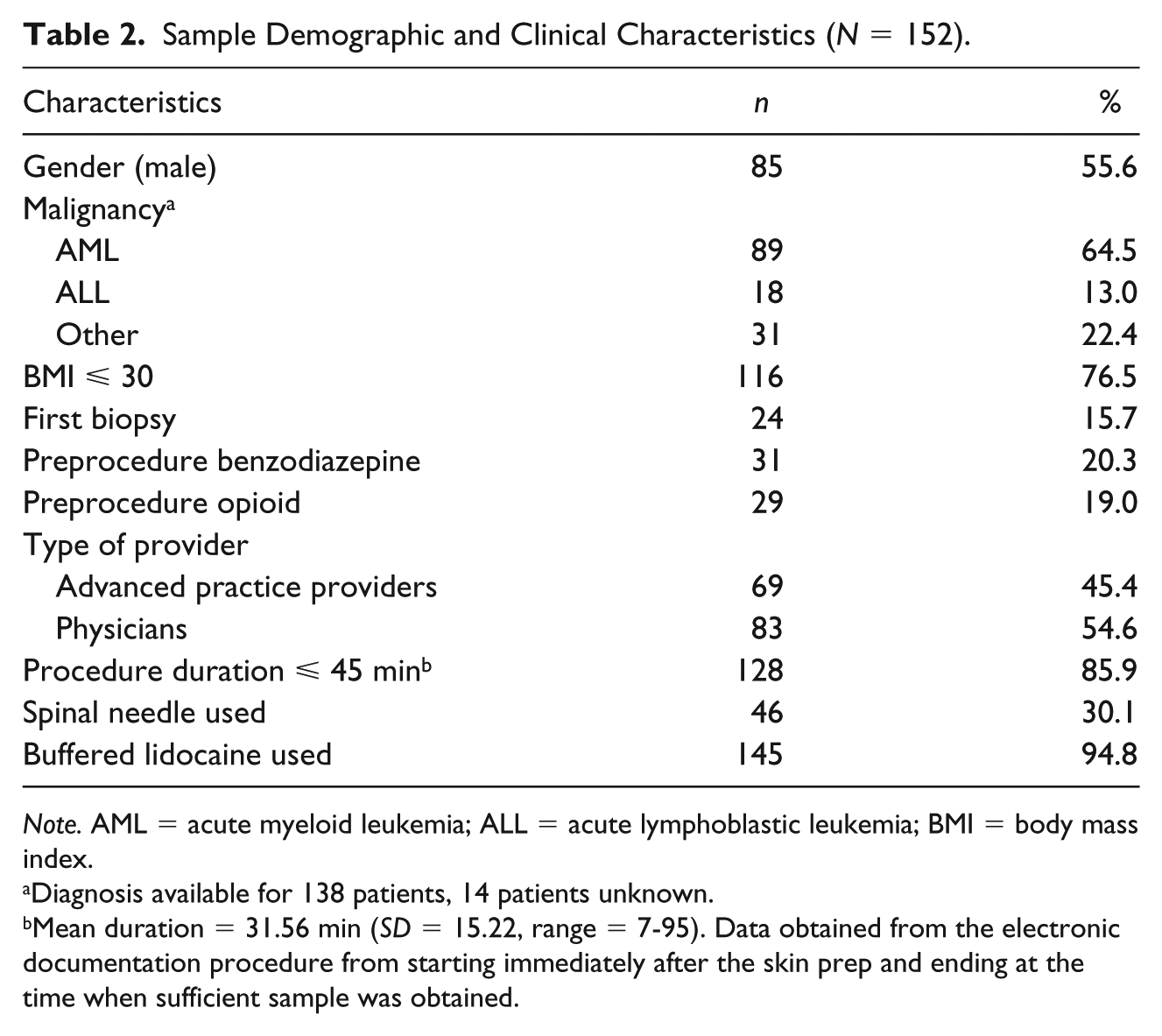
Note. AML = acute myeloid leukemia; ALL = acute lymphoblastic leukemia; BMI = body mass index.
Diagnosis available for 138 patients, 14 patients unknown.
Mean duration = 31.56 min (SD = 15.22, range = 7-95). Data obtained from the electronic documentation procedure from starting immediately after the skin prep and ending at the time when sufficient sample was obtained.
Correlates for Preprocedure Pain, Distress, and Premedication
Mean preprocedure BPI average pain item over the prior 24 hr was 2.68 (SD = 2.96), and 27% (n = 41) reported moderate to severe pain at or above the cutoff point of > 5. Mean preprocedure distress was moderate (M = 3.74, SD = 3.13), and 47% of the sample reported moderate-to-severe distress levels (Table 3). Baseline average pain was modestly and positively associated with BMI (r = .20, p < .05), but was not significantly correlated with age, gender, biopsy status, or malignancy type (all p > .05). Preprocedure pain was moderately correlated with preprocedure distress (r = .31, p < .001). Individuals reporting preprocedure pain below the threshold of 5 (none-mild pain) were less likely to receive an opioid (χ2 = 4.85, p < .05). Seventy-one percent (n = 29) of those with moderate or severe pain (⩾5) prior to the procedure did not receive an opioid. The relationship between pain levels (none or mild compared with moderate or severe) and receipt of a benzodiazepine was not statistically significant.
Pain Severity, Pain Quality and Character, and Distress Over Time.
