
Abstract
Coronavirus disease 2019 (COVID-19) has spread rapidly throughout the world. Still, little is known about the psychological experiences of patients who received inpatient isolation treatment in order to improve the well-being of these patients. We randomly recruited 10 COVID-19 patients who received inpatient isolation treatment at a designated hospital in Wuhan from February to March 2020 and were discharged after recovery. The data were collected via a semi-structured interview over WeChat video and analyzed them using Calaizzi’s descriptive phenomenological method. COVID-19 patients experienced significant psychological stress during hospitalization that continued after recovery and discharge. This can be categorized into three themes: (1) negative emotions experienced; (2) uncertainty of treatment provided; and (3) worries about readjusting to daily life. The insight into a patient’s psychological experiences can support the timely implementation of personalized nursing interventions within hospitals and the community to improve the patient’s mental well-being and recovery trajectory.
Keywords
Introduction
Since the first case that was detected in 2019, the novel coronavirus disease (COVID-19) has spread rapidly around the world. Due to the large number of countries affected by COVID-19, the World Health Organization (WHO) listed the disease as a pandemic of international public health emergency (Cucinotta & Vanelli, 2020; Maier & Brockmann, 2020; World Health Organization, 2020). Common symptoms include fever, cough, dyspnea, chest pain, and fatigue (Chan et al., 2020; Lauer et al., 2020). However, in severe cases, the disease can progress to pneumonia, thrombocytopenia, diarrhoea, nausea, and the appearance of ground-glass shadows in the lungs on X-ray imaging (Chan et al., 2020). As COVID-19 is highly communicable, the standard treatment protocol involves isolating the patient to minimize transmission to healthy individuals (Cascella et al., 2020; Hellewell et al., 2020; Lake, 2020). Patients in China would typically be isolated for approximately 20 days, depending on the remission of symptoms and duration of viral shedding (Zhou et al., 2020). The current COVID-19 pandemic has also brought about significant psychological distress to the general public due to the imposed restrictions on social activities, leading to depression, anxiety, alcohol abuse, and rising levels of suicides (Ahmed et al., 2020; Razai et al., 2020; Thakur & Jain, 2020).
During the early period of the COVID-10 outbreak that required inpatient isolation, the members of the present research team followed a group of medical workers in a Wuhan hospital in February 2020, noting significant psychological stress in the isolated COVID-19 patients. A recent study on recovered COVID-19 patients reported that up to 96.2% experience post-traumatic stress symptoms associated with COVID-19, highlighting a need for psychological interventions to improve well-being (Bo et al., 2021). Additionally, clinical studies have shown that negative emotions can affect the autonomic nervous system as well as the endocrine system, thereby reducing the ability of the immune system to resist pathogens, increasing the risk of infection, and prolonging recovery time (Fredrickson & Levenson, 1998; Kop et al., 2011). Based on previous research in a population of Chinese influenza patients, anxiety and depression are common, especially among those who receive inpatient treatment, and these conditions lead to overall poorer quality of life scores (Yang et al., 2017). Therefore, inpatient isolation treatment represents a unique and invaluable opportunity for healthcare workers to implement psychological interventions to alleviate long-term psychological distress post-recovery.
Previous research has demonstrated that inpatient isolation is associated with negative impacts on patients’ psychological well-being, based on higher scores for depression, anxiety, and anger (Abad et al., 2010). Specifically, it has been found that isolation treatment could sometimes in fact be a greater stressor as compared to the infection itself (Gammon, 1998). This therefore raises the need for nurse interventions that can help to alleviate these negative effects of isolation treatment so as to allow effective coping and improved psychological well-being (Gammon, 1998).
While there is unanimous agreement across the literature that patients who receive inpatient isolation treatment experience significant psychological distress, there is no information on nursing interventions that can help improve patient outcomes in an isolation ward during a pandemic. Additionally, the bulk of the literature currently available pertains to the psychological burdens of frontline workers and how they can be alleviated through different interventions in future pandemics, a topic that is entirely different from the psychological needs of patients (Shechter et al., 2020; Sun et al., 2020; Tan et al., 2020). The currently available studies also have focused more on the relationship between anxiety and depression symptoms and patient demographic or illness severity (Dai et al., 2020). While there is sufficient evidence to suggest that COVID-19 patients do indeed experience psychological distress during and after treatment, few specific details are known about why they experience such distress. Having a better understanding of the challenges these patients face will aid in the generation of interventions to minimize psychological distress for patients and, in turn, help to improve their recovery trajectory. Such information will be vital for future pandemics.
