
Abstract
The aim was to determine whether 24-hour urine sodium excretion predicted event-free survival of patients with heart failure (HF) and diabetes mellitus (DM). Twenty-four hour urine sodium, as an indicator of dietary sodium, was collected from 107 patients with HF and comorbid DM. Patients were followed for a median period of 337 days to determine time to the first event of either all-cause hospitalization or cardiac-related mortality. There were 44 patients (41%) who had an event of death or hospitalization. Cox regression showed that higher urine sodium (>3.8 gm/day) was associated with 2.8 times greater risk for an event than lower urine sodium after controlling for age, gender, New York Heart Association class (I/II vs. III/IV), left ventricular ejection fraction, and body mass index. These data suggest that dietary sodium restriction may be beneficial for patients with HF and DM.
Heart failure (HF) is a chronic, progressive condition, associated with frequent hospitalization and emergency department visits with high mortality rates (Benjamin et al., 2018). In the United States, more than a million patients are annually discharged after hospitalization for decompensated HF, with 21% of those patients rehospitalized within 30 days (Akintoye et al., 2017; Davis et al., 2017). The prognosis of patients who are hospitalized for HF is poor, with 31% dying within 1 year after the first hospitalization (Chang et al., 2018). Presence of comorbid conditions is one of the main causes of poor prognosis in patients with HF (Ruiz-Laiglesia et al., 2014). Diabetes mellitus (DM) is the most common comorbid condition affecting as many as half of patients with HF (Chang et al., 2018; Ruiz-Laiglesia et al., 2014). Patients with HF and comorbid DM have about 1.5 times higher risk for all-cause or HF-related hospitalizations, readmissions, or death compared to those without DM (Dauriz et al., 2017).
Dietary sodium restriction is a commonly recommended self-management behavior for patients with HF to prevent fluid retention, hypervolemia, and exacerbation of HF symptoms (Lennie, Chung, & Moser, 2013). Presence of higher sodium intake in DM in patients with HF has been suggested to increase the risk of fluid retention, hypervolemia, and acute decompensated HF (Rosano, Vitale, & Seferovic, 2017). This may be explained by glucose having similar osmotic characteristics as sodium compounding fluid shifts from intracellular and extravascular spaces into intravascular space causing hypervolemia (Rosano et al., 2017). Previous investigators have supported the beneficial effect of dietary sodium restriction on mortality and hospitalization for acute decompensated HF that accounts around 40% of all HF hospitalization (Chang et al., 2018; Lennie et al., 2011; Michalsen, Konig, & Thimme, 1998). In most of these studies, DM was controlled in the analysis and thus, less is known about its contribution to outcomes in the presence of high sodium intake.
On the other hand, there is evidence to suggest that dietary sodium restriction may worsen the prognosis of people with DM (Ekinci et al., 2011; Ginsberg, 2000; Oh, Lee, Jun, & Lee, 2016). Lower dietary sodium intake in patients with DM has been demonstrated to adversely affect insulin resistance, blood glucose levels, and serum lipids, placing them at greater risk for cardiovascular complications (Ginsberg, 2000; Oh et al., 2016). Ekinci et al. (2011) found a significant association of low dietary sodium intake with increased all-cause and cardiovascular mortality and in a sample of patients with DM, half of who had a history of cardiovascular disease.
These previous studies, however, provide limited insight into whether reduced or increased dietary sodium intake have an adverse effect on the outcomes for the patients with HF and comorbid DM. Therefore, the aim of this study was to determine whether dietary sodium intake predicted event-free survival between patients with HF and DM.
Methods
Design and Sample
This was a secondary analysis of data obtained from our previous studies conducted between 2007 and 2010 (Lennie et al., 2011, 2018; Saleh, Wu, Salami, Yousef, & Lennie, 2018). The database consisted of 361 patients with HF who were recruited from outpatient clinics in the community hospitals or academic medical centers in Kentucky, Georgia, Indiana, and Ohio in the United States. A subsample of 107 patients who had HF and comorbid DM were included in this study. Eligibility criteria for inclusion were: (1) diagnosis of chronic HF with either preserved or reduced ejection fraction confirmed by a cardiologist, (2) diagnosis of DM, (3) on stable doses of HF medications, and (4) able to read and speak English. Exclusion criteria were: (1) referred for heart transplantation, (2) history of cerebral vascular accident or acute myocardial infarction within the previous 3 months, (3) terminal illnesses such as end-stage liver failure, (4) on maintenance peritoneal or hemodialysis, or (5) prescribed a diet other than for HF and DM.
