
Abstract
Providing effective screening tools to nurses is necessary to improve patient outcomes and health care quality. This research examines if the modification of two electronic health record sepsis screening tools using a combined systemic inflammatory response syndrome (SIRS), modified early warning score (MEWS), and national early warning score (NEWS) criteria improves the recognition of sepsis by nurses. Medical-surgical/telemetry units at a medical center in the Midwest were examined using a quasiexperimental design. Modifications of tool 1 captured 18% more correct classifications of sepsis (odds ratio [OR] = .82, 95% CI = [0.68, 0.98]), triggering for 10% fewer patients, t(1033) = 9.31, p < .001. 95% CI = [0.078, 0.119]. Modifications of tool 2 captured 3 times more correct alerts (OR = .29, 95% CI = [0.24, 0.35]), triggering for 46% fewer patients, t(1033) = 24.38, p < .001. 95% CI = [0.420, 0.493]. The updated criteria showed significant improvement toward correctly identifying sepsis and presents the opportunity to develop an effective tool that balances sensitivity with specificity.
Introduction and Background
The health care landscape is constantly changing with demands to improve the quality, efficiency, and effectiveness of care provided to patients. Registered nurses (RN) comprise the largest segment of the health care workforce, and are recognized leaders in improving quality (Dunton, Gajewski, Klaus, & Pierson, 2007). Sepsis and septic shock remain the two most common and costly diagnoses in the hospital, and are significant contributors to overall patient morbidity and mortality (Sjoding & Hyzy, 2017). With an aging population, and greater demands on health care professionals, providing a more effective electronic screening tool to assist RNs in recognizing patients at risk of or deteriorating from sepsis and septic shock is foremost in preventing increased patient mortality.
Sepsis and septic shock have been identified as both high volume and high cost complications of hospitalization, often requiring stays in intensive care units (ICU) and/or resulting in death (Lehman & Thiessen, 2015; National Quality Forum [NQF], 2012). According to the Agency for Healthcare Research and Quality (AHRQ) sepsis was the sixth most common primary reason for hospitalization in 2009 (NQF, 2012). Kadri et al. (2017) examined patients based on clinical criteria of sepsis and septic shock over a 10-year period, and discovered increased sepsis incidence from 12.8 to 18.6 cases per 1,000 hospitalizations. Between the years 2004 and 2009, hospital stays as a result of sepsis had an annual increase of approximately 13% (Gaieski, Edwards, Kallan, & Carr, 2013). Rhee et al. (2017) found that incidence of sepsis did not meaningfully change from 2009 to 2014.
Estimates place mortality rates from sepsis and septic shock between 14.7% and 29.9% with an estimated 229,044 related deaths in 2009 (Gaieski et al., 2013; Lehman & Thiessen, 2015). Mortality from septic shock remains high, with an approximate rate of 50.7% in 2014 (Kadri et al., 2017). Rhee et al. (2017) found that in-hospital mortality decreased, but overall death or discharge to hospice did not have a statistically significant change from 2009 to 2014. This places sepsis and septic shock as the third most common cause of death in the United States behind heart disease and cancer, and a factor in one to every two to three hospital deaths (Gaieski et al., 2013; Lehman & Thiessen, 2015; Liu et al., 2014). Treating sepsis and septic shock cost the United States health care system an estimated US$20.3 billion to US$24.3 billion from 2007 to 2011 (Gaieski et al., 2013; Lehman & Thiessen, 2015).
The importance of early identification of sepsis signs and symptoms is recognized in the literature, and nurses are identified as the leaders in this effort (Bruce, Maiden, Fedullo, & Kim, 2015; Bushnell, Demaray, & Jaco, 2014; Kleinpell, Aitken, & Schorr, 2013). Vital signs serve as the first indication of sepsis and septic shock, which is a process that typically falls under the purview of the RN (Bushnell et al., 2014; Capuzzo et al., 2012). Therefore, RNs are identified as the first line of defense for recognizing sepsis and septic shock, placing them in a key position to initiate the early, goal-identified treatment required to reduce sepsis-related mortality (Kleinpell et al., 2013). Bushnell et al. (2014) determined that educating nurses regarding early detection of sepsis decreased mortality by 30%.
The Society of Critical Care Medicine’s (SCCM; 2015) “Surviving Sepsis Campaign” bundle recommends measuring lactate levels, drawing blood cultures, and administering a broad-spectrum antibiotic within 1 hr of presentation of sepsis or septic shock, crystalloid at 30 mL/kg for hypotension within the first 3 hr, and vasopressors for hypotension that does respond to the initial fluid resuscitation by the 6-hr mark (Dellinger et al., 2012). The implementation of nurse-driven sepsis recognition and protocols improves compliance with certain aspects of the “Surviving Sepsis Campaign” bundle (Bruce et al., 2015; Society of Critcal Care Medicine (SCCM), 2015; Tromp et al., 2010).