Our present study aims to highlight specific themes where nursing interventions can be implemented to improve the psychological wellbeing of COVID-19 patients who undergo inpatient isolation treatment. These were generated based on data collected regarding the psychological experiences of COVID-19 patients who underwent inpatient isolation treatment in a designated hospital in Wuhan, China through video call interviews. The interviews focused on the psychological burdens of patients during and after treatment for COVID-19. Although no nursing interventions were actively implemented in this study, the results still provide insight regarding nursing interventions that can be easily implemented in future pandemics and that will support the psychological needs of patients.
Method
Study Design and Participants
We performed a descriptive study via video interviews over WeChat video in Mandarin Chinese. The interviews were conducted by two experienced researchers over a month from September to October 2020. One researcher was in charge of conducting the interview, while the other was in charge of taking interview notes. The study used a phenomenological approach to obtain detailed descriptions of the experiences of COVID-19 patients who had received inpatient isolation treatment. Ten participants over the age of 18 were randomly selected and recruited on a rolling basis from among COVID-19 patients treated in the isolation treatment ward of a designated hospital in Wuhan city, China. Patients were included only if they consented to participate and are willing to cooperate during the study. Patients were excluded if they did not stay in the isolation ward for more than 2 weeks, did not demonstrate clear thinking, did not appear capable of providing an accurate description of genuine feelings and experiences, or did not provide consent to participate in the study. The participants were thoroughly informed of the purpose, significance, time required, and voluntary nature of the research study. Informed consent for participant in the study and permission for audio-recording of the interview were obtained before performance of the interview. To ensure the participants’ confidentiality, their names were replaced with serial numbers. To ensure data security, the audio recordings of the interviews were used only for this study and were deleted immediately after analysis.
Data Collection
We prepared a preliminary framework for the interview questions and adapted it accordingly during the interview based on patient’s answers. We also started the interviews by asking how the patients were feeling to build researcher-subject rapport, in order to help patients share their opinions freely in a safe space. We also ensured that the two researchers conducting the interviews had sufficient training in communication skills and transcription. We first obtained permission from the participants to audio-record the interview sessions and then explained the purpose, significance, and the time required for the research in detail. The data were collected via a semi-structured, open-ended, video interview via WeChat that lasted approximately 25 minutes on average, and included the patient’s age, education level, marital status, occupation, income, and length of hospitalization. Broad data-generating questions were used to acquire detailed descriptions of participants’ experiences including: “How do you feel about being diagnosed with COVID-19?”; “How was your mental state during the treatment?”; “How was your mood during the recovery period?”; “What are you most worried about right now, since you have recovered and been discharged from the hospital?”
Data Analysis
As the video interviews were audio recorded, the researcher who conducted the interviews would perform audio transcription of the sessions on the same day. In the event that some parts of the audio recording were muffled, the researcher would refer to the interview notes prepared by the other researcher present during the interview. Relevant transcription for publication was later translated into English by professional translators. We analyzed the qualitative data using Colaizzai’s seven-step method: (1) observing the patient’s facial expression and body language during the interview and becoming familiar with the information provided by participants by reading their accounts repeatedly; (2) analyzing data to extract the semantics from participants’ responses and to qualify the relevance of statements in the context of the research question; (3) noting recurring opinions amongst participants; (4) summarizing encoded opinions to distil meaningful concepts; (5) writing detailed descriptions of responses from each participant to interview questions; (6) identifying recurring themes by comparing responses among participants; and (7) verifying responses with participants and asking clarifying questions to ensure the accuracy and authenticity of the information collected.
Trustworthiness
We improved the credibility and reliability of the present study by implementing these strategies: (1) ensuring participants met the study criteria; 2) discussion of the subject topic with study participants before determining the research question; (3) extraction of information from responses relevant to the research question and distillation of themes by two researchers independently; (4) collection of data by a researcher who had been involved in providing care to patients in order to reduce the Hawthorne effect; (5) collection of data by personnel who had received formal training and had experience in conducting qualitative research, data collection, processing, and analyses; and (6) independent analysis of data by two researchers prior to discussion and comparison of findings to reach a consensus on the themes and clusters of the results.
