
Abstract
This qualitative systematic review synthesizes recent qualitative studies of culturally tailored interventions to better understand the experiences that individuals who are members of ethnic minorities have when undergoing type 2 diabetes treatment in the United States. Such interventions have been shown to be effective among ethnic minority populations; however, no qualitative synthesis has reported on recent findings from studies of these interventions. This systematic review identified seven relevant qualitative studies from five electronic databases—CINAHL, PsycINFO, PubMed, Ovid, and Web of Science—published from 2009 to 2019, and used a thematic synthesis review methodology. Methodological rigor was assessed for an appraisal of study quality. Five themes were identified as experiences of culturally tailored diabetes interventions: culturally appropriate healthy lifestyle behaviors, knowledge about diabetes care, emotional supports, access to the healthcare system, and family involvement. The findings of this review can be utilized as resources for improving diabetes care for ethnic minorities.
Keywords
Introduction
In the United States, diabetes mellitus is the seventh-leading cause of death (Centers for Disease Control and Prevention [CDC], 2019), and type 2 diabetes (T2DM) is the most unequally treated chronic disease afflicting ethnic minorities (Murdoch-Flowers et al., 2019). Indeed, compared with non-Hispanic whites, who are diagnosed with T2DM at a rate of 7.4% (CDC, 2017a), in ethnic minority populations T2DM is prevalent: among Hispanics, the same rate is 12.1%; Asian Americans, 8.0%; and African Americans, 12.7%. These same ethnic minorities have increased mortality rates as a result of T2DM, too (CDC, 2017b). They are also disproportionately underserved by healthcare services (Joo, 2014; Lagisetty et al., 2017), even though they account for high medical expenditures (American Diabetes Association, 2018; Lagisetty et al., 2017). Because of English language deficiency or financial constraints, they suffer limited access to healthcare systems.
Culturally tailored diabetes programs are an important strategy to overcome these health inequities, prevent diabetes complications, and improve care for ethnic minorities (Joo, 2014; Lagisetty et al., 2017). Culturally tailored interventions operate by “employing the native language, integrating cultural dietary preferences, encouraging family participation and support, and holding open discussions of cultural beliefs and treatment practices for diabetes (e.g., home remedies, oriental medicine)” (Choi & Rush, 2012, p. 379). By paying attention to patients’ needs and cultural values, considering patients’ language needs and literacy levels, and educating patients about diabetes self-management, culturally tailored diabetes interventions represent patient-centered care (Brunk, Taylor, Clark, Williams, & Daniel, 2017; Lagisetty et al., 2017).
Several clinical trials of culturally tailored interventions have evaluated their impact on diverse ethnic minorities with T2DM (Choi & Rush, 2012; Hu, Wallace, McCoy, & Amirehsani, 2014). A systematic review found evidence that culturally tailored interventions for minorities in high-income countries are effective and efficient (Attridge, Creamer, Ramsden, Cannings-John, & Hawthorne, 2014). Another systematic review of culturally tailored diabetes interventions with Asian American cultures are also effective (Joo, 2014). These interventions demonstrated improved blood sugar control, increased self-care skills, and increased diabetes knowledge (Attridge et al., 2014; Choi & Rush, 2012; Joo, 2014). Studies have also explored ethnic minorities’ perceptions to identify factors that might help them control their T2DM (Joo & Lee, 2016; Shiyanbola, Ward, & Brown, 2018; Zamudio, Sanchez, Altschuler, & Grant, 2017). The factors such as bilingual healthcare professions and bilingual educational programs that were identified were recommended for culturally tailored programs.
To date, however, no study has analyzed and synthesized the experiences that ethnic minority groups in the Unites States actually have with culturally tailored T2DM interventions. What the ethnic groups undergoing interventions thought about their culturally tailored diabetes interventions is unclear. To further improve these interventions, it is crucial to identify the common perceptions minority groups have about the interventions they experience.
Aim
The aim of this study was to systematically review empirical qualitative studies that presented findings about the experiences and perceptions that ethnic minorities in the United States with type 2 diabetes (T2DM) had about culturally tailored interventions. The research question was “What recent qualitative evidence exists of the experiences and perceptions that ethnic minorities in the United States have of culturally tailored diabetes interventions?”
Methods
Study Design
This study used a qualitative systematic review protocol that employs thematic synthesis (Thomas & Harden, 2008). A review protocol is composed of the following: (1) choose a topic and aim, (2) review the literature using keywords and search terms, (3) assess the critical appraisal with retrieved literature, (4) extract data, assemble the findings, and synthesize themes, and (5) publish the results (Thomas & Harden, 2008). A qualitative systematic review is a relatively new and rapidly developing methodology in nursing research that synthesizes common themes from evidence that may be useful in nursing practice (Butler, Hall, & Copnell, 2016; Ring, Ritchie, Mandava, & Jepson, 2010). To ensure systematic reporting, this review followed the PRISMA statement (Moher, Liberati, Tetzlaff, Altman, The PRISMA Group, 2009) and the PICO framework (Robinson, Saldanha, & McKoy, 2011).
