
Abstract
The study aimed to develop and test the Coronary Artery Disease Empowerment Scale in Korea and assess its initial aspects of validity and reliability. The participants included 301 patients diagnosed with coronary artery disease, receiving regular outpatient and inpatient care. Data were collected from August to December 2019. The exploratory factor analysis resulted in extracting 25 items and three factors—self-determination, emotional self-regulation, and personal competence of disease management perception—with a cumulative explanatory power of 55.40%. A significant correlation was found between the Korean versions of the Cardiac Self-efficacy Scale (r = .31, p < .001) and the Health Empowerment Scale (r = .45, p < .001). The internal consistency reliability of all items was .93. The developed instrument can be used to evaluate empowerment in patients with coronary artery disease and identify an improved instrument to measure empowerment. However, further testing of the newly developed Coronary Artery Disease Empowerment Scale is required.
Introduction
Coronary artery disease (CAD) is among the most common chronic diseases and requires active healthcare maintenance to prevent a relapse (Arnett et al., 2019). As concerns about the healthcare of CAD patients increase, more studies are being conducted on how to improve their healthcare, but only some concepts—such as knowledge, anxiety, self-efficacy, and awareness of risk factors—are being considered extensively by these studies (Baek & Son, 2015; Kim & Kim, 2017; Zhang et al., 2017). Therefore, more studies are required to identify and evaluate the concepts of empowerment that can be used.
In healthcare, “empowerment” is a popular and widely used term that has garnered increased attention since the World Health Organization (1998) defined health empowerment as a process by which people can gain greater control over the decisions affecting their lives and health. Subsequently, conceptual analysis and instrument development have been performed by studies for various types of patient empowerment (Alves et al., 2018; Anderson et al., 2000, 2003; Ching et al., 2020; Khanian et al., 2020; Park & Park, 2013; Shin & Park, 2015). Specific and effective interventions are being actively developed based on the clear concept of empowerment appropriate for patients.
In Korea, due to the lack of a disease-specific empowerment instrument, researchers used modified and supplemented instruments to suit the subject (Son & Kim, 2017), or expanded them to include all health conditions, rather than specific diseases (Ko & Kang, 2018). Recently, an empowerment enhancement intervention study was attempted in patients with chronic diseases in Korea, but the effect of empowerment enhancement was indirectly verified by measuring uncertainty, self-care agency, self-efficacy, and participation (Kim & You, 2017; Oh & Kim, 2016). This is due to the absence of an empowerment measurement that reflects patients’ characteristics; thus, research on measuring and evaluating empowerment should precede research on intervention and effectiveness, to accurately measure the change of empowerment before and after an intervention.
In particular, CAD patients, unlike patients with other chronic diseases, do not experience symptoms after an acute episode; thus, these patients lack an understanding of the disease and have less motivation for secondary prevention (Dullaghan et al., 2014). It has been reported that the rate of practicing healthcare is low (Kähkönen et al., 2018). Therefore, CAD patients need to be empowered to learn how to take care of their health and manage symptoms that may recur after the intervention; thus, a CAD disease-specific empowerment assessment instrument is required.
The existing patient empowerment instrument for evaluating CAD patients (Lewin & Piper, 2007) focuses on interactional aspects. The study was conducted in one acute National Health Service Trust in England to investigate coronary care patients’ perceptions of their care related to empowerment and strengthening patient choice. The instrument showed that CAD patients encountered a lack of options during discharge counseling and treatment by healthcare professionals in the empowerment process. However, there were limitations to the development of the instrument because it did not include intrapersonal and behavioral aspects. Empowerment is a comprehensive concept that involves intrapersonal, interactional, and behavioral aspects (Shin & Park, 2015; Zimmerman, 1995). Therefore, it is necessary to develop for CAD patients an instrument that reflects the concept of empowerment and enhances self-care by regulating intrapersonal aspects and practice of continuous self-care to control the behavioral aspects of the disease.
Developing an instrument appropriate for CAD patients will help identify patients’ empowerment status and develop intervention strategies to enhance empowerment for factors with low empowerment identified in the evaluation of the empowerment level. In this study, we aimed to create an instrument to assess empowerment, an important concept in patient-centered treatment for CAD patients.
The Study
Aim
This is a methodological study to develop the Coronary Artery Disease Empowerment Scale (CADES) in Korea and assess its initial aspects of validity and reliability. The study was conducted according to the instrument development and validation steps proposed by DeVellis (2017).