Measurements of Variables
Demographic
Age, gender, marital status, and ethnicity were obtained by patient interview.
Body mass index
Body mass index (BMI) was expressed as the ratio of weight in kilograms divided by height in meters squared. Height was measured using a stadiometer and weight by a professional digital scale using standardized protocols (Saleh et al., 2017; Saleh, Elshatarat, et al., 2018).
New York Heart Association
New York Heart Association (NYHA) functional class was obtained by patient interview using a standardized form. Both interrater and intrarater reliabilities in classify patients among our samples were demonstrated previously (Lennie et al., 2018). Due to low frequency, patients who were in NYHA functional class I were combined with those who in functional class II and those in class III were combined with patients in functional class IV.
Other clinical characteristics
Prescribed medication therapy, left ventricular ejection fraction (LVEF), and serum sodium, cholesterol, triglyceride, low density lipoprotein, high density lipoprotein, and random blood sugar were collected by patients’ interview or medical record review.
Dietary sodium intake
Dietary sodium intake was estimated by measuring urinary sodium excretion (UNa) from a single 24-hour urine sample. The 24-hour UNa was measured in mmoles and converted to g (g = mmole × 22.99/1000). Twenty-four hour UNa is considered a valid estimate of dietary sodium intake. Approximately 90% of sodium intake is excreted in the urine over a 24-hour period under normal insensible perspiration conditions (McLean, 2014). The 24-hour UNa in patients with HF has been used as a predictor of cardiac-related hospitalization and mortality and successful self-management (Chung et al., 2006; Lennie et al., 2011).
Event-free survival
The outcome of this study was the combined end-point of time to the first event defined as all-cause hospitalization or cardiac-related mortality during the 12-month follow-up period. Data on the date and cause of hospitalization were obtained by monthly telephone contact with patients or their family members and their responses were confirmed by careful medical record review. In the case of death, family members or healthcare providers were contacted and all data were verified by review of hospital records and public death record.
Procedure
Institutional Review Board approval was obtained for this study from each participating site. Patients were referred by nurse practitioners to a research assistant. The research assistant verified the eligibility. Interested patients signed informed consent to participate after full detailed information about the study was provided. Participating patients completed a short demographic questionnaire and a face-to-face structured interview with a research assistant to determine NYHA functional class. Patients were then scheduled for home visits to provide specific written and verbal instructions about the 24-hour urine collection and all equipment needed for the procedure. Patients were instructed to continue their usual eating and drinking habits and to start collection after the first morning void and to continue collection for the next 24 hours with a final void the next morning. To ensure the adequacy of urine collections, patients were provided with a log to record the time and volume of each void and were contacted by phone calls on the first morning of urine collection to remind them with the procedure. Research assistants verified the adequacy of collections based on the logs record.
Statistical Analysis
SPSS software for Windows (version 25.0; IBM Corporation) was used to analyze the data. Patient characteristics were described using frequencies with percentages or means with standard deviations depending on the level of measurement. Patients were divided into low and high urinary sodium excretion based on the median split of the 24-hour UNa levels (3.8 gm/day). Comparisons between the low and high urinary sodium groups were accomplished using the 2-sample t test or ϰ2 test of association. Cox regression was used to determine the association between 24-hour urine sodium and event-free survival of the combined end-points of all-cause hospitalization or cardiac-related mortality after controlling for age, gender, BMI, LVEF, and consolidated NYHA classes. The Omnibus test of model coefficients based on chi-square test was used to determine whether the overall Cox regression model predicts the time to event. Confidence interval for the hazard ratios was obtained for all independent variables at 95% and α level was set a priori at 0.05.
Result
Patient Characteristics
Baseline demographic and clinical characteristics of patients are summarized in Table 1. The mean age of patients was 63 years (range = 33-85 years). Most patients were male, white, and married or cohabitating. Less than two thirds of patients were obese. Nearly half of patients were in NYHA functional class I or II, with an average LVEF of 35% (range = 13-79%). The majority of patients were prescribed angiotensin converting enzyme inhibitors, β-blocker, diuretics, and statins and around a quarter was prescribed angiotensin II receptor blocker, aldosterone antagonist, and nitrates. Patients predominantly used either oral hypoglycemic agents or insulin, while only 12% used a combination of both therapies. A greater proportion of patients in high urine sodium group were obese and prescribed aldosterone antagonist compared with those in the low urine sodium group.
