
Abstract
The aim of this study is investigating the efficiency of educational intervention based on PRECEDE model on promotion of osteoporosis prevention behaviors in women. This quasi-experimental study was conducted on 200 women registered in two health centers of Fasa city, Fars province, Iran in 2017 to 2018. A questionnaire including items evaluating demographic information and PRECEDE model constructs was used for measuring nutrition and walking performance of studied women in osteoporosis prevention before and 12 months after intervention. Bone mineral density (BMD) was recorded at the lumbar spine and femur before and 12 months after intervention. One year after intervention, the intervention group showed a significant increase in knowledge, attitude, self-efficacy, reinforcing factors, enabling factors, nutrition, and walking performance compared to the control group. Also, the value of lumbar spine and hip BMD T-Score of the intervention group was increased, while this value was reduced in the control group. Our findings showed that educational interventions based on PRECEDE model can positively affect prevention behaviors from osteoporosis by improving subjects’ knowledge, attitude, enabling factors (resources such as health care access and services that can provide motivation for prevention behaviors from osteoporosis in women), self-efficacy, and reinforcing factors.
Introduction
Osteoporosis is the most prevalent metabolic and chronic bone disease determined by the reduction of bone density and the loss of bone microstructures. Reduction of bone density happens gradually and its symptoms do not appear unless a bone fracture happens. Hence, this disease is called the silent disease of the century (Brecher et al., 2002; Solomon et al., 2006). Epidemiologically, almost 8 million women and 2 million men are suffering from osteoporosis and more than 18 million people are in exposure of osteoporosis in the USA. By getting older, osteoporosis happens more often, because bone structure decreases progressively. Fractures caused by osteoporosis result in some problems including chronic pain, dependence on others, reduction of life quality and the increase of death rate (Braunwald et al., 2001). Previous studies revealed that, age, sex, menopause, family history in bone fracture, lack of vitamin D (Gerber et al., 2015), lack of physical activity (Muir, Ye, Bhandari, Adachi, & Thabane, 2013), hypothyroidism and parathyroid dysfunction (Acar et al., 2016) are effective factors on variations of bone density.
According to World Health Organization (WHO), A “Normal” T-Score is from + 1 to −1. “Osteopenia” is the term used for a T-Score ranging from −1 to −2.5 and “Osteoporosis” is the term used for a T-Score of −2.5 and below (Cosman et al., 2014). Compared to men, women are highly in exposure of osteoporosis (Adachi et al., 2010) and almost 200 million women are suffering from this disease around the world (Shirazi et al., 2006). Bone density of women in all ages is significantly less than men with same ages and in both sexes the maximum bone density is obtained up to the age of 30 and then, by getting older, bone density reduces (Cosman et al., 2014). Every 3 seconds, one fracture caused by osteoporosis happens around the world, and every 22 seconds, one fracture happens in the spine (Schwellnus et al., 2011). One out of two women aged 50 experiences a fracture in the spine and one out of three men of the same age experiences a fracture in the hip bone (Schwellnus et al., 2011).
In a study performed in Fars province, Iran, based on WHO criteria, the prevalence of osteoporosis in the lumbar spine, femoral neck, and total femur were 10%, 6.1%, and 24%, respectively (Tohidi, Dabbaghmanesh, Fattahi, & Ranjbar Omrani, 2010). Another study, conducted in Fasa, Iran, indicated that 34.1% of studied women were suffering from osteoporosis (Nobakht Motlagh et al., 2013).
Medical expenses related to osteoporosis treatment are high (Moayyeri et al., 2006) and in the USA, medical expenses related to fracture treatment caused by osteoporosis is calculated at almost 22 billion dollars (Blume & Curtis, 2011). If efficient prevention actions are not promoted among people, it is predicted that by 2040, expenses related to osteoporosis problems will reach to 200 billion dollars around the world (Babatunde, Himburg, Newman, Campa, & Dixon, 2011).
Results of different studies indicated that exercising and receiving sufficient calcium and vitamin D have a great effect on improving bone density and bone mineral density (BMD) (Kelley & Kelley, 2006). Among adults, appropriate nutrition can save the density and strength of bone. Different nutrients with sufficient calcium can result in the enhancement of bone strength and the improvement of life quality of people (Madureira, Bonfá, Takayama, & Pereira, 2010). Regular physical activity improves bone health, and by increasing muscle strength and body balance, it will have a great effect on overall body health (Tüzün, Aktas, Akarirmak, Sipahi, & Tüzün, 2010). Physical activity is suggested as a nonmedical intervention for increasing bone density at young ages and preventing the reduction of bone density in middle age. Osteoporosis is preventable and the important factor in osteoporosis prevention is recognizing the ideas, lifestyles, and daily habits of people for improving the quality and efficiency of their lives (Egbunike, Wood, & Grant, 2009). Therefore, teaching prevention behaviors, such as physical activities and proper nutrition, as a simple and effective method has a great effect on prevention of this disease. One of the most important objectives of WHO is to increase the number of women educated in osteoporosis (Sedlak, Doheny, Estok, & Zeller, 2005), because recognizing effective factors in changing a behavior facilitates the change of that behavior. Hence, investigating effective factors on prevention behaviors from osteoporosis among women via educational patterns is essential (Khorsandi, Shamsi, & Jahani, 2010). Specialists believe that the efficiency of an educational program depends on the use of health education models and theories (Araban et al., 2013). Theories and patterns provide a systematic perspective for analyzing the failures and successes of a process and provide much-needed guidelines for investigating and determining educational programs and interventions (Araban et al., 2013). One of these efficient models is PRECEDE pattern, which is a process for changing inappropriate behaviors and investigates the possible consequences of an educational program (Jeihooni, Kashfi, Hatami, Avand, & Bazrafshan, 2019). This pattern was then developed to PRECEDE–PROCEED model, which is one of the most well-known models in health education and promotion. The term “PRECEDE” is related to the predisposing constructs (knowledge, attitude, and self-efficacy), reinforcing factors (family members, friends, doctors, and health officials), and enabling factors (resources such as health care access and services that can provide motivation for osteoporosis prevention behaviors in women). Also the word “PROCEED” is related to the political, regulative, and organizational constructs in educational development (Sharma, 2016). This model was presented by Larens Green and Marshal Croter and it is an approach for analyzing the effective factors in changing behavior determined by an individual’s motivation for being engaged in changing behavior process (Sharma, 2016).
