
Abstract
Sarcopenia is a common and progressive skeletal muscle condition, often described as an intermediate stage in the development of frailty and disability in patients with diabetes. This can be improved through physical activity and exercise. This descriptive phenomenological study explored the exercise experiences of older adults with diabetes and sarcopenia. Individual interviews were conducted following semi-structured interview guidelines, and narratives were analyzed using Giorgi’s method. Data saturation was achieved after interviewing 14 purposively sampled older patients with diabetes and sarcopenia. The study identified three main themes: encountering difficulty during exercise, recognizing the advantages of exercise, and constructing a suitable exercise model. While older adults with diabetes and sarcopenia may encounter difficulty during exercise, they also experience positive feedback from exercise. Understanding the limitations of older adults, individualizing exercise models based on their exercise experiences, and providing appropriate interventions and necessary emotional support can effectively prevent diabetes and sarcopenia.
Introduction
Diabetes is a global public health issue that affects approximately 425 million adults (20–79 years old), and its prevalence is projected to reach an estimated 700 million by 2045 (International Diabetes Federation, 2019). Older patients with diabetes are at a higher risk of developing sarcopenia, a pre-frail stage commonly observed in patients with diabetes (Sinclair et al., 2017). Sarcopenia is characterized by an age-related decline in skeletal muscle and low muscle strength or physical performance (Cruz-Jentoft et al., 2019). Many studies have shown a strong association between sarcopenia and adverse health outcomes, such as falls, physical disability, hospital admission, long-term care placement, inferior quality of life, and mortality (Bianchi & Volpato, 2016; Chen et al., 2014; Han et al., 2018). Lifestyle modifications are important for improving and maintaining mobility and metabolic health in individuals with type 2 diabetes and sarcopenia (Mesinovic et al., 2019). Therefore, exercise plays an important role in the control of diabetes and the prevention of complications. In addition, moderate exercise can reduce blood sugar, enhance the effectiveness of insulin, and strengthen the absorption of glucose by skeletal muscles (Marzetti et al., 2017).
However, only 17% of older patients with diabetes adhere to the recommended physical activity duration of 150 min/week (Ramadhan et al., 2019). Older adults unnecessarily refrain from activities because of misunderstandings of the aging process and believe that the cost-effectiveness of exercise training is minimal. They think they are too old to learn how to exercise and benefit from exercise (Lee et al., 2008). It may also result from their self-conceptions formed through their experiences of frailty, observations of their body changes, and the external evaluations and definitions of their physical well-being (Kenter et al., 2015). Previous studies have suggested that exercise interventions should be given based on the patients’ life history, the influence of life events (diseases), and their behavioral patterns developed over time (Whaley, 2007). However, studies on exercise in diabetes have mainly focused on the quantitative analysis of literature reviews to discuss the effectiveness of exercise (Ferriolli et al., 2014). As studies on subjective exercise experiences of older adults with diabetes and sarcopenia remain insufficient, the primary purpose of this study was to explore the exercise experiences of such a population through descriptive phenomenology. This method affords a greater in-depth understanding of people’s life experiences, further enhancing holistic patient care quality (Matua & Van Der Wal, 2015). This experience can provide important information to health workers to understand older adults with diabetes and sarcopenia and provide proper furtherance for health and promotion of exercise by encouraging exercise behavior to manage and improve chronic health conditions.
Methods
Study Design
This descriptive phenomenological study was conducted at the Division of Endocrinology and Metabolism of a medical center in northern Taiwan between December 2018 and April 2019. Data were collected using one-on-one audio-recorded semi-structured interviews, with questions including “Please talk about your exercise experience,” “Which of these exercises do you think are helpful to you?” “Which factors influence your regular exercise according to your exercise experience?” “How do you feel about your exercise experience?” and “What else would you like to talk about that I did not ask?” The interview guide used in this study was compiled based on literature reviews and clinical observations, followed by a consensus by the study team. The participants’ feelings, emotions, and nonverbal expressions were also documented during the interviews. Interviews were conducted in an independent examination room in the clinic. Each interview lasted approximately 30 to 60 minutes, depending on the participants’ physical conditions and whether the description of their experience was adequate. Participants could interrupt the interviews on their will.