Research Ethics
Ethics approval was received for this research from the native Ethics Committee. The composition and working procedures of the ethics committee conforms to the Declaration of Helsinki and the principle of International Ethical Guidelines for Biomedical Research Involving Human constituted by the World Health Organization (WHO) and the Council for International Organizations of Medical Sciences (CIOMS).
Results
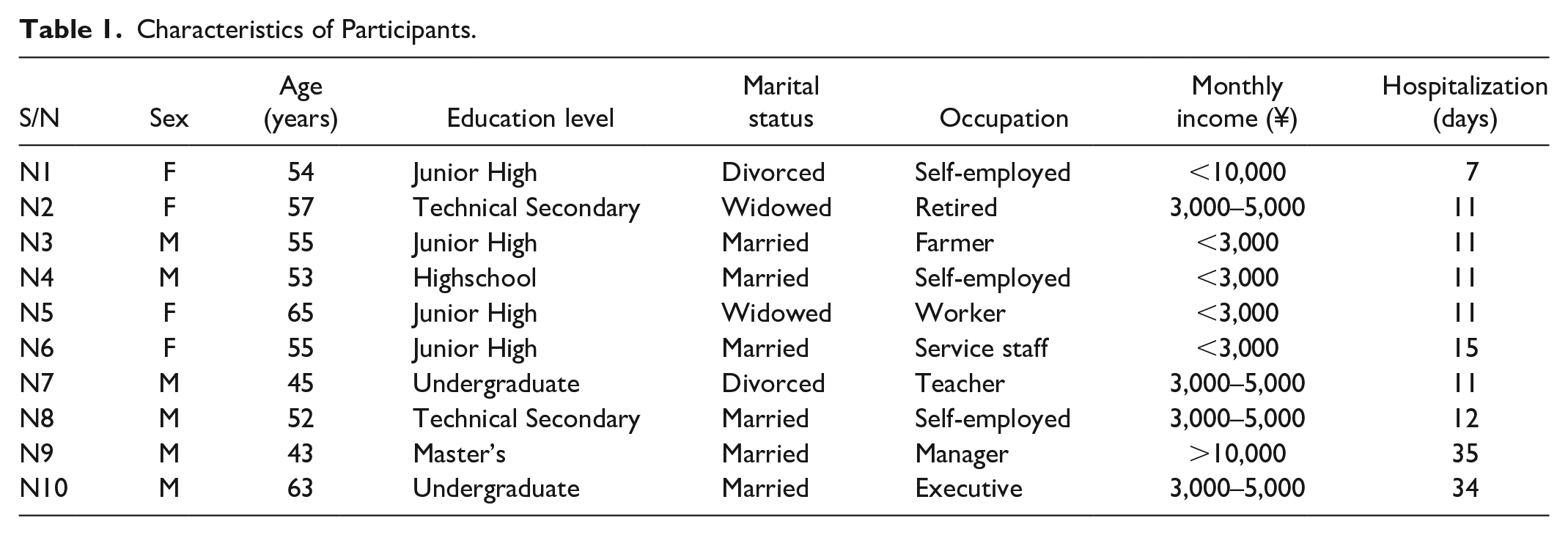
The study participants included 10 patients who had received inpatient isolation treatment for COVID-19 in a designated hospital in Wuhan city, China, between February and March 2020 (Table 1). Participants were treated in the isolation ward for 15.8 days on average.
Characteristics of Participants.
Through the analysis of the responses from the 10 COVID-19 patients, three themes were extracted: negative emotions experienced; uncertainty of treatment provided; and worries about readjusting to daily life.
Panel: Theme categories and clusters Negative emotions experienced Nervousness, anxiety and insomnia Fear and helplessness Nervous breakdown and denial Uncertainty of treatment provided Not confident of treatment efficacy Worried about side-effects of medications Worries about readjusting to daily life Worries about relapse Fear of discrimination and stigma
Negative Emotions Experienced
The first theme cluster identified was negative emotions experienced by COVID-19 patients in the inpatient isolation wards. Isolation wards are often high-stress environments, because of the restrictions placed on patients, with healthcare workers shuttling hurriedly to tend to patients needing medical attention. As the healthcare workers in the isolation wards were overloaded, patients often experienced difficulties getting information from healthcare workers regarding their conditions and treatment plans. Additionally, some had limited contact with their family members who were also staying in other isolation wards and had no way to learn the condition of their family members. As such, several patients reported anxiety, depression, and insomnia due to feeling discomfort from the illness, their confinement in the isolation ward, and the lack of medical attention and updates about their own condition and their family member’s condition from the medical team.
