
Abstract
This qualitative descriptive study aimed to explore expectations of patients and healthcare experts for an online self-management program for rheumatoid arthritis. Participants were recruited from rheumatology clinics, medical centers, and universities in Taiwan. Individual face-to-face, semi-structured interviews were conducted with patients (n = 16) and healthcare experts (n = 7). Content analysis of the interview data resulted in five subthemes for expectations of an online self-management program: information about how the disease trajectory would impact future health status, availability of opportunities for self-monitoring, opportunities to interact with fellow patients and healthcare providers, simplicity and ease-of-use of the program, and methods to facilitate patient-motivation. These subthemes formulated two overarching themes: content and format. An online self-management program for patients with rheumatoid arthritis should provide evidence-based information about disease variables and behaviors aligned with the specific needs of the individual and adopt strategies that encourage and increase motivation and confidence.
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune inflammatory disease with a prevalence varying from 0.3% to 1% (World Health Organization [WHO], 2020); in Taiwan, the prevalence is approximately 0.4% (Tang & Wu, 2019). Within a decade of onset, at least 50% of patients experience work disability and deterioration of synovial joints can be severe enough to lead to complete disability (Sok et al., 2019; Thomas et al., 2019; WHO, 2020). These symptoms result in a reduction in daily activities and reduced work capacity, which effects quality of life for patients with RA (Sok et al., 2019; Thomas et al., 2019).
The onset of RA typically occurs between 20 and 40 years of age (WHO, 2020). The average life span in Taiwan continues to gradually increase (Ministry of the Interior, 2020), indicating individuals with RA will be living with the disease for more than 40 years. Hence, patients need to learn how to live with and care for this chronic condition, and which can be accomplished with self-management interventions (Barlow et al., 2002; Chen et al., 2016; Shao et al., 2021).
The goal of treatment for chronic conditions such as RA is to minimize the impact of the disease and optimize physical, emotional, and social health, which can be accomplished with self-management interventions (Barlow et al., 2002). Self-management has been defined by Barlow et al. (2002, p. 178) as “the individual’s ability to manage the symptoms, treatment, physical and psychosocial consequences and lifestyle changes inherent in living with a chronic condition.” Thus, self-management is more than simply adhering to treatment guidelines. Self-management requires patients to acquire knowledge about their disease, modify behaviors, and use strategies proactively to reduce discomfort, which can help patients develop confidence to deal with disease-related problems and maintain behavioral changes to maximize well-being (Dures & Hewlett, 2012).
Numerous studies have demonstrated that arthritis self-management programs can benefit patients over and above those achieved by usual care (Dougados et al., 2015; Shao et al., 2021). However, most self-management programs are office-based, which presents limitations for participation of patients unable to travel from home (Azevedo et al., 2015; Shigaki et al., 2013; Stinson et al., 2016). Participation is especially difficult for patients who reside in areas far from a medical office or clinic, or whose pain levels interfere with mobility (Prothero et al., 2017; Shigaki et al., 2013). These problems can be mitigated by exploiting the benefits of online programs, which are more readily available as the use of Internet technology has become more common (Azevedo et al., 2015). Providing online self-management programs for patients with RA could improve quality of life for patients with travel limitations.
Providing online programs via the Internet allows remote access to medical and public health practices, which is supported by home computers as well as mobile devices, such as mobile phones (smartphones), remote patient monitoring devices, and personal digital assistants (PDAs), such as tablets (Cohen et al., 2017; Hood, 2017; WHO, 2011). The advantages of online programs include reductions in geographical constraints (Revenäs et al., 2016), access to medical information and medical care 24 hours a day, 7 days a week (Hood, 2017; Usher-Smith et al., 2017; van Kruijssen et al., 2015), and the benefit of privacy (Stinson et al., 2016).
