
Abstract
The study was planned and administered as a descriptive study to determine how COVID-19 pandemic affected the lifestyle behaviors of individuals. The study was administered from 30 June to 30 September by including 615 adult individuals who had been exposed to the COVID-19 pandemic. Of the healthy lifestyle behaviors scale II, the total mean score was found to be 126.37 ± 18.58. The health responsibility (p = .032) and nutrition (p = .004) subscale mean scores of women were found to be significantly higher than men, while the spiritual development subscale mean scores of men (p = .047) were found to be significantly higher than that of women. It was found in this study that individuals did not regularly maintain healthy lifestyle behaviors in general during the pandemic period according to the subscales of health responsibility, physical activity, nutrition, spiritual development, interpersonal relationships, and stress management.
Introduction
The COVID-19 disease is causing a global epidemic with large numbers of deaths and infected individuals. In order to control the spread of the COVID-19 virus, public space restrictions and quarantine practices must be implemented. These restrictions and quarantine practices cause short- and long-term negative effects on cardiovascular health, mainly related to unhealthy lifestyle and anxiety (Mattioli et al., 2020). Since individuals have to be in a limited space in the household, this also prepares the ground for many health problems. It is thought that conditions such as inactivity and malnutrition may pave the way for cardiovascular diseases (CVD) and worsen the disease process in those with existing cardiovascular disease (Mattioli & Ballerini, 2020).
In the guideline on primary prevention of cardiovascular disease, it is stated that “In order to reduce the risk of cardiovascular disease, adults should perform at least 150 minutes of moderate intensity activity per week, or 75 minutes of vigorous aerobic physical activity per week (or an equivalent combination of moderate and vigorous activity)” (Arnett et al., 2019; Mattioli & Ballerini, 2020; World Health Organization, 2020a). Many guidelines recommend that individuals do exercises that can be done at home during the quarantine, maintain a healthy diet, abstain from smoking, and get enough sleep. In this context, there is a change in the habits of individuals to cope with the pandemic such as an increase in alcohol consumption or drug use (World Health Organization, 2020b).
Cardiovascular diseases, which have an important place among chronic diseases, are the most important causes of morbidity and mortality in the world and our country. The increase in the average age of societies, unhealthy diet, sedentary lifestyle, and the widespread smoking habit are among the main causes of CVD. Moderate weight gain and excessive obesity increase the risk of CVD and all-cause mortality. Smoking is an independent risk factor for CVD and this risk depends on the number of cigarettes smoked (Yeşil & Altıok, 2012). There are reports stating that COVID-19 causes worse effects in smokers (Reddy et al., 2020). It is important to reveal how individuals change their smoking habit during this pandemic, because smoking has an important effect on the development of CVD and worsening of the disease. It is clear that a healthy diet, non-smoking and physical activity have positive effects in preventing and controlling cardiovascular risk factors (Yeşil & Altıok, 2012).
A healthy lifestyle change is important for ensuring and maintaining heart health. A global action promoting healthy diet and physical activity following quarantine is imperative to encourage people to return to a healthy lifestyle (Mattioli et al., 2020). During the pandemic, physical activity and nutritional habits change due to the limited space the individuals have (Tural, 2020). In order to prevent the cardiovascular and pulmonary complications that COVID-19 may cause on individuals, it will be important to determine the behavioral changes in the lifestyle of individuals.
Methods
Purpose
The research was planned and implemented as a descriptive study to determine how the COVID-19 pandemic affected the lifestyle behaviors of individuals. In this study, an answer was sought to the question of how the COVID-19 pandemic affects the lifestyle behavior of individuals.
Design and Setting
The universe of the research consisted of individuals over 18 years of age between June 30 and September 30, 2020, who had been exposed to the COVID-19 pandemic and informed about the aim and expectations from the research and who gave their consent to participate in the study.
Participants
In the study, the number of subjects to be included in the study to obtain 80% power at the level of α = .05 was determined as 385, taking into account the 3-month research period by simple random sampling. However, considering the losses, it was calculated to include at least 500 adults in the study. Individuals who agreed to participate in the study, who had been exposed to the COVID-19 pandemic, aged 18 and over, were included in the study. Individuals under the age of 18, and those who were not willing to participate in the study were excluded. In this context, 615 individuals were included in the study.
Data collection and measures: In the study, the data were collected using an “online survey on the internet” by the researchers between June 30 and September 30, 2020 due to implementation of social distance and contact restrictions across the country within the scope of the COVID-19 pandemic. The data in the study were collected using the “Sociodemographic characteristics and change in lifestyle behavior research form” created by the researchers and the “Healthy Lifestyle Behaviors Scale-II.”