“My partner and I both had fever. My partner’s condition was more severe than mine, but the hospitals did not admit her. Her condition subsequently deteriorated, and I became even more anxious. In addition, the whole treatment process was so terrible I would rather be dead.” (N5)
“My physical condition was very poor when I was admitted into the hospital. I had fever, felt like I could not breathe, was very stressed out, and could not sleep well.” (N10)
“I had to stay in the isolation ward throughout the day during my hospitalisation. I would lie on the bed to receive injections and infusions, and watch the medical staff in protective equipment scurrying around in the ward. When I could not fall asleep at night, my tears start falling unknowingly.” (N6)
“I always heard strange noises at night when I was trying to sleep. The patients in the adjacent beds were tossing and turning, and the medical monitors were very noisy. I had never experienced this before.” (N1)
“I wished the doctor could show me my medical reports and provide detailed information about my condition. This way I could have been less anxious about my illness.” (N2)
As these patients received treatment for COVID-19 in the early months of the outbreak, there was little available information on COVID-19 and treatments. To ensure their safety, healthcare workers wore multiple forms of personal protective equipment that covered their full bodies. This coupled with the news of borders closing between provinces and the increases in the number of cases also led to patients experiencing fear, helplessness, and anger.
“I feel that this is scarier than SARS. It was terrifying to see the number of isolated patients after entering the inpatient isolation ward.” (N8)
“I feel terrified when I see the number of cases increase on the news reports. The even more terrifying and uncomfortable experience is when they collect the nasopharyngeal samples. It makes my nose very uncomfortable and it affects me a lot.” (N4)
“I am afraid that I will infect others. I don’t want to harm anyone. Our country has sacrificed so much to save me.” (N6)
“I am extremely angry. There were very few beds available at the time I was admitted. As such, I experienced significant delays.” (N1)
Patients with COVID-19 exhibit few and very mild symptoms during the initial stage of infection. However, with reports of high death rates from COVID-19 as well as the progression of their illness, patients often experienced high levels of fear and anxiety upon confirmation of their diagnosis, worrying that they would also succumb to the disease.
“When I initially found out that I had been infected, my frame of mind was turned upside down. I could not believe I was infected. I thought I had the common cold and suspected there could be a mistake. I am usually very health conscious and rarely fall sick.” (N6)
“When I was diagnosed, my heart almost shattered. I even wrote my suicide note in my memo.” (N2)
“My family lives within a half a kilometer radius from Huanan Seafood Market. As it was difficult to seek medical treatment in the initial stages, I stayed home for 21 days before being able to seek treatment at another designated hospital. That made me so miserable. Those who were admitted into the hospital at the same time as me had all recovered, but I was the only one who did not get well. I was very scared. Every small movement exhausted me. At the same time, I am worried my oxygen saturation would drop.” (N1)
“My partner died during the COVID-19 pandemic. After receiving this news, I felt that there was no more meaning in life for a long time.” (N5)
“My mood was unstable during the treatment, and I often had heart palpitations. I had moments every day when I felt unusually nervous. Sometimes it was so uncomfortable I would rather die.” (N10)
Uncertainty of Treatment Provided
The second theme cluster surrounded uncertainties about the treatments provided for COVID-19. As COVID-19 was an emerging disease in February 2020, there were still no curative treatments available that ensured recovery and the available treatments largely managed only symptoms. Patients had high expectations regarding the effectiveness of the treatments provided, and while they were eager to recover quickly, they were also worried about the effectiveness of the treatments.
“I was worried the treatment plan was not specific to my condition. I felt tired after a little movement. Even after I was discharged from the hospital, I wonder if it will continue to be like this.” (N1)
“I often feel out of breath. I didn’t feel that the medication had that much of an effect.” (N10)
“During the treatment, my body temperature kept fluctuating and I worried daily that it might increase. I wondered if my illness could not be treated and why I could not be discharged. I wished to get better soon. I wanted to go home.” (N8)
As COVID-19 is a newly emergent infectious disease, there is still no curative treatment available. A portion of patients showed intolerance to the antiviral drugs. The patients depended greatly on the available supportive medications as they were eager to recover quickly, but they subsequently became concerned about the potential toxic side effects.