Participants
Patients who complained about experiencing symptoms of sarcopenia received a referral from the attending physician to be evaluated for eligibility for our study. Subsequently, we recruited participants using criterion sampling for which the inclusion criteria were: (1) aged 65 years and above, (2) ability to communicate in Mandarin or Taiwanese, (3) regular exercise after being diagnosed with diabetes (30 minute/session, three times/week), (4) diagnosis of sarcopenia by walking speed < 0.8 m/sec and handgrip strength < 26 kg for men and < 16 kg for women (Thompson et al., 2013), and (5) a score of > 4 on the SARC-F Questionnaire, a 5-item questionnaire used to elicit self-reports from patients with signs of sarcopenia, as recommended by EWGSOP2 (Ida et al., 2019).
Data Analysis
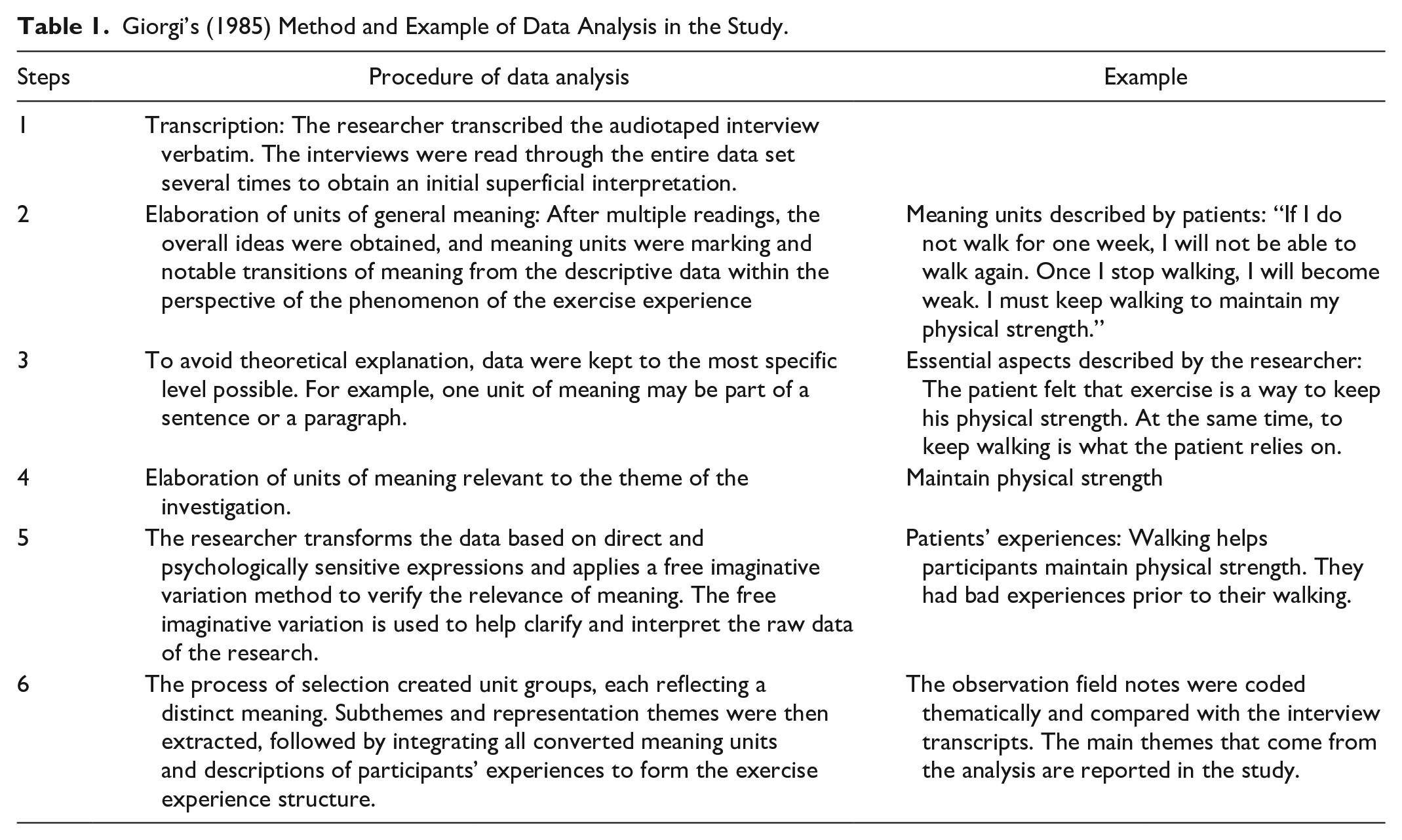
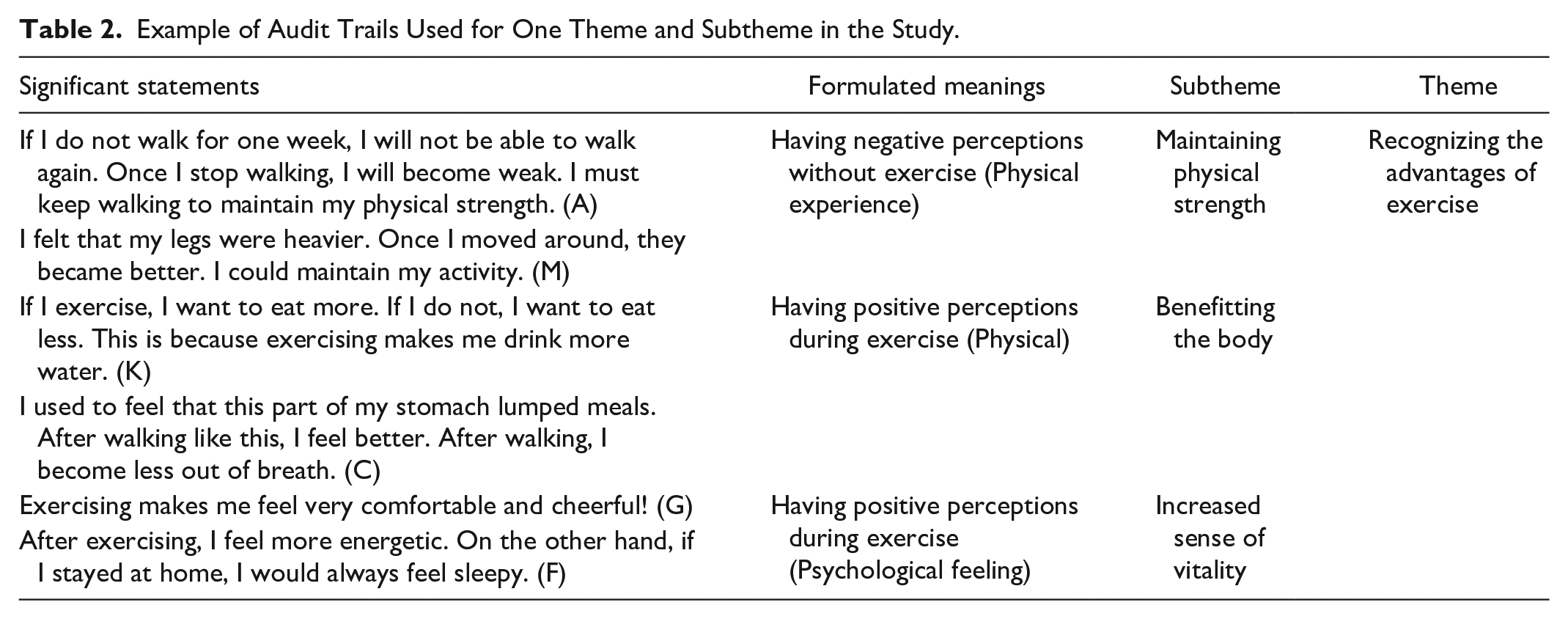
The participants were identified using codes to protect their anonymity. Their statements were identified by letter sequencing from A to N. All records and documents were analyzed using Giorgi’s (1985) analytical method, as shown in Table 1. An example of the audit trails used for one theme and subtheme is shown in Table 2. For rigorousness, the credibility, transferability, dependability, and confirmability proposed by Lincoln and Guba (1985) were adopted. The researcher and participants established a trust relationship. A neutral and uncritical attitude was maintained throughout the process to ensure that participants could freely talk about their experiences. Participants of different ages, sexes, and types of cohabiters were selected to increase their transferability. The research team accurately converted the recorded data into transcripts; peers and three qualitative study experts examined the study results to ensure the suitability and accuracy of the data analysis. The researcher collected the interview data to ensure consistency. Once the exhaustive analysis was completed, two participants were invited to provide feedback, and adjustments were made accordingly. Participants’ feedback and peer reviews were conducted to ensure neutrality in the research. In the research process, the interview guides, recorded data, original transcription, record of the analytic transcoding process, and research results were retained by the researcher.
Giorgi’s (1985) Method and Example of Data Analysis in the Study.
Example of Audit Trails Used for One Theme and Subtheme in the Study.