Meador and Linnan (2006) used the PRECEDE model to plan men’s health programs in a managed care setting. Mo and Mak (2008) investigated the application of the PRECEDE model in understanding mental health promotion behaviors in Hong Kong. Tabasi Nejad, Mohseni, Khanjani, and Ahmadi Tabatabaei (2018) investigated the application of PRECEDE–PROCEED model in promoting physical activity among women for osteoporosis prevention, and after educational intervention, the average scores of predisposing, reinforcing and enabling factors and also osteoporosis prevention behaviors were significantly increased in intervention group. Khani Jeihooni, Kashfi, Zareei Kooshkghazi, and Kashfi (2017) investigated an educational program based on PRECEDE model on fruit and vegetable consumption by female high school students in Fasa, Iran. The average scores of predisposing (knowledge and attitude), reinforcing, and enabling factors showed significant differences in intervention group compared to the control group. In a quasi-experimental study by Jeihooni, Hidarnia, Kaveh, Hajizadeh, and Askari (2015), 120 subjects (60 subjects in the intervention group and 60 subjects in the control group) under cover of health centers of Fasa, Iran, were selected in 2014. In their study, a questionnaire evaluating demographic information and health belief model (HBM) constructs was used to measure the nutrition and walking performance of subjects in osteoporosis prevention before, immediately after, and 6 months after intervention. Immediately after and 6 months after intervention, the intervention group showed significant enhancement in knowledge, perceived susceptibility, perceived severity, perceived benefits, perceived barriers, self-efficacy, internal cues to action, nutrition, and walking performance compared to the control group.
Due to osteoporosis complications and the importance of prevention behaviors from this disease among women, the purpose of this study was to investigate the efficiency of educational intervention based on PRECEDE pattern on promotion of prevention behaviors from osteoporosis among women living in Fasa city, Fars province, Iran.
Methods and Materials
The present research is a quasi-experimental study performed on 200 women under the cover of health centers of Fasa city, Fars province, Iran in 2017 to 2018. Among six urban health centers of Fasa city, two centers were randomly selected as intervention and control groups. Simple random sampling was used based on the number of health records of the households covered by the centers. The subjects of each group were then invited to a special meeting in a health center. The objectives of this study were explained and a consent letter about their participation in this research was signed by them. The inclusion criteria of current research included women aged from 30 to 60 years with no mental or psychological disability, rheumatoid arthritis, malabsorption, osteoporosis (women without osteoporosis are diagnosed by BMD), bone infection, food allergy, or any congenital anomalies. The exclusion criteria were subjects’ decision to withdraw from the study and being absent from more than two educational sessions.
Sample size was determined based on the study by Ghaffari, Tavassoli, Esmaillzadeh, and Hassanzadeh (2012), in which the average score and standard deviation of received calcium before and after intervention was 813.31 ± 264.75 and 1096.61 ± 590.21 mg in studied groups. Based on mentioned reference and B = 0.90, α = 0.05, S1 = 264.75, S2 = 590.21, µ1 = 813.31 and µ2 = 1096.61, 55 subjects were estimated for each group, and by considering the sample drop, 100 subjects were selected for each group. Figure 1 indicates the flow chart of present research.
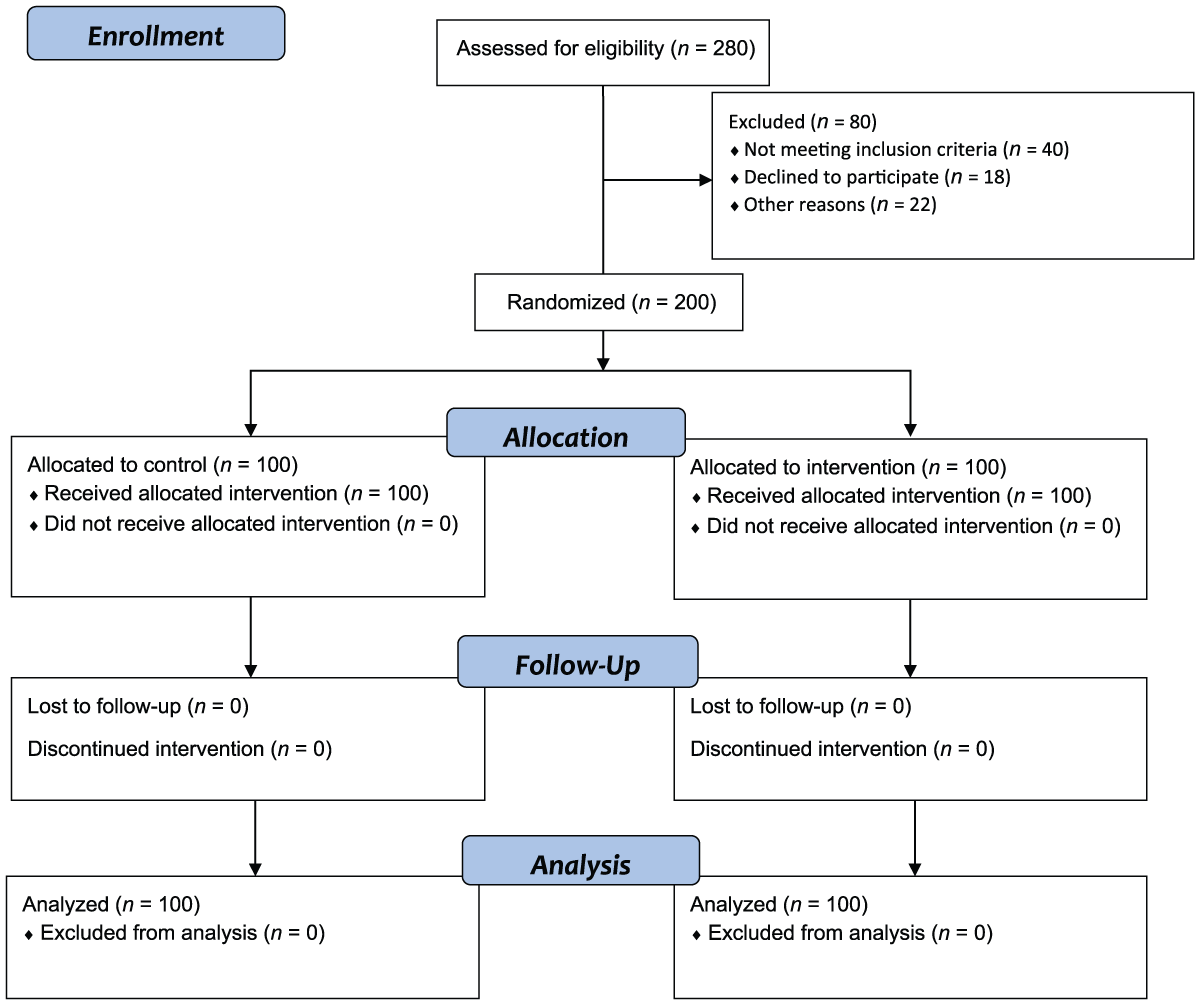
Flow chart of the study.