Methodology
Development of CADES
Based on a preliminary literature review and the analysis results obtained from individual in-depth interviews with CAD patients on empowerment, the conceptual framework of the instrument was first developed (Kim, 2020; Kim & Shin, 2021). Data were collected between January 3 and February 11, 2019; each interview session lasted 30 to 60 minutes. The data saturation point was reached by repeating in-depth interviews with 10 patients, and no new ideas or opinions could be derived. The data were analyzed using qualitative content analysis. As patient empowerment focuses on the individual level, it is reportedly similar to psychological empowerment (Jørgensen et al., 2018), which emphasizes the level of empowerment of individuals and includes intrapersonal, interactional, and behavioral aspects (Zimmerman, 1995). Therefore, we categorized the items into three areas through literature review, analysis of existing instruments, and interviews: intrapersonal aspect (i.e., perceived competence and knowledge on lifestyle management, sense of control of one’s own healthcare, self-acceptance to change, and motivation for voluntary behavior), interactional aspect (i.e., information search, active communication between patients and healthcare professionals, and supportive relationships), and behavioral aspect (i.e., self-management in one’s life and coping behavior with disease). Duplicate items and items with low relevance to empowerment were deleted by the researchers (one professor of nursing were nurse in the Cardiology Intensive Care Unit, one nurse with more than 10 years of clinical experience, and one nurse with experience in instrument development). After the modification and complementation process of clarifying ambiguous expressions, 64 preliminary question items were prepared. Based on the analysis of the existing empowerment instrument, a five-point Likert response scale was created for the instrument. The scale for quantification was determined by the five-point Likert scale, in which the number of reaction categories was determined according to the phenomena and research objectives of the researcher (DeVellis, 2017).
Evaluation of CADES
Participants
The participants were adults diagnosed with CAD who were routinely undergoing outpatient and inpatient treatment. Because 300 or more participants were required to conduct factor analysis for the final question item composition (DeVellis, 2017), 315 participants were selected considering the dropout rate, and the data of 301 (95.6%) participants were analyzed, excluding 14 who did not have sufficient responses. After all data with missing values were excluded, the remainder did not represent the entire population. However, data with up to 50% missing values showed results similar to the data with no missing values (Ko & Tak, 2016; Othman & Yahia, 2018). Responses with more than 50% missing items were excluded from the analysis.
Instrument
The instruments used for validity evaluation in the evaluation stage are as follows.
To assess the concurrent validity, we used the Korean version (Kang et al., 2010) of the Cardiac Self-efficacy Scale developed by Sullivan et al. (1998). Concurrent validity is a type of criterion validity verified by the relationship with the scores obtained from tests that have already been validated (DeVellis, 2017). In a previous study (Anderson et al., 2000), self-efficacy was used as a component of empowerment, although empowerment has a broader theoretical perspective than self-efficacy (Zimmerman, 1995). In studies developing an empowerment scale (Garcimartín et al., 2020; Park et al., 2017; Park & Park, 2013), the correlation with the self-efficacy scale was analyzed to assess the validity. It has 16 questions, and responses are provided on a five-point Likert scale ranged from 0 to 4. Higher scores indicate higher cardiovascular self-efficacy. Reliability (Cronbach’s α) was .87 to .90 (reliability for sub-factors: Control Symptoms = .90, Maintain Functioning = .87) at the time of instrument development (Sullivan et al., 1998). In Kang et al.’s (2010) study, the reliability (Cronbach’s α) was .80. In this study, the reliability (Cronbach’s α) was .92.
To assess criterion validity using a validated instrument that measures a concept similar to the one used in the current instrument for CAD patients’ empowerment (DeVellis, 2017), we used a modified and translated version of the Diabetes Empowerment Instrument-Short Form (DES-SF) developed by Anderson et al. (2003), which is the Korean version of the Health Empowerment Scale (K-HES). The K-HES (Park & Park, 2013) is a tool for measuring empowerment in older adults, which has acceptable reliability (internal consistency) and validity (construct and convergent validity). It has eight questions scored on a five-point Likert scale ranging from 1 to 5. The higher the score, the higher the empowerment level. The reliability (Cronbach’s alpha) was .84 in Anderson et al. (2003) and was .80 (Cronbach’s α) in Park and Park (2013). The convergence, construct, and content validities were verified. In this study, the reliability (Cronbach’s α) was .58.