Ethical Consideration
The Institutional Review Board approved this study at the medical center before the participants were recruited. Before the interviews, participants were informed of the research purpose. In addition, their right to accept other treatments was not influenced. They were informed that they could refuse to participate in the study, and their rights and doctor-patient relationships were not influenced. The participants voluntarily participated and signed informed consent forms before participating in the study. The participants’ feelings, perspectives, and experiences were collected, understood, and analyzed with a respectful and nonjudgmental attitude. To ensure the privacy of every participant, the data were displayed anonymously, and the identities and records of the interviewer and participants were strictly classified. In addition, all research data were adequately preserved.
Results
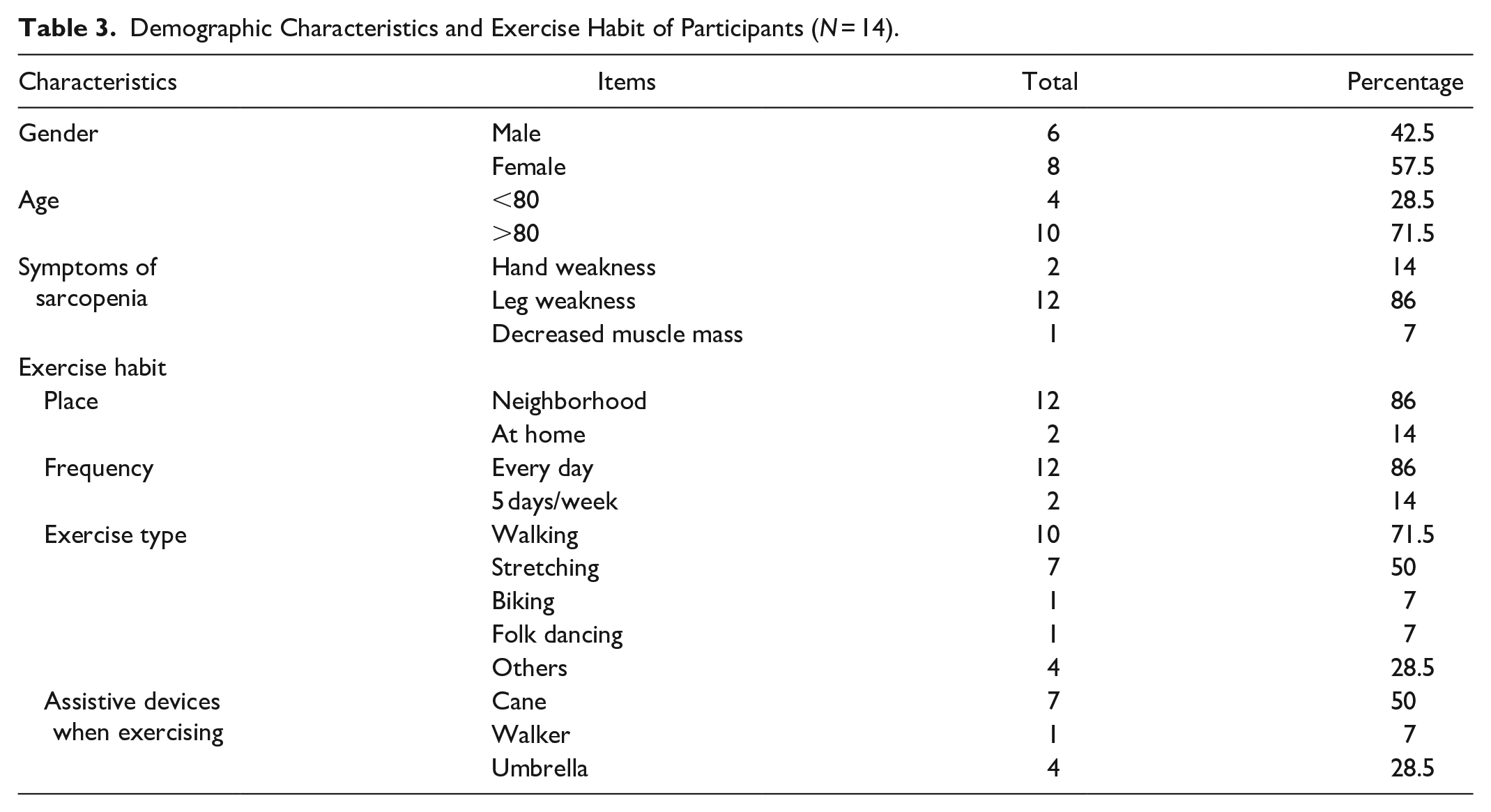
This study reached data saturation with 14 participants with diabetes and sarcopenia aged 71 to 94 years, with an average age of 84 years. There were six men and eight women. The average grip strength was 20.4 kg for men and 14.4 kg for women. Their usual walking speed was around 0.55 m/min. The demographic sarcopenia characteristics of the participants are shown in Table 3.