Online self-management programs that include virtual visits allow more time for patient-provider dialog during consultations and have the potential to improve management of a chronic disease (Rask et al., 2021). Primary care providers (PCPs) of patients with chronic disease reported feeling the time allotted to in-person patient care was inadequate (Rask et al., 2021). These authors concluded an online self-management program could benefit both patients and PCPs by increasing patients’ access to information and reducing the time needed by PCPs for in-person discussions. It is not surprising that 86% of patients with RA suggested it would be useful to develop a web-based RA self-management program (Azevedo et al., 2015).
There is a limited availability of online self-management programs designed specifically for patients with RA. Although Lorig et al. (2008) demonstrated an Internet-based Arthritis Self-Management Program proved effective in improving health status for a large group of patients (N = 855 patients), the study was conducted in the US with a heterogeneous population of patients with arthritis, including not only RA, but also osteoarthritis and fibromyalgia. Therefore, the outcomes may differ from a program that focuses exclusively on patients with RA. Whitehead and Seaton (2016) conducted a systematic review of the literature involving online programs and found programs focused primarily on patients with diabetes and cardiovascular disease, and most studies were conducted in western regions of the world. However, online self-management programs designed for Asian adults with RA are limited.
Qualitative research can provide insight into contextual circumstances when developing intervention programs (Jansen et al., 2010). Numerous studies have demonstrated online programs should be based not only on the needs of the patients for whom the intervention is targeted, but also the expectations of the end-users (Azevedo et al., 2015; Nightingale et al., 2017; Rantala et al., 2020). In Taiwan, the overall access to the Internet reached 79.2% in 2018 (InsightXplorer Market Research Consultants, 2018), suggesting this is an ideal time to develop an online self-management program for patients with RA. Therefore, the aim of this study was to obtain qualitative interview data about the perspectives of an online self-management program for both patients with RA and healthcare experts involved in caring for patients with RA. Interview data were analyzed in order to answer the following research question: “What would be your expectations of an online self-management program for patients with RA?”
Methods
Study Design and Participants
This study used a descriptive qualitative study design (Creswell, 2003; Sandelowski, 2000, 2010) with audio recorded face-to-face semi-structured interviews as the aim was to explore and describe the expectations of patients’ and experts’ of an online RA self-management program. To strengthen rigor and comprehensiveness the study was conducted and reported according to the consolidated criteria for reporting qualitative research (COREQ) checklist for qualitative research (Tong et al., 2007).
Patients were recruited by purposive sampling from the outpatient rheumatology clinic of a medical center in northern Taiwan and were included if they met the following criteria: a confirmed diagnosis of RA at least 6 months prior to the study, aged 20 years or over, had Internet access, and were able to communicate in Mandarin or Taiwanese. Patients who met the inclusion criteria were referred to the first author by their primary nurse. Twenty-two patients were invited to participant, however six declined for the following reasons: treatments interfered with participating (n = 2), there was a change in their condition (n = 1), and a lack of interest (n = 3).
Healthcare experts were recruited from a range of specialties from the same medical center as the patients, as well as two additional medical centers, and a school of nursing. Experts were included if they met the following criteria: worked in areas related to RA care, worked full-time, and ≥3 years of work experience. Experts included one rheumatologist, two RA nurse practitioners, and four experts in rheumatology nursing and electronic healthcare (e-health). Interviews were conducted with 16 patients with RA and the multidisciplinary group of experts (n = 7).