In a quality improvement project on medical–surgical units, implementing a sepsis screening tool and nurse-driven protocol for drawing lactate levels based on a positive screening reduced mortality by 30% (Bushnell et al., 2014). It was found that providing education and using a multidisciplinary approach with nurse-activated sepsis screening protocols decreases mortality because of the time-sensitive nature of the interventions (Bushnell et al., 2014). Sharpe (2015) describes a screening and testing tool developed by bedside RNs to identify sepsis outside of the ICU and emergency department (ED) that helped reduce sepsis mortality by 64% at a single medical center. When implemented across other hospitals in the same health system, there was a 47% drop in sepsis mortality (Sharpe, 2015).
Bone et al. (1992) define sepsis as “the systemic inflammatory response to infection” (SIRS; p. 1644). It is defined as having one or more of four key characteristics: a temperature greater than 38°C or less than 36°C, heart rate greater than 90 beats per minute, a respiratory rate greater than 20 breaths per minute or hyperventilation with a PaCO2 less than 32 mmHg, and an alteration in white blood cells (WBC) with a count greater than 12,000/cu mm, less than 4,000/cu mm, or greater than 10% immature neutrophils (Bone et al., 1992). The definition is further broken down into two additional categories, severe sepsis and septic shock, which are determined by changes in vital signs, laboratory values, hypoperfusion, and organ dysfunction (Matot & Sprung, 2001).
An international coalition updated the definitions of sepsis and septic shock in 2016 (Singer et al., 2016). With no defined pathology or definitive test for sepsis diagnosis, a series of descriptions and clinical criteria serve as the updated definitions for sepsis and septic shock (Singer et al., 2016). Sepsis is separated from infection by an abnormal or life-threatening condition that occurs when the body responds to an infection by injuring its own tissues and organs (Singer et al., 2016). The clinical criteria for sepsis has been updated to reflect a sequential organ failure assessment (SOFA) score. This score is based upon physiological measures and laboratory values.
The Institute for Healthcare Improvement (IHI) found that developing a highly reliable process using modified early warning score (MEWS) screening augmented patient monitoring and improved sepsis recognition and escalation to providers (Doerfler et al., 2015). Roney et al. (2015) identify that many early warning scoring systems and clinical tools have been adopted to detect hospitalized patients at risk of clinical decompensation. First validated in 2001, Subbe, Kruger, Rutherford, and Gemmel developed a simple scoring system for RNs to identify patients at risk for decompensation. The MEWS scoring tool examines five physiological parameters: systolic blood pressure, pulse rate, respiratory rate, temperature, and mental status (alert, reacting to voice, reacting to pain, unresponsive; Subbe, Kruger, Rutherford, & Gemmel, 2001).
Burch, Tarr, and Morroni (2008) found that the proportion of patients who died in the hospital increased as the MEWS score increased. Patients who had a score of 3 to 4 had a 59% increased risk of mortality, and those with a score greater than five had a 79% increased risk of mortality (Burch et al., 2008). Cei, Bartolomei, and Mumoli (2009) measured composite mortality, transfer to a higher level of care, and length of stay for patients on a general medical-surgical floor. Patients with a MEWS of 3 to 4 had a 22.5% to 31.8% increased risk of death compared with patients who had a MEWS of 0 (Cei et al., 2009). Patients who had a MEWS greater than 5 had 40% greater risk of death than patients who had a MEWS of 0 (Cei et al., 2009).
In 2010, as part of a national effort to better predict overall patient deterioration, the Acute Medicine Task Force of the Royal College of Physicians and the National Health System (NHS) in England maximized Vital-PAC Early Warning Score (ViEWS) to predict in-hospital death within 24 hr of vital sign data collection (Smith, Prytherch, Meredith, Schmidt, & Featherstone, 2013). The national early warning score (NEWS) stems from that evaluation and has been applied to other clinical outcomes such as cardiac arrest, and unanticipated ICU admission (Smith et al., 2013). NEWS, in addition to the physiological criteria utilized by MEWS, incorporates supplemental oxygen and peripheral capillary oxygen saturation (SpO2) measurements as part of the early warning criteria (Smith et al., 2013).
Because of the positive predictive value of the NEWS scores to detect clinical deterioration, it was recommended that the NHS adopt this tool in conjunction with other efforts to assist in the detection of clinical deterioration of patients (Smith et al., 2013). Brabrand et al. (2017) evaluated six different early warning scores—including NEWS—in an effort to validate the ability of these scores to determine patients at increased risk of mortality. NEWS succeeded in predicting good outcomes but did not have perfect discrimination or calibration (Brabrand et al., 2017). Although not specifically designed for sepsis screening, both MEWS and NEWS are adept at identifying patients who demonstrate signs of clinical deterioration (Brabrand et al., 2017; Smith et al., 2013).