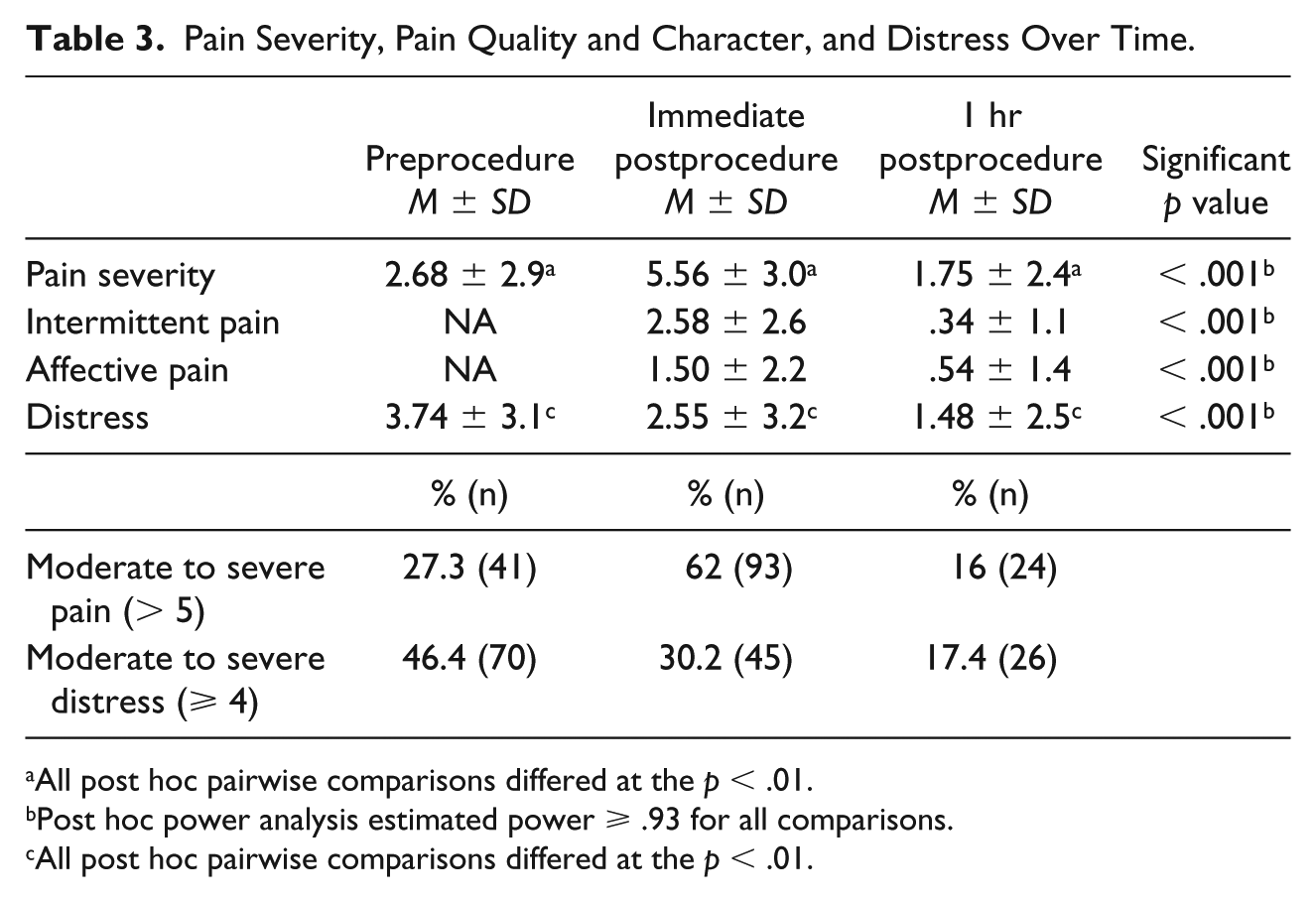
All post hoc pairwise comparisons differed at the p < .01.
Post hoc power analysis estimated power ⩾ .93 for all comparisons.
All post hoc pairwise comparisons differed at the p < .01.
Preprocedure distress levels were significantly higher for those undergoing BMAB for the first time (M = 5.25, SD = 2.16) compared with those who had a prior BMAB (M = 3.47, SD = 3.15, t = 2.60, p < .001). Differences in preprocedure distress between females (M = 4.26, SD = 3.28) and males (M = 3.30, SD = 2.95) approached statistical significance (t = 1.90, p = .06). Preprocedure distress was not significantly associated with BMI or AML (acute myeloid leukemia) versus other malignancies. Individuals who reported a distress level below 4 were less likely to receive a benzodiazepine (χ2 = 8.20, p < .01); however, 70% (n = 49) of those with elevated distress (⩾ 4) did not receive premedication with a benzodiazepine.
Administration of an opioid was not significantly related to age, BMI, malignancy type, first-time biopsy status, or baseline distress. Similarly, no significant relationships were noted between benzodiazepine use and age, BMI, malignancy type, baseline pain, or initial biopsy status. Receipt of a benzodiazepine was associated with female gender (χ2 = 8.34, p < .01).
Correlates for Immediate Postprocedure Distress and Pain Recall
Immediate postprocedure distress recall was mild (M = 2.55, SD = 3.23, t = −5.48, p < .001), although 30% of participants (n = 45) reported a level >4. Postprocedure distress was significantly correlated with preprocedure distress (r = .33 p < .001). Immediate postprocedure distress recall differed significantly by gender (female, M = 3.56, SD = 3.63; male, M = 1.75, SD = 2.64, t = 3.53, p < .001), and administration of a benzodiazepine (M = 4.31, SD = 3.87) versus no benzodiazepine (M = 2.35, SD = 3.17, t = 2.04, p < .05). No other demographic or treatment-related variables were significantly associated with distress.
Mean immediate postprocedure pain intensity recall was moderate (M = 5.56, SD = 3.53) with 62% (n = 94) reporting moderate to severe pain (⩾ 5). Postprocedure pain was associated with preprocedure pain (r = .24, p < .01). Immediate postprocedure pain recall differed significantly by gender with females reporting greater pain (M = 6.24, SD = 3.00) than males (M = 5.21, SD = 3.00, t = 2.51, p < .05). No other demographic or treatment-related variables were significantly associated with postprocedure pain severity. Several procedure-specific variables collected as part of this study were evaluated (Table 2). Duration of procedure, amount of lidocaine, and use of a spinal needle had no influence on postprocedure pain and distress levels.
Correlates for Immediate Postprocedure Pain Quality and Related Symptoms
Table 3 shows the mean scores for the intermittent pain and affective pain dimensions with the SF-MPQ-2, which assessed dimensions of sensory and affective pain experiences. Mean scores for individual word choices were evaluated to better understand painful sensations evoked from BMAB, and only two emerged as moderate in severity (>3), “shooting” and “sharp” at the immediate postprocedure recall. Both decreased considerably from immediately following the procedure to 1 hr after the procedure: “shooting” (M5min = 3.8, SD = 3.7 to M1hr = .48, SD = 1.6) and “sharp” (M5min = 3.6, SD = 3.6 to M1hr = .58, SD = 1.8). Mean scores for all other descriptors remained below a value of 3.