Data Collection
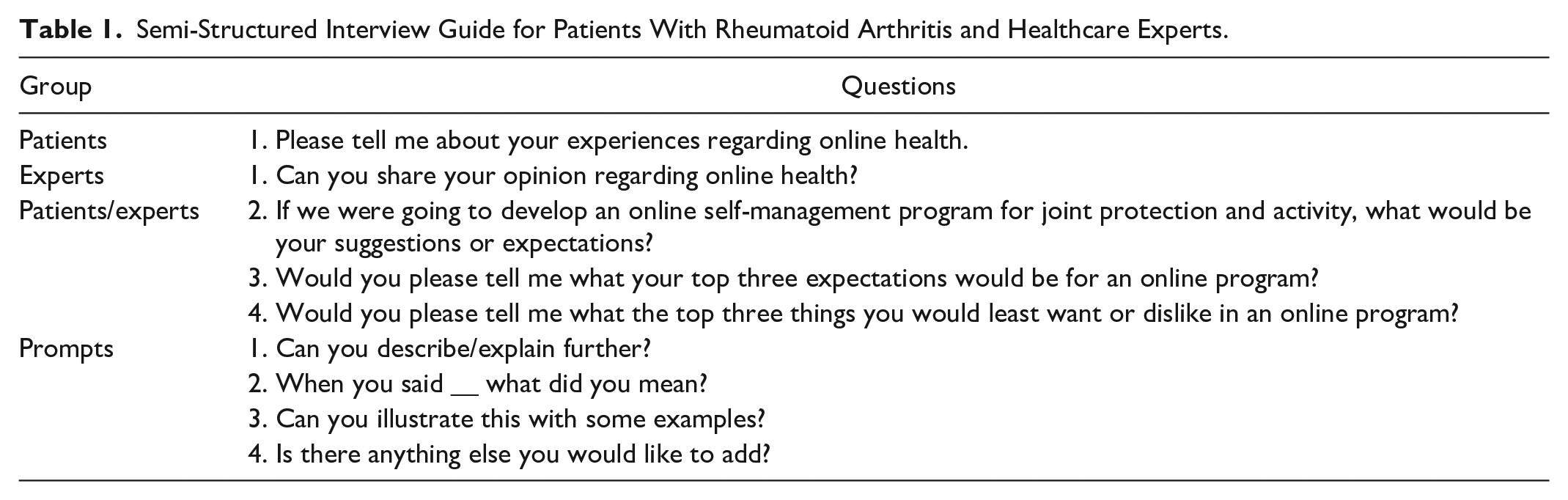
Data were collected with audio recorded individual in-depth, semi-structured, face-to-face interviews from January to May 2019. An author-developed interview guide based on a review of the literature on self-management of RA and online programs was used. The guide was reviewed by a four-person panel comprised of one registered nurse with experience in clinical rheumatology, two experts in rheumatology nursing and online health programs, and one researcher experienced in qualitative studies. The interview guide was modified after review by the panel, and pilot-tested by interviewing two patients with RA and one expert in RA to confirm the clarity of the language and concepts of the questions (Table 1). In order to emphasize that the focus of the online program would be self-management of RA, we provided all participants with the following description: “Our online program will focus on self-management of rheumatoid arthritis. Self-management can enhance an individual’s ability to manage their symptoms, treatments, physical and psychosocial consequences, and lifestyle changes inherent in living with a chronic condition” (Barlow et al., 2002, p. 178).
Semi-Structured Interview Guide for Patients With Rheumatoid Arthritis and Healthcare Experts.
All interviews were conducted by the first author who had postgraduate training in qualitative research methods, previous experience in qualitative research, and clinical experience treating patients with chronic disease. All interviews were conducted in Mandarin or Taiwanese in a quiet room with only the participant and the interviewer present. A sign on the door indicated no interruptions were allowed. Nonmedical terminology was used to facilitate understanding and to encourage patients to discuss their expectations and opinions in the broadest sense. During the interviews the researcher maintained detailed field notes in order to record personal impressions of the interviews as well as non-verbal responses of the participants.
Demographic and clinical information of the patients was also collected during the interview, which included age, gender, educational level, and duration of RA. Demographic information for the experts in RA included age, gender, duration of RA care, and the number of years of experience with online health. All interviews lasted between 20 and 65 minutes, with an average length of 36 minutes. Data collection and analysis of verbatim transcriptions of the interviews occurred simultaneously. Recruitment of participants was discontinued when data were saturated, which occurred when no new categories were described during the coding process of the final interviews with patients and experts (Creswell, 2003). Although this occurred with the 15th patient and 6th expert, additional interviews were conducted to increase the richness of the data.