Ethical considerations
For the ethical protection of participants, the study was approved by the Bioethics Committee of a private university prior to data collection (IRB No. DIRB-201904-HR-E-09). The study participants were informed of the purpose of the research, the interview procedure, management and disposal of the collected data, participation, and discontinuation of the interview. Participation was voluntary, and participants signed a consent form before the study was conducted. Data were collected from August to December 2019.
Data analysis
Collected data were statistically processed using SPSS version 22.0 (IBM, Chicago, IL, USA). The general and disease-related characteristics of the participants were analyzed using frequencies, percentages, means, and standard deviations. The Kaiser-Meyer-Olkin (KMO) test and Bartlett’s Sphericity test were used to examine whether the collected data were suitable for factor analysis (Alves et al., 2018; Ching et al., 2020; DeVellis, 2017). To validate construct validity, item analysis was used to calculate the correlation coefficient between items and corrected item-total correlation, and exploratory factor analysis was performed to analyze the instrument’s dimensions. We used the Cardiac Self-efficacy Scale to assess the concurrent validity by performing Pearson’s correlation coefficient analysis, and for the confirmation of criterion validity, we used K-HES. Cronbach’s alpha was calculated to assess the internal consistency reliability.
Results
Validity Testing
Content validity
To test the content validity, the preliminary questions (64 items) were reviewed by 10 specialists (four professors of nursing, three nurses with more than 10 years of clinical experience, two cardiologists, and one nursing Ph.D. with experience in instrument development) to examine the Index of Content Validity (CVI) three times. The researcher requested 10 experts to participate in assessing the content validity through e-mail, and after receiving approval to participate in the study, the content validity questionnaire was sent and data were collected. The CVI for individual items (I-CVI) scored 1 point for “not appropriate,” 2 points for “relevant and requires a lot of correction,” 3 points for “relevant but requires minor correction,” and 4 points for “very appropriate”; if revision was necessary, a revision opinion was suggested. The overall scale’s CVI (S-CVI) was calculated by dividing the number of experts who scored 3 or 4 points in the I-CVI by the total number of experts participating in the evaluation. The results of the content validity test revealed that all the I-CVI were above 0.80, S-CVI was 0.92, and the contents of the instrument were appropriate for assessing the empowerment of CAD patients (Polit et al., 2007).
However, in the content validity that was tested three times, according to the opinions of experts, terms such as “manage my illness,” “health management,” and “self-management” were unified and examples of physical change, treatment, management, and adverse consequences were provided. The scale was also revised to reflect opinions on the movement between aspects (moving from behavioral to interpersonal aspects) and to supplement the related items in the aspects (items on support, such as family). Additionally, questions that were ambiguous and difficult to understand—in which the relationship with empowerment could not be found—and overlapping items were deleted. Using the revised items, a preliminary survey was conducted for CAD patients.
The total number of researchers participating in the preliminary survey of empowerment was set to 10 based on a prior study (Park et al., 2017; Shin & Park, 2015) on instrument development, which reported that 5 to 10 researchers was the appropriate number for such a study. Data were collected during July 8 to 25, 2019. In the preliminary survey, the researchers examined the time required for completing the survey, degree of item comprehensibility, letter size, layout adequacy, and question length adequacy. Moreover, they consulted a scholar of Korean literature. Based on the results, 30 intrapersonal aspect items were revised to 29 items (“I try to keep my motivation for disease management” was deleted due to similarity to other items); 17 interactional aspects items were revised to 15 items (deleted similar items to others, such as “I tell the healthcare professionals the requirements for disease management”); and 17 behavioral aspects items were revised to 10 items (among the coping behavior items, those related to pursuit of social support were moved to the supportive relationship of the interpersonal aspect, while items similar to others, such as “I use a method of prevention before stress comes,” were deleted). The final version of the survey questionnaire had 54 items.