Sepsis is a high cost, high resource illness that increases length of stay for affected patients. There is consensus in the literature that rapid recognition of patient deterioration is a hallmark of improved patient outcomes and survival rates. To improve the recognition and time for treatment of patients who receive a diagnosis of sepsis, a sensitive, specific, and easy to understand tool needs to be available within the electronic health record (EHR) for RNs at the bedside. A tool, which is overly sensitive, places a burden upon the RNs and has the potential to overlook patients who would benefit from early intervention. It is imperative to provide bedside RNs with a more targeted and functional sepsis screening tool to assess for early intervention and decrease the time to treatment.
The current tools used by the research institution fire off two different levels of criteria. The first tool (yellow warning) triggers based on 30 criteria that combine physiologic and laboratory values based on systemic inflammatory response syndrome (SIRS) criteria (Table 1). The second (red warning) triggers off 11 more serious physiologic criteria and laboratory values (Table 1) based on the original septic shock definition as described by Bone et al (1992). When the EHR detects changes in these measurements within the last 8 hr to 14 hr, two different pop-up windows (yellow and red) are triggered for the RN depending on the severity of the change in vital sign measurements as part of a best practice advisory (BPA). Due to the large number of criteria that trigger an alert, the BPA creates alarm fatigue and confusion for the RN.
Summary of Current Vital Signs and Modifications.
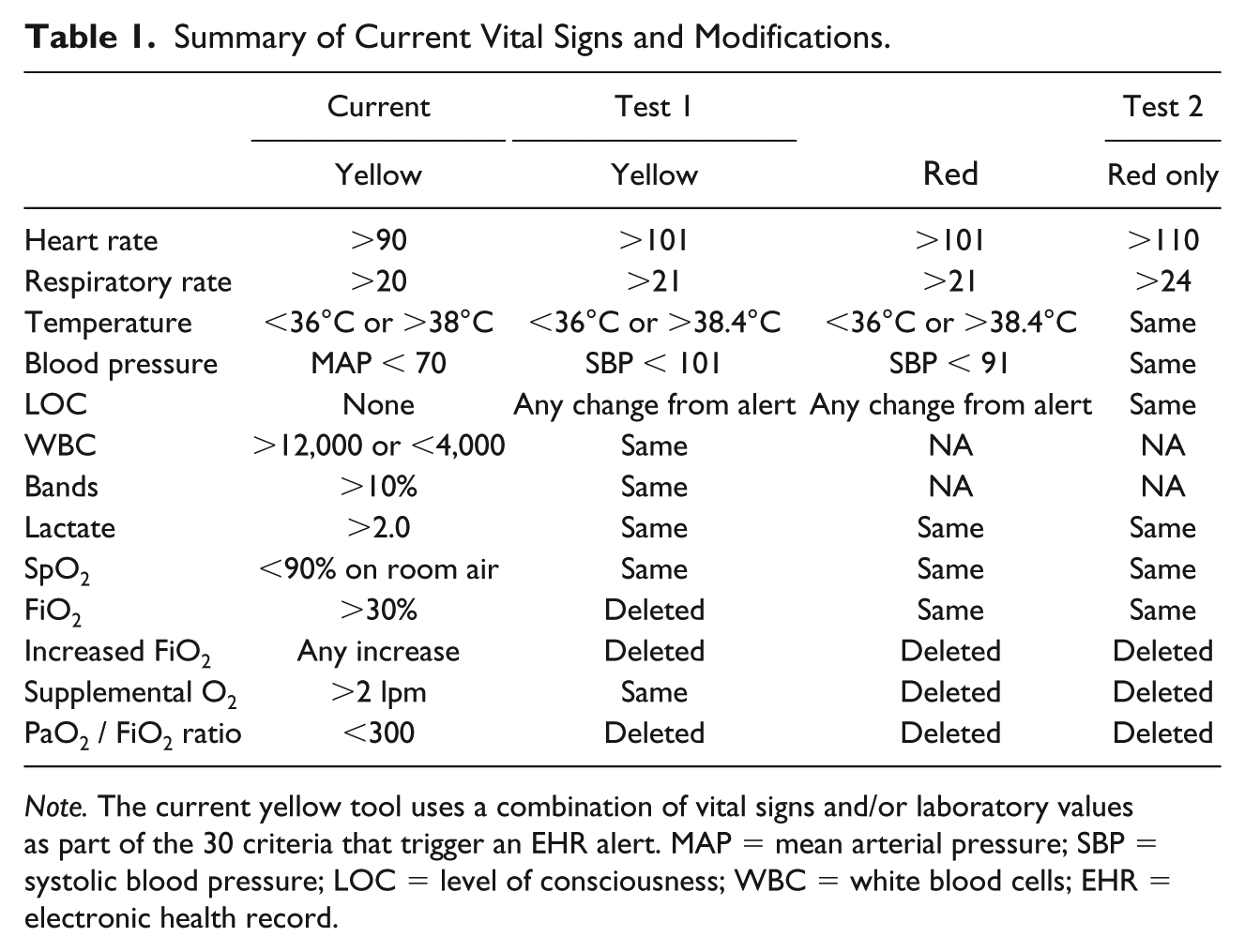
Note. The current yellow tool uses a combination of vital signs and/or laboratory values as part of the 30 criteria that trigger an EHR alert. MAP = mean arterial pressure; SBP = systolic blood pressure; LOC = level of consciousness; WBC = white blood cells; EHR = electronic health record.