Demographic Characteristics and Exercise Habit of Participants (N = 14).
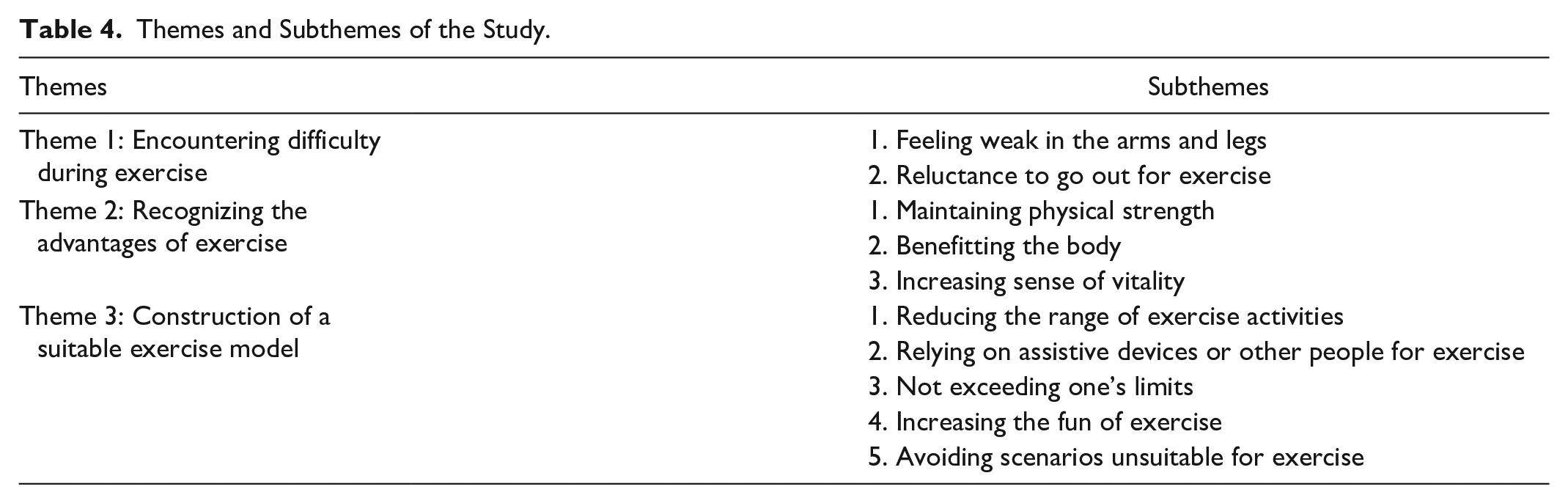
The results emerged into three themes and 10 subthemes, including encountering difficulty during exercise (feeling weak in the arms and legs and reluctance to go out for exercise), recognizing the advantages of exercise (maintaining physical strength, benefitting the body, and increasing the sense of vitality), and construction of a suitable exercise model (reducing the range of exercise activities, relying on assistive devices or other people for exercise, not exceeding one’s limits, increasing the fun of exercise, and avoiding scenarios unsuitable for exercise) (Table 4).
Themes and Subthemes of the Study.
Theme 1: Encountering Difficulty During Exercise
Feeling weak in the arms and legs
The participants noticed that their physical conditions led to difficulties in executing actual exercise behavior. Because most patients had symptoms of sarcopenia, they felt soreness and fatigue in their legs and knees.
My legs were sore, and I felt that my legs were tired. In addition, my knees felt weak, and I could not walk. (A)
The weakness in the upper limbs was manifested not only during exercise but also in daily functions, which may hinder the participant’s engagement in regular exercise.
My arms could not pick up something heavy. They felt weak! (H) One month’s portion (of medicine) felt heavy. I steamed the pumpkins because I did not have the strength in my arms to fry them. (L)
Reluctance to go out for exercise
Aging, diabetes, and sarcopenia increased the difficulty of exercise for the body, which influenced participants’ self-confidence in exercise. The participants did not want to walk and climb, did not feel like walking and going out, felt reluctant and too lazy to go out, and forced themselves during the exercise process because of the difficulty of moving their bodies and the influence of the external environment. Thus, this resulted in a dilemma for the participants when they had to exercise, even though they had been told the benefits of exercise on health. Thus, physical function can be seriously affected psychologically.