Search Strategy
Five electronic databases—CINAHL, PsycINFO, PubMed, Ovid, and Web of Science—were used to search recent empirical qualitative studies published between January 2009 and February 2019: CINAHL (2009-2019), PsycINFO (2010-2019), PubMed (2009-2019), Ovid (2009-2018), and Web of Science (2009-2019). To ensure an accurate database search, the search was initially performed in February 2019 and then repeated in March 1, 2019. The following keywords and Medical Subject Headings (MeSH) terms with operators were combined in the search: (“culturally tailored” or “culturally appropriate” or “culturally targeting”) and (“qualitative research” or “qualitative study” or “focus group” or “interview”) and (“diabetes mellitus” or “type 2 diabetes”) and (“immigrants” or “ethnic minority”). The following additional search terms were also used: (“experience” or “perception”) and (“education” or “program”)
Inclusion and Exclusion Criteria
This qualitative systematic review adopted the PICO (Participant, Phenomenon of Interest, Context, Outcome) framework (Pettigrew & Roberts, 2005). In this study, “Participant” refers to adults who are members of an ethnic minority with T2DM living in the United States, “Phenomenon of Interest” refers to culturally appropriate diabetes care, “Context” refers to culturally tailored diabetes interventions, and “Outcome” means perceptions and experiences of diabetes care during culturally tailored interventions.
Included literature were English language studies published in peer-reviewed journals that (1) represented primary research, (2) studies that were qualitative or used mixed methods, (3) included individuals with T2DM and identifying as ethnic minorities who live in the United States, (4) focused on culturally tailored interventions for T2DM, and (5) included participants’ experiences while participating in the interventions.
Excluded literature were studies that focused on prediabetes interventions for ethnic minorities, targeted populations that were not ethnic minorities or that had other diseases, reported healthcare providers’ experiences, and reported practical recommendations regarding culturally tailored interventions.
Study Selection and Quality Appraisal
Figure 1 illustrates the study screening and selection process, which was conducted by the first author and double-checked by the second author. The initial electronic database search identified 212 studies; 67 of these remained after duplicates were removed. Screening of abstracts excluded 55 further studies. Five more studies were excluded after full-text review because they did not meet the inclusion criteria. The seven studies that remained were then assessed for eligibility.
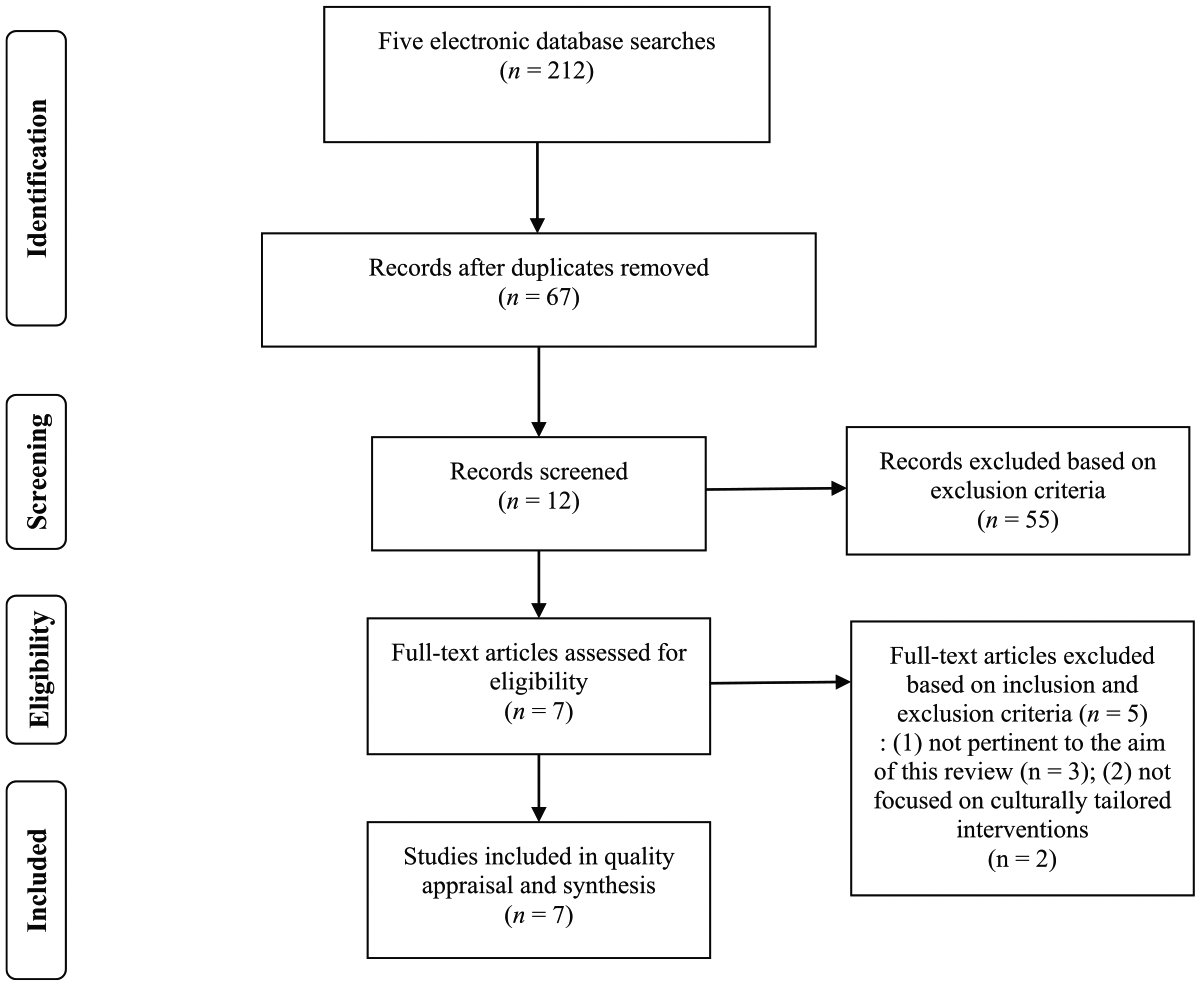
PRISMA flow chart of screening and selection process.