Sociodemographic characteristics and change in lifestyle behavior research form
This form, prepared by the researchers in line with the literature (Akgün Şahin, & Biçer, 2015; Aksoy & Uçar, 2014; Bostan & Beşer, 2016; Kolaç et al., 2018; Yalçınkaya et al., 2007), consists of 39 items and 2 parts. In the first part, there are 13 items comprising sociodemographic characteristics questions such as age, gender, and the marital status. In the second part, there are 26 items questioning if there is a change in the lifestyle behavior due to the COVID-19 pandemic.
Healthy Lifestyle Behaviors Scale II
This scale was developed by Walker et al. (1987), revised again in 1996, and named as “Healthy Lifestyle Behaviors Scale II” (Walker & Hill-Polerecky, 1996; Walker et al., 1987). The validity and reliability of the scale was confirmed by Bahar et al. (2008). The scale measures the health-enhancing behaviors in relation to an individual’s healthy lifestyle. The scale consists of 52 items and has 6 sub-factors. The subgroups include spiritual development, health responsibility, physical activity, nutrition, interpersonal relationships, and stress management. The subscales include health responsibility (Bostan & Beşer, 2016; Chen et al., 2020; Sungur et al., 2019; World Health Organization, 2020b; World Health Organization, 2020c), physical activity (Aksoy & Uçar, 2014; Muslu & Özçelik Ersü, 2020; Peksoy Kaya & Kaplan, 2020; Uncu & Üstündağ, 2018; Yeşil & Altıok, 2012), nutrition (Akgün Şahin, & Biçer, 2015; Bahar et al., 2008; Bozhüyük et al., 2012; Mattioli & Ballerini, 2020; Şen et al., 2017; Türk Nöroloji Derneği Yönetim Kurulu Üyeleri, 2020), spiritual development (Duran, et al., 2018; Küçükberber et al., 2011; Küçükcankurtaran & Özdoğan, 2020; Tural, 2020; Walker et al., 1987), interpersonal relationships (Dilber & Dilber, 2020; Göger et al., 2019; Kolaç et al., 2018; Mattioli et al., 2020; Walker & Hill-Polerecky, 1996), and stress management (Kılınç et al., 2016; Macit, 2020; Reddy et al., 2020; World Health Organization, 2020c; Yalçınkaya et al., 2007). The overall score of the scale gives the score for the healthy lifestyle behaviors. All items of the scale are positive. The scale is a 4-point Likert rating. The answers are accepted as never (1), sometimes (2), often (3), and regularly (4). For the whole scale, the lowest score is 52 and the highest score is 208. The Alpha reliability coefficient of the scale is .94. The Alpha coefficient reliability value of the sub-factors of the scale varies between .79 and .87 (Bahar et al., 2008; Walker & Hill-Polerecky, 1996; Walker et al., 1987).
Ethical Considerations
Permission was obtained from ethics committee application of the study. Individuals who were willing to participate in the study were informed about the purpose and expectations of the study in line with the Declaration of Helsinki and written consents were obtained by voluntary participation.
Statistical Analysis
The statistics of the study were analyzed with the IBM SPSS Windows 21.0 package program (IBM Corp. Armonk, N.Y. USA). In the statistical evaluation of the study, for the numerical and percentage distributions was used to assess the sociodemographic characteristics and the change in lifestyle behavior due to the COVID-19 pandemic. In addition, the Student t test for the two group evaluations of variables and the Oneway ANOVA test for comparisons of three groups and above were used to compare sociodemographic characteristics and scale scores. The results were evaluated at 95% confidence interval and the significance level of p was accepted as <.05.