Intermittent pain decreased from immediately after the procedure to 1 hr (M = 2.58, SD = 2.56 vs. M = .34, SD = 1.12, t = 11.28, p < .001) as did affective pain (M = 1.50, SD = 2.44 vs. M = .54, SD = 1.36, t = 5.44, p < .001). Immediate postprocedure affective pain recall was associated with younger age (r = –.18, p < .05) and greater baseline distress (r = .18, p < .05). Affective pain was greater for females (M = 2.03, SD = 2.43) compared with males (M = 1.08, SD = 1.99, t = 2.62, p < .01), and higher for preprocedure benzodiazepine administration (M = 2.37, SD = 2.86) compared with no benzodiazepine (M = 1.28, SD = 2.02, t = 2.39, p < .05). Immediate affective pain recall had no significant associations with BMI, biopsy status, malignancy type, or opioid administration, but was moderately correlated with DT scores (r = .51, p < .001).
Females had greater Intermittent pain recall at 5 min postprocedure (M = 3.04, SD = 2.60) than males (M = 2.20, SD = 2.49, t = 2.01, p < .05). Having a non-AML malignancy was associated with higher intermittent pain (M = 3.22, SD = 2.88) relative to those with a diagnosis of AML (M = 2.11, SD = 2.21, t = 2.67, p < .01). No significant associations were observed with age, BMI, biopsy status, baseline pain or distress, or preprocedure benzodiazepine or opioid administration.
Comparisons of Distress and Pain Over Time by Premedication Use
Distress was analyzed over time as a function of premedication administration to examine medication effects. Table 4 presents mean distress scores over time for the split-plot 3 (time) × 2 (medication) ANOVAs. There was a significant main effect for time from preprocedure to 1 hr postprocedure (F = 34.81, p < .001), and post hoc analyses using Bonferroni corrections revealed significant differences between all three time points (all p values < .01). As well, there was a significant main effect for benzodiazepine administration with those receiving medication reporting greater distress than those who did not (F = 11.28, p < .001). The time-by-medication interaction was significant (F = 4.74, p < .01; Figure 1). Post hoc comparison of between-subject simple effects showed significant differences in distress at both preprocedure and immediate postprocedure recall time points (all p values < .01) with those receiving a benzodiazepine reporting greater distress than those who had not. There was no significant difference in these groups by the 1-hr postprocedure time point. Similar post hoc simple effect comparisons within-subjects demonstrated that those receiving a benzodiazepine had no significant reduction in distress from preprocedure to immediate postprocedure recall. All other comparisons within-groups across time were significantly different (p < .01).
Mean Distress and Pain Scores Over Time by Premedication Administration.
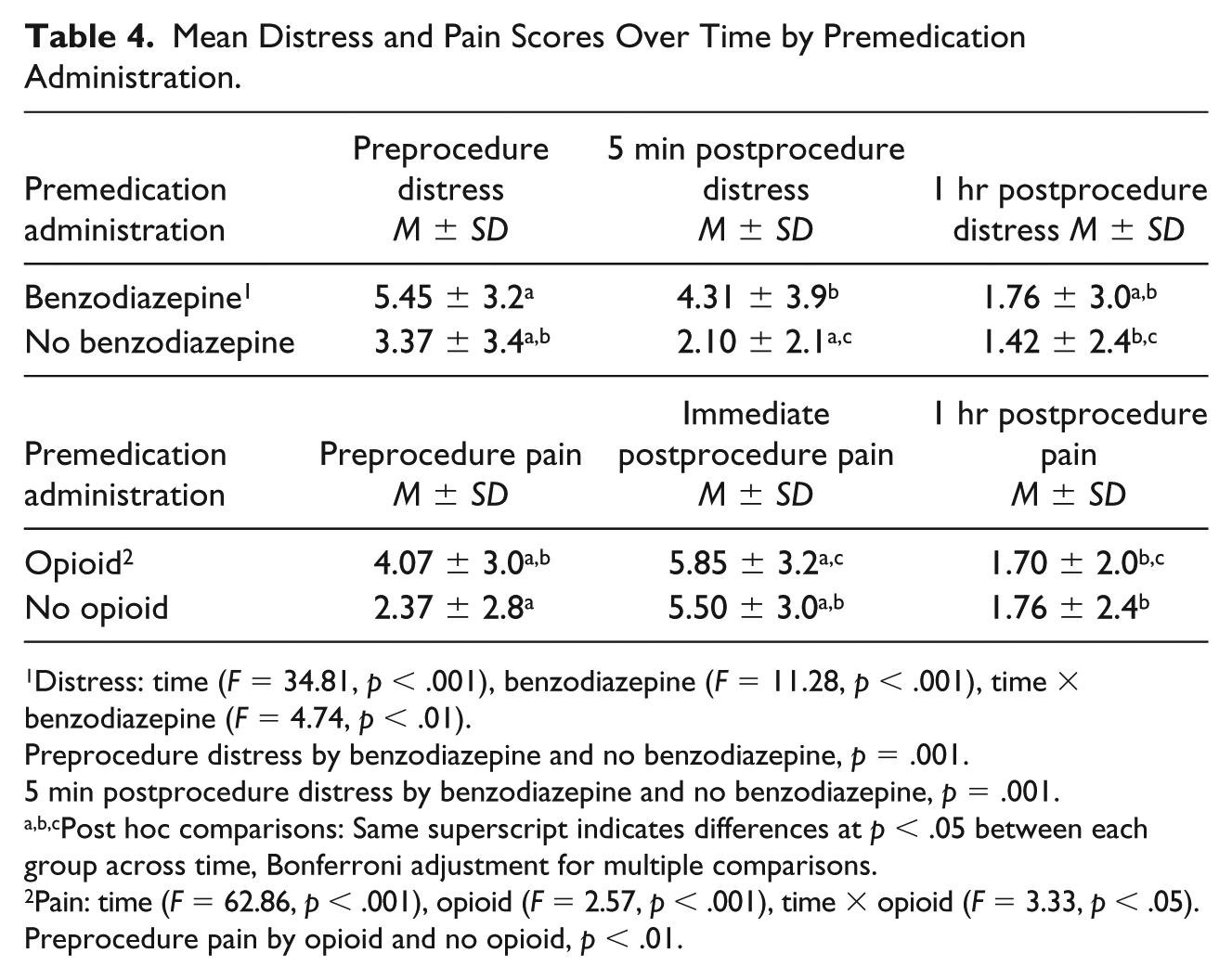
Distress: time (F = 34.81, p < .001), benzodiazepine (F = 11.28, p < .001), time × benzodiazepine (F = 4.74, p < .01).