Characteristics of the participants
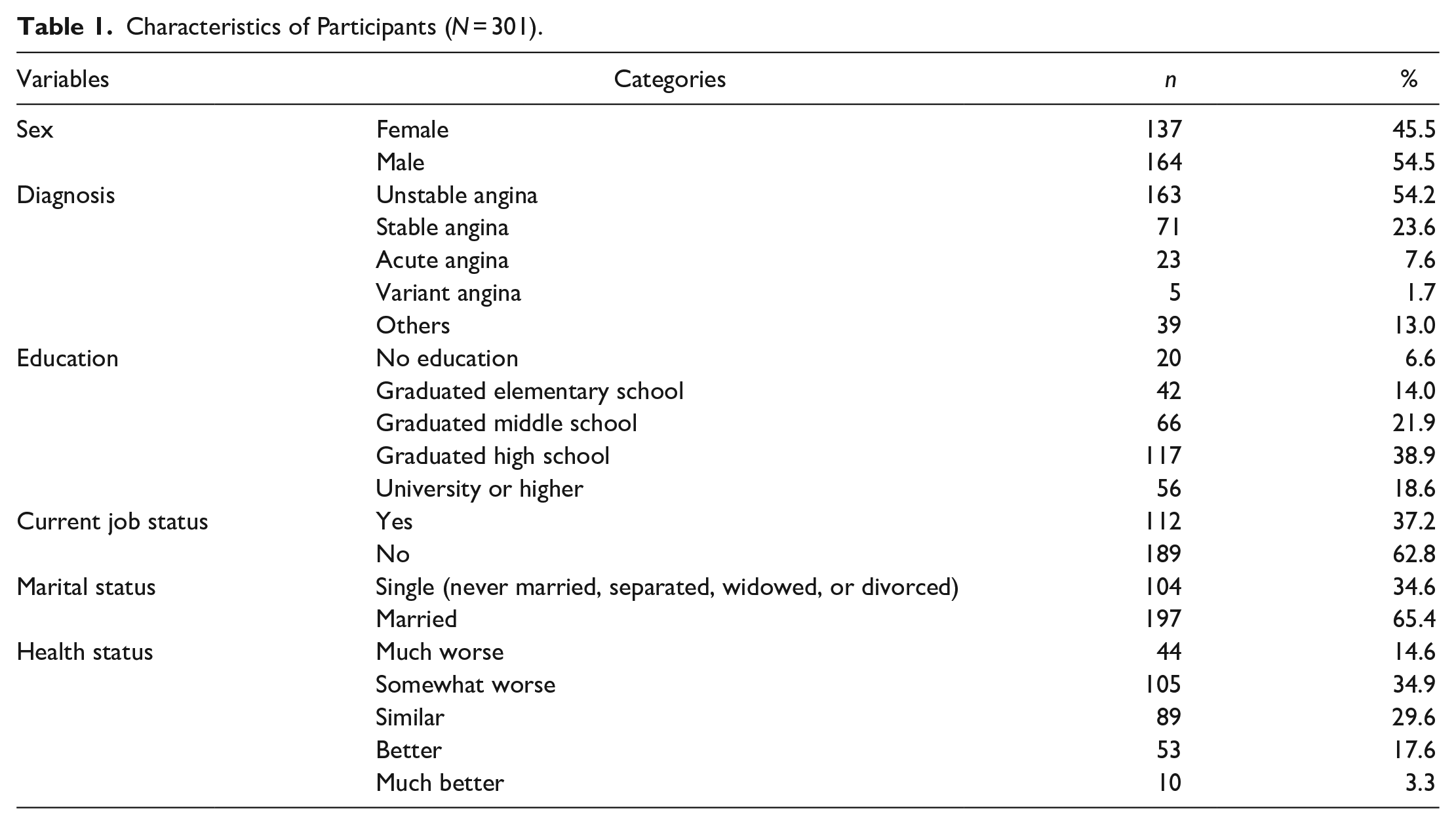
The study participants comprised 137 women (45.5%) and 164 men (54.5%); their mean age was 64.75 years (range: 40–87 years); and the mean time since their diagnosis was 62.67 months. The most common type of diagnosis was unstable angina for 163 patients (54.2%). Compared to other people of the same age without a CAD diagnosis, 44 (14.6%) reported their health status was much worse than others, 105 (34.9%) said it was somewhat worse, 89 (29.6%) reported their status was similar, 53 (17.6%) answered that they were in better condition than others, and 10 responded that they were in a much better condition (3.3%) (Table 1).
Characteristics of Participants (N = 301).
Item analysis
In item analysis, the mean, standard deviation, skewness, and kurtosis of each item were reviewed first to determine whether the collected data were suitable for factor analysis. The analysis result revealed that the skewness value of the data was −.76 to .02 and the kurtosis value was −.58 to .78. The absolute value of the skewness did not exceed 3, and the absolute value of the kurtosis did not exceed 10, satisfying the normality assumption of the data (Kline, 2011). Next, the corrected item-total correlation was calculated to examine the contribution of the items. Since items with a correlation coefficient of less than .30 are judged to have a low discrimination capacity (Hair et al., 2010), items with correlation coefficients of less than .30 were considered for deletion. The corrected item-total correlations ranged from .34 to .75, with no correlation coefficient less than .30.