After selecting intervention and control groups, a pre-test questionnaire (based on PRECEDE model) was filled out by two groups and subjects were introduced to the bone density evaluation center of Fasa city in order to evaluate their bone density and results were recorded. Bone density was evaluated by DEXA (dual-energy X-ray absorptiometry) using Hologic system in bones from L1 to L4. Information obtained from densitometer included bone density in the lumbar spine and femur which is recorded and based on the definition according to the criteria WHO in T-Score. Densitometer (DEXA) was same for all participants before and after the intervention.
Educational intervention for the intervention group included 10 educational sessions for 50 minutes by giving a presentation, asking and answering questions and group discussion, and also using educational posters, pamphlets, films, and PowerPoints. The educational program was performed by a PhD scholar in health education and promotion and an orthopedist with the cooperation of two specialists in community medicine. Educational sessions were held for four groups with 25 members twice a week in health center of Fasa city for 100 subjects of the intervention group as follows:
First session: Introducing osteoporosis, symptoms, complications, and diagnosis.
Second session: Risk factors, symptoms, complications and diagnosis (knowledge).
Third session: A 55-year-old woman suffering from osteoporosis and bone fracture was invited to talk about this disease and its complications. In this section, attitude of subjects about osteoporosis prevention was emphasized (as role playing and talking about personal experiences; knowledge and attitude).
Fourth and fifth sessions: The role of nutrition in osteoporosis prevention, appropriate diet, changing attitude and decision making, self-efficacy in tracking proper diet based on presented pattern, and recording activities in determined forms were discussed, and women in the study were provided food containing calcium (self-efficacy and behavior).
Sixth and seventh sessions: The role of exercising, proper physical activities, self-efficacy in walking and recording the duration of walking in determined form were emphasized (self-efficacy and behavior).
Eighth and ninth sessions: These sessions were held with the presence of a family member, doctors, and health center officials as reinforcing factors and social supports, and their supporting role in facilitating and providing appropriate food and walking performance and BMD test was emphasized (reinforcing and enabling factors).
Tenth session: Previous contents were reviewed and educational booklets were given to subjects.
Subjects were divided into groups with 8 to 10 members and the role of peers and friends as facilitating factors in taking prevention behaviors from osteoporosis was mentioned, and subjects started walking in a determined direction (reinforcing and enabling factors). Also, for retaining and promoting subjects’ activities, an educational short message service (SMS) about osteoporosis was sent to them once a week and a WhatsApp group was provided for exchanging information; also, every month, one educational session was held for tracking subjects’ activities (reinforcing factors, enabling factors, and behaviors). Twelve months later, a questionnaire was filled out by two groups and subjects performed bone-density evaluation test and results were recorded. It should be noted that the control group received no educational, program, and that at the end of investigation, in order to observe ethical standards, one educational session about osteoporosis and the importance of prevention behaviors from this disease was held for the control group.
The tool used for gathering data was a questionnaire for evaluating demographic information (age, body mass index [BMI], job status, educational level, household income, number of deliveries, consumption of tobacco production, and family history in osteoporosis) and constructs of PRECEDE model. This questionnaire was arranged based on other similar studies (Babatunde et al., 2011; Egbunike et al., 2009; Ghaffari et al., 2012; Jeihooni et al., 2015; Khani Jeihooni et al., 2017; Madureira et al., 2010; Tabasi Nejad et al., 2018). Twenty-five questions were asked about knowledge of osteoporosis and prevention behaviors and each correct answer had a score of 1 and each incorrect or “no idea” answer had a score of 0. The range of scores in this section was from 0 to 25. Attitude was evaluated by 15 questions in five-point Likert scale from “completely disagree” (1) to “completely agree” (5) ranging from 15 to 75. Self-efficacy was evaluated by 15 questions in five-point Likert scale from “completely disagree” (1) to “completely agree” (5) ranging from 15 to 75. Ten questions were asked about reinforcing factors (social supports) evaluating perceived social supports from families, doctors, health center officials and, among others, on a five-point Likert scale from “never” (0) to “very much” (4) ranging from 0 to 40. Ten questions evaluated enabling factors by asking questions such as “How much having food containing calcium is easy for you?” on a five-point Likert scale from “never” (0) to “completely” (4) ranging from 0 to 40. Nutrition performance was evaluated by 10 questions asking the type and amount of nutrients an individual had had in the previous week ranging from 0 to 14. They were asked to write down the mean consumption of each item over the past week according to the items of questionnaire. The consumed amount of the research units in each item was changed from 0 to 14. Walking performance was evaluated by seven questions, including duration and type of walking (light, medium, and hard), during the past week based on given guideline (ranging from 0 to 21). Subjects’ performance was recorded in determined forms through self-reporting answers (Jeihooni et al., 2015).