Purpose
The purpose of this quality improvement project was to determine if the modification of a sepsis and septic shock screening tool improves the recognition of sepsis and early detection of patient deterioration. The modified screening tool combined (a) systemic inflammatory response syndrome, (b) MEWS, and (c) national early warning score criteria.
Method
The research examined all patients above the age of 18 years admitted during the 2-week data-gathering period to any one of the medical-surgical and telemetry/progressive care units at a tertiary, academic, Magnet-designated institution in the Midwest. Due to the broad epidemiology of sepsis, no particular patient characteristics were queried, with admission to the hospital being the primary inclusion criteria. Excluded from the sample were patients admitted with a suspected diagnosis of sepsis or septic shock, ICU patients, ED patients, and patients admitted on the bone marrow transplant (BMT) unit, the inpatient psychiatric unit, and the obstetrics/labor and delivery unit. For the purpose of this project, ICUs and the ED were excluded from the data collection process because of the specialized patient populations they serve, and various patient factors that exclude RNs from implementing the current sepsis protocol. BMT and obstetrics/labor and delivery were excluded due to ongoing quality improvement projects using unit-specific screening tools based on their specialized patient population. The inpatient psychiatric unit was excluded because the patients are not screened for sepsis as part of the routine workflow.
A quasiexperimental design was used to compare sepsis screening tool firing incidences for patients over a 2-week period. All modifications were tested on an inactive portion of the sepsis warning system within the EHR, which provided the opportunity to and measure occurrences in real time against the RN tool in current use. No changes were made to the active RN sepsis screening tool. Each of these platforms has two different warnings; a yellow warning indicating sepsis and a red warning indicating septic shock. Modifications were made to both the yellow and red sepsis screening tools within the inactive platform.
The sepsis screening tool relies on direct measurement methods of vital sign data. Primary vital sign data are entered by RNs and nursing assistants (NAs) into the EHR of the institution and incorporated into the sepsis screening tool. The screening tool triggers based on this vital sign data and laboratory values examined over the last 8 hr to 14 hr. A key portion of the RN screening tool requires a patient to have both signs and symptoms of infection as well as a positive response for risk of infection. During this study, the “risk for infection” question was removed, requiring a positive response in the “signs and symptoms” of infection category to trigger a firing—consistent with SIRS definitions indicating an infectious source.
During the first round of data collection, changes were made to the inactive platform with vital sign definitions consistent with a MEWS/NEWS score of 3 to 4. The respiratory rate trigger was raised to greater than 21, heart rate greater than 101, and temperature greater than 38.4. A neurological level of consciousness category was included, and any choice that was not “alert” became part of the test criteria. The yellow warning criteria was changed from a mean arterial pressure (MAP) less than 70 value to a systolic blood pressure (SBP) less than 101, and the red warning changed to an SBP < 91 (Table 1). Lactate values, WBC count, and measures of bands were maintained consistent with SIRS criteria. Other oxygen demand criteria as well as combined physiologic and laboratory values were deleted from both warnings because they were inconsistent with MEWS/NEWS theory (Table 1).
During the second 2-week round of data collection, all of the vital sign and laboratory value changes made during the first data set were maintained, and additional modifications were made to the yellow warning criteria in attempts to move toward a single screening measure rather than the two-tier system currently in use. The heart rate was changed to greater than 110, and the respiratory rate to greater than 24 (Table 1). Two additional lines of lab value criteria were also removed in an attempt to improve specificity.
Initial data were extracted from the EHR of the institution based on a report created by the primary investigator. The report included patient name, medical record number, patient unit location, patient status at time of the alert (alive or deceased), gender, age, ethnic group, race, alert base description, date and time alert occurred, alert recipient, recipient role, action taken when alert fired, and rationale for overriding the alert. This report was obtained daily during each of the 2-week study periods.
Deceased patients and units excluded from the study were deleted from the sample prior to coding. Because the alert was never cleared from the inactive platform, it triggered every time the chart was opened as such, multiple firings by providers within a close time frame were deleted from the sample. Whenever possible, the test firings on the provider platform were correlated with an RN firing at the same time to assist in appropriately measuring the effectiveness of the proposed changes.