Preprocedure distress by benzodiazepine and no benzodiazepine, p = .001.
5 min postprocedure distress by benzodiazepine and no benzodiazepine, p = .001.
Post hoc comparisons: Same superscript indicates differences at p < .05 between each group across time, Bonferroni adjustment for multiple comparisons.
Pain: time (F = 62.86, p < .001), opioid (F = 2.57, p < .001), time × opioid (F = 3.33, p < .05).
Preprocedure pain by opioid and no opioid, p < .01.
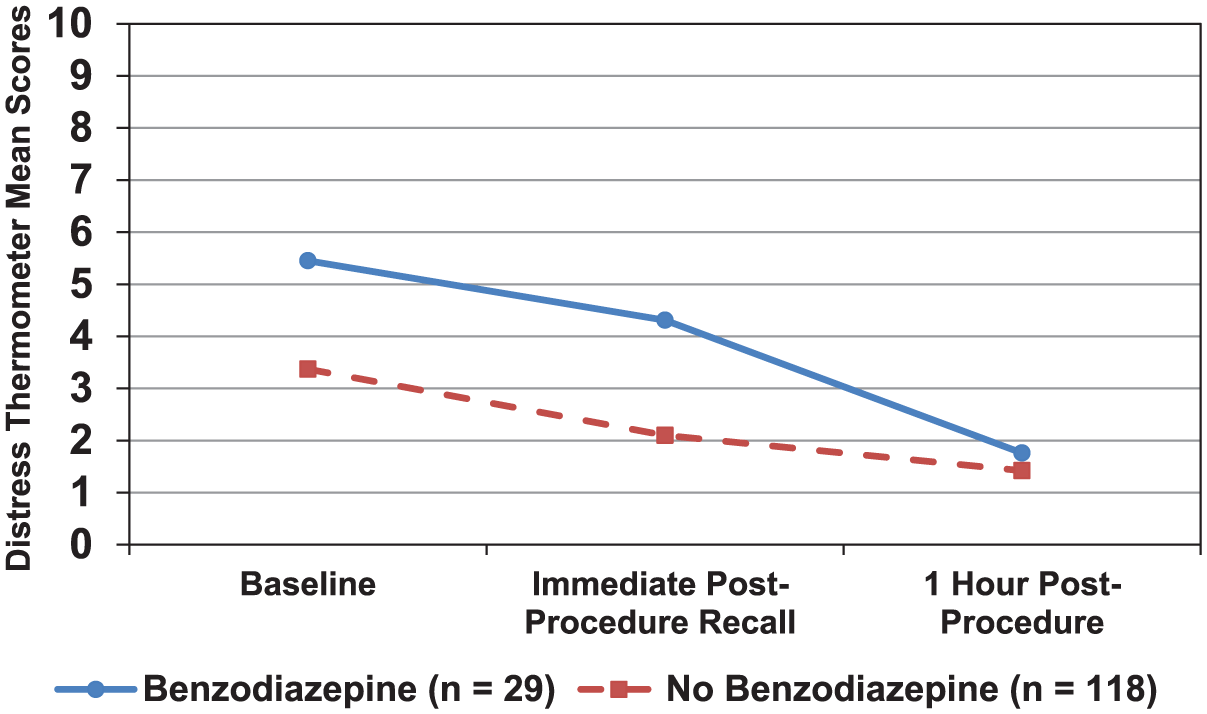
Mean distress scores for patients receiving premedication with a benzodiazepine versus no benzodiazepine over time.
Pain over time as a function of premedication administration was examined. Table 4 presents mean pain scores across time for the split-plot 3 (time) × 2 (medication) ANOVAs. With respect to pain severity, there was a significant main effect for time (F = 62.86, p < .001). Post hoc analyses using Bonferroni corrections revealed significant differences between all time points (all p values < .001) with pain recall increasing during procedure before resolving. There was no significant effect for opioid administration, though the time-by-opioid interaction was significant (F = 3.33, p < .05, Figure 2). Post hoc analyses of this interaction showed that patients who received or did not receive an opioid still experienced greater pain from preprocedure to immediate postprocedure recall that then decreased from immediate postprocedure recall to the 1-hr time point (all p values < .05). Despite the administration of an opioid in those with higher baseline pain (p < .01), there were no statistically significant differences with procedure recall of pain at 1-hr postprocedure.