Ethical Considerations
Ethical approval was granted by the Research Ethics Committee of the university (No. 201702125B0) prior to recruitment of participants. Before obtaining written informed consent, the researchers provided a verbal description of the design and purpose of the study. Participants were informed that participation was entirely voluntary, they were assured their anonymity and confidentiality would be preserved, and they could withdraw from the study at any time and for any reason without any consequences to their care. After potential participants fully understood this information and completed the consent form, interviews were conducted. During the transcription process, personal data were removed and fictitious names were assigned.
Data Analysis
Content analysis is used to evaluate qualitative interview data when the focus of the study is to extract categories (Bengtsson, 2016). In this study, inductive content analysis was employed to gain a greater understanding of the expectations of the patients and experts regarding an online program for self-management of RA. First, audio recorded interview data were transcribed verbatim and analyzed using the procedure described by Graneheim and Lundman (2004). Second, the third and fourth authors analyzed the data independently using content analysis. All transcripts and field notes transcripts were read several times to obtain a general impression of the whole. Data were analyzed line-by-line and manually assigned codes to key thoughts and ideas; coding was not managed with a software program. Key categories and coded lines of text which represented expectations of patients and experts were identified and highlighted. Similar codes that belonged to the same content were then grouped into potential sub-categories and main categories. Finally, the third and fourth authors then checked and discussed the identified categories and subcategories. If there were any disagreements, these were resolved through discussions between the two authors and outside experts in content analysis. Categories and subcategories were revised until consensus was reached. Organization and labeling of the categories were continually checked and modified throughout the analytical process. The two data sets for patients and experts were analyzed individually and then the results were compared.
Conducting interviews in the interviewer’s native language and managing multiple translations can negatively affect the quality of the data (MacLean et al., 2004). Of the 16 patients with RA, 7 spoke Taiwanese, a popular form of non-written language. To decrease discrepancies between the spoken Taiwanese language and written Chinese, the accuracy of the Chinese transcripts was examined by two Taiwanese/Chinese bilingual experts. Only meaningful quotations were selected from the data and translated into English to illustrate the relevance of the findings. These quotes from the Chinese transcripts were translated into English by a bilingual (Mandarin/English) expert in qualitative research. Finally, the research team examined the transcripts to ensure congruence among the Taiwanese language, Chinese language, and the English translation to ensure the participants’ original meaning was retained. No repeat interviews were conducted.
Rigor
Trustworthiness of the interview data was established with credibility, dependability, transferability, and confirmability (Guba & Lincoln, 1983; Sandelowski, 1986). The researchers’ training and experience in qualitative research and careful description of data collection and analysis were used to enhance credibility. Dependability of the findings was assured by pilot testing the interview guide, and the same open-ended questions and prompts with all participants were applied. Transferability of the data included a detailed description of participants’ background, to increase the understanding of the experiences of a broad range of persons with RA in Taiwan. Finally, confirmability was demonstrated by using semi-structured interview questions, using participant quotes to illustrate their expectations and maintaining a neutral, objective perspective to ensure that findings evolved from participants’ perceptions rather than reflecting the researchers’ biases.
Results
The mean age of the patients with RA was 56.3 years (SD = 12.0); almost all were female (93.8%), and the duration of RA ranged from 5 to 26 years (M = 10.94, SD = 5.50). The mean age of the experts in RA care was 48.9 years (SD = 3.89); experience with RA ranged from 1 to 25 years (M = 9.9 years, SD = 10.5). Characteristics of patients and experts are shown in Table 2.
Characteristics of Participants: Patients With Rheumatoid Arthritis (RA) and Experts in RA.