I felt too lazy to go out. I do not want to walk! I still had to walk daily. (A) Usually, I am not particularly eager to go out when I go home . . . This is because my feet are so sore . . . I am already 88 years old and do not tell me to walk so far, every day. No way! (N) My sister cares a lot about me. She always asks me to go out for a walk, so I just have to move around. (I)
In this study, the participants eventually continued to exercise, and multiple factors had influenced their participation. For example, one patient had to exercise to maintain physical strength to participate in family activities.
Exercise helps me maintain the physical strength of going out with my family. On holidays, my children take us somewhere farther. (B)
Some participants hoped to continue exercising to maintain their health because of family expectations, while others increased their activities to reduce their sedentary lifestyles. Moreover, one participant exercised alone or with a company of family members.
My son keeps telling me to go exercise, so I keep walking. (F) My son takes me to go out and walk daily after work. We walk for a long time and take a long route. (N)
The exercise experience makes them connect with family and feel a sense of being cared for. Recognition by the family was a key motivation for participants to continue exercising. Even though they were somewhat physically limited, the participants continued to exercise when they received emotional support from the family.
Theme 2: Recognizing Advantages of Exercise
The participants recognized the advantages of exercise. They found that exercising can maintain their physical strength, benefit the body, and increase their sense of vitality. These are crucial realizations that they obtained from maintaining exercise.
Maintaining physical strength
Despite aging, even with sarcopenia, the participants would still acquire the energy needed to maintain physical strength from regular exercise. In addition, exercise can maintain the physical ability to move without feeling weak, prevent the feeling of heavy feet, and prevent difficulty during exercise.
If I do not walk for one week, I will not be able to walk again. Once I stop walking, I will become weak. So I must keep walking to maintain my physical strength. (A) I felt that my legs were heavier. Once I moved around, they improved. I could maintain my activity. (M)
Benefitting the body
The participants in this study felt that exercise improved their appetite and water intake. After exercising, they wanted to drink water and eat something. In addition, walking after meals helps digestion.
If I exercise, I want to eat more. If I do not, I want to eat less. This is because exercising makes me drink more water. (K) I used to feel that this part of my stomach lumped meals. After walking like this, I feel better. After walking, I become less out of breath. (C)
The participants also mentioned the advantages of exercise on chronic diseases, such as diabetes and heart disease.
I feel that exercising is important. It is important for diabetes. It can make my blood sugar level more stable. (E) Riding the bicycle is beneficial to the heart. (H)
Increased sense of vitality
The participants continued to maintain their exercise daily. They felt that exercising increased their sense of vitality and felt comfortable, cheerful, and less tired.
Exercising makes me feel very comfortable and cheerful! (G) After exercising, I feel more energetic. However, if I stayed at home all the time, I would always feel sleepy. (F)
Theme 3: Constructing a Suitable Exercise Model
Older participants with diabetes and sarcopenia experienced physical limitations (i.e., feeling weak in their arms and legs and activity intolerance) and inner struggles (i.e., felt too lazy to go out and distressed when exercising) during exercise. Recognizing their limitations can help patients build new body images and adjust their exercise patterns. They would construct suitable exercise models that provide accommodation, such as reducing the range of exercise activities, relying on assistive devices or other people for exercise, not exceeding one’s limits, increasing exercise fun, and avoiding scenarios unsuitable for exercise.
Reducing the range of exercise activities
The participants narrowed their range of exercise activities to their homes, local communities, or nearby parks. They switched to exercising at home because of decline in mobility, weak legs, and the fear of falling when going out. A patient said: I cannot walk far right now, and I only walk at home. Therefore, I exercise at home by standing up and crouching down while holding a handrail (the patient demonstrated while speaking). (D)
One participant developed a set of at-home exercises, such as walking, standing, crouching, patting the body, stretching in bed, and swinging the hands.
I swing my hands. There is a teacher. I watch his videotapes and follow his moves every morning for many years. (M.
The participants indicated that they would still leave the house whenever possible. They would go to a familiar community or park nearby.
Now I only walk in the park near my house. (I) I move around in the park or alley after meals for 30 minutes. (C)
Relying on assistive devices or other people for exercise
Some participants progressed from casually using assistive devices to rely on them for exercise. Others were accompanied by family members or helpers when going out to exercise.
I use an umbrella as a cane to walk more steadily. Older people have to be concerned about falling when they go out. (K) My foreign caregiver always pushes me to the park in the wheelchair three times a day, and then I start walking and exercising in the park. (F)
The participants are concerned about safety, even though being dependent may change their self-conceptions.