This study used the Critical Appraisal Skills Programme Qualitative Research Checklist (2013) to assess the studies’ methodological rigor and trustworthiness (Critical Appraisal Skills Programme, 2013). With 10 questionnaires, the checklist assesses a qualitative study’s aim, sampling method, ethics, data collection and analysis process, and findings. Each author independently appraised each study’s methodological rigor using the tool; the authors then compared the results. The authors reached a consensus that all included studies have high methodological rigor (see Table S1).
Data Extraction and Synthesis
Table 1 is a summary table that was constructed by the first author to extract data from the included studies; the second author checked the table for accuracy. The table includes the following information about the studies: author(s) and year of publication; research discipline, research design, and setting of the study; study aim; sample, sample size, mean age of sample, and sampling method; data collection methods; data analysis technique and theoretical framework; and major findings.
Summary of Studies Included in the Review.
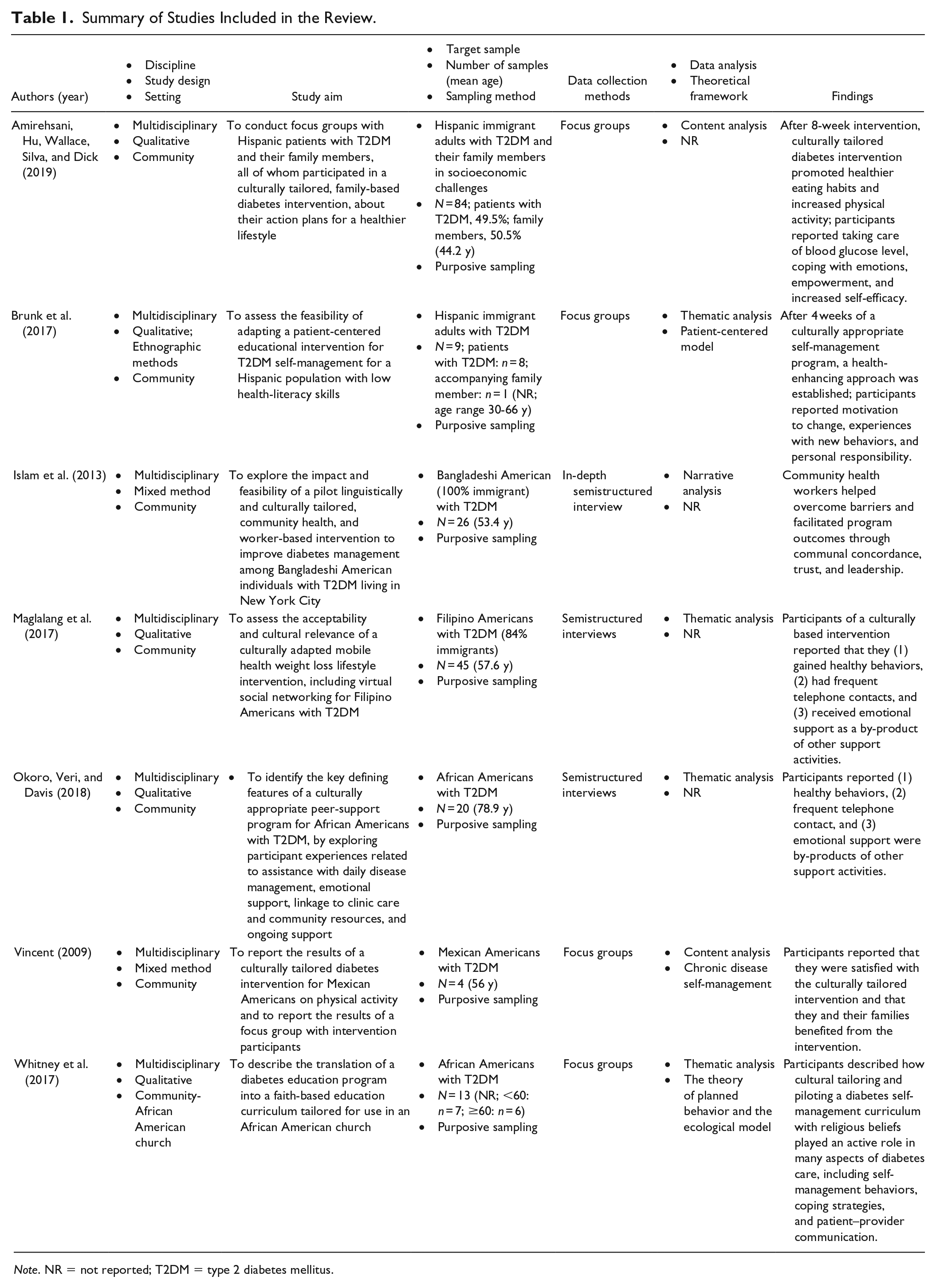
Note. NR = not reported; T2DM = type 2 diabetes mellitus.