Using the patient sample data, two separate reports were generated approximately 2 weeks following the last daily report of sepsis BPA firings. These reports included all ICD-10 codes for sepsis and ANGUS criteria that query for infection codes and organ dysfunction codes. A patient in the sample was coded for sepsis if he had two or more organ dysfunction codes and an ICD-10 infection code or sepsis code. Multiple patient encounters over the study period were coded as a unique patient visit for the purposes of data analysis.
General demographic data of interest such as age, gender, ethnicity, and body mass index (BMI) were collected during each phase of the research project as these factors are known to affect mortality and length of stay and present the opportunity for further analysis (Martin, Mannino, & Moss, 2006; Nguyen, et al., 2016; Sakr et al., 2013). As mortality was not examined in the scope of this study, BMI analysis is not included.
The same procedure was followed for the second round of data collection.
Ethical Considerations
Institutional review board (IRB) approval was obtained from the institution where the research occurred to ensure appropriate ethical practices and patient protections.
Results
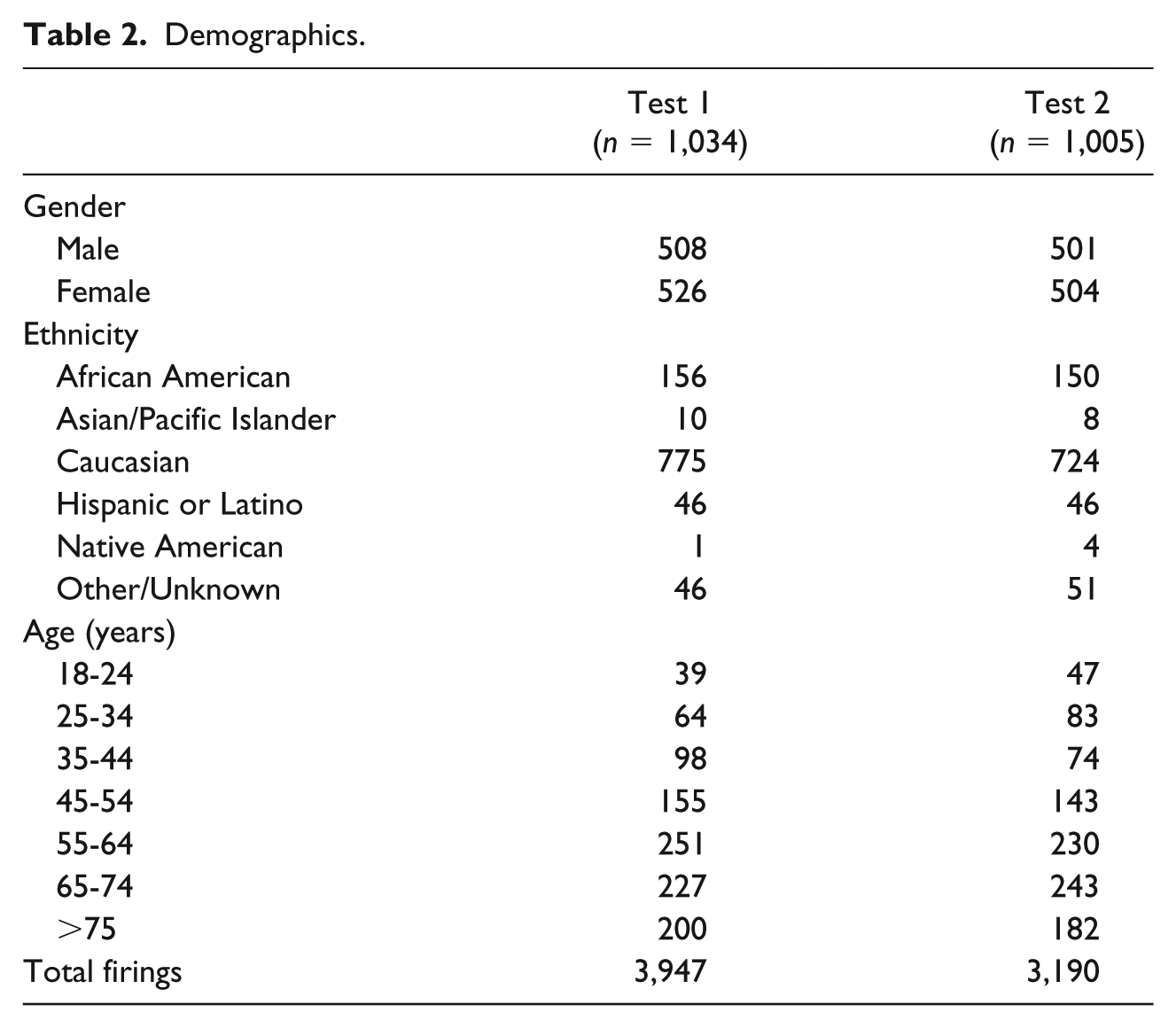
Test 1 examined 1,034 patients and had 3,947 firings for all tools in a 2-week period (Table 2). Subjects were equally divided between male and female, with the majority of participants being Caucasian between the ages of 55 years and 74 years (Table 2). This test showed current yellow warning sepsis tool with a specificity of 0.71 and sensitivity of 0.36 for catching sepsis, whereas current red warning sepsis shock tool showed a specificity of 0.17 and sensitivity of 0.93 toward catching sepsis (Figure 1). Revisions to the sepsis screening tool utilizing MEWS and NEWS vital sign definitions showed some improvement. Test 1 updated yellow warning sepsis tool showed a specificity of 0.80 and sensitivity of 0.23; updated red warning sepsis shock tool showed specificity of 0.64 and sensitivity of 0.52. Figure 1 examines these results.