Data Analysis
Item validity of this questionnaire was evaluated by calculating item effect size higher than 0.15 and content validity ratio higher than 0.78. In order to determine the face validity of the tool, a list of arranged items was considered by 40 women aged from 30 to 60 years with similar demographic, economic, and social characteristics to the target population. For determining content validity, ideas of 12 specialists (out of research team) in health education and promotion (n = 10), orthopedist (n = 1) and biostatistician (n = 1) were used. Based on Lawshe’s table index, items with content validity ratio (CVR) value higher than 0.56 for 12 people were considered acceptable and retained for subsequent analysis. In the present research, calculated values for most of the items were higher than 0.70. Total internal consistency of the tool, by calculating Cronbach’s alpha, was 0.87. The internal consistency of knowledge was 0.88, attitude was 0.86, self-efficacy was 0.75, reinforcing factors was 0.79 and enabling factors was 0.81.
Ethical Considerations
For ethical consideration, the present research was confirmed by the ethical committee (ethical code: IR.FUMS.REC.2017.155) of Fasa University of Medical Sciences, Fasa, Iran and also a consent form was signed by subjects and they were assured that their information would remain confidential. Obtained data were analyzed by SPSS22 software through chi-square test, independent t-test and paired t-test and the significance level was considered 0.05.
Results
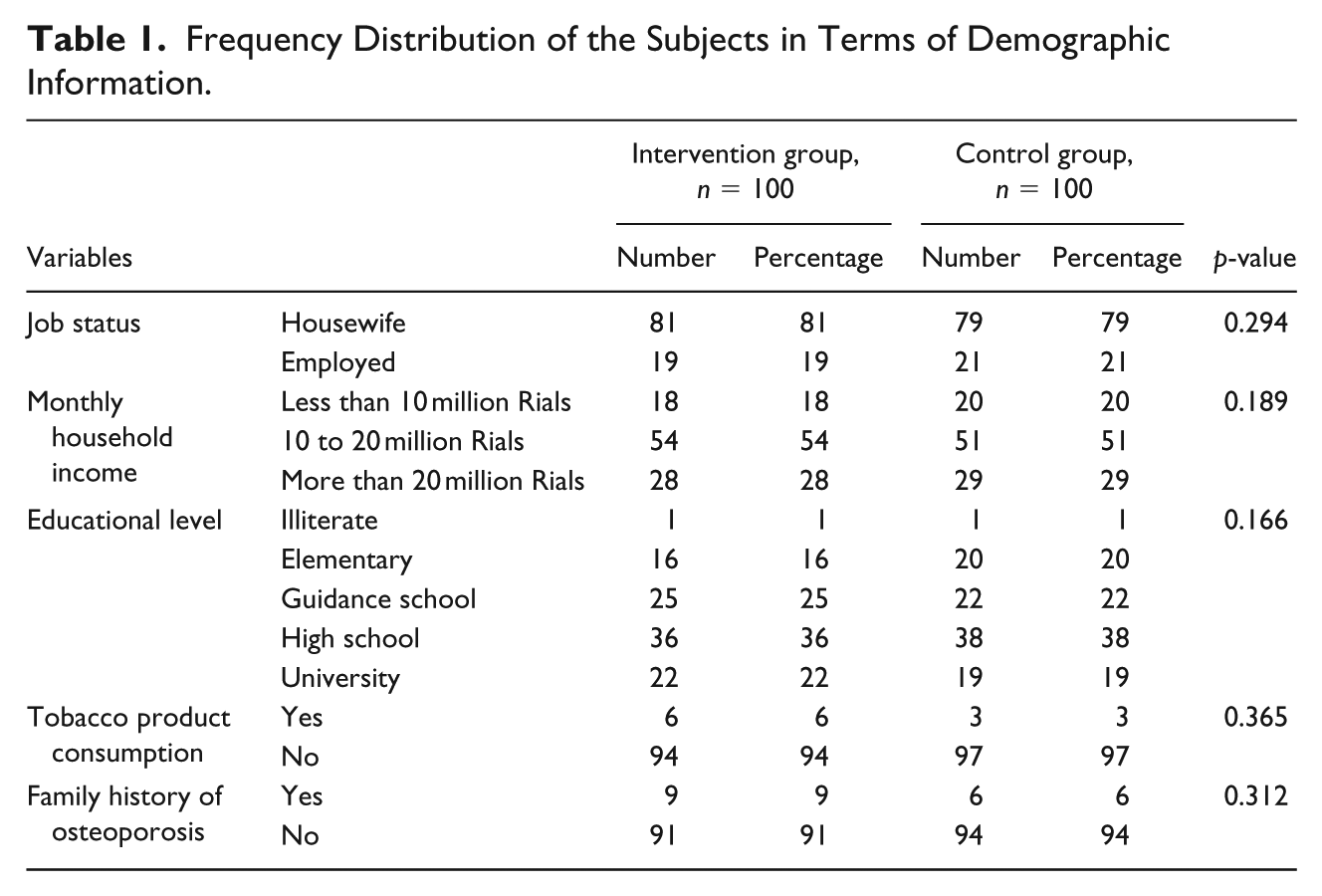
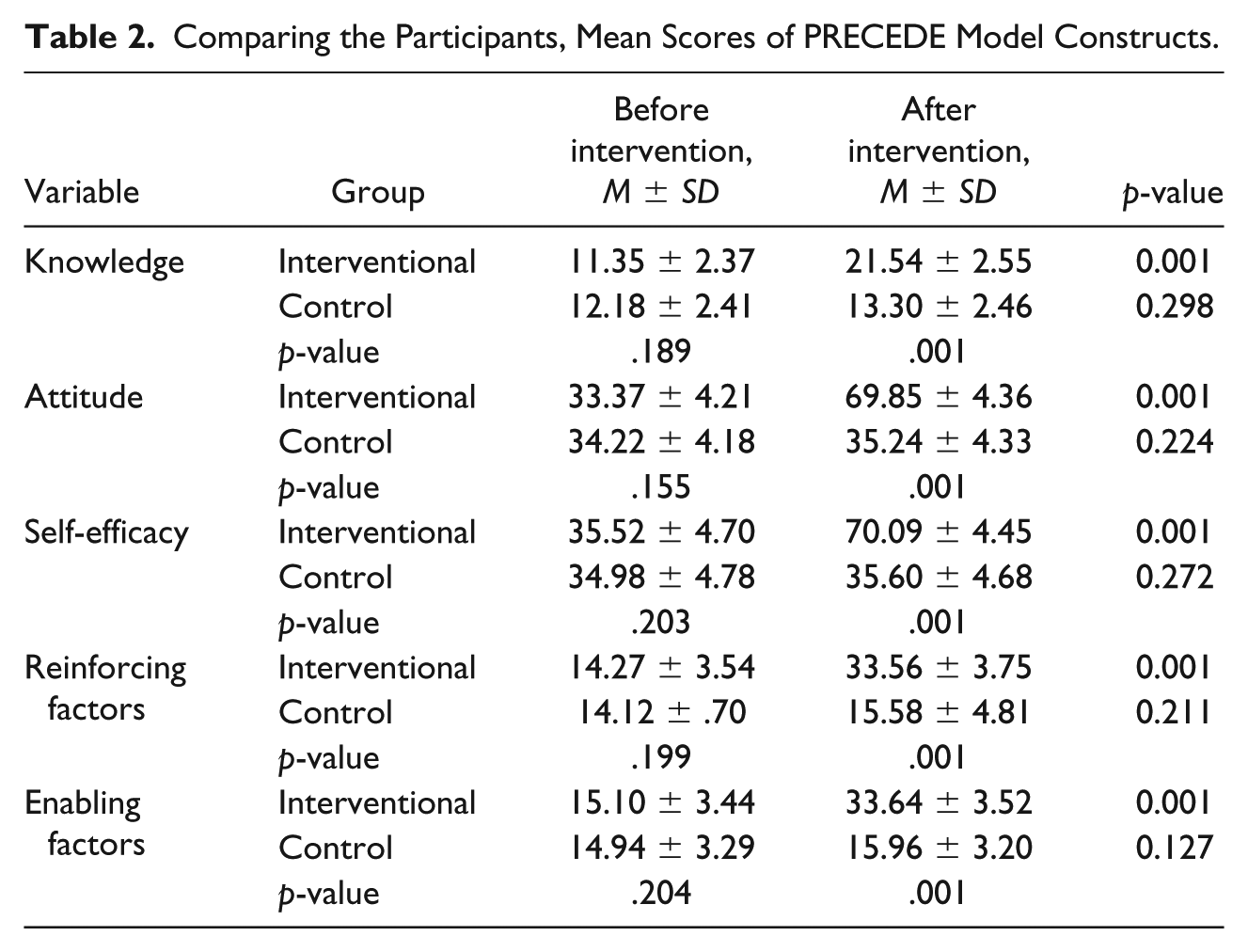
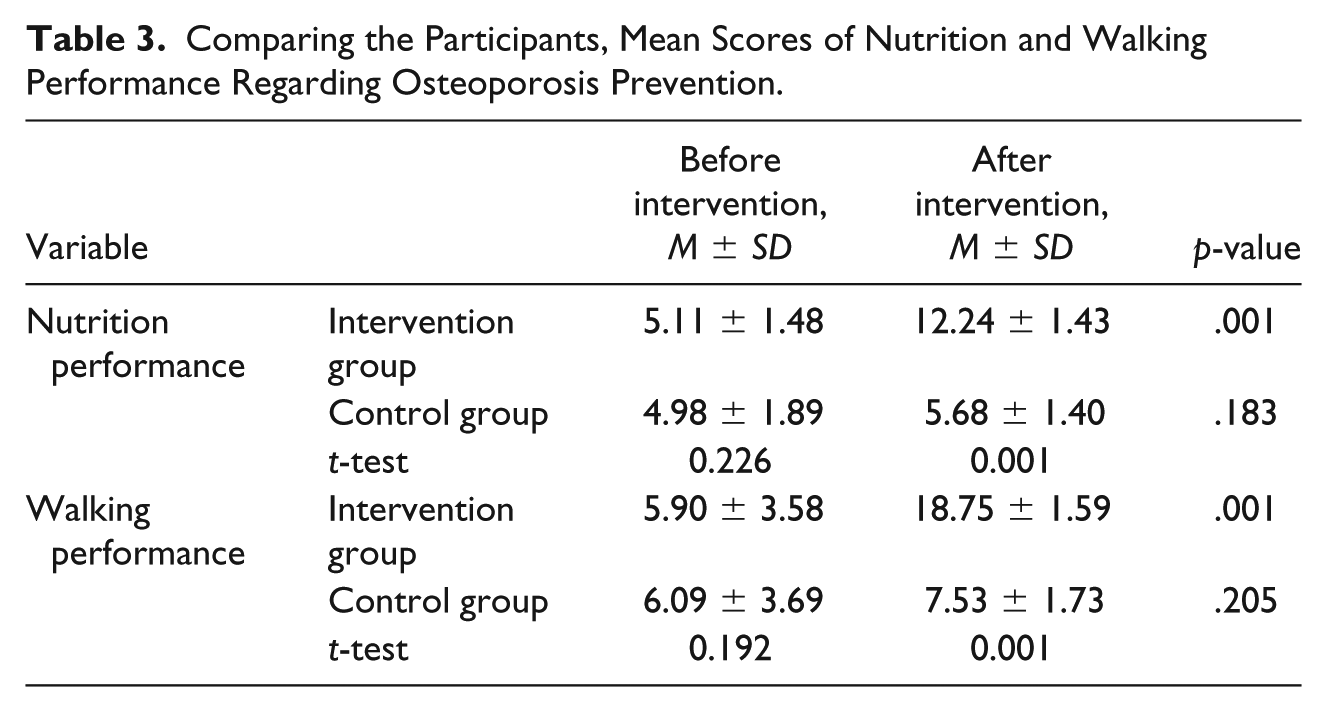
In the current study, 200 women aged from 30 to 60 years participated. The average age in the intervention group was 47.14 ± 5.66 and the average age in the control group was 47.88 ± 5.35 (p = .265). The average BMI in the intervention group was 22.74 ± 3.23 and the average BMI in the control group was 22.47 ± 3.72 (p = .208). Also, the average numbers of deliveries in the intervention and control groups were 2.77 ± 1.52 and 2.68 ± 1.57, respectively (p = .186), and based on independent t-test, there were no significant differences between the two groups before educational intervention. Chi-square test indicated that there were no significant statistical differences between intervention and control groups in educational level (p = .166), monthly household income (p = .189), job status (p = .294), tobacco products consumption (p = .365), and family history of osteoporosis (p = .312) (Table 1). Results revealed that before educational intervention, there were no significant differences between the two groups in knowledge, attitude, self-efficacy, reinforcing factors, enabling factors, nutrition performance, and walking performance, however, 1 year after intervention, intervention group had significant enhancement in mentioned variables, whereas the control group had no changes (Tables 2 and 3).