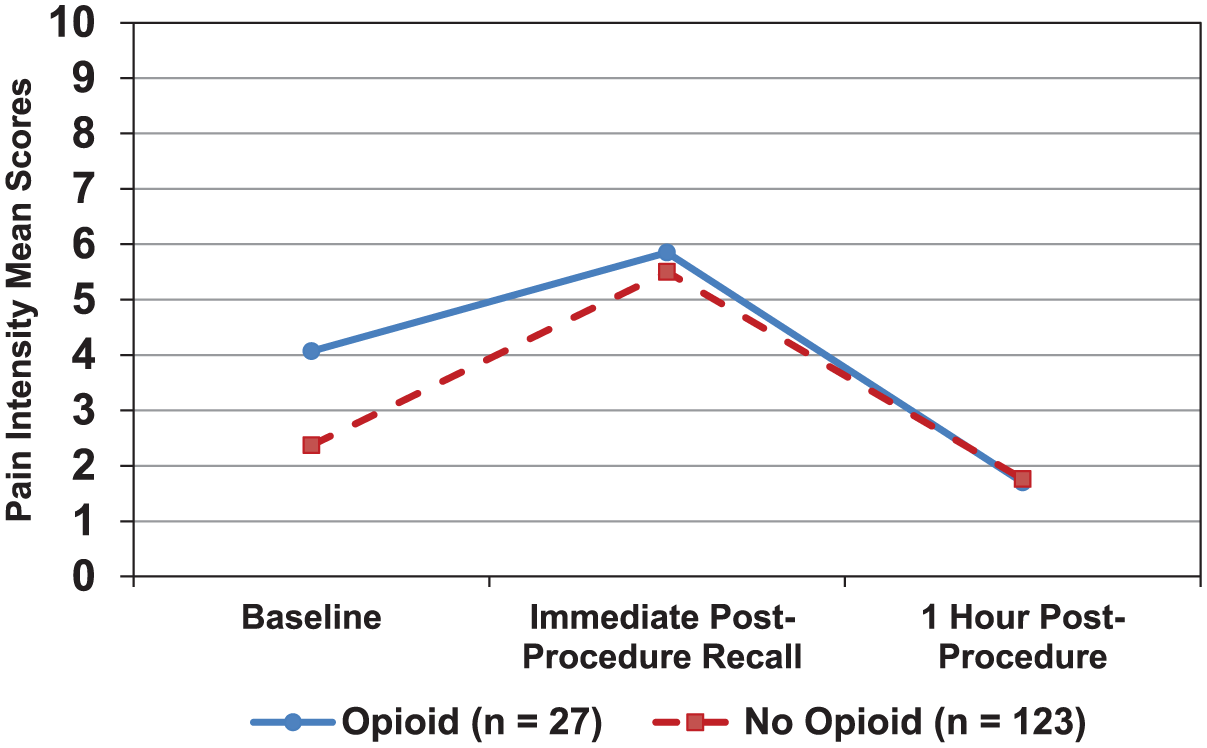
Mean pain scores for patients receiving premedication with an opioid versus no opioid over time.
Multivariate Predictors of Immediate Postprocedure Distress, Pain, and Pain Quality
Hierarchical linear regression of 5-min postprocedure distress immediate recall controlling for baseline distress (R2 = .11, F = 17.95, p < .001) demonstrated that adding the significant predictor of gender (p < .01) and benzodiazepine administration approaching significance (p = .06) improved the model (R2 change = .07, F = 6.44, p = .002; Table 5). There was no significant interaction between gender and benzodiazepine administration. Hierarchical multiple regression of 5-min postprocedure pain recall controlling for baseline pain (R2 = .06, F = 9.83, p < .01) with the addition of predictors, gender, and malignancy type (p values < .05), significantly improved the model (R2 change = .08, F = 6.36, p < .01; Table 6).
Hierarchical Linear Regression Model Parameters for Immediate Postprocedure Recall of Distress.
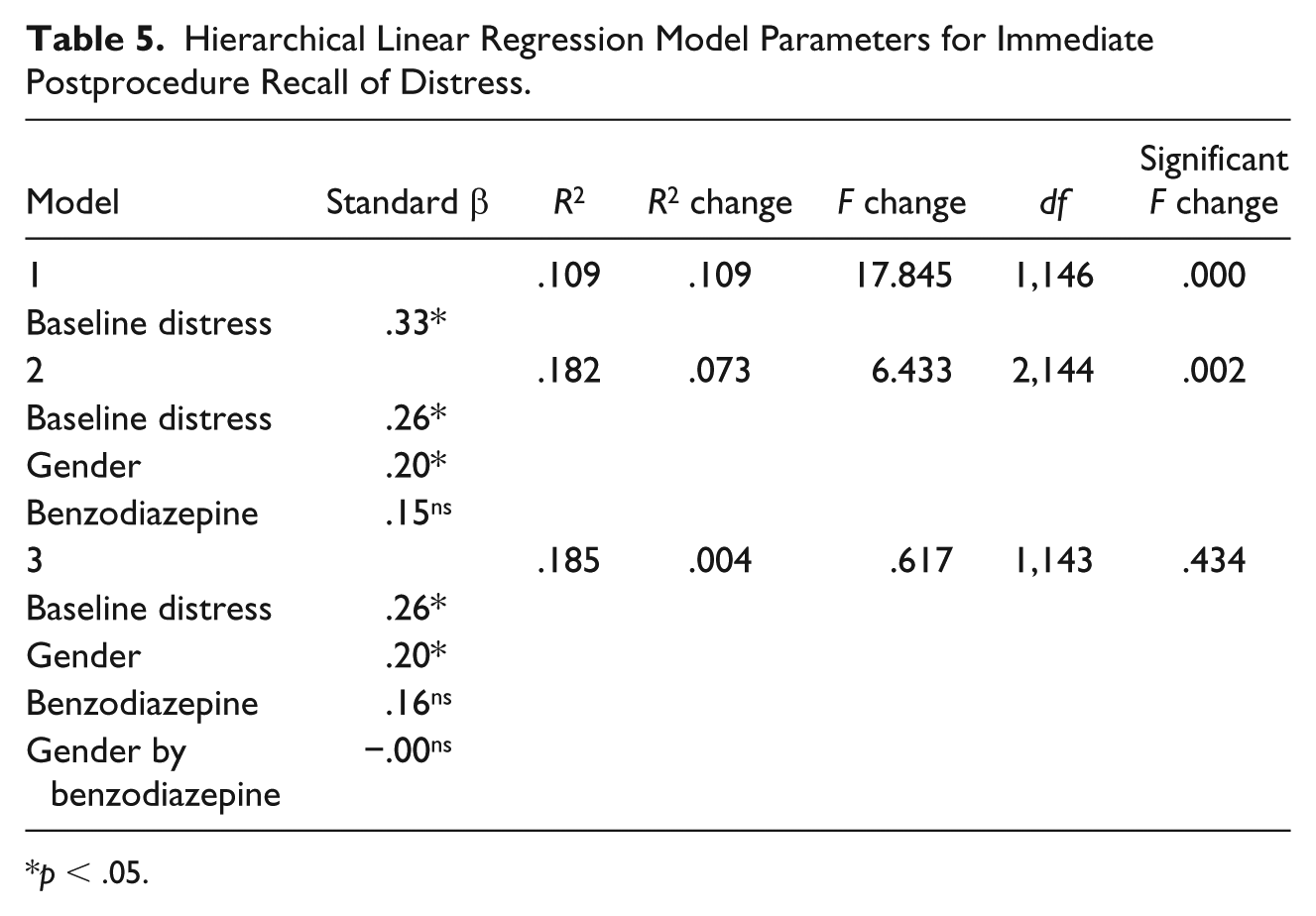
p < .05.