Not exceeding one’s limits
According to their physical conditions, the frequency and duration of the participants taking breaks tended to increase, and their standards and demands tended to decrease, as they just did their best to maintain physical activity.
I walked for one hour in the morning. If I feel tired, I stop for a break and then go on. (A) Being old, it is good enough to just exercise. (N)
Increasing the fun of exercise
Exercise can be fun when it involves going out with family and eating something during or after exercise.
I prefer to go out with my daughter. I always walk to McDonald’s for some fries. Then I go to . . . I walk after drinking something. I feel less tired. (L)
Alternatively, participants could chat or gossip with people during breaks or after exercising in the park. Thus, social engagement through exercise was important for the participants.
My friends at church exercise at a small park every day at eight o’clock. It is like dancing, and it is more fun when we do it together! After dancing, we chat for a long time. It is good to live and kill time as an older person. (N)
Avoiding scenarios unsuitable for exercise
The participants avoided going out for exercise when weather condition was poor or when it was a holiday. Weather factors are a considerable obstacle. Participants preferred to exercise on warm and sunny days.
I always leave the house at noon in the winter so that it is warmer. (M) If it rains, I do not. When it is cold, I do not go! (K)
Discussion
The research results explain how exercise is used in life through the involvement of older people with diabetes and sarcopenia. Participants with difficulties in exercising reflect their physical limitations. The study results are consistent with previous studies in which physical limitations include decreased activity levels, slow gait, and poor physical endurance in patients with sarcopenia (Cruz-Jentoft et al., 2019; Mesinovic et al., 2019). Angiopathies because of long-term high levels of blood sugar and neuropathy affected poor muscle performance in patients with diabetes (Fuggle et al., 2017; Nomura et al., 2018). Physical limitations and obstacles during exercise have also been investigated in older adults with diabetes, frailty, and obesity. It is believed that cardiovascular conditions, skeletal muscle pain, and the physical discomfort experienced during exercise, such as chest pain, shortness of breath, and dizziness, are the key factors that lead to less confidence in exercise (Franco et al., 2015; Lidegaard et al., 2016; Whipple et al., 2019).
This study further analyzes the physical activities the participants engaged in, mostly walking or stretching at home, with little resistance or endurance training. Consequently, the effects of improving muscle strength and daily functions cannot be achieved. The American Diabetes Association (2016) recommended progressive resistance training as a safe and effective approach for muscle strength training for older patients with diabetes and that it should be widely promoted. A similar suggestion was provided by a previous study on older patients with sarcopenia (Freiberger et al., 2016). Therefore, future exercise designs for older adults with diabetes and sarcopenia should consider the overall physical condition of individuals. In addition, the intensity and duration of exercise should be adjusted gradually to assist them in achieving sufficient exercise muscle strength training.
Even participants who regularly exercised encountered difficulties physically or emotionally. Although such participants would feel reluctant to exercise, they would still go out. This observation is in contrast with the population of older adults with chronic back pain who enjoy exercise experiences for relief from embodied pain and a sense of positivity and gratitude (Hay & Connelly, 2020). Most participants felt stressed about their physical discomfort. Consequently, the participants often have to go through an internal turmoil to force themselves to exercise before exercising. Motivation and self-efficacy of perceived physical capability were significant for adults’ physical activity (Ayotte et al., 2010). Older adults’ inner struggles and the potential to facilitate their motivation in physical activity should be considered (Lee et al., 2020). These emotional processes have not been described in previous studies. Understanding the exercise experiences of older adults is critical for individualized care. Moreover, even those who regularly exercised expressed a lack of motivation and interest in adherence.
Nonetheless, the participants still managed to overcome the above difficulties and continued to exercise regularly. This may be mainly due to their values toward the family: the desire to participate in family activities or reach family expectations. Most older adults in the study lived with their families. Whether it is to seek assistance from a foreign domestic helper or to exercise accompanied with their children, exercise has become an essential daily routine for families. Other motives of older adults to regularly exercise may include maintaining autonomy, independence, and experiencing meaningfulness (Bardach et al., 2016).