This review employed thematic analysis/synthesis (Thomas & Harden, 2008), a process useful for identifying important themes from existing qualitative data. The process first identifies and codes recurrent themes in qualitative data. Second, prominent and significant themes based on similarity are aggregated and organized hierarchically. Finally, higher and more comprehensive themes are generated (Thomas & Harden, 2008). The first author conducted the initial analysis and synthesis, and the second author confirmed the results, which are presented in Table 2.
Summary of thematic analysis.
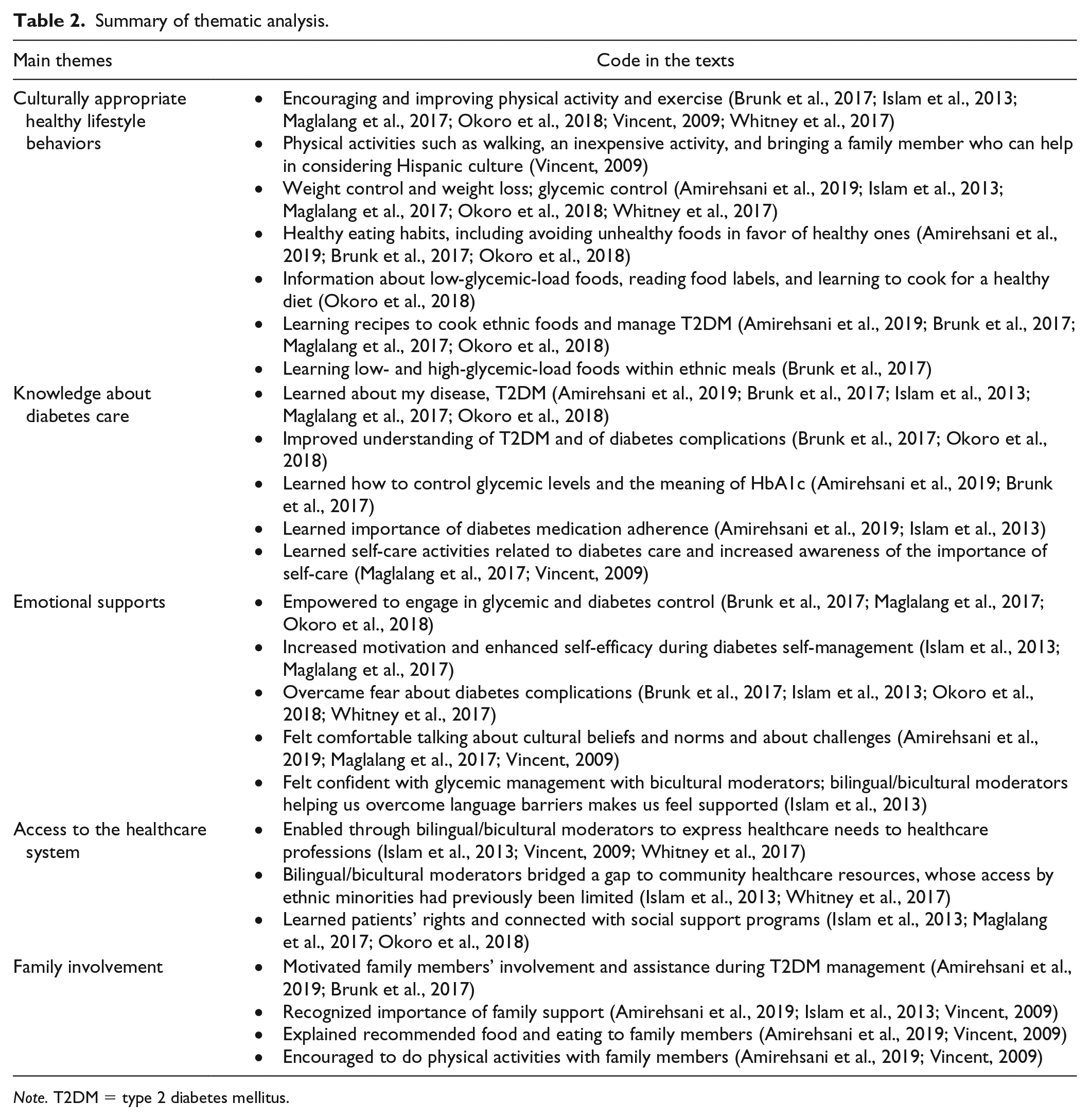
Note. T2DM = type 2 diabetes mellitus.