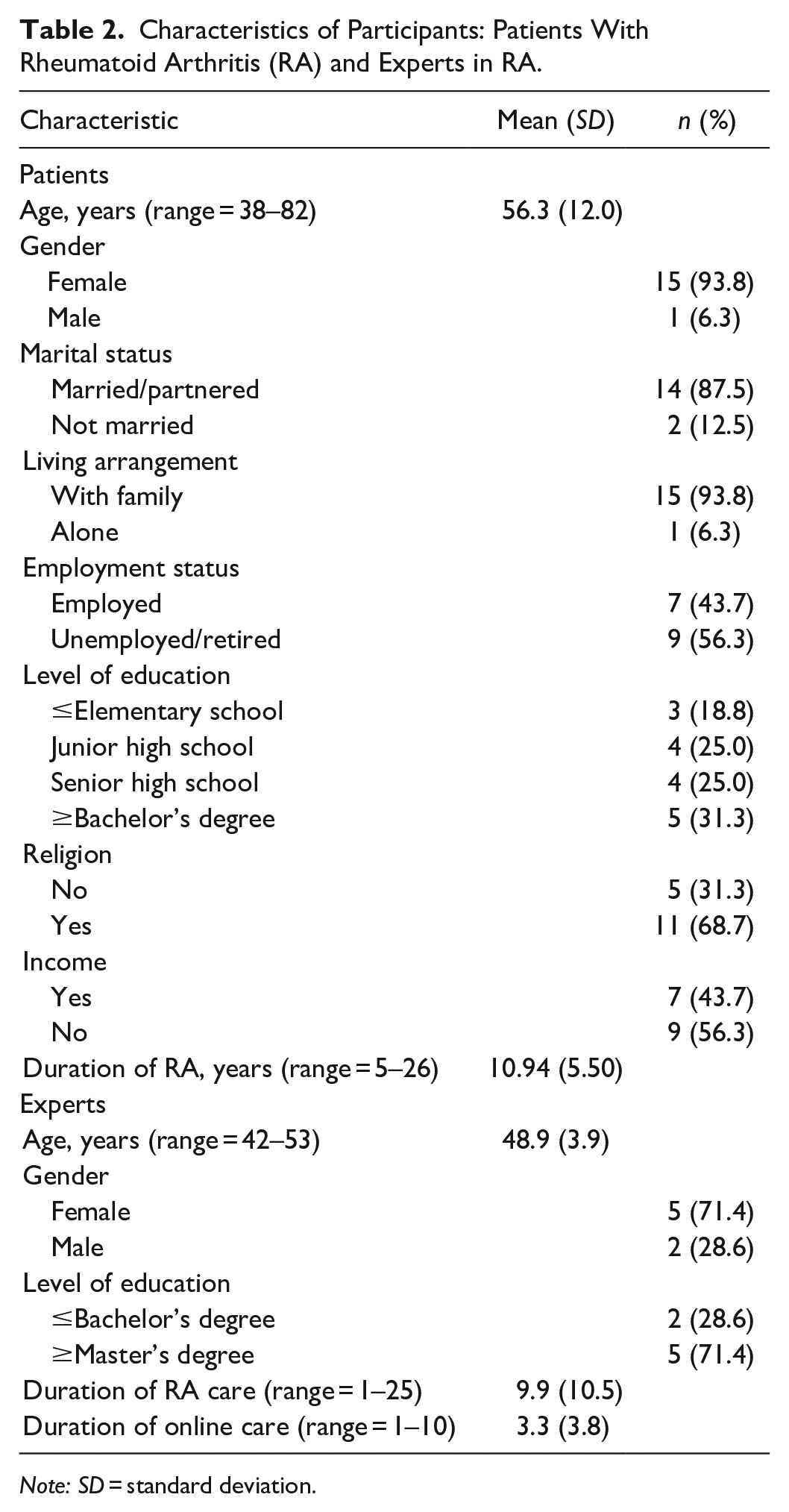
Note: SD = standard deviation.