Frequency Distribution of the Subjects in Terms of Demographic Information.
Comparing the Participants, Mean Scores of PRECEDE Model Constructs.
Comparing the Participants, Mean Scores of Nutrition and Walking Performance Regarding Osteoporosis Prevention.
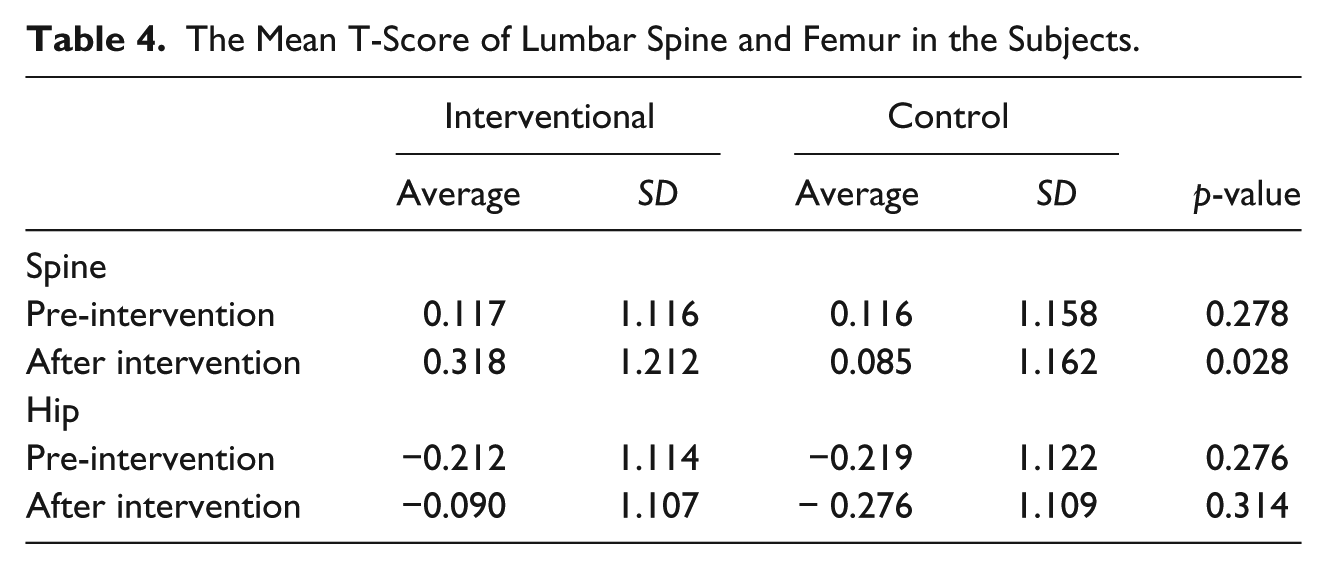
The comparison of bone density T-Score in the lumbar spine (p = .278) and femur (p = .276) in the studied women showed that before intervention, there was no significant difference between the intervention and control groups in this regard. However, 12 months after intervention, the value of lumbar spine BMD T-Score of the intervention group was increased, while, this value was reduced in the control group (p = .028). Also, the value of hip BMD T-Score in the intervention group was increased, whereas it decreased in the control group (p = .314) (Table 4).
The Mean T-Score of Lumbar Spine and Femur in the Subjects.
Discussion
Changing lifestyles, especially by receiving sufficient calcium and performing physical activities, are some factors that should be taught to women using community-based interventions such as PRECEDE model (Jeihooni et al., 2015; Tabasi Nejad et al., 2018). The purpose of the current study was to investigate the effect of educational intervention based on PRECEDE pattern on prevention behaviors from osteoporosis in women living in Fasa city, Fars province, Iran. In the current study, before educational intervention there was no significant difference between the intervention and control groups in demographic variables, average scores of knowledge, attitude, self-efficacy, reinforcing factors, enabling factors, nutrition performance, walking performance, and BMD of subjects, indicating the minimum effect of confounding factors on the obtained results. Also, present results revealed that 1 year after educational intervention, the average score of the intervention group’s knowledge about osteoporosis and its prevention behaviors had significant enhancement, whereas the control group had no changes. The present study also revealed that educational intervention through giving presentations, group discussions, asking and answering questions, providing a WhatsApp group for exchanging information, sending educational SMS, giving educational booklets, and introducing osteoporosis, its symptoms, complications, and diagnosis for intervention group caused significant enhancement in subjects’ knowledge. Studies by Lai, Chua, and Chan (2013), Okumus et al. (2013), Babatunde et al. (2011), Curry, Hogstel, Davis, and Frable (2002), Oh et al. (2014), Nielsen et al. (2008), Kalkım and Dağhan (2017), Jo et al. (2018), Niazi, Ghafari, Noori, and Khodadoost (2013), Laslett, Lynch, Sullivan, and McNeil (2011), Huang, Su, Chien, and Guo (2011) and Shakil et al. (2010) indicated that educational intervention results in significant enhancement in subjects’ knowledge about osteoporosis.