Exploratory factor analysis
To identify whether the items selected through the item analysis were suitable for factor analysis, the sample fit value of the KMO test was calculated, and Bartlett’s Spherical test was performed. The KMO value was .92 and Bartlett’s Spherical test showed that χ2 = 12,970.46 (df = 1,431, p < .001), confirming the appropriateness for factor analysis (Leech et al., 2005). As the estimation method, because the multivariate normal distribution of the measured variables was confirmed, the maximum likelihood classification method was applied, and the varimax rotation method was used.
Figure 1 displays the scree plot. The horizontal axis represents the number of factors, and the vertical axis represents the eigenvalues. It can be seen that the eigenvalues drop sharply from Factor 1, and the slope becomes gentle from Factor 4. In addition, as a result of confirming the point where the eigenvalues rapidly decrease, three factors were considered appropriate. In the second factor analysis, the number of factors was fixed to three.
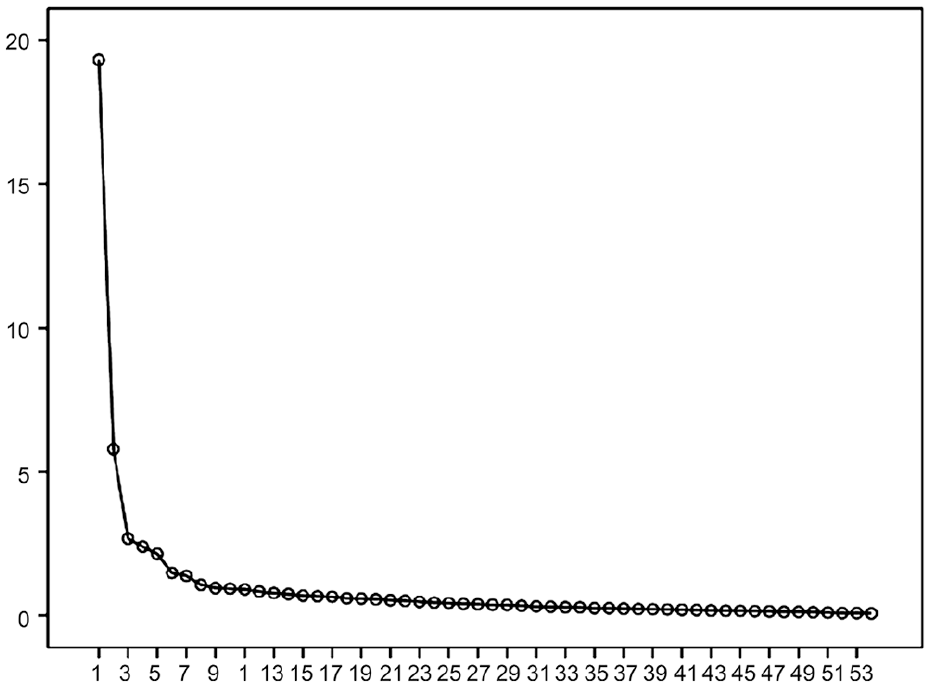
Scree plot.
From the secondary factor analysis, three factors were selected and extracted. The item extraction was based on the difference of 0.30 or more of commonality, 0.30 or more of factor loading, and more than 0.20 of factor load between factors (Hair et al., 2010). The rotated factor matrix was used as the result values for reference. Consequently, 18 items in the first and 11 items in the second factor analysis were deleted because they did not satisfy the criteria; the items did not have distinctive characteristics apart from the statistical values. Finally, in the third factor analysis, three factors and 25 questions were derived. Factor 1 had an eigenvalue of 6.27 and an explanatory power of 25.06%, and the factor loading value of 12 items was 0.56 or higher. Factor 2 had an eigenvalue of 4.07 and an explanatory power of 16.29%, and the factor loading value of seven items was 0.55 or higher. Factor 3 had an eigenvalue of 3.51 and an explanatory power of 14.05%, and the factor loading value of six items was 0.57 or higher. The cumulative explanatory power of the final three factors was 55.40% (Table 2).
Factor Loading of Items (N = 301).