Sample Characteristics.
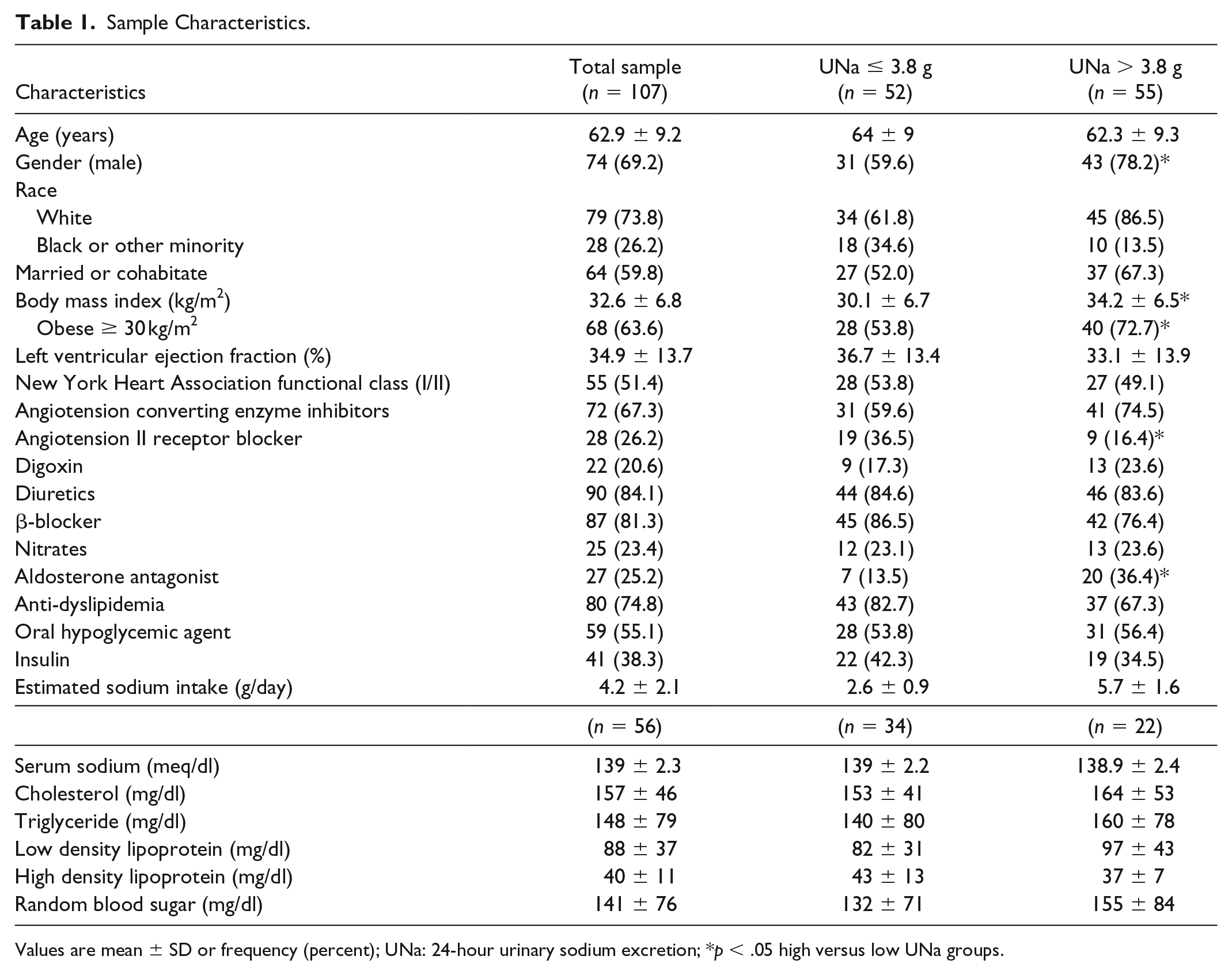
Values are mean ± SD or frequency (percent); UNa: 24-hour urinary sodium excretion; *p < .05 high versus low UNa groups.
24-hour UNa and Event-Free Survival
There were two deaths (2%) and 42 hospitalizations (39%) during median follow-up of 337 days (25th, 75th quartile; 117-401 days). A comparison of events between high and low urine sodium groups is presented in Table 2.
Event-Rates and Median Time to First Event for the Total Sample and Patients with Low and High Dietary Sodium Intake.