Results
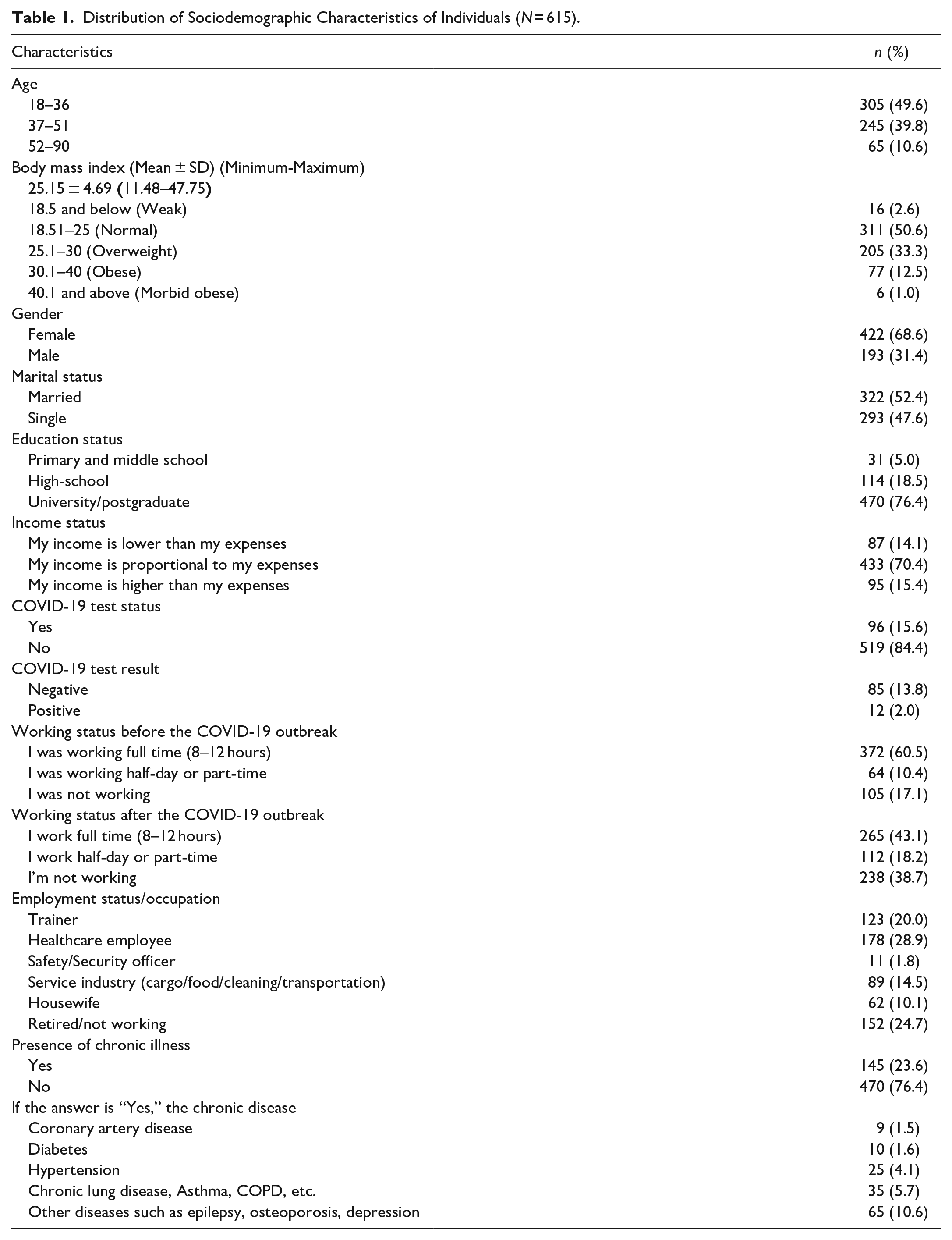
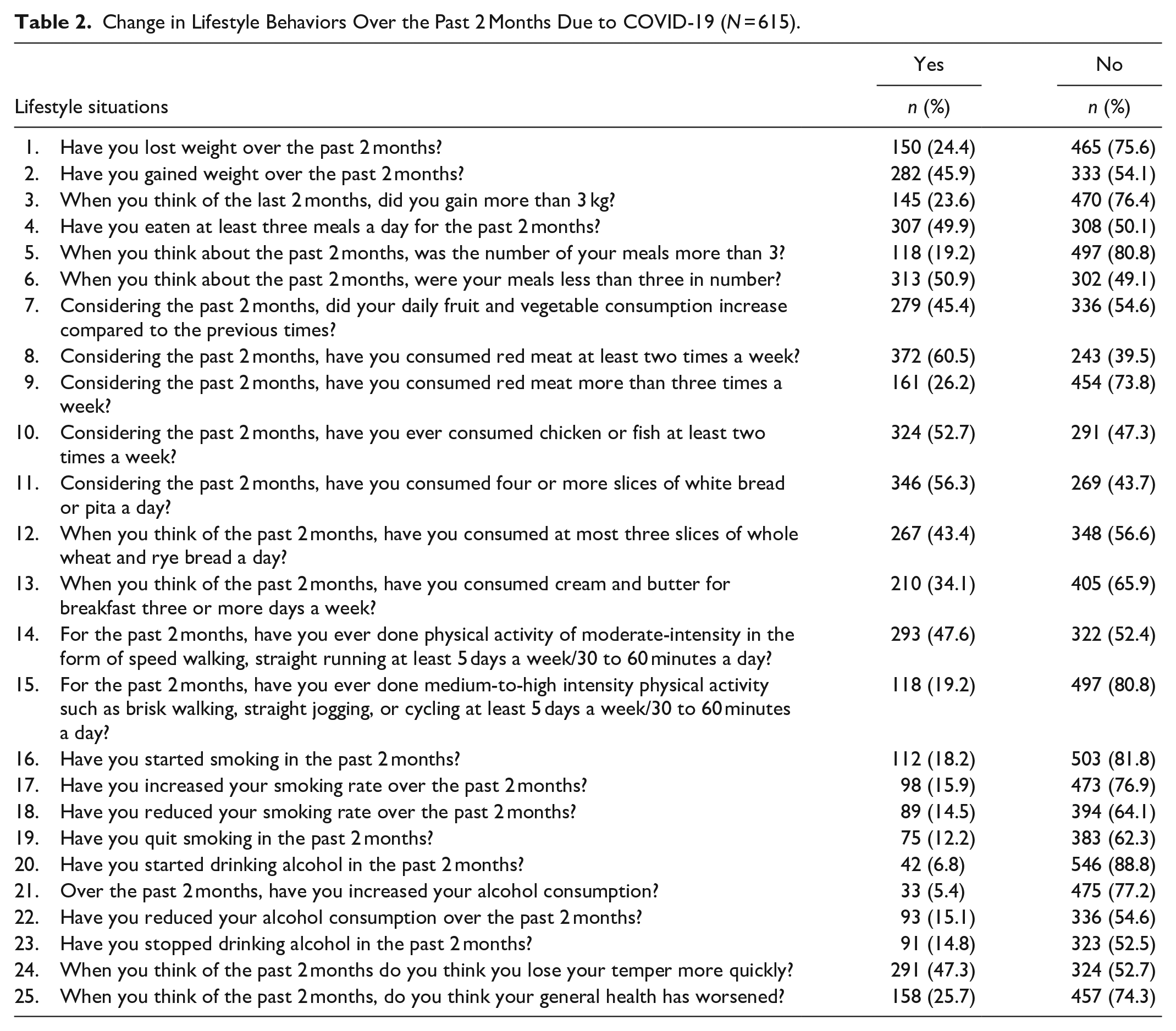
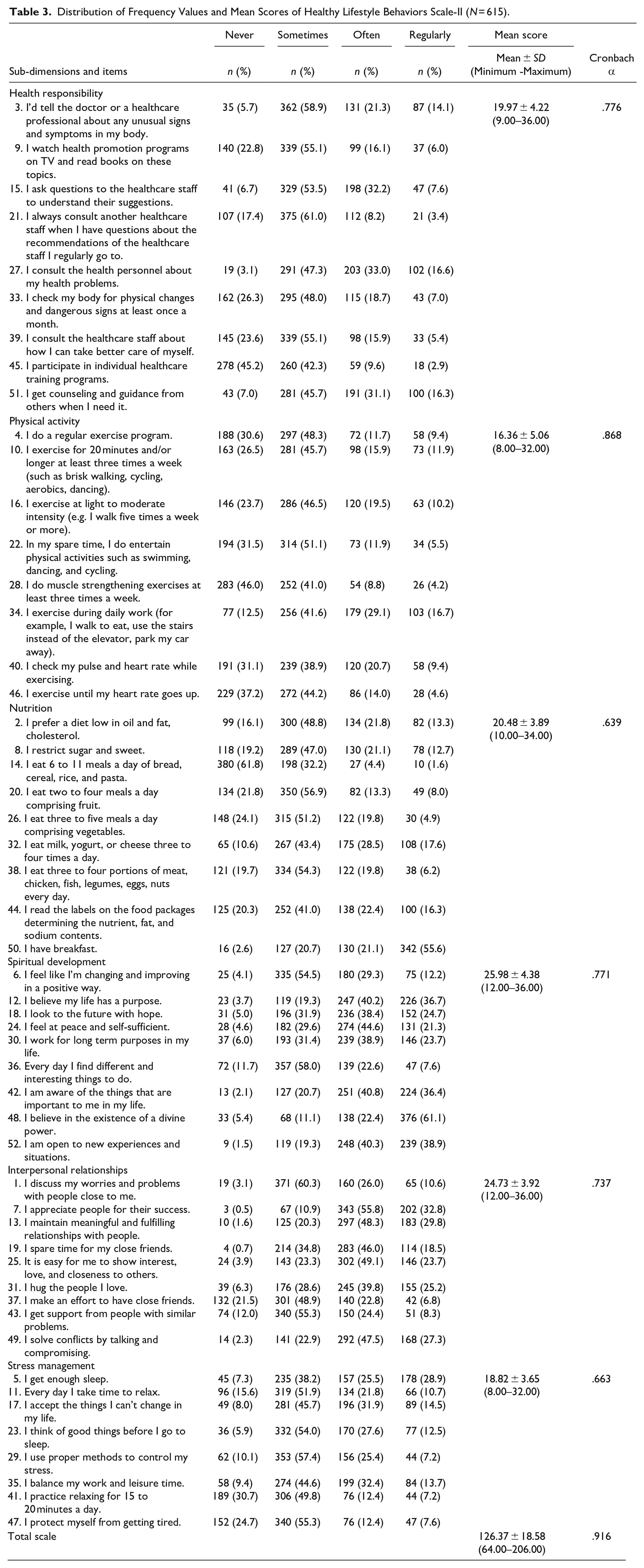
In this study, 68.6% of participants were women (Table 1). It was evaluated whether the individuals participating in the study had changes in their lifestyle behaviors due to the COVID-19 pandemic. During the pandemic period, 23.6% of the participants were found to have gained more than 3 kg, 50.9% had less than three meals a day, the daily consumption of fruit and vegetables of the majority did not increase compared to the previous times (54.6%), and the majority of the participants (73.8%) did not consume red meat more than three times a week; however, the rate of those who consumed chicken or fish at least twice a week was found to be 52.7% (Table 2). It was determined that the majority of consumers (56.3%) consumed four or more slices of white bread and pita a day, and those who consumed a maximum of three slices of whole wheat and rye bread a day were at a lower rate (43.4%) (Table 2). In the research, the rate of those who did medium-intensity physical activity in the form of speed walking or straight running at least 5 days a week/30 to 60 minutes a day was found as 47.6%, while the rate of those who did