In the current study, 1 year after educational intervention, the average score of the intervention group’s attitude had significant enhancement indicating the effect of PRECEDE pattern on the increase of positive attitude of subjects. In PRECEDE model, predisposing factors, such as attitude, are important motivating factors in changing behavior. In the present research, positive attitude facilitated adopting proper behaviors (nutrition and walking performances) in osteoporosis prevention. Presenting contents in one of the educational sessions by a woman suffering from osteoporosis and bone fracture as a pattern caused changes in attitude toward prevention behaviors. Emphasizing the benefits of adopting prevention behaviors from osteoporosis and providing group discussions, asking and answering questions, presenting films, and sending educational and motivational SMS for subjects changed subjects’ positive attitude. Also, for improving their attitude, an educational booklet was given to subjects. In study by Puttapitakpong et al. (2014) on 430 women aged from 20 to 35 years, subjects obtained their information about osteoporosis from TV and the Internet and they had sufficient knowledge and positive attitude toward this disease; however, almost 80% of subjects did not follow proper prevention behaviors from osteoporosis. In a study by Mohammadi, Ghofranipour, and Gholami-Fesharaki (2015) on female guidance school students, the intervention group received an educational program in two educational sessions for 60 minutes, and 1 month after intervention the average score of their attitude had significant enhancement, whereas the control group had no changes. In studies of Amini, Tavousi, and Niknami (2014), Mohammed, Ellife, and Lawend (2014), (Azar, Solhi, Zohoor, and Hosseini (2012) and Shakil et al. (2010), educational intervention caused the enhancement of subjects’ attitude about osteoporosis.
The present study indicated that 1 year after educational intervention, the average score of self-efficacy of the intervention group had significant enhancement, whereas the control group had no changes. Self-efficacy is an individual’s belief about his/her abilities in the successful performance of a specific behavior and it is an important and effective construct in educational theories. Therefore, in designing educational programs, the special role of this construct in behavioral habits, such as nutrition and exercising, should be considered. In the present study, one way of increasing subjects’ self-efficacy in osteoporosis prevention behaviors was encouraging them to have nutrients containing calcium and presenting an appropriate nutrition pattern, as well as recording subjects’ activities in determined forms. In a study of Swaim et al. (Swaim, Barner, and Brown (2008), self-efficacy had a significant relationship with prevention behaviors from osteoporosis. In a study by (Malekshahi, Haidarnia, Niknami, and Aminshokravi (2014), self-efficacy was a predictor of receiving calcium in women aged from 30 to 50. In studies of Solimanian, Niknami, Hajizadeh, Shojaeezadeh, and Tavousi (2014), BaghianiMoghadam, Khabiri, Morovati, Dehghan, and Falahzadeh (2016; Ali Khani Jeihooni, Alireza Hidarnia, Mohammad Hossein Kaveh, Ebrahim Hajizadeh, Alireza Askar, 2015) and self-efficacy was one of the important constructs in predicting walking performance in osteoporosis prevention among studied women. In a study by Khorsandi, Hasanzadeh, and Ghobadzadeh (2012), the level of knowledge and self-efficacy of osteoporosis prevention was low. Results of other studies are in agreement with the results of this study, indicating the increase of average score of self-efficacy after educational intervention (Babatunde et al., 2011; Bhurosy & Jeewon, 2013; Jeihooni, Jamshidi, Kashfi, Avand, & Khiyali, 2017; Jeihooni, Kashfi, Bahmandost, & Harsini, 2018; Khiyali, Aliyan, Kashfi, Mansourian, & Jeihooni, 2017; Oh et al., 2014; Zong & Duan, 2014).
Results of the present study indicated significant differences between intervention and control groups 1 year after educational intervention in enabling factors. Providing educational booklets for subjects, availability of doctors, health center officials, and BMD test centers, and also providing a WhatsApp group for exchanging information, sending SMS, holding educational sessions, tracking subjects’ activities after educational sessions, presenting educational contents through asking and answering questions, and educational films and images caused the enhancement of subjects’ abilities in performing prevention behaviors from osteoporosis. In a quasi-experimental study by Tabasi Nejad et al. (2018) on 120 women aged from 15 to 49 years, physical activities for osteoporosis prevention based on the PRECEDE–PROCEED pattern were taught for subjects and after educational intervention, the average score of enabling factors, predisposing factors, and reinforcing factors of the intervention group increased. In studies by Kashfi et al. (Seyed Mansour Kashfi, Jeihooni, Rezaianzadeh, and Karimi (2014), Jeihooni et al. (2019), Jeihooni and Moradi (2018), and Hazavehei, Khani Jeihooni, Hasanzadeh, and Amini (2010), educational intervention caused the increase of the average score for enabling factors in the intervention group.
In the current investigation, 1 year after educational intervention, the average score of reinforcing factors (social supports) of the intervention group had significant enhancement. Holding educational sessions for doctors, health center officials, and families as social supports, and engaging them in educational programs and creating peers and friends groups and tracking their activities caused the increase of average score of reinforcing factors in intervention group. Results of present study are in a good agreement with the results of Tabasi Nejad et al. (2018), Jeihooni, Fereidouni et al. (2018), Jeihooni, Hidarnia, Kaveh, Hajizadeh, and Askari, (2016), Jeihooni and Rakhshani (2018) and Kashfi, Khani Jeihooni, and Rezaeianzade (2012).
In the present research, before educational intervention there were no significant differences in the average score of women’s performance in taking prevention behaviors from osteoporosis in intervention and control groups, and the performance of each group in following an appropriate diet and exercising was less than average. The present theory-based educational program, by emphasizing effective factors in promoting prevention behaviors such as having an appropriate diet (having fruits, vegetables, and foods containing calcium) and exercising through presenting films, posters and pamphlets, explaining the advantages or disadvantages of prevention behaviors, increasing subjects’ self-efficacy and engaging social supports, such as families, caused the improvement of prevention behaviors from osteoporosis in intervention group. Hazavehei et al. (2007) reported an increase of walking performance and received calcium after educational intervention in the intervention group. In a study of Al Seraty and Ali (2014) on 100 female university students, after educational intervention, subjects’ performance in receiving calcium and performing physical activities improved significantly.