Demographics.
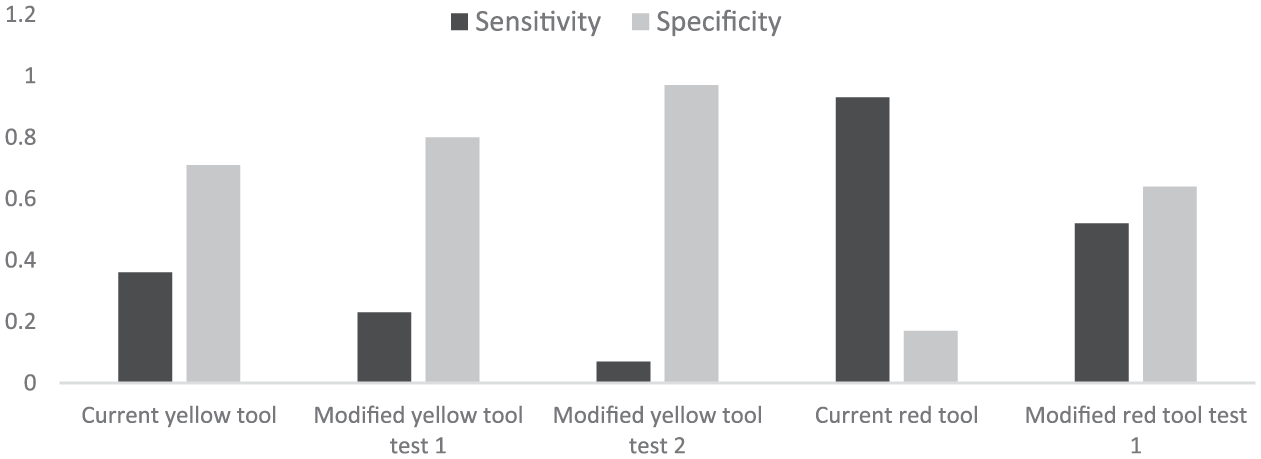
Sensitivity and specificity of all sepsis screening tool tests.
Decreasing the number of occurrences of the sepsis screening tool triggering within the EHR was also examined. On average, during Test 1, the updated yellow warning sepsis tool fired for approximately 10% fewer individuals than the current yellow sepsis tool, t(1033) = 9.31, p < .001, 95% CI = [0.078, 0.119]. The updated red warning sepsis shock tool, during Test 1, fired for approximately 46% fewer patients than the current red warning sepsis shock tool, t(1033) = 24.38, p < .001. 95% CI = [0.420, 0.493]. On average, current syellow warning sepsis tool fired 0.23 times more than the updated yellow warning sepsis tool, t(1033) = 9.77, p < .001 95% CI = [0.18, 0.27]. The current red warning sepsis shock tool fired, on average, 1.75 times more often than updated red warning sepsis shock tool, t(1033) = 24.59, p < .001 95% CI = [1.61, 1.89].
The odds ratio (OR) to establish a correct classification of firing for a patient with sepsis, or not firing for a patient without sepsis also showed improvement with the updated sepsis screening tools. Comparing current yellow warning sepsis tool with the updated yellow warning sepsis tool demonstrated an 18% improvement in correct classifications (0.82, 95% CI = [0.68, 0.98]). The updated red warning septic shock tool was able to capture approximately 3 times more correct sepsis classifications than the current red warning septic shock tool (29, 95% CI = [0.24, 0.35]).
The second round of data collection was tested for sensitivity and specificity to assess the feasibility of moving to a single sepsis screening tool. Sample size (n = 1,005) and demographic data were similar to the first sample with 50% of the participants being male and female. The majority (n = 743) were Caucasian, and the majority of the patients were between the ages of 55 years and 74 years (Table 2). Test 2 had 3,190 total firings over a 2-week period (Table 2). This testing showed yellow warning sepsis tool with increased specificity of 0.97 but low sensitivity of 0.07 (Figure 1). No red warning septic shock tool data were tested during this round of data collection with the intent of moving toward a single-tier warning system. Based on the initial sensitivity results, further analysis was not obtained.
Analysis was conducted using SAS 9.4 software.