medium-high-intensity physical activity was 19.2% (Table 2). In the study, it was determined that 18.2% had started smoking, 15.9% increased their smoking rates, 6.8% started to consume alcohol, 47.3% lost their temper more quickly, and 25.7% thought that their general health status had worsened (Table 2). The total mean score for the Healthy Lifestyle Behaviors Scale-II was 126.37 ± 18.58, and the sub-dimension mean score was between 16.36 and 25.98 (Table 3). While the total scale internal consistency (Cronbach’s alpha value) was .916, the sub-dimension internal consistency was between .639 and .868 (Table 3).
Distribution of Sociodemographic Characteristics of Individuals (N = 615).
Change in Lifestyle Behaviors Over the Past 2 Months Due to COVID-19 (N = 615).
Distribution of Frequency Values and Mean Scores of Healthy Lifestyle Behaviors Scale-II (N = 615).
In the study, the women’s health responsibility (p = .032), nutrition (p = .004) sub-dimension mean scores were found to be significantly higher than those of men, while the men’s spiritual development sub-dimension mean scores (p = .047) were significantly higher than those of women, and the physical activity subscale mean score (p < .000) of single individuals was significantly higher than that of married ones. Nutrition (p < .000), spiritual development (p = .028), stress management (p = .012), and the total scale subscale mean scores (p = .003) of those with university-undergraduate and graduate education were significantly higher than those with primary-middle and high school graduates. Physical activity (p = .031), spiritual development (p < .000), interpersonal relations (p = .025), stress management (p = .001), and the general scale mean scores (p = .001) of those whose income was higher than their expenses were found to be significantly higher than those whose income was lower and proportionate. Those who tested negative for COVID-19 had significantly higher health responsibility (p = .011), physical activity (p = .001), stress management (p < .000), and general scale mean scores (p = .002) than those with positive test results, while the subdimension mean scores for physical activity (p = .014), spiritual development (p = .033), and the interpersonal relationships (p = .027) of those with no chronic diseases were significantly higher than those with chronic diseases (Table 4).
Healthy Lifestyle Behaviors Scale-II Score Distribution According to Sociodemographic Characteristics of Individuals (N = 615).