Hierarchical Linear Regression Model Parameters for Immediate Postprocedure Recall for Pain.
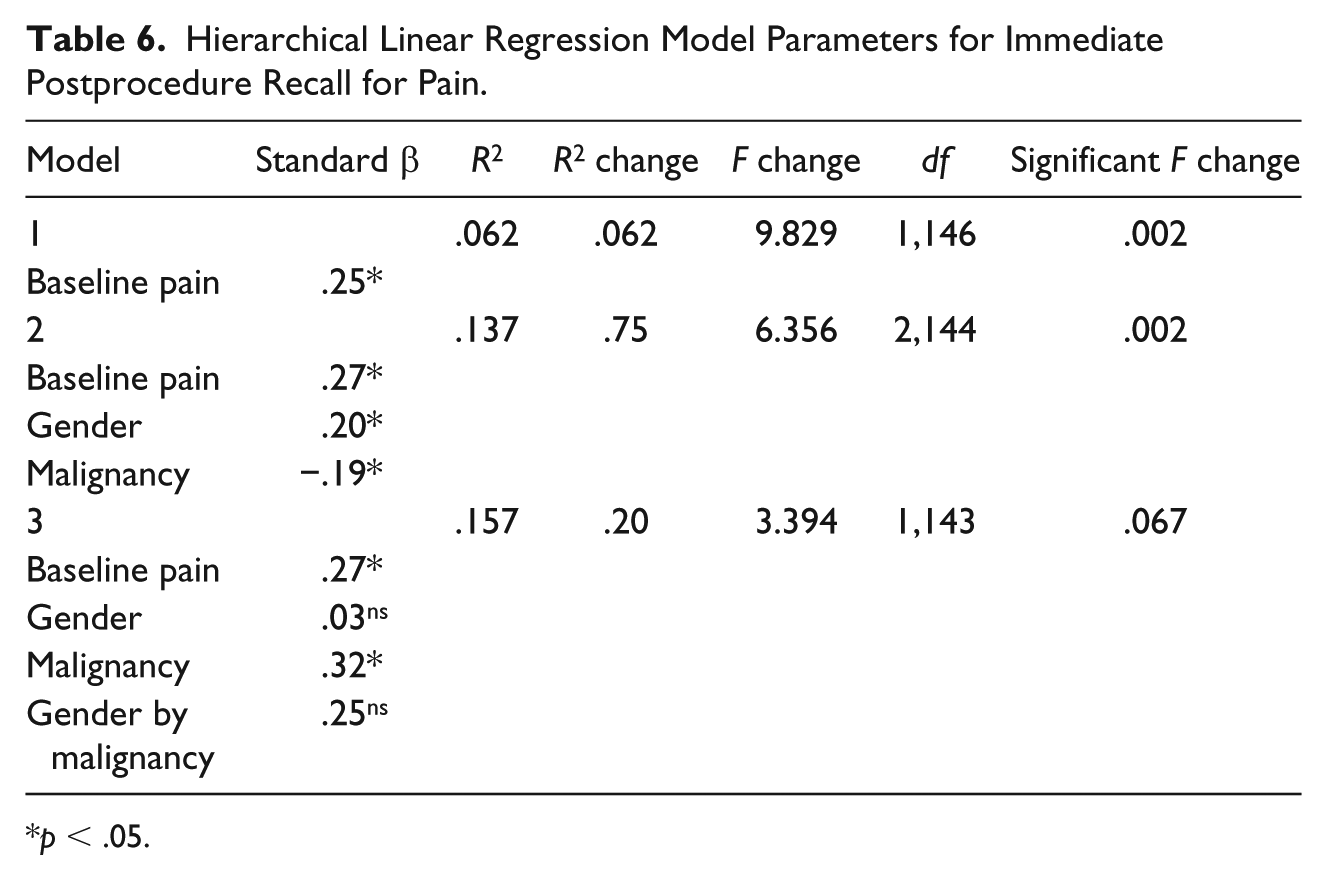
p < .05.
Postprocedure intermittent pain was significantly predicted by gender and having a non-AML malignancy (all p values < .05). Hierarchical multiple regression demonstrated that gender and malignancy type accounted for a significant amount of variance in intermittent pain (R2 = .07, F = 5.63, p < .01) with both gender and malignancy type being significant predictors (p values < .05). Significant predictors for postprocedure affective pain were gender, baseline distress, age, and administration of a benzodiazepine (p values < .05). Hierarchical multiple regression showed that these variables accounted for a significant amount of variance in affective intermittent pain (R2 = .10, F = 4.01, p < .01).
Discussion
This study of 152 adults undergoing BMAB procedures found that BMAB is associated with variable levels of pain and distress. At baseline, 27% (n = 41) of patients were experiencing moderate to severe average pain (⩾5-10) over the past 24 hr, but immediately following the procedure, 62% (n = 93) recalled moderate to severe pain during the procedure and in 41% (n = 62), this pain was severe (⩾ 7). One hour following the procedure, only 16% (n = 24) of patients reported pain ⩾ 5. These findings closely approximate the frequency for moderate to severe pain of 63.7% reported by Portnow et al. (2003), and is similar to estimates from other studies (Lidén et al., 2012; Valebjørg et al., 2014) even for severe pain (Lidén et al., 2009). Cross-study comparisons on patterns and prevalence of BMAB pain must be cautiously interpreted due to the wide variations in preprocedure analgesic and sedation protocols.
Moderate to severe preprocedure distress levels (⩾4) were present in 46% of the sample, and only 30% of these patients received anxiolytic premedication. DT scores did decrease by 32% at the 5-min postprocedure immediate recall and 60% from baseline at 1 hr following the procedure (p < .001). For 39%, this drop might have been attributed to the administration of an opioid or a benzodiazepine, and for others this could have occurred from relief that the procedure was over. Distress encompasses emotions such as worry, nervousness, and fear, (NCCN, 2018), and may be a better indicator for psychological experiences than anxiety alone (Holland et al., 2010). In this hospitalized sample, different from most BMAB studies of outpatients, baseline distress may have been present not only in anticipation of the procedure, but also as a preexisting symptom related to hospitalization or other circumstances. Approximately 30% of patients with cancer receiving supportive care have significant distress (Funk, Cisneros, Williams, Kendall, & Hamann, 2016).