Results
Study Characteristics
Table 1 summarizes characteristics of the seven included studies (Amirehsani et al., 2019; Brunk et al., 2017; Islam et al., 2013; Maglalang et al., 2017; Okoro et al., 2018; Vincent, 2009; Whitney et al., 2017). All studies were published between 2009 and 2019, five since 2017.
The studies included 201 total participants (Hispanic: 48%; Filipino American: 22%; African American: 16%; and Bangladeshi American: 14%). All participants of the seven studies were adults (approximate age range: 30-79 years) who were diagnosed with T2DM. In several of the studies, all participants were immigrants to the United States; one study included as participants both immigrants and individuals born in the United States but identifying as an ethnic minority (Maglalang et al., 2017). Five studies were qualitative studies, and two were mixed method. For data collections, four studies used focus groups and three used semistructured individual interviews. Four studies’ data were collected in participants’ original language (such as Spanish or Bengali) by bilingual researcher or moderators. These data were then translated in English for analysis (Amirehsani et al., 2019; Brunk et al., 2017; Islam et al., 2013; Vincent, 2009). Other studies, whose participants were African Americans and Filipino Americans, collected data in English (Maglalang et al., 2017; Okoro et al., 2018; Whitney et al., 2017). Four studies used thematic synthesis for their qualitative analysis (Brunk et al., 2017; Maglalang et al., 2017; Okoro et al., 2018; Whitney et al., 2017). Only three studies demonstrated a theoretical framework that they utilized for their studies (Brunk et al., 2017; Vincent, 2009; Whitney et al., 2017). No studies connected study results to a theoretical model. One study author’s research discipline was nursing (Vincent, 2009); the rest were multidisciplinary healthcare majors (n = 6).
Culturally Tailored Diabetes Interventions
All participants of the studies received culturally tailored diabetes interventions in community-based settings, such as community health centers or churches. Types of interventions included diabetes management programs such as self-management education and programs supporting healthy behavior. These interventions prioritized ethnically and culturally appropriate content and were person centered, considering such things as literacy levels, ethnic foods, and traditional remedies. One study utilized a telehealth with smartphone application for delivering its intervention (Maglalang et al., 2017), and another applied a peer-support system with phone calls (Okoro et al., 2018). All seven studies included glucose self-monitoring, dietary guidance education, informative health services, and continuous follow-up services to meet patient needs.
Interventions were delivered by research staff, healthcare professionals, or community health workers trained in bilingual/bicultural communication (Amirehsani et al., 2019; Brunk et al., 2017; Islam et al., 2013; Vincent, 2009). One study employed a bilingual certified diabetes educator for their education sessions (Vincent, 2009). Intervention durations varied, but they ranged from 4 weeks to 6 months. Some studies not only invited T2DM patients to participate but also enlisted family members in intervention sessions to support T2DM patients (Amirehsani et al., 2019; Vincent, 2009).
Five themes emerged from the thematic synthesis of the studies: (1) culturally appropriate healthy lifestyle behaviors, (2) knowledge about diabetes care, (3) emotional supports, (4) access to the healthcare system, and (5) family involvement (see Table 2).
Theme 1: Culturally Appropriate Healthy Lifestyle Behaviors
The first theme identified from the studies was that interventions employed culturally appropriate healthy lifestyle behaviors. Healthy lifestyle behaviors refer to healthy eating habits, cooking for weight control, and regular exercise (Maglalang et al., 2017; Okoro et al., 2018).
Four studies informed participants about healthy meals; warned against eating unhealthy foods, including unhealthy fats; and encouraged them to adopt healthy eating habits (Amirehsani et al., 2019; Brunk et al., 2017; Maglalang et al., 2017; Okoro et al., 2018; Vincent, 2009). Participants said they tried to quit junk food and sodas, substituting them with healthier foods, such as fresh vegetables and salads (Amirehsani et al., 2019; Brunk et al., 2017; Maglalang et al., 2017). In Brunk et al. (2017), one Hispanic participant said that “I have learned to eat better” (p. 192). Some studies reported that participants reduced portion sizes after interventions and were advised to read food labels (Amirehsani et al., 2019; Okoro et al., 2018; Vincent, 2009).
During the interventions’ cooking demonstrations, participants were advised about more than just healthy lifestyle behaviors; the nutrition and food-consumption information that would help participants control their glucose was culturally appropriate (Amirehsani et al., 2019; Brunk et al., 2017; Okoro et al., 2018). One participant in Okoro et al. (2018) said, “Eating and cooking, she [intervention moderator] tells you not to eat as much grease and bake mostly, or boil it” (p. 340). Hispanic participants in Amirehsani et al. (2019) were encouraged to stay away from fried tortillas.