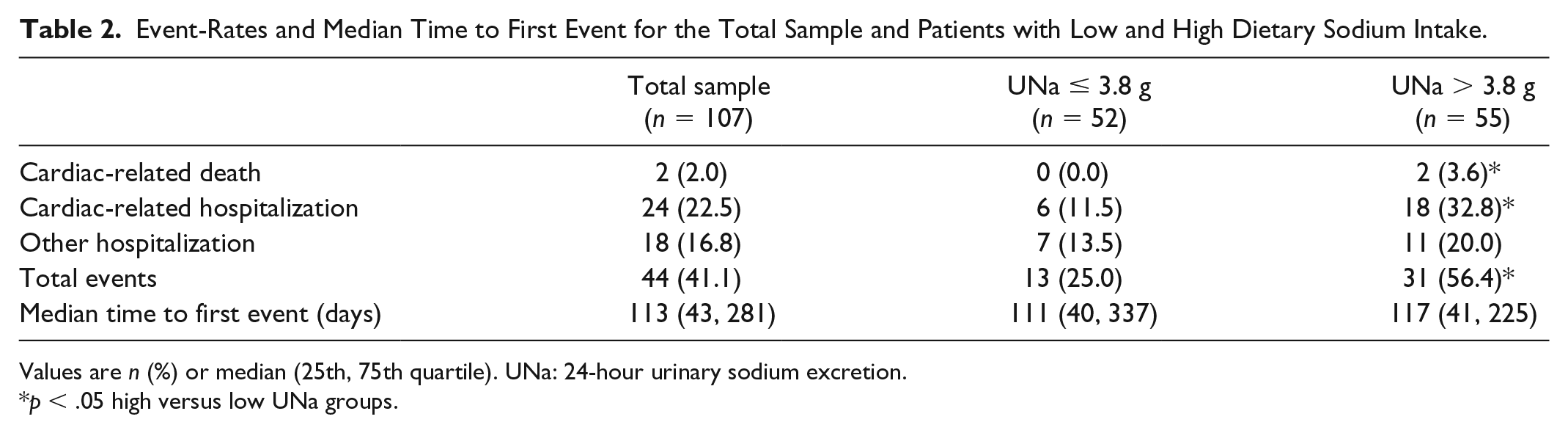
Values are n (%) or median (25th, 75th quartile). UNa: 24-hour urinary sodium excretion.
p < .05 high versus low UNa groups.
The chi-square of the Omnibus test of model coefficients was significant (ϰ2 = 19.04, p < .01) which indicated that the Cox regression model adequately predicted time to event (Figure 1). Patients in high urine sodium group had shorter event-free survival than patients in low urine sodium group (hazard ratio [HR] = 2.8, 95% confidence interval [CI] = 1.3-5.7) controlling for age, gender, BMI, LVEF, and NYHA functional class. NYHA was a significant predictor of time to all-cause hospitalization or cardiac-related death; whereas age, gender, BMI, and LVEF were not significant (Table 3). Patients in NYHA functional class III or IV were 2.4 more likely to experience an event compared with those in NYHA functional class I or II.