Patterns in mean pain severity ratings differed from mean distress levels in that pain intensity increased from baseline to the postprocedure recall time point, and then diminished at the 1-hr postprocedure time point. Distress levels progressively decreased over time. This spike in pain is consistent with procedure-induced pain. Although all patients received a local anesthetic, this does not mitigate the transient suctionlike pain experienced when obtaining a marrow aspirate or exertion of pressure from the biopsy (Hjortholm et al., 2013). It seems intuitive that health care professionals would appreciate the intense nature of BMAB pain; however, Kuball et al. (2004) documented that 50% of nurses and physicians failed to recognize severe pain in their patients undergoing BMAB. This emphasizes the importance of assessing patients’ pain levels during and after BMAB, and appreciating the need to treat pain.
Our study demonstrates a role for anxiolysis in patients with concerning distress levels; however, patients who received anxiolytics did not experience a therapeutic reduction in distress until 1 hr after the procedure. This raises issues as to whether the timing, route of administration, and pharmacokinetics for preprocedure benzodiazepines were appropriate for patients in this study. Nearly all anxiolytics were given orally requiring time to onset of action. Only 16 of the 45 patients (36%) who had moderate to severe recalled distress (DT scores ⩾ 4) 5 min after the procedure had received a preprocedure benzodiazepine. Twenty-five of these 45 patients (56%) reported distress ⩽ 3 at 1 hr following the procedure. Administration of a shorter-acting agent such as intravenous midazolam might be more advantageous for patients undergoing BMAB, and data from this study and others support the need for more aggressive individualized plans of care to address patients’ anxiety and/or distress associated with BMAB. Giannoutsos, Grech, Maboreke, and Morgenstern (2004) showed in their post-BMAB survey of 112 patients that those who received a sedating agent, not only experienced less pain, but also expressed less apprehension if faced with another BMAB procedure.
Consonant with findings from Kuball et al. (2004), our prediction models identified females at greater risk of pain. Being female was also a risk of experiencing distress, and others noted the same for anxiety (Tanasale et al., 2013). Type of malignancy, other hematological malignancies (e.g., ALL, acute lymphoblastic leukemia, and multiple myeloma), or solid tumors also predicted increased pain scores. Our findings did not show a significant association for first time BMAB and pain, although a significantly higher mean preprocedure distress level was observed in patients having BMAB for the first time. We did not find a significant effect on postprocedure pain and distress with prior BMAB. For 88% of the 89 patients with AML and 73% of the 48 patients diagnosed with other malignancies, this was not their first BMAB. Tanasale et al. (2013) found no influence on pain and anxiety from prior BMAB procedures. On the contrary, Johnson, Burke, Plews, Newell, & Parapia, (2008) who conducted a randomized controlled trial (RCT) with 48 patients found that regardless of the intervention (placebo vs. nitrous oxide), those having past BMAB procedures had increased pain. Degen et al. (2010) surveyed 412 patients about their most recent and prior BMAB experiences noting that unbearable pain with previous BMAB predicted a similar outcome. Because we only collected information on whether patients had a previous BMAB, we were unable to ascertain the impact of past pain severity on current BMAB pain. We did not find any association of BMI with pain and distress, and others corroborated that BMI was unrelated to pain from BMAB (Degen et al., 2010; Kuball et al., 2004; Vanhelleputte et al., 2003).
Our analyses did not reveal significant associations between procedure-specific variables (e.g., total duration of the procedure, use of spinal needles, and type of provider) and pain and distress. Some noted that shorter needle insertion and bone marrow extraction times, and BMAB performed by more experienced providers can lead to less pain (Kuball et al., 2004), yet others found that years of experience had no bearing on BMAB pain (Tanasale et al. (2013). Although we did not collect information on providers’ years of experience performing BMAB, all providers (e.g., physicians vs. advanced practice providers) were credentialed to independently perform BMAB.
Higher immediate postprocedure recall of affective pain measured by the MPQ-SF-2 was associated with younger age, greater baseline distress, being female, and receiving a preprocedure benzodiazepine. These results underscore the importance of measuring the emotional aspects of the BMAB experience.
Despite the fact that pain and anxiety are common experiences with BMAB procedures, a limited number of studies demonstrate the effectiveness of protocols to manage these symptoms. Interventions such as the administration of analgesics (e.g., systemic opioids and local anesthetics), anxiolytics, and less often inhaled nitrous oxide have been tested in various combinations (Chakupurakal et al., 2008). One RCT showed that pretreatment with tramadol significantly reduced the percentage of patients with moderate to severe pain associated with BMAB compared with placebo (p = .029; Vanhelleputte et al., 2003). Another RCT found no significant effects on pain for two different strengths (200 µg and 100 µg) of sublingual fentanyl to placebo (Kuivalainen et al., 2013). A combination of a local anesthetic with titration of midazolam (5–10 mg), a benzodiazepine and sedative hypnotic, proved more effective in providing a more comfortable experience (p < .01), and improved pain relief (p = .01) compared with inhaled nitrous gas alone in 46 patients undergoing BMAB (Chakupurakal et al., 2008). In a descriptive study of 22 patients previously given midazolam for BMAB and all receiving nitrous oxide and oxygen in a 50/50% mixture, (Entonox®), 94% of patients rated Entonox® either better or equal to midazolam in decreasing pain (Gudgin, Besser, & Craig, 2008). Steedman et al. (2006) in their RCT also documented better pain control with Entonox® and local anesthetic as well as patient preference for this therapy compared with local anesthetic alone. Nitrous oxide 50%/oxygen 50% resulted in significantly less pain for men compared with women (Johnson et al., 2008). Varying doses and routes of lorazepam, a benzodiazepine, have shown some therapeutic amnestic benefit for procedure recall, which can lead to a greater willingness of patients to undergo the procedure again in the future (Milligan, Howard, & Judd, 1987; Park et al., 2008).