Participants were also advised to adopt culturally appropriate physical activities for their health and weight control. In Amirehsani et al. (2019), participants reported that they would increase the number of hours they spent walking. Participants in Vincent (2009), considering their own economic status and culture, noted they could adopt walking and dance strategies and proposed to adopt walking because it is inexpensive (Vincent, 2009). Bangladeshi American participants in Islam et al. (2013) improved their health through gender-specific and home-based physical exercise.
Theme 2: Knowledge About Diabetes Care
Participants in all seven studies, who said they had little knowledge about T2DM before interventions, reported that they learned something new about diabetes—specifically, principles of glycemic control. These reports represent the second theme: disseminate knowledge about diabetes care.
Before interventions, participants said that they “lack . . . knowledge” about the meaning of glucose level and HbA1c (Amirehsani et al., 2019; Brunk et al., 2017). From the interventions, however, participants reported that they learned more about the disease from educational sessions, including the importance of glucose monitoring and the complications that can arise from diabetes. As one participant in Whitney et al. (2017) observed, “Knowledge is power and when we started coming to the . . . classes . . . most of us didn’t know about testing . . . what our sugar count was or whether it was high or low, we’re just eating and we didn’t know” (p. 12). Several studies employed bilingual moderators in their educational services and were sensitive to language and literacy levels when conveying terminology related to diabetes care. One participant in Brunk et al. (2017) said, “I learned a lot of things. And that sheet with the [picture of the] woman and complications [of diabetes] helped me understand a lot” (p. 190).
Some studies reported that participants became more aware of self-care requirements such as adhering to diabetes medication. In Amirehsani et al. (2019), participants stated that they planned to take medication regularly for diabetes “to change my attitude and take my medicine like I am supposed to” (p. 91). In other studies, participants said that they had more knowledge of and skill with diabetes self-care (Maglalang et al., 2017; Vincent, 2009).
Theme 3: Emotional Supports
Providing emotional support, a feature of all the studies under review, is the third theme that emerged as a theme of culturally tailored diabetes interventions. In most of the studies, participants described feeling motivated, supported, and empowered in their diabetes care while receiving the services. Participant engagement with intervention moderators for glycemic control empowered participants and motivated them to control their own T2DM (Brunk et al., 2017; Maglalang et al., 2017). In addition to increasing self-efficacy, empowerment helped participants cope with stress. In Maglalang et al. (2017), participants expressed that a service utilizing a smartphone application was very helpful and that they felt supported by it. In Whitney et al. (2017), African American participants said that the culturally tailored interventions combined with the church-based spiritual supports they received helped them “weather” their stress regarding diabetes care and overcome their fear of diabetes complications. Also, participants reduced their anxiety and anger and said they were able to control both more than before (Amirehsani et al., 2019; Brunk et al., 2017). One patient in Amirehsani et al. (2019) said, “My life already changed since I started coming to these meetings” (p. 91) and “This program had helped me a lot . . . Well, I feel better. I don’t feel like I used to” (p. 93). In Okoro et al. (2018), African American participants said they felt emotionally supported to have someone to talk to about their symptoms: “I was going through some mental stuff and she talked to me, talked me down and got me started going to see somebody about the problems that I was having so it’s working out really well because I do feel better” (p. 5).
Some participants noted that they felt comfortable with the programs because of the bilingual/bicultural moderators (Islam et al., 2013). With these moderators, participants whose first language is not English or who had limited English fluency did not feel hindered by language barriers (Islam et al., 2013). Participants communicated their cultural beliefs and concerns regarding diabetes care the bicultural moderators (Islam et al., 2013; Maglalang et al., 2017; Okoro et al., 2018; Vincent, 2009). One participant in Maglalang et al. (2017) said, “People [intervention moderators] are aware of the culture. I don’t have to explain” (p. 148).
Theme 4: Access to the Healthcare System
Participants in five of the studies said the culturally tailored diabetes interventions facilitated their access to the healthcare system (Islam et al., 2013; Maglalang et al., 2017; Okoro et al., 2018; Vincent, 2009; Whitney et al., 2017). This access is therefore the fourth theme of the studies under review.
According to Islam et al. (2013), before intervention, participating ethnic minorities had limited access to healthcare system. However, participants were coached how to ask questions of their healthcare providers (Islam et al., 2013; Maglalang et al., 2017). Participants said that they learned to express their symptoms and healthcare needs to their physicians (Islam et al., 2013). Participants said that they had a “gap” of access to the healthcare system before, but their bilingual moderators “bridged the gap” to healthcare resources (Islam et al., 2013). Bicultural moderators helped to deliver participants’ concerns about diabetes care and fulfilled healthcare needs (Vincent, 2009). In addition, participants were informed of community healthcare centers and social resources they can use for their diabetes care (Vincent, 2009; Whitney et al., 2017).