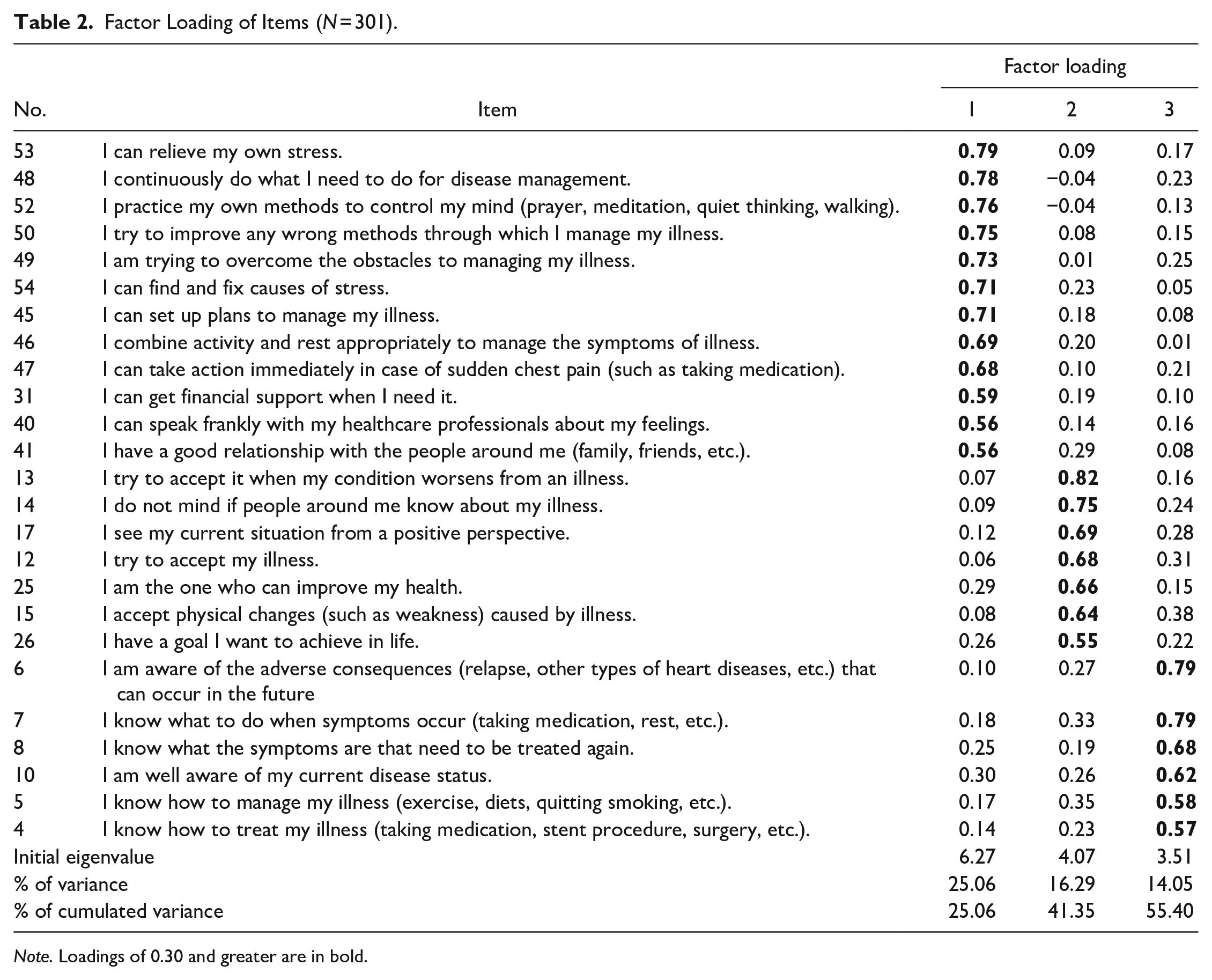
Note. Loadings of 0.30 and greater are in bold.
The final instrument included self-determination, emotional self-regulation, and personal competence of disease management perception, reflecting the implications of the selected items.