We suggest that the interviewed older adults with diabetes and sarcopenia generally perceived that exercise is beneficial to health in a way that helps maintain physical strength and increases the sense of vitality, which is in line with previous studies on patients with diabetes (Bardach et al., 2016; Lidegaard et al., 2016). Similarly, the observed active attention toward health issues, desire to maintain health, and motivation to participate in exercise for more benefits on health is consistent with previous studies (Franco et al., 2015), which indicated that older adults who continued to exercise showed improvements in their physical and mental health. In addition, the participants believed that exercise can alleviate chronic diseases and enhance the quality of life by controlling blood sugar levels, strengthening cardiovascular functions, and preventing falls, corroborating the results of Funayama and Funayama (2013). This study further reports that the participants often experience fatigue, lack of physical strength, and poor digestion before engaging in regular exercise and thus felt the urgent need to exercise to maintain health and daily life functions. Aging cannot be avoided; delaying aging progress and maintaining physical strength and daily functions are the ultimate goals of older adults in this study. Hence, it is worthwhile to adopt a more positive attitude toward exercise. Furthermore, exercise assists in alleviating not only diabetes but also in improving the overall health of older adults.
Narrowing the range of activity, utilizing assistive devices, seeking assistance from others, not exceeding their own limits, increasing the fun of exercise, and avoiding situations unsuitable for exercise are examples of constructing suitable exercise models to maintain exercise. First, in terms of reducing the range of activities, it is mainly in response to one’s physical limitations and the accessibility of exercise facilities (Whipple et al., 2019). In our study, we observed that participants would readjust the intensity of their exercise and be more likely to regularly engage in exercise. This observation is in agreement with that of a qualitative study by Mackichan et al. (2013). Older adults with long-term pain engage in more straightforward activities like regular exercise. However, limitations in activities can potentially compromise autonomy by increasing social isolation and conditioning. The other aspect of the participants’ regular exercise was self-identity with physical limitations (Kenter et al., 2015). Therefore, designing exercise routines and equipment suitable for at-home or in-park activities helps promote exercise among patients with sarcopenia. Although some participants reported using umbrellas and crutches, most still relied on family members or foreign domestic helpers. Hence, the future technological development of new assistive devices is very important.
Second, regarding “not exceeding one’s limit,” it is recommended, particularly for older adults, that when exercising, one should focus on one’s own physical conditions and stop or take countermeasures when necessary (Chu & Huang, 2003). On the other hand, the participants would “increase the fun of exercise” as an approach to self-reinforce the engagement of such activities, corresponding with the results of a previous study (Korkiakangas et al., 2009). Entertainment such as exercising with family members, having snacks during or after exercise, chatting, or gossiping in the park with people during breaks can increase exercise motivation, enhancing the benefits of incorporating exercise into a part of everyday routine.
Finally, the environment is one of the biggest challenges in maintaining regular exercise. For example, poor weather conditions—too cold, too hot, or rainy days—would delay an individual’s participation in outdoor activities, further affecting their willingness to exercise (Ogawa et al., 2019). In addition, participating in outdoor exercise activities under bad weather conditions can increase the risk of accidents, particularly in older populations (Wagner et al., 2019). Therefore, it is essential to develop more indoor exercise activities.
Limitations
The limitation of this study was that the participants were older adults with diabetes and sarcopenia; therefore, the results of this study cannot be generalized to other populations. Moreover, the participants were recruited from one medical center, which failed to represent all older adults with diabetes and sarcopenia. Therefore, future research should explore the exercise experiences of such population in various hospitals and institutions to gain a comprehensive understanding of the topic.
Conclusion
In summary, this study employed a descriptive phenomenological method to explore the exercise experiences of older adults with diabetes and sarcopenia. First, patients would experience difficulties in either starting or maintaining regular exercise. However, when the benefits of regular exercise—improved/maintained physical strength and an increased sense of vitality were perceived—the patients would be more likely to construct a suitable exercise model for themselves to follow. Given that older patients with diabetes are at a higher risk of sarcopenia, they should be actively encouraged to take early action on prevention by starting exercises that can increase muscle strength, delaying the decline of daily functions. Tailored exercise design, which considers individual physical conditions, accessibility of exercise facilities, weather conditions, and newly developed assistive devices, should be the primary focus when providing holistic patient care to older adults with diabetes and sarcopenia to increase patient compliance and confidence in exercise.
Interestingly observed from this study, family support also serves as a strong positive reinforcement for engagement in exercise. Therefore, it is recommended to form regular support group meetings for patients who initially start exercising to share exercise experiences. In addition, it is necessary to regularly monitor the blood sugar levels of patients to determine whether diabetic neuropathy or microvascular disease affects motor function, as a reference to provide patients with more precise individualized care.
Footnotes
Acknowledgements
We would like to thank the 14 participants for making this study possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.