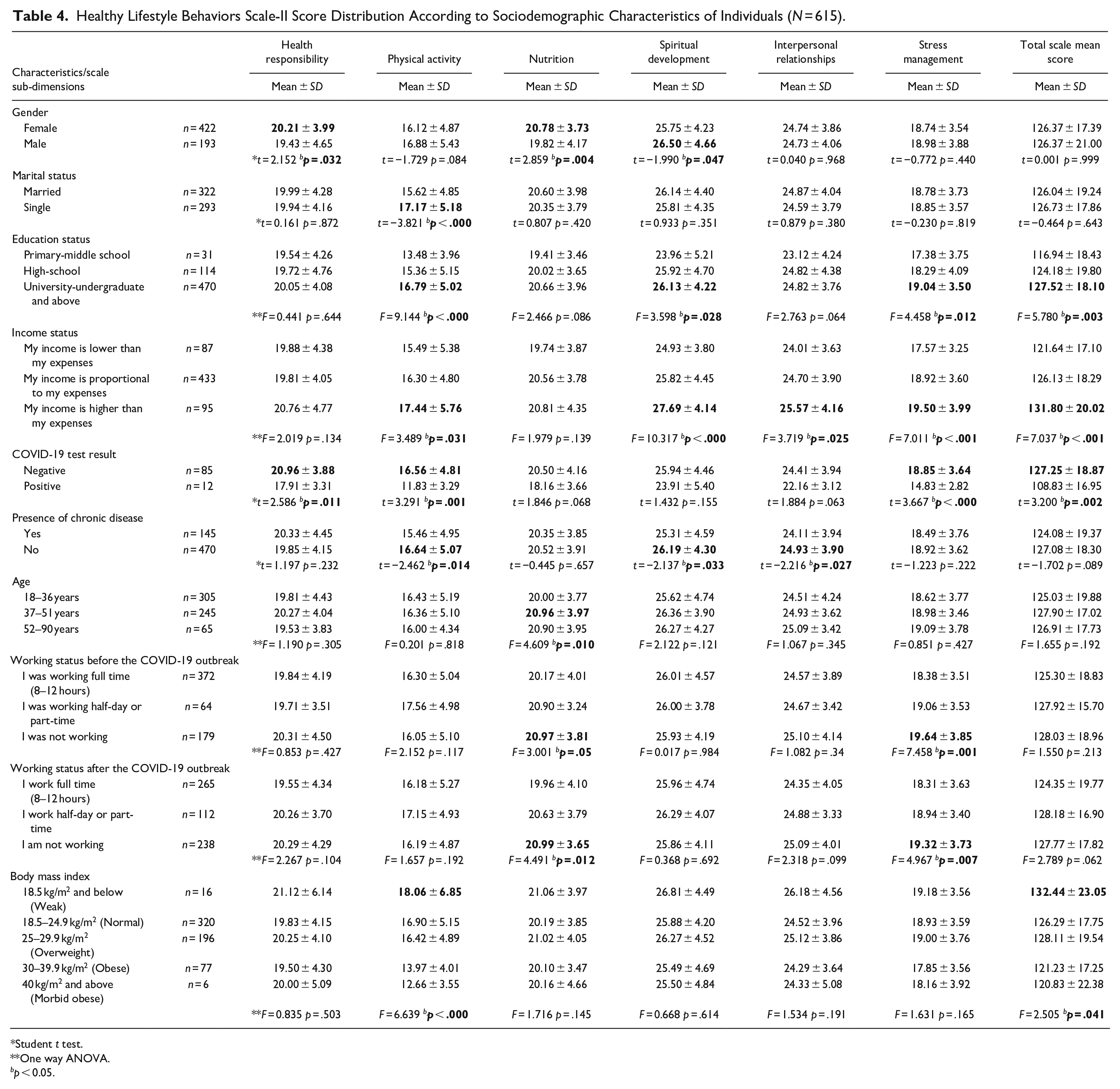
Student t test.
One way ANOVA.
bp < 0.05.
It was found that the nutritional sub-dimension mean score (p = .010) of the 37 to 51 age group was significantly higher than the other age groups. When the healthy lifestyle behavior was evaluated according to the working status after the COVID-19 epidemic, it was found that the nutrition (p = .012) and stress management (p = .007) sub-dimensions mean scores of the non-working group were significantly higher than those of the working groups. It was found that the physical activity (p < .000) sub-dimension and general scale mean scores (p = .041) of the individuals in the underweight category according to the body mass index (BMI) were significantly higher than those in the other BMI categories (Table 4).
Discussion
The aim of this study was to determine how the COVID-19 pandemic affected the lifestyle behaviors of individuals. The World Health Organization (WHO) emphasizes the importance of attempts to prevent the spread of COVID-19 and the protection of healthy lifestyle behaviors in breaking the chain of infection during the pandemic process (Peksoy Kaya & Kaplan, 2020; Sliwa, et al., 2021).
Recent studies show that the COVID-19 pandemic causes negative changes in individuals’ diet, sleep, and physical activity patterns (Dilber & Dilber, 2020; Küçükcankurtaran, & Özdoğan, 2020; Macit, 2020).
Smoking is a common risk factor for coronavirus disease infection. Smoking damages, the immune system and the individual’s susceptibility to infections, making smokers more vulnerable to infectious diseases (Türk Nöroloji Derneği Yönetim Kurulu Üyeleri, 2020). In the study, it was determined that 18.2% of the individuals had started smoking, 15.9% had increased their rate of smoking, 6.8% had started using alcohol, 47.3% lost their temper more quickly, and 25.7% thought that their general health status had worsened (Table 2).
In a study, it was found that individuals skipped lunch more frequently during the pandemic period than before the pandemic (p < .001). On the contrary, it was determined that there was a significant increase in consumption of three or more meals per day (p < .001). In the same study, the frequency of consumption of meat, eggs, legumes, nuts, milk and its products, fruits, cooked vegetables, cereal products, chocolate and sweets, junk food, and herbal tea had increased significantly (p < .05) (Küçükcankurtaran, & Özdoğan, 2020).