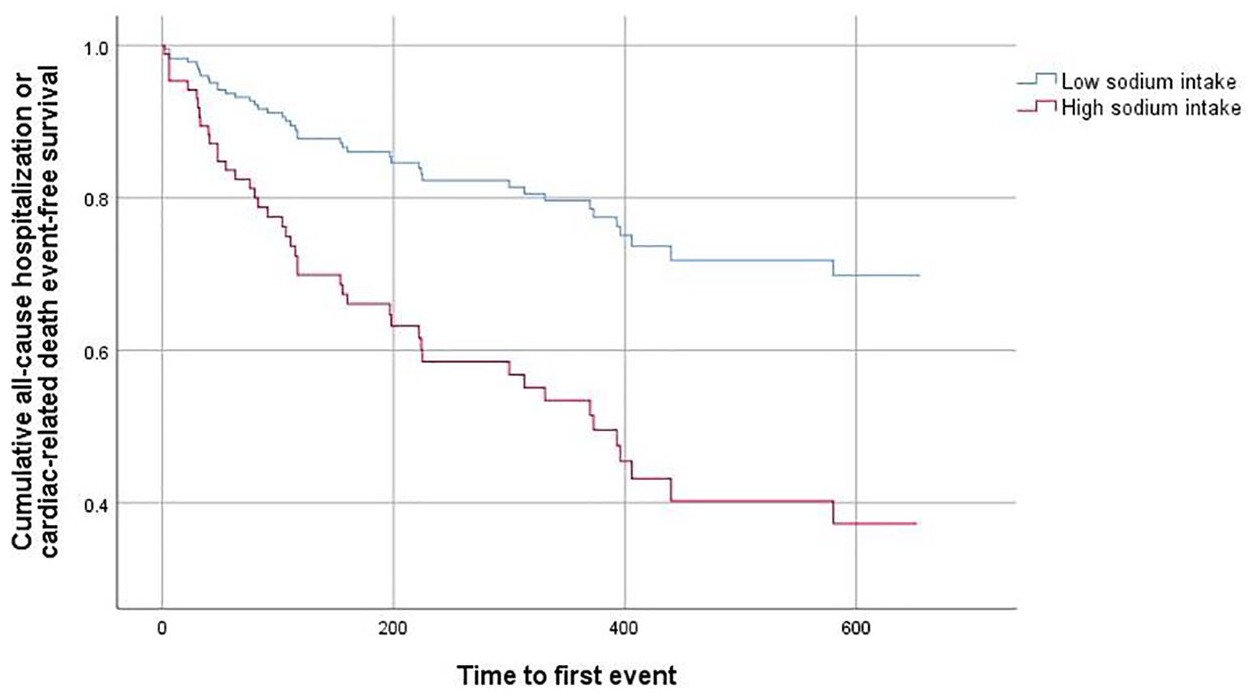
Cox regression for time to all-cause hospitalization or cardiac-related death between patients above and below the cut-point of 3.8 g for 24-hour urinary sodium excretion.
Cox Proportional Hazards Regression Model for Time to All-Cause Hospitalization or Cardiac-Related Death.
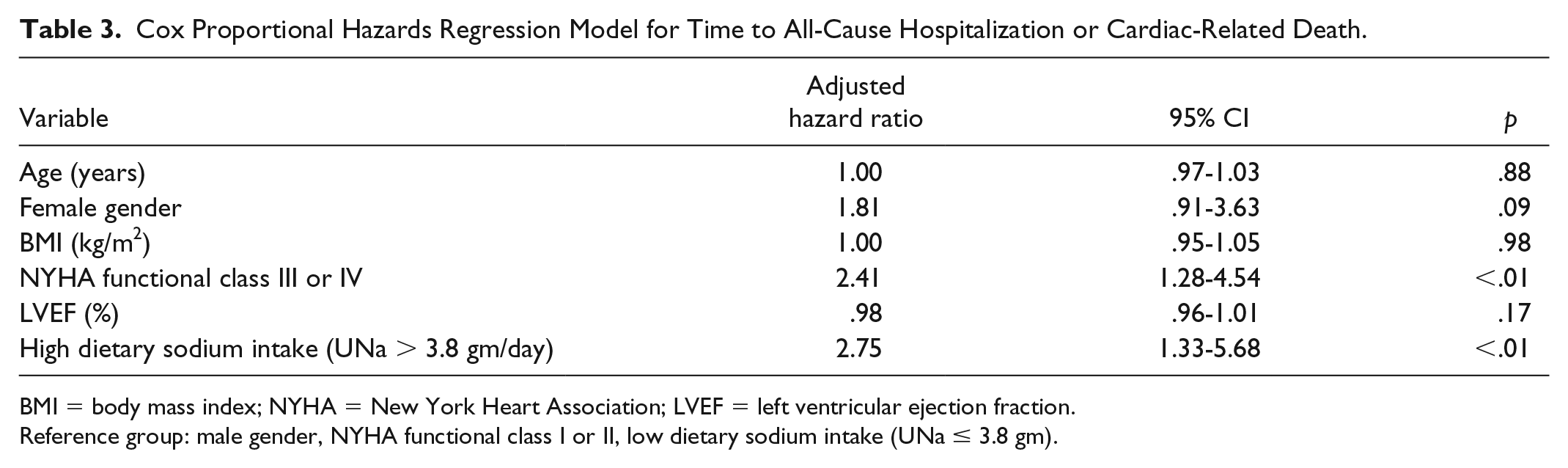
BMI = body mass index; NYHA = New York Heart Association; LVEF = left ventricular ejection fraction.
Reference group: male gender, NYHA functional class I or II, low dietary sodium intake (UNa ≤ 3.8 gm).