Theme 5: Family Involvement
The fifth theme, family involvement, emerged from five of the studies (Amirehsani et al., 2019; Brunk et al., 2017; Islam et al., 2013; Maglalang et al., 2017; Vincent, 2009). Participants said that culturally tailored interventions facilitated family members’ support and assistance for their diabetes care (Amirehsani et al., 2019; Islam et al., 2013; Vincent, 2009). Brunk et al. (2017) reported that family members’ assistance is necessary to control diabetes. For example, because healthy eating is a key factor in T2DM treatment, sharing dietary information with family members encouraged the participants to improve diabetes management. As participants in Amirehsani et al. (2019) observed, “family can help by not eating a lot in front of us,” and they vowed “to try harder to live better with our families and to tell them what we are learning, what foods are good and what foods are bad” (p. 91). One participant in Vincent (2009) noted that “I explain to them (family) why they have to eat less, or why they have to eat another type of food, and in reality it’s the same food, only that it’s being prepared differently, healthier” (p. 525).
Some studies encouraged participants to do physical activity with their family members. For example, Vincent (2009) provided culturally appropriate exercise programs that involved family members at home. A participant in Amirehsani et al. (2019) noted, “I’m planning to go to the park at least three times a week with my daughters now that it is good weather and exercising with them. It could be beneficial for them too” (p. 92). Participants even suggested including family members in the interventions’ educational programs (Amirehsani et al., 2019).
Discussion
This study’s aim was to synthesize ethnic minorities’ experiences with and perspectives on culturally tailored diabetes programs, as reported in qualitative research studies in the United States published between 2009 and 2019. The seven included studies involve adult participants in the United States, all of whom were members of ethnic minorities, such as Hispanic immigrants, African Americans, Bangladeshi- and Filipino-Americans; and all of whom had been diagnosed as having T2DM for more than 1 year. Across the populations and studies, five themes emerged from the evidence of the experiences and perceptions that ethnic minorities in the United States have of culturally tailored diabetes interventions: culturally appropriate healthy lifestyle behaviors, knowledge about diabetes care, emotional supports, access to the healthcare system, and family involvement.
First, it was known that improving lifestyle behaviors is important for T2DM care. For example, regulation of diet was key for glucose controls with T2DM ethnic minorities (Joo & Lee, 2016). The physical activities and efforts to regulate body weight that participants were encouraged to do also aligns with other systematic reviews and with randomized controlled trials that show evidence of culturally tailored diabetes programs effectively controlling weight control and having significant impact on HbA1c with ethnic minorities (Leake, Bermudo, Jacob, Jacob, & Inouye, 2012; Song et al., 2010). This qualitative review adds evidence that healthy lifestyle behaviors were perceived by ethnic minority participants as valuable.
Second, participants in the studies perceived themselves as becoming more informed about their disease, T2DM, and about the complications that can result from it. Specifically, participants said that they gained knowledge about glucose levels, HbA1c, and medication adherence from educational sessions. Ethnic minorities receive disproportionately less disease information than people in majorities; thus, they have little knowledge about disease information (Joo, 2014). Several clinical trials of culturally tailored diabetes programs among immigrants reported that knowledge of diabetes improved with a diabetes knowledge test tool from the baseline (Choi & Rush, 2012; Hu, Amirehsani, Wallace, McCoy, & Silva, 2016; Sun, Tsoh, Saw, Chan, & Cheng, 2012). Evidence from this study suggested that certified and bilingual diabetes educators were key factors in the success of culturally tailored interventions. Increase knowledge about diabetes results in increased self-care by participants (Joo, 2014).
The third theme this review identified was emotional supports. Many participants of the studies said that they were motivated and empowered. They also said they had close relationships with their bilingual/bicultural intervention moderators. A close relationship with moderators makes it possible to overcome fear of diabetes. Finally, participants said they felt confident in managing T2DM and not only satisfied with the interventions, but also thankful for them. This qualitative result aligns with earlier descriptive studies that reported that ethnic minorities highly valued emotional aids (Brown, Garcia, Kouzekanani, & Hanis, 2002; Hu et al., 2014). The emotional supports participants reported demonstrate the value of culturally tailored diabetes interventions.
Fourth, study participants reported improved access to the healthcare system. Participants highlighted that moderators helped them find community healthcare resources and that the culturally tailored interventions acted as a bridge to the healthcare system. Appropriate referral services to community resources and healthcare providers has been noted as key factor of health promotion to minority populations (Lagisetty et al., 2017). This review adds that bilingual/bicultural moderators acted as advocates for study participants.
Finally, participants in the studies reported family involvement in their interventions. As the meaning of cultural tailoring (Choi & Rush, 2012), studies reported that family support and participation were encouraged. Previous research has shown that minorities participating in family-based diabetes interventions improved their physical activity levels and had a positive impact on glycemic controls (Brown & Hanis, 2014; Hu et al., 2016).
Some recommendations stemming from the included studies were identified. In three studies, participants reported insufficient time to adopt culturally tailored strategies (Amirehsani et al., 2019; Maglalang et al., 2017; Vincent, 2009). Because participants were unaccustomed to the taste of the healthy foods that intervention moderators recommended (Amirehsani et al., 2019; Maglalang et al., 2017; Vincent, 2009). Thus, it is recommended that future interventions provide enough time to adjust to the recommended dietary changes.
In addition, two studies reported low retention rates. Some participants noted difficulty regularly attending intervention programs and found it hard to complete education sessions due to irregular work schedules (Islam et al., 2013; Maglalang et al., 2017). Culturally tailored interventions need to consider participant access and make an effort to ensure minority retention in the programs.