Test of concurrent validity and criterion validity
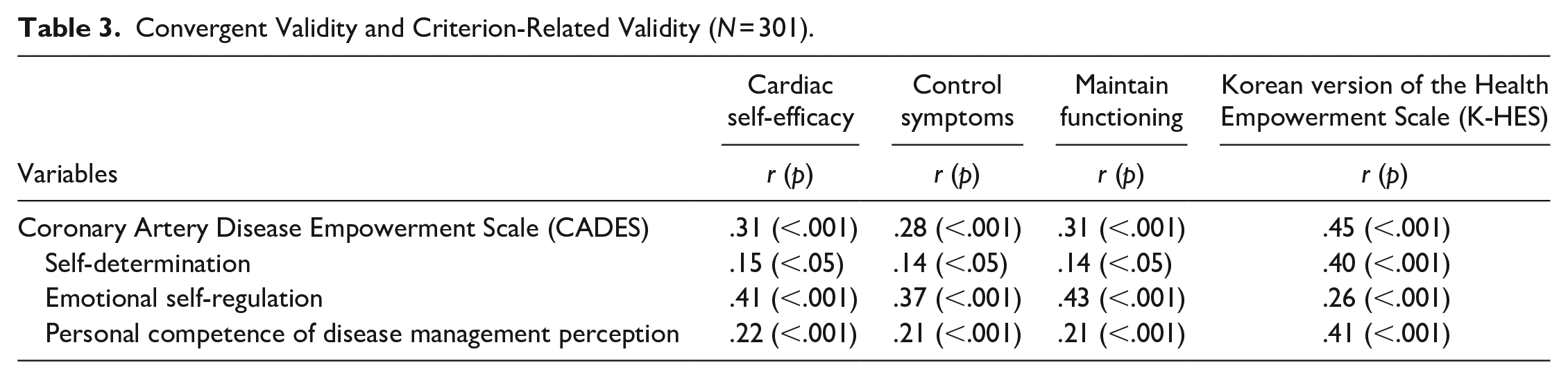
The scores measured by the instrument developed in this study showed correlation with the Cardiac Self-efficacy Scale scores (r = .31, p < .001), ensuring concurrent validity. Pearson’s correlation coefficient for the eight items of the K-HES was .45 (p < .001), indicating a significant correlation and ensuring the verification of the criterion validity (Table 3).
Convergent Validity and Criterion-Related Validity (N = 301).
Reliability Testing
For the reliability verification of the instrument, we used Cronbach’s α coefficient for measuring internal consistency. The final instrument’s Cronbach’s α coefficient was .93. Factor 1 (self-determination) had a Cronbach’s α of .93, Factor 2 (emotional self-regulation), .89, and Factor 3 (personal competence of disease management perception), .89 (Table 4).
Results of the Reliability Analysis.

Discussion
Validity
In this study, an exploratory factor analysis was conducted as a validity analysis to develop the Korean version of the CADES, comprising three factors and 25 items. From the first and second factor analyses, 18 items and 11 items, respectively, were removed as they did not satisfy the statistical criteria, which were based on a difference of commonality of .30 or more and a factor loading of .20 or more (Hair et al., 2010). However, in addition to the statistical criteria for excluding items, the researchers checked every item to determine that each had no distinct characteristics or confirmed problems, such as overlapping loading on two factors.
Among the final three factors, the first factor is termed self-determination because it includes questions about behavioral aspects such as coping with stress, spiritual ability, and self-management; interactional aspects such as support systems (family, friends); economic support exploration; and active communication with healthcare professionals. Many studies on empowerment have focused only on intrapersonal factors (Bolton & Brookings, 1998; Brookings & Bolton, 2000; Peterson et al., 2006), whereas this study makes a significant contribution by developing an instrument encompassing various factors. Additionally, an instrument for the empowerment of female patients with breast cancer was divided into interactional and behavioral factors (Shin & Park, 2015), whereas this study showed these as an integrated factor. It is important for healthcare professionals and patients to maintain a supportive relationship based on mutual trust so that patients can demonstrate their abilities (Cerezo et al., 2016; Musavinasab et al., 2016). Furthermore, exploring the information provided by healthcare professionals could help improve their empowerment when treating patients (Jerofke & Weiss, 2016; Prigge et al., 2015), and we were able to identify that the interactional aspects were closely related to the patient’s self-directed actions. Therefore, it can be interpreted that for the patient’s empowerment, the interactional and behavioral aspects combine to become a single self-determination empowerment factor. Although integrated as one combined empowerment factor, the advantage is that this factor includes all the subareas to provide a comprehensive measurement of two closely related factors. However, since the interactional and behavioral aspects were reduced to one factor in this study, further studies are needed to explore the aspects distinctly.
The second factor is termed emotional self-regulation because it includes questions about self-acceptance to physical changes, sense of control of one’s own healthcare, and motivation for voluntary behavior. In this study, emotional and psychological factors were identified as important attributes, and these factors to improve empowerment were loaded as one. This also differs from the existing empowerment instrument (Lewin & Piper, 2007) for CAD patients that only focuses on the interactional aspect. The empowerment instrument for CAD patients developed in this study appropriately includes the important attribute of empowerment for the disease; thus, it should be used in future studies to measure and interpret this element.