“I have been continuously taking Abidol and read that there could be adverse reactions to Abidol. I frequently wonder if I might get these side effects. I am very worried!” (N1)
“I was hospitalised for a long time and have taken a lot of medication. I am not sure whether there will be sequelae and how it could affect my life after.” (N10)
Worries about Readjusting to Daily Life
Lastly, the third theme cluster pertained to future-oriented concerns and worries about readjusting to daily life. With growing knowledge about COVID-19, there have been reports of relapse after recovery, creating a certain degree of psychological distress on patients. They were also worried about how COVID-19 might affect their health long-term.
“I thought I would gradually recover after I was discharged from the hospital. However, I started having some symptoms again such as chest tightness, muscle weakness, low-grade fever and loss of appetite. My partner is gone. I am worried I will relapse after this hospitalisation and worried about how to return to normalcy. I am especially worried about whether my heart and lungs have been compromised.” (N5)
“I saw on the news that a lot of people relapsed after recovery. What should I do if I also relapse?” (N9)
Even though the patients had recovered and been discharged from the hospital, they were still bothered and worried about their social situation post-hospitalization. They expressed concerns about whether they posed risks to their family members and community, and were worried that they might be shunned or stigmatized.
“I am worried people might discriminate against those of us who have been previously infected. How do I prove to others that I am no longer contagious? I had to get the hospital to certify that I am no longer contagious before I could be discharged.” (N4)
“I have not told my family that I was sick and I am worried they will find out that I was sick.” (N6)
“I am worried that I will be treated like a contagious person when I return to my community. I am also worried that I might infect my family members and my neighbours, and that friends will view me negatively.” (N7)
Discussion
Our present study sought to identify themes for which nursing interventions can be implemented to improve the psychological wellbeing of COVID-19 patients who receive inpatient isolation treatment. To do so, we performed a descriptive phenomenological study via video call interviews with 10 COVID-19 patients who received inpatient isolation treatment in February 2020. Based on the interviews, we identified three main themes, namely negative emotions experienced, uncertainty of treatment provided, and worries about readjusting to daily life. Patients overall experienced significant distress during their hospitalization due to the discomfort from the illness, feeling helpless about getting necessary medical attention, and also worry about their family members who were also sick. As there was also no curative treatment at the time, patients were understandably worried that the treatments available might not be effective and that there might be other side effects as well. Even after recovery, patients reported being worried about having a relapse, given the reports, and also were concerned about being shunned and stigmatized within their social circles. Overall, our observations are consistent with previous reports of COVID-19 patients experiencing anxiety and depression symptoms and significant distress during isolation treatment (Dai et al., 2020; Hao et al., 2020; Ma et al., 2020). A unique observation in our study that has not been previously reported is the social challenges experienced by COVID-19 patients as they ease back into their daily lives. This highlights a potential avenue where community initiatives can be applied, so as to not let social challenges further exacerbate anxiety and depression symptoms among recovered COVID-19 patients.
At the start of our study in September 2020, the number of new infections worldwide was continuing to rise rapidly, and asymptomatic cases were also detected in some parts of China. As the COVID-19 pandemic continued, the emotional burden experienced by the public increased, and if unaddressed, these emotions could progress to long-term psychological distress, with effects including low self-esteem, insomnia, depression, and anxiety. Healthcare workers can understand the causes of negative emotions and actively carry out intervention measures, such as the Emotional Freedom Technique (EFT) and Mindfulness-Based Stress Reduction (MBSR), to mitigate negative emotions. EFT is a psychotherapy method combining acupoint stimulation guided by the meridian theory in traditional Chinese medicine (TCM) and elements from established therapies including exposure therapy and cognitive behavioural therapy (Church et al., 2012). MBSR, on the other hand, focuses on bringing non-judgmental awareness to sensations, emotions, cognitions, and perceptions; acceptance of these feelings; and subsequent mental relaxation (Carlson & Garland, 2005; Irving et al., 2009).