Review Limitations
There are some limitations to this qualitative systematic review. First, this review only included journal articles published in English; studies published in other languages and doctoral dissertations were excluded. Second, this review only included qualitative studies that were conducted in the United States between 2009 and 2019. Third, participants in the included studies were mixed, including ethnic minorities born in the United States as well as foreign-born immigrant populations. The included ethnic minorities could not represent all ethnic minorities living in the United States. Fourth, the included studies did not consider educational level or socioeconomic status of their study participants. Fifth, the limited number of qualitative studies under review and the limited number of ethnic minorities means the results may not be generalizable to all ethnic minorities living in the United States. Finally, retrieved studies focused on positive aspects of culturally tailored diabetes interventions with focus groups and individual interviews. Thus, studies might have a reporting bias.
Implications for Nursing Practice, Research, and Healthcare Policy
Culturally tailored diabetes support programs are promising interventions for ethnic minority populations. During diabetes management, nurses and other healthcare professions should be aware of cultural values and should sensitively listen to the healthcare needs those populations express. Finally, they should provide bilingual and bicultural healthcare when it is needed.
Future qualitative research into culturally tailored interventions should identify and develop a theoretical framework for improving and strengthening the intervention. Only three of the studies in this review applied a theoretical model to their study, and none developed a model or framework. Second, to ensure culturally tailored programs are widely accepted and applied to underserved populations, they should adopt the American Diabetes Association standards and National Diabetes Education Program guidelines. Only one study applied the American Diabetes Association standards to their intervention (Vincent, 2009).
This qualitative systematic review synthesized ethnic minorities’ experiences with and perspectives on culturally tailored diabetes programs from seven qualitative studies with a limited range of minority populations that were conducted in the United States. There is some qualitative research evidence on culturally tailored interventions for ethnic minorities from other countries such as the Netherlands and United Kingdom (Jager, van der Sande, Essink-Bot, & van den Muijsenbergh, 2019; Wilkinson & Randhawa, 2012). To better understand intervention implementation, future studies are recommended with a greater diversity of ethnic groups of the world.
Interventions in the studies in this review were delivered by bilingual moderators, such as community health workers and bilingual research staff. To ensure study rigor, it is recommended that future interventions be delivered by culturally competent healthcare providers, such as certified diabetes educators. Second, it is recommended that future qualitative studies and reviews capture the experiences of bicultural healthcare providers when delivering culturally tailored interventions. This will contribute to overall understanding of culturally tailored intervention implementation. In addition, some studies utilized telehealth for delivery of culturally tailored programs. Additional research into the use of telehealth to demonstrate its impact with ethnic minorities’ health is recommended.
Healthcare policymakers and healthcare researchers should consider the value culture plays in ensuring ethnic minorities’ quality of care. More research funding should be made available to clearly demonstrate the effectiveness of culturally tailored projects. Finally, the themes identified in this qualitative systematic review need to be considered as resources for improving diabetes care to ethnic minorities.
Conclusion
This qualitative systematic review is the first study to synthesize the experiences that individuals in the United States with T2DM who are members of ethnic minority cultures have when participating in culturally tailored interventions. This study identified how these individuals experienced the interventions as culturally sensitive, emotionally supportive, and person centered. Nurses and other healthcare professions, nursing researchers, diabetes educators, and healthcare policymakers should consider adopting such interventions when designing and evaluating diabetes intervention programs for ethnic minorities.
Supplemental Material
2019-09-17_Supplementary_file_2_search_terms_and_search_strategy_CNR-L-19-193.R2 – Supplemental material for Experience of Culturally-Tailored Diabetes Interventions for Ethnic Minorities: A Qualitative Systematic Review
Supplemental material, 2019-09-17_Supplementary_file_2_search_terms_and_search_strategy_CNR-L-19-193.R2 for Experience of Culturally-Tailored Diabetes Interventions for Ethnic Minorities: A Qualitative Systematic Review by Jee Young Joo and Megan F. Liu in Clinical Nursing Research
Supplemental Material
2019-09-17_Supplement_file_TableS1_qualitative_appraisal_CNR-L-19-193.R2 – Supplemental material for Experience of Culturally-Tailored Diabetes Interventions for Ethnic Minorities: A Qualitative Systematic Review
Supplemental material, 2019-09-17_Supplement_file_TableS1_qualitative_appraisal_CNR-L-19-193.R2 for Experience of Culturally-Tailored Diabetes Interventions for Ethnic Minorities: A Qualitative Systematic Review by Jee Young Joo and Megan F. Liu in Clinical Nursing Research
Footnotes
Author Contributions
Study design: JYJ
Data collection, analysis, and synthesis: JYJ, MFL
Manuscript writing: JYJ
Critical revisions for important intellectual content: JYJ, MFL
Study supervision: JYJ, MFL
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Research Foundation of Korea(NRF) grant (2018R1C1B5029635).
Ethical approval
Because no human subjects were engaged in this study, no Institutional Review Board approval was required.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.