With the prolongation of the lockdown period at home due to the pandemic, an increase in activities such as sitting and lying, and a decrease in regular physical activity and sports activities have been observed. Physical activity has a positive effect on reducing depression and anxiety as well as maintaining the energy balance (Chen et al., 2020; Macit, 2020). In a study conducted to determine the physical activity levels of adults in the COVID-19 pandemic, it was found that individuals’ moderate physical activity levels decreased during the pandemic period (p < .001) (Küçükcankurtaran, & Özdoğan, 2020). In this study, it was determined that the rate of those who did medium-intensity physical activity in the form of fast walking and straight running at least 5 days a week/30 to 60 minutes a day was 47.6%, while the rate of those who did medium-high-intensity physical activity was 19.2% (Table 2).
In Macit (2020)’s study, it was found that individuals experienced 1.0 ± 1.5 kg body weight gain in a total of 17.30 ± 13.9 days, and 80.9% (n = 276) showed a decrease in physical activity (Macit, 2020). In this research, it was determined that the rate of those who gained more than 3 kg during the past 2 months of the pandemic was 23.6% (Table 2). Adequate and balanced nutrition is important in order to be healthy before or in the presence of infectious diseases. Therefore, it is important to maintain a healthy diet during the COVID-19 pandemic. A healthy diet is extremely effective in strengthening the immune system. Energy and nutrients obtained with adequate and balanced nutrition support the immune system (Muslu & Özçelik Ersü, 2020). The World Health Organization’s healthy eating recommendations for adults during the COVID-19 pandemic are stated as follows: Consuming fresh and unprocessed foods every day (fruits, vegetables, legumes, whole grain products, oilseeds, and foods of animal origin), preferring raw vegetables and fresh fruits for snacks instead of foods with high sugar, fat or salt content, consuming less salt and sugar, choosing healthy fats, consuming oils containing unsaturated fatty acids instead of saturated fatty acids, white meat instead of red meat and consuming low-fat dairy products are recommended (Muslu & Özçelik Ersü, 2020; World Health Organization, 2020b). In the study, it was determined that 50.9% had less than three meals a day during the pandemic period, and the majority of the participants (73.8%) did not consume red meat more than three times a week. In addition, it was determined that the majority (56.3%) consumed four or more slices of white bread and pita a day (Table 2).
In the study, it was aimed to evaluate the individuals’ lifestyle behaviors to be physically active and to make healthy dietary choices, and to be aware of the physiological and psychological resources in order to control stress and to activate them during the pandemic, with the use of the HLBS-II scale. When the literature was examined, it was seen that studies were carried out in different groups to determine healthy lifestyle behaviors. However, in the only study conducted in our country during the pandemic, students with a mean age of 20.89 ± 1.95 years had a mean HLBS-II total score of 55.76 ± 12.05, and the mean score from the nutrition sub-dimension was 20.34 ± 4.29, the physical activity sub-dimension score was 16.84 ± 5.14 and the stress management sub-dimension score was 18.58 ± 4.29 (Peksoy Kaya & Kaplan, 2020). It was seen that the rate of students showing healthy lifestyle behaviors was at a very low level compared to the studies before the pandemic. When other studies conducted before the pandemic were examined, in a study conducted with healthcare workers, the total score of the Healthy Lifestyle Behaviors Scale-II was determined as 121.18 ± 18.40 (24). In a study conducted with factory workers, the total score was found to be 130.70 ± 21.98 (Kolaç et al., 2018). Şen et al. (2017) determined the mean score of health vocational school students as 118.01 ± 21.0. In this study, it was determined that individuals did not regularly maintain healthy lifestyle behaviors during the pandemic period according to the sub-dimensions of health responsibility, physical activity, nutrition, spiritual development, interpersonal relationships, and stress management (Table 3).
In the study, the women’s health responsibility (p = .032) and nutrition (p = .004) sub-dimension mean scores were found to be significantly higher than men, while the men’s spiritual development sub-dimension mean scores (p = .047) were found to be significantly higher than those of women (Table 4). It was observed that men had higher spiritual feelings during the pandemic period, but they did not cope well enough in nutrition and health responsibility issues, and they were inadequate in acquiring or maintaining healthy living habits. Health responsibility is when the individual feels an active role in being informed about their own health problems and seeking medical help when necessary (Şen et al., 2017). In the study, it was determined that the health responsibility of women was more developed than men (Table 4). Sungur et al. (2019) found that the only statistically significant difference between men and women was in the spiritual development dimension. Similar to our study, the authors found that men’s spiritual development sub-dimension scores were higher than those of women’s. However, the authors stated that the other subscale scores were similar between men and women (Şen et al., 2017). In the study of Uncu and Üstündağ (2018), it was found that there was no statistically significant difference between the mean scores of the healthy lifestyle behaviors sub-dimension by gender. In the study of Şen et al. (2017), although there was no statistically significant difference, it was found that the healthy lifestyle behavior scores of male students were higher than that of female students. Kılıç et al. (2016) found that men displayed higher healthy lifestyle behaviors than women.