The environment of isolation wards is harsher than that of normal wards. One reason is that healthcare workers must wear multi-layer protective clothing, which can depersonalize the interactions between patients and healthcare workers. While the protective gear needed to prevent healthcare workers from being infected cannot be changed, measures should be taken to increase the comfort of patients within the wards. Potential measures include adjusting the amount of light in the ward and minimizing noise from the monitors, patients, and other medical equipment to facilitate an environment that improves the quality of rest for patients (Rowlands & Noble, 2008). For patients who are immobile, nurses can regularly help them to move to keep them comfortable (Van Bogaert et al., 2014). When using the sputum aspirator, nurses can explain the procedure to patients and administer the treatment gently to minimize injury and fear toward the procedure. Light music and uplifting stories can also be broadcasted over the public address system to keep patients’ spirits high (Mackrill et al., 2014). Patients who have more energy can be engaged in activities such as drawing patterns on the protective clothing of nurses and physicians, to help increase intimacy between the patients and the healthcare workers. These measures to improve comfort within the isolation wards may help to reduce the psychological distress experienced by the patients and aid their quicker recovery.
Patients in inpatient isolation treatment also struggle with social isolation, as they are prohibited from seeing their family and friends freely. As such, it is important to implement humanistic care for patients and foster a sense of community within the wards. This could be achieved by creating a wish wall where patients can write well wishes and draw images meant to encourage other patients and healthcare workers in the ward. Such positive messages could help to alleviate psychological stress and improve moods within the wards. Patients with acute and critical illnesses should also be placed in separate wards from those with less severe illness, in order to prevent psychological distress to other patients (Rowlands & Noble, 2008). For cases among a family cluster, the family members can be arranged within the same ward, so they are able to emotionally support each other during the hospitalization.
The patients also consistently mentioned concern about the effectiveness and potential side effects of the treatments they received. Frequent and efficient communication with patients likely would help to reduce patients’ doubts about their conditions and treatments. This can be implemented using a WeChat group between the nurses and patients. Additionally, healthcare workers can also follow up with patients and their experiences on the medications, to ensure that they are not experiencing any side effects from the treatments.
The observation that COVID-19 patients experience significant difficulties in adjusting to daily life after recovery, which is the third theme we identified in our study, also emphasizes the need for community management and psychological support. Positive and active guidance to the community can help the population better understand the current state of the pandemic and to remain vigilant. Such guidance can be provided through websites, WeChat groups, community bulletin boards as well as other social media channels with the use of comics, texts, and videos to disseminate scientifically accurate information about the prevention and treatment of COVID-19. This would in turn increase awareness within the community and also alleviate fears among recovered COVID-19 patients and among those worried about exposure to recovered patients, helping patients to build confidence in adjusting to daily life.
Finally, community-based psychological counseling and consultations can be provided by professional medical staff workers to provide timely psychological interventions to patients in need. This would provide humanistic care in comfortable and private consultations to help patients transition back to daily life with confidence. This can be implemented via online psychological services such as counseling hotlines and WeChat online counseling. This would provide patients with outlets to seek personalized help for their various psychological needs. Through these channels, patients with high psychological risks can also be referred to receive more long-term psychological interventions.
Conclusion
This study employed a phenomenological approach in qualitative research to analyze the psychological experiences of 10 COVID-19 patients who received inpatient isolation treatment in a hospital in Wuhan and were discharged after recovery. Three themes were extracted: negative emotions experienced, uncertainty about treatments provided, and worries about readjusting to daily life after recovery. The results from this study highlight the psychological distress experienced by patients and the urgent need for psychological interventions by healthcare workers to ensure the well-being of COVID-19 patients during the isolation period. A number of nursing interventions can be actively adopted to improve the mental well-being of patients, which will likely help to accelerate their recovery time and even equip them with psychological tools that can continue to help them cope as they transition back to daily life. A limitation of the present study is the small number of participants, which represent a narrow range of experiences, and thus, future studies involving larger groups are needed. Such studies can also begin to identify differences among patients with differing characteristics. Additionally, it would be of interest in the future to compare outcomes among patients who receive nursing interventions during inpatient isolation treatment with outcomes among those that did not. Such research would provide insight into whether nursing interventions have any impact on patients’ recovery trajectory as well as long-term effects on psychological health.
Footnotes
Acknowledgements
The authors want to thank the patients for taking time and being vulnerable in sharing their difficult experiences during the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The protocol for conducting medical research on human subjects has been approved by the Ethics Committee of Army Medical Center of PLA (2020(108)). The composition and working procedures of the ethics committee conforms to the Declaration of Helsinki and the principle of International Ethical Guidelines for Biomedical Research Involving Human constituted by the World Health Organization (WHO) and the Council for International Organization of Medical Sciences (CIOMS).