Discussion and Implications
Determining the baseline information provides insight into the weakness of current tools and the difficulty for the RN in determining patient deterioration based on an electronic alert within the EHR. Brabrand et al. (2017) comment that a score perfectly identifying patients at risk will have inherent low specificity, so compromise must be achieved when designing a measuring tool. The results of this study are consistent with this concept. Some specificity and sensitivity were improved with the addition of MEWS/NEWS, particularly as demonstrated by the updated red warning septic shock tool. However, the challenge remains in finding the right combination of criteria that will have a positive predictive value for diagnosing sepsis, but not falsely fire too often.
The reduction in the overall sepsis screening triggers by using MEWS/NEWS criteria was a key finding of this research. These modifications alone pose the opportunity to improve RN awareness of patient deterioration and provide more rapid patient treatment by reducing the number of times the sepsis screening tool alerts for the RN. By reducing the number of alerts the RN receives within the charting workflow, there are fewer opportunities for alarm fatigue to develop, while improving attention to more accurate alerts.
The results indicate that moving toward one sepsis screening tool instead of the two-tier system that currently exists may provide additional opportunity to moderately decrease the sensitivity, with a reasonable increase in specificity. Red warning septic shock tool is not particularly sensitive in sepsis detection, but it does an excellent job of identifying a sick patient who needs further intervention. The possibility exists that the yellow warning sepsis tool could be eliminated and the red warning septic shock tool modified in ways that are consistent with MEWS/NEWS, while relying on the laboratory values of SIRS, as displayed in Table 3.
Proposed Criteria Changes to Sepsis Screening Tool.
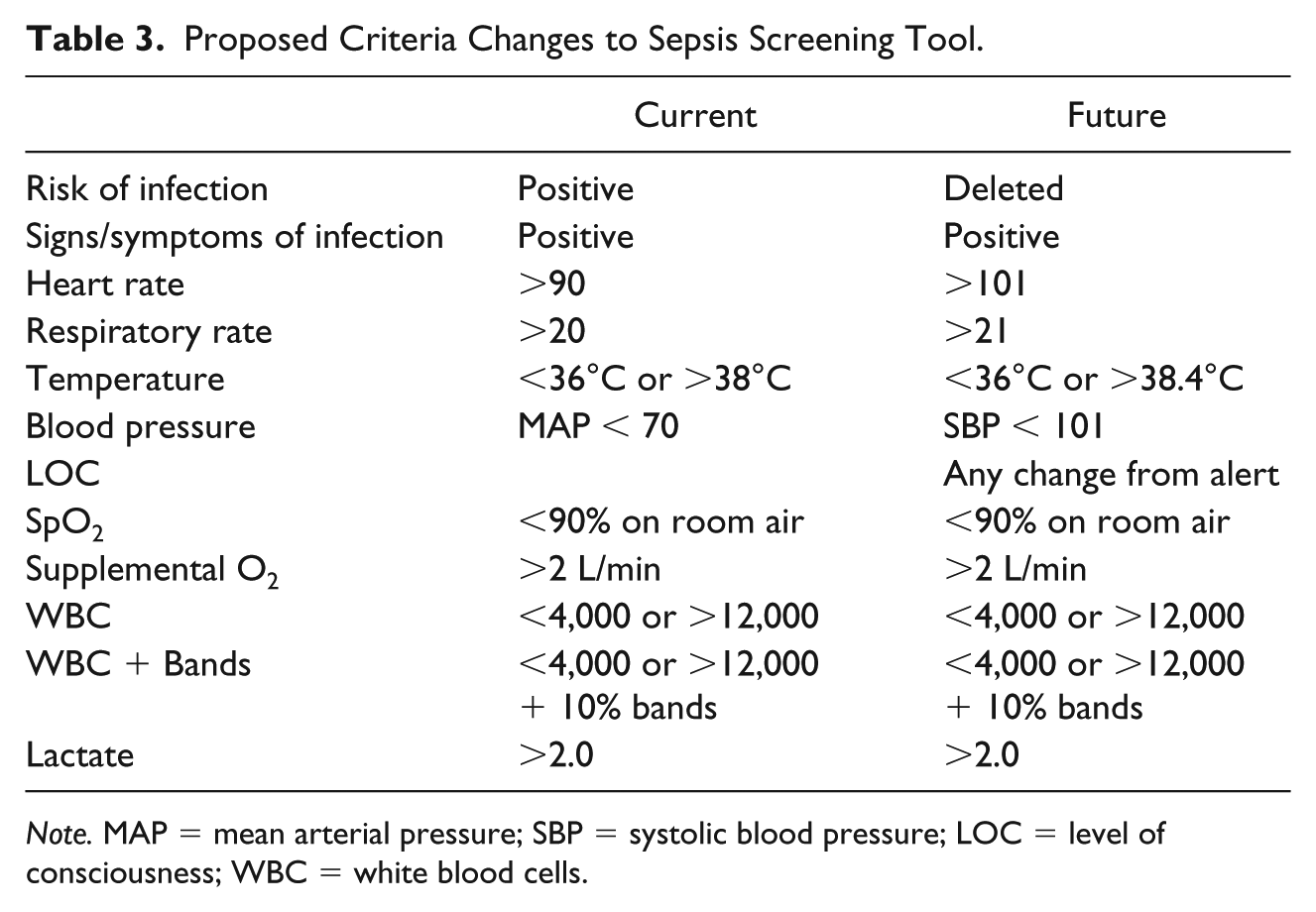
Note. MAP = mean arterial pressure; SBP = systolic blood pressure; LOC = level of consciousness; WBC = white blood cells.