The study by Tarshizi, Anousheh, Ghofranipour, Ahmadi, and Hoshyarrad (2009) showed that the subjects’ physical activity levels before the training was not appropriate. However, by applying the health belief model (HBM) training in the intervention group, a significant difference was observed in this area.
Mehrabbeik, (2010) indicated significant statistical differences in subjects’ physical activity after educational intervention in the intervention group compared to the control group, which was in agreement with the results of present study. However, before and after intervention, daily received calcium and vitamin D did not show any significant differences. Shojaezadeh, Sadeghi, Tarrahi, Asadi, and Lashgarara (2012) indicated that in the second stage of the study, the level of received calcium was significantly enhanced. However, in the third stage of the study (3 months after intervention), the value of received calcium reduced. In a study by Lein, Turner, and Wilroy (2016), after educational intervention, the average score of received calcium improved and the average score of perceived barriers reduced. Shobeiri, Hesami, Khodakarami, and Soltanian (2015) investigated the effect of consultation on prevention behaviors from osteoporosis in women who were referred to health centers in Hamedan, Iran. In this study, the intervention group received an educational program for 4 weeks. The results revealed that, immediately after and 2 months after intervention, nutrition performance of the intervention group was significantly better than that of the control group. The results of the mentioned study are similar to the results of Hsieh et al. (2014), who indicated that educational programs have a great effect on promoting prevention behaviors from osteoporosis. A study by Tussing and Chapman-Novakofski (2005) showed significant differences in received calcium before and after intervention, and by designing an educational program based on HBM and rational action theory, the value of received calcium was enhanced. In a study by Niazi et al. (2013), educational intervention caused the improvement of subjects’ physical activity. In a study of Vahedian-Shahroodi et al. (2016), after educational intervention, subjects showed significant differences in knowledge, perceived severity, perceived self-efficacy, cues to action, perceived benefits, and calcium intake, whereas they showed no significant differences in perceived susceptibility, perceived barriers, and physical activity. In other similar studies, educational intervention caused the improvement of subjects’ performance in osteoporosis prevention (Bhurosy & Jeewon, 2013; Brecher et al., 2002; Chan, Ko, & Day, 2005; Kalkım & Dağhan, 2017; Oh et al., 2014; Zong & Duan, 2014). In the current study, 1 year after intervention, the intervention group indicated significant improvement in the T-Score of bone density in lumbar spine and thighs, whereas in the control group the mentioned factor was reduced, indicating the effect of educational intervention based on PRECEDE pattern on prevention behaviors from osteoporosis and promotion of bone density of studied women in the intervention group. In a study by Khani Jeihooni et al. (Jeihooni et al., 2015), 6 months after educational intervention, the value of the lumbar spine BMD T-Score of the intervention group was increased to 0.127, whereas in the control group, this value was reduced to −0.043 and the value of the hip BMD T-Score in the intervention group was increased to 0.125, but in the control group, this value was decreased to −0.028.
Huang et al. (2011) revealed that perceived advantages result in significant improvement in osteoporosis prevention behaviors of the intervention group. Also, the effect of the educational program on social supports from families, friends and health professionals was significant in the intervention group. Self-efficacy of the intervention group was one of the variables enhanced due to the educational program, and the BMD of intervention group was improved, whereas the BMD of the control group was reduced. Zhao, Zhang, and Tian (2007) indicated that exercising and receiving calcium have a great effect on subjects’ bone density. In another study investigating the effect of exercising on bone density, body balance, and self-efficacy of women revealed that compared to the control group, bone density in the femur and body balance were significantly enhanced in the intervention group; however, self-efficacy of two groups was not changed (Jessup, Horne, Vishen, & Wheeler, 2003). Egbunike et al. (2009) investigated the effect of a 12-week exercise program on BMD of the neck, waist and femur in 70 women aged from 18 to 22 and indicated a significant increase in BMD of the waist, neck, and femur of studied subjects after intervention. Cohen et al. (2013) indicated that family-based intervention causes the enhancement of bone density of subjects. In a study of Pérez et al. (2013), educational intervention caused the increase of BMD in the intervention group. Results of Wen, Huang, Li, Chong, and Ang (2017) showed that after a 10-week intervention period, there were no significant changes in the BMD of both groups. In Warriner et al. (2012), 17.3% of the intervention group completed digital topological analysis (DTA) compared to 5/2% of the control group (12/1% difference). Results of Díaz-Correa et al. (Díaz-Correa, Ramírez-García, Castro-Santana, and Vilá (2014) showed that 61/6% of participants had a low level of knowledge about osteoporosis and they were less likely to receive osteoporosis consolation by care physicians, perform a BMD test, or take calcium and vitamin D supplements.
Conclusion
The results of the present study indicated that educational intervention based on the PRECEDE model leads to the increase of knowledge, attitude, self-efficacy, reinforcing and enabling factors, and consequently, promotion of prevention behaviors from osteoporosis and improvement of bone density of studied subjects. According to the vulnerability of women, social supports and enabling factors, such as the availability of educational contents, entertainment and sports facilities, and bone density evaluation centers, play an important role in prevention behaviors from osteoporosis. Presenting educational programs for family members, doctors, and health professionals, and also presenting educational contents via social media, are highly demanded. The results of the current study showed the importance of education regarding osteoporosis prevention in women and revealed that policy makers should provide osteoporosis prevention programs in all health centers. Such programs, if implemented regularly, might positively affect people’s health behavior and lifestyles.
In this study, referrals to one center were made for the intervention group and to another one for the control group. It would be better if referrals to both centers were divided into two groups.
Footnotes
Acknowledgements
The authors wish to express their gratitude to the Department of Research and Technology of Fasa University of Medical Sciences for their financial supports and also all the participants for their contribution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Department of Research and Technology of Fasa University of Medical Sciences, Fasa, Iran.