Discussion
This study demonstrated that high urine sodium excretion, as an indicator of dietary sodium intake, was associated with shorter time to all-cause hospitalization or cardiac-related mortality among patients with HF and comorbid DM. In previous studies showing higher sodium was associated with shorter event-free survival, in which comorbidities, including DM, were controlled (Arcand et al., 2011; Lennie et al., 2011; Song, Moser, Dunbar, Pressler, & Lennie, 2014). Thus, this is among the first studies to demonstrate that higher sodium intake was associated with shorter event-free survival in a population of patients with HF and comorbid DM.
Investigators in previous studies made comparisons among patients using sodium intake cut-points of 2.8 to 3 gm/day based on food diaries (Arcand et al., 2011; Song et al., 2014) and 24-hour UNa (Lennie et al., 2011). Our results were based on 24-hour UNa groups divided at a higher median split of 3.8 gm/day. This would suggest that the subpopulation of patients with HF and DM tended to consume foods high in sodium. There is limited evidence to support the current dietary sodium intake guidelines for either HF or DM management for all patients with HF. There are data to suggest that recommendations may vary among the various HF subpopulations (Lennie et al., 2011; Song et al., 2014). For example, dietary sodium intake of <3 gm/day was demonstrated to be associated with longer event-free survival only among patients in NYHA class III and IV, whereas, sodium intake of <2 gm/day was noticed to have no benefits for all patients with HF (Lennie et al., 2011; Song et al., 2014). Regardless, our results suggest that patients with HF and comorbid DM may benefit from dietary sodium restriction of <3.8 gm/day. Whether patients with HF and comorbid DM would benefit from a lower level of sodium intake, similar to the nutritional guidelines for DM or HF management will need further investigation.
A large number of patients with high urine sodium in our study were obese compared with those with lower urine sodium. Although obesity is a risk factor of cardiovascular disease and DM, it was demonstrated to have a paradoxical protective effect against several pathological consequences associated with cardiovascular disease or DM (Hainer & Aldhoon-Hainerová, 2013; Voulgari et al., 2011). Studies on patients with established HF or those with DM and without heart disease confirmed better health-related outcomes among those with greater BMI (Hainer & Aldhoon-Hainerová, 2013; Lee et al., 2017; Voulgari et al., 2011). In contrast, BMI was not a predictor of event-free survival in our study. Similarly, several other have reported that higher BMI was not protective among patients with HF and comorbid DM (Adamopoulos et al., 2011; Lee et al., 2017; Pinho et al., 2015). These findings from previous studies suggest that comorbid DM may negate the protective role of obesity against the adverse effects of HF.
There are several limitations that should be noted. First, our results were based on a sample of predominantly white, male patients, suggesting that caution should be used in generalizing to other subpopulations with HF and comorbid DM. A study with a larger sample of females would provide a better understanding the relationships among sex, dietary sodium intake, and outcomes in patients with HF and comorbid DM. Second, this was an observational study; consequently, a causal relationship between dietary sodium intake and event-free survival cannot be drawn. Third, we used urine sodium excretion as an indicator of assess dietary sodium intake, which may be altered by medications used to treat HF. However, we enrolled patients with compensated HF on stable medication regimen for at least 3 months. Sodium excretion in these patients has been demonstrated to be a reliable indicator of dietary sodium intake as they have stable fluid and sodium statuses (Damgaard et al., 2006). Fourth, dietary sodium intake was estimated from a single 24-hour UNa, which may not reflect habitual dietary sodium intake. Nevertheless, the consistency of our results with previous studies provides credibility of our results.
Conclusion
Prior evidence suggested that dietary sodium intake restriction for patients with DM may increase risk of cardiac disease and other complications. However, the health outcomes were unknown for patients with HF and comorbid DM. Our data provide evidence that dietary sodium restriction was beneficial for patients with HF and comorbid DM. However, given the current uncertainty regarding the appropriate level of sodium restriction in HF (Yancy, 2018), additional studies are needed before providing specific recommendations for dietary sodium intake.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institute of Nursing Research NIH RO1NR009280, National Institute of Nursing Research NIH P20NR0106791, American Heart Association, Great Rivers Affiliate Postdoctoral Fellowship, National Center for Research Resources, NIH UL1 RR025008, National Center for Advancing Translational Sciences, NIH UL1TR000117, General Clinical Research Centers NIH: Indiana University M01RR000750, Atlanta Veterans Administration Medical Center, and Clarian Health Partners (Indiana).