With software enhancements made during the course of this study, the opportunity exists to track the most common reasons the RN-driven sepsis protocol is not utilized. This could lend insight into the rationale for not implementing the existing protocol and provide a measurable outcome that can be improved in the future. Another option for improvement includes locking out the sepsis tool for 48 hr after a patient has been to the operating room, thereby eliminating one of the major triggers of the sepsis screening tool.
Progress was made in improving the sensitivity and specificity of the sepsis screening tool, but it is unlikely that the correct combination of vital signs and laboratory data was found to provide an overall solution. Neither MEWS nor NEWS is heavily validated throughout the inpatient environment, but the results of this research indicate that early warning scores, when combined with laboratory values indicating infection, may provide insight into identifying sepsis and septic shock in the inpatient population (Roney et al., 2015). Further research should be done to examine vital sign modifications in conjunction with lab values to more efficiently screen patients at risk of, or decompensating from, sepsis.
There are numerous clinical indications for modifications to the sepsis screening tool. Improving patient outcomes by earlier detection of sepsis is paramount. In this regard, reducing the number of alerts within the EHR that the RN must filter helps to achieve this goal. Furthermore, with no diagnostic test to confirm sepsis as a diagnosis, hospitals and health systems must rely more heavily on screening tools, which increases the importance of establishing a reliable tool. Once a reliable tool has been established, consistent RN protocol implementation is necessary to improve patient outcomes.
Limitations
A key limitation relies on the RN accurately charting vital signs, particularly the respiratory rate of patients (Sharpe, 2015). Because obtaining vital sign data is a task often delegated to NAs on the study units, there is concern that the respiratory rate was not appropriately counted due to time constraints inherent within the position. This is easily overcome with education stressing the importance of accurate vital sign measurement. This project excludes patients from the ED in the analysis because the institution uses a different screening tool for those patients. The literature identifies the ED as the primary source for sepsis identification, and it is likely that modifications to the sepsis screening tool would improve patient outcomes by reducing the time to treatment if the study had included the ED. This study only examined patients on medical-surgical and telemetry/progressive care units. ICU patients are at high risk of sepsis but have multiple compounding factors affecting vital sign ranges, and the aim of this project was to improve an early recognition tool. With higher levels of monitoring available in ICU units, results could be skewed. The “risk of infection” component of the sepsis screening tool was eliminated for the purposes of this study and was not closely examined as to the statistical impact on the overall impetus for the sepsis screening tool firing. Patient census on study units was unable to be obtained during the study periods, which contributed to some slightly inflated CIs within the data.
Conclusion
Improvement was made in both the sensitivity and specificity of the sepsis screening tools by using a combination of recognized early warning scores, and the number of times the sepsis screening tool fired within the EMR was significantly reduced. Utilizing different early warning scores in combination with SIRS criteria has not been previously examined in the literature and merits further testing. Moving forward, the health care system plans to continue testing modifications of the tool with the hopes of system-wide implementation later this year.
There is great opportunity within the EHR to utilize multiple early warning scores, and laboratory values to create a sepsis and septic shock screening tool to assist the RN at the bedside in recognizing patient deterioration. Developing and implementing an effective screening tool will improve patient quality outcomes and has the potential to reduce length of stay, and reduce mortality across inpatient settings. Sepsis is a high-cost condition and places a heavy burden on the health care system. Earlier recognition of this condition presents an opportunity to utilize the RN skill set and reduce the burdens placed upon health care systems by this condition.
Footnotes
Acknowledgements
The authors thank the following persons: Rhonda Coffman, DNP, ARNP, ACNP-BC, FNP-C, assistant professor, Creighton University, Omaha, NE; Michelle M. Koeppen RN, MSN, clinical analyst, Health Information Technology Services, University of Kansas Health System; Greg Locker, BSN RN-BC, clinical informatics specialist, the University of Kansas Health System; Aroop K. Pal, MD, FACP, FHM, associate professor, associate section leader, Hospital Medicine, Associate CMIO, the University of Kansas Health System; and Steven Q. Simpson, MD, FCCP, FACP, professor of medicine, interim division director, Division of Pulmonary and Critical Care, the University of Kansas Heath System.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.