Kolaç et al. (2018) stated in their study that the HLBS II mean total score and physical activity mean scores of single individuals were higher than those of married individuals. Similarly, Uncu and Üstündağ (2018) found that the health responsibility, physical activity, and stress management scores of single individuals were statistically significantly higher than those who were married. It is thought that the high stress management scores of the married people may be due to the economic and social negative effects of the pandemic as a source of stress. Kılınç et al. (2016) also stated in their study that married people showed higher healthy lifestyle behaviors than single ones. On the contrary, physical activity levels of single individuals were found to be better than those who were married in this study (Table 4).
Küçükberber et al. (2011) found that married, undergraduate, and post-graduates, those with a good socio-economic status and those without any additional disease exhibited better healthy living behaviors. Göger et al. (2019) found that there was no relationship between the individuals’ educational status and healthy lifestyle behaviors. Kılınç et al. (2016) also stated that individuals with a high level of education showed better healthy lifestyle behaviors than those with a low level of education. Similarly, in this study, it was found that those with university-undergraduate and postgraduate education, those with higher income than their expenses and those without chronic diseases led a healthier lifestyle. In addition, in this study found that those who were negative for COVID-19 test exhibited significantly better healthy lifestyle behaviors than those who tested positive (Table 4).
Infections increase the body’s energy and nutrient needs. In addition, adequate nutrition is important in order to be healthy in the presence of an infectious disease. Maintaining a healthy diet supports the strong immune system (Muslu & Özçelik Ersü, 2020). In the study, when the healthy lifestyle behavior was evaluated according to the working status after the COVID-19 epidemic, the nutritional (p = .012) and stress management (p = .007) sub-dimension mean scores of the non-working group were significantly higher than those of the working groups, and since they were at home, they were found to have healthy eating habits and methods of coping with stress (Table 4).
Adequate and balanced nutrition is one of the basic conditions for the society and individuals to be healthy and strong, to develop economically and socially, and for increased level of welfare. Proper nutrition is one of the preconditions of prevention from metabolic diseases and a healthy life (Bozhüyük et al., 2012). In the study, it was determined that the nutrition sub-dimension mean score (p = .010) of the individuals in the 37 to 51 age group was significantly higher than those in the other age groups (Table 4). In another study similar to this study, it was found that the health responsibility and interpersonal relations sub-dimensions of individuals in the 18 to 24 age group, the physical activity and mean total score of individuals in the 25 to 31 age group, and the nutritional scores of individuals in the 32 to 33 age group were higher (Uncu & Üstündağ, 2018). Sungur et al. (2019) stated in their study that individuals aged 40 to 65 years were more sensitive than individuals aged 39 and under in terms of showing healthy lifestyle behavior, and individuals aged 39 and younger were more sensitive than those aged 65 years and above. Göger et al. (2019) also found in their study that as age increased, their healthy lifestyle behavior decreased and there was a negative relationship between them.
Being overweight or obese increases the risk of developing health problems such as high blood pressure, high blood cholesterol, cardiovascular diseases, stroke, diabetes, some types of cancer, arthritis, and respiratory failure. On the other hand, being weak is an undesirable situation that negatively affects the immune system and can cause weakness and inefficiency in daily life (Bozhüyük et al., 2012). However, in the study, it was found that underweight individuals displayed higher healthy lifestyle behaviors and performed more physical activity (Table 4). Similarly, Göger et al. (2019) stated that there was a negative relationship between the BMI variable and health responsibility, physical activity, stress management and HPL II total scores, and that as the BMI decreased, they displayed higher healthy lifestyle behaviors.
Conclusion and Recommendations
As a result, it was determined in the study that individuals did not regularly maintain healthy lifestyle behaviors during the pandemic period in terms of the sub-dimensions of health responsibility, physical activity, nutrition, spiritual development, interpersonal relationships and stress management.
It is known that lifestyle significantly affects health. The positive effects of individuals’ proper eating habits and being physically active on the immune system are very important in preventing a disease. It is recommended to explain the effects of COVID-19 disease on individuals who do not have healthy eating habits, do not do physical activity, smoke, and consume alcohol, and do not show healthy lifestyle behaviors, and to explain the importance of the disease by using the media and social media sites, to reach individuals and to take initiatives to raise awareness.
Study Limitations
Data collection was carried out online over the internet due to pandemic restrictions. For this reason, there was a problem in reaching sufficient data in the desired time.
Footnotes
Acknowledgements
The authors would like to thank the person who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.