The third factor is termed personal competence of disease management perception because it includes questions about the patients’ awareness of their competence and knowledge on lifestyle management. This study is differentiated from those on the existing empowerment instrument by including awareness empowerment questions about patients’ competence and knowledge to understand the unexpected relapse results of CAD patients, disease management, and treatment method, thus resulting in an instrument that reflects participant characteristics. For CAD patients, the higher the awareness of symptoms, the better the engagement in healthy behaviors (Qiu et al., 2020). Additionally, it was reported that when CAD patients were aware of their understanding of the disease, they improved dietary control and increased physical activities (Mosleh & Almalik, 2016). Therefore, the ability and knowledge of CAD patients are important in health care. The empowerment instrument for chronic disease patients such as those with diabetes (Aghili et al., 2013), chronic obstructive pulmonary disease (Khanian et al., 2020), and rheumatic disease (Alves et al., 2018) enhanced their responses by significantly considering the individual’s competence in obtaining appropriate knowledge and information for independent self-control. The third factor can be used as an instrument to assess the empowerment of personal competence of disease management perception and to improve patients’ role performance and long-term practice of self-control.
After identifying the correlation between the self-efficacy of cardiovascular patients and Korean senior health empowerment, all items and sub-factors were significant in the finalized 25 questions. Moreover, the findings showed that there was a weak correlation with self-efficacy. This result shows that self-efficacy is used in a similar sense as empowerment and as a component as well as a result of empowerment (Kashani et al., 2016; Köhler et al., 2018), but it cannot be interpreted as the same concept, implying that empowerment is a broader theory. In addition, the correlation coefficient should be between .40 and .80 when testing the validity, and a correlation coefficient of less than .40 suggests that the newly developed instrument and other reference instruments may be measuring a different concept (Lee et al., 2009; Park, 2005). The instrument developed in this study showed a moderate correlation with K-HES, establishing concurrent validity.
Reliability
This instrument’s reliability was verified by examining the internal consistency of the items. No item deletion caused an increase in the Cronbach’s α coefficient. The internal consistency of the total items was 0.93, indicating high reliability (Kline, 2000; Nunnally & Bernstein, 1994). It is necessary to develop an instrument with established reliability through further research. Moreover, the Cronbach’s α range in the subareas was .89 to .93. Thus, the reliability of the total instrument and of each factor is high; hence, it is possible to use the scores for each factor for evaluation.
Limitations
This study was conducted with CAD patients in some of Korea’s advanced general hospitals and general hospitals; therefore, it has limited generalizability because of a biased sample collection. In addition, repeatability could not be verified because test-retest reliability was not attempted. In subsequent studies, it is necessary to conduct test-retest reliability to check whether the test score is stable and reliable. This was the first attempt to understand the factor structure for the empowerment of CAD patients; therefore, only exploratory factor analysis was performed. When assessing an instrument that has already been validated, assessing the validity of the conceptual framework through confirmatory factor analysis is appropriate (Geldhof et al., 2014); hence, subsequent studies can reconfirm the factor structure for the empowerment of CAD patients derived from this study and conduct confirmatory factor analysis to validate the instrument. Although the K-HES used for criterion validity verification is an instrument with verified validity and reliability, its internal reliability was low in this study; thus, future studies with larger sample sizes are required for further clarification.
Conclusion
CAD patients need to evaluate their empowerment and use it in their healthcare to learn how to manage the disease and their health by themselves, recognize symptoms, and determine the treatment that works best for them. Numerous studies have evaluated empowerment and confirmed the effectiveness of interventions for patients with chronic diseases. However, studies on CAD patients have been relatively few in this regard. Therefore, this study developed question items that can reflect the empowerment of CAD patients. The developed instrument has adequate validity and reliability, establishing the basis for using it further and more broadly. In the future, to evaluate the stability of the instrument developed in this study and secure its validity, we suggest an iterative study through randomization and expansion of the applicable regions. Moreover, we suggest that studies be conducted on empowerment and related factors of CAD patients in nursing practice by using the developed instrument. Further, the foundation for maintaining specific healthcare and utilizing continuous nursing strategies should be established. Finally, we propose further research on the development of a practical intervention for the empowerment of CAD patients and assessing its effects to enhance the quality of the nursing practice and positively influence the nursing specialization.
Footnotes
Acknowledgements
The authors are grateful to the CAD patients who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2018R1C1B5085519).