The effects of combinations of anxiolytics and opioids have been studied, but no definitive conclusions can be drawn as to the best regimens for controlling both pain and anxiety with BMAB (Hjortholm et al., 2013; Talamo, Liao, Bayerl, Claxton, & Zangari, 2010; Wolanskyj et al., 2000). Some investigators documented that an oral opioid and benzodiazepine not only reduced recall, but lessened pain with BMAB (Dunlop, Deen, Lind, Voyle, & Prichard, 1999). Others detected no statistical differences in pain, anxiety, or distress between a placebo arm and oral hydromorphone and lorazepam treatment arm (Wolanskyj et al., 2000) or a meaningful difference in pain and anxiety with oral oxycodone and lorazepam (Talamo et al., 2010). To date, inconclusive data as to the best pre- and intratreatment protocols for pain and anxiety reduction with BMAB have led to wide variations in practice. Regardless, the use of a preprocedure local anesthetic remains the mainstay for the management of pain.
Advances in procedure technology such as powered devices have been associated with less pain compared with the traditional manual needling approach (Miller et al., 2011). The benefits of nondrug measures for reducing pain, anxiety, and distress should not be underestimated. Even the simplest, safe, and inexpensive strategies, such as providing information support prior to BMAB (Degen et al., 2010), encouraging patients to listen to music during the procedure (Shabanloei, Golchin, Esfahani, Dolatkhah, & Rasoulian, 2010), delivering structured music interventions (Danhauer, Vishnevsky, & Campbell, 2010; Yinger & Gooding, 2015), and using distraction (Hjortholm et al., 2013) can have positive effects in decreasing procedure-related pain, anxiety, and distress. Modifying environments with nature scenes and sounds, while having no significant effect on pain and anxiety with BMAB, was associated with a trend toward higher satisfaction with the experience (Lechtzin et al., 2010). More time-intensive behavioral and psychological interventions have demonstrated efficacy with needle-related procedure pain and distress. A systematic review documented that the largest treatment effect sizes were observed with distraction, combined cognitive–behavioral interventions, and hypnosis (Uman, Chambers, McGrath, & Kisely, 2008). Combinations of pharmacological and nonpharmacological interventions should at least be considered for those at risk of reporting higher levels of pain and anxiety prior to the procedure (Lord & Bhuller, 2012).
Limitations
Although all patients in this study had BMAB with local anesthetic, investigators did not control preprocedure administration of opioids or benzodiazepines. The drug, route of administration, and time-to-effect were not taken into account in the statistical modeling for those receiving premedication. Given this limitation, variations in practice do make study findings more generalizable to settings without standard BMAB premedication protocols. Variations in practice, however, may have hampered the ability to identify significant predictors of pain and distress. We measured distress and not anxiety as studies had, and therefore, lacked comparator data to interpret our results. A strength of this study was the inclusion of hospitalized patients as the majority of studies on BMAB pain and anxiety primarily focus on outpatient populations. However, by studying hospitalized patients, this may have affected distress levels as patients might have been likely to encounter the stress of more aggressive therapies, changes in health status, separation from family and home environments, and possibly greater financial concerns. Finally, data were not collected on other potential complicating factors (e.g., insufficient aspirates, difficult insertions, or re-entry or needling) that can also contribute to pain and distress.
Conclusion
Although several studies describe pain severity and anxiety with BMAB, our study uniquely evaluated pain quality, related symptoms, and distress. Similar to other studies, we documented a high percentage of patients undergoing BMAB with moderate to severe pain and a somewhat lower percentage for moderate to severe distress. Postprocedure distress was associated with preprocedure distress, which emphasizes the need to evaluate existing distress. Unlike anxiety, distress encompasses psychological, behavioral, social, spiritual, and/or physical experiences. Moreover, distress is common among persons with cancer and is easily measured in routine clinical practice using the DT. Screening patients for higher preprocedure distress can be useful in determining the need for sedation. We also observed that females were at greater risk of pain and distress, and affective pain was higher for females. Potential gender differences in responses to BMAB should be considered when planning interventions for BMAB pain and distress. Participants in our study reported greater severity for “shooting” and “sharp” pain sensations from BMAB. Local anesthetic alone does not prevent the transient and intense pain from aspiration of bone marrow (Hjortholm et al., 2013). Our results indicate that premedication with an oral opioid or benzodiazepine may not be adequate if the timing and dosing are not optimal to achieve acceptable analgesia and sedation.
Conflicting data do exist to explain factors that contribute to pain and anxiety from BMAB. Additional studies are still needed using standard multivariable patient-reported and clinical outcomes to identify significant predictors that place patients at high risk for poorer outcomes. Future research should focus on designing and testing treatment protocols and clinical decision support tools to help clinicians make informed judgments as to optimal ways to manage pain, anxiety, and distress in patients undergoing BMAB.
Relevance to Practice
BMAB procedures are often performed within a provider-centric culture with decisions to forego systemic premedication often influenced by the need to promote workflow efficiency, limit recovery time, and decrease additional patient care demands (e.g., monitoring). Analgesics and sedating agents have adverse effects such as unintended advancing sedation and respiratory depression, which may make clinicians reluctant to optimize premedication therapy due to concerns regarding patient safety. This study demonstrated that single analgesic or oral benzodiazepine agent or no systemic premedication at all is associated with concerning levels of pain and distress. Nurses should advocate for optimal premedication regimens and nondrug measures, and assess and document the magnitude of pain, anxiety, and distress with BMAB. The implementation of evidence-based guidelines, especially the NCCN guidelines for assessing and managing distress, can lead to greater awareness of patient experiences and support clinical decision-making to improve patient outcomes (Fulcher & Gosselin-Acomb, 2007).
Footnotes
Acknowledgements
The authors wish to thank Christine Fearn, BSN, RN, Carrie Marvill, MSN, RN, AOCNS, and Kristen Bink, MSN, RN, AGCNS-BC, for their support of this research.
Author Contributions
All authors made substantial contribution to the article and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Contributions are specified: Concept and design were contributed by A.E.M., R.L.T., R.S.C., and R.C.P; acquisition of data by A.E.M.; analysis and interpretation of data by A.E.M., R.L.T., S.C.P., R.S.C., and R.C.P. The article was drafted or revised critically for important intellectual content by the authors A.E.M., R.L.T., S.C.P., R.S.C., and R.C.P. Finally, A.E.M., R.L.T., S.C.P., R.S.C., and R.C.P. approved the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a research grant from the DAISY Foundation, Glen Ellen, CA 95442 awarded to Amy E. Moore.