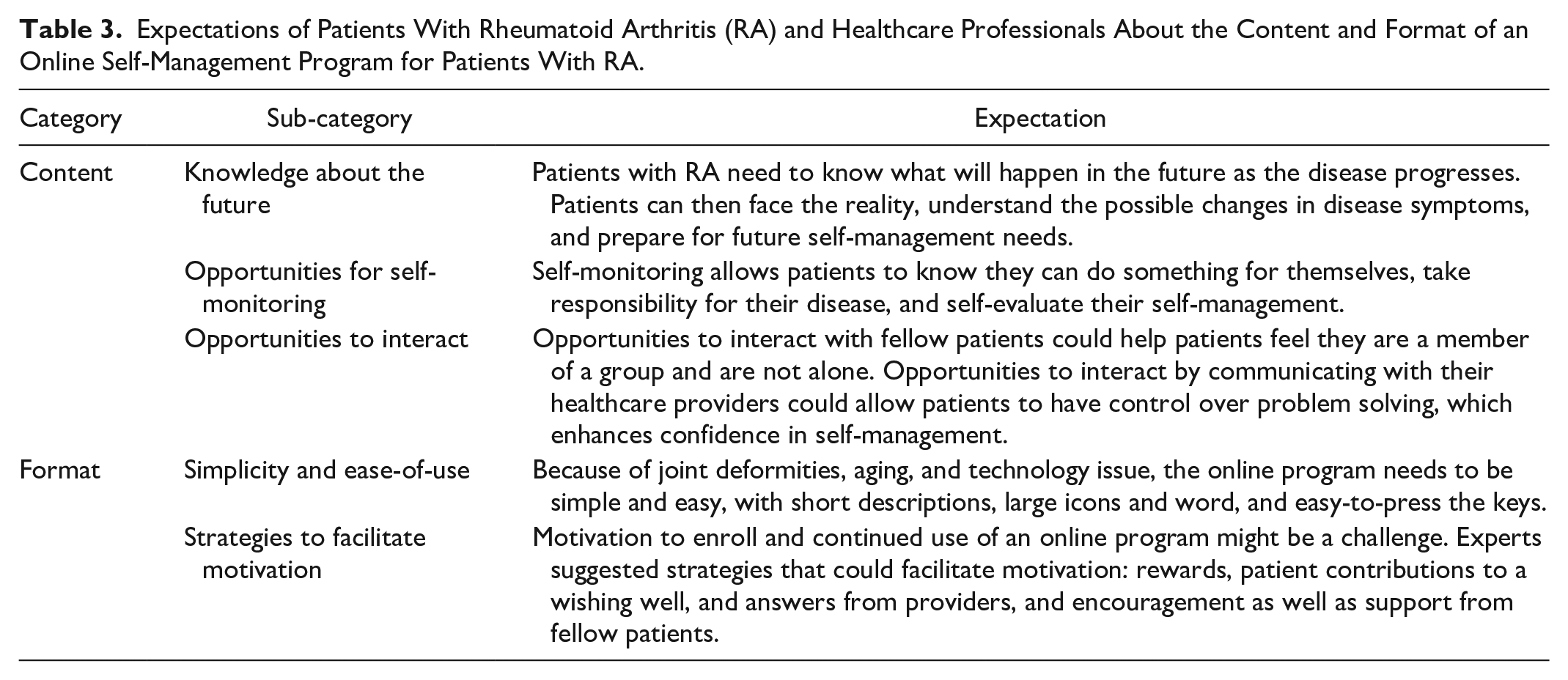
Patients and professionals identified five common expectations of an online self-management program for RA: information about how RA would impact future health status; opportunities for self-monitoring; opportunities for patients to interact with their healthcare providers and fellow patients; program simplicity and ease-of-use; and strategies for facilitating patient motivation. Across the common expectations, the five subthemes two overarching themes were formulated: “content of the program” and “format of the program.” An overview of the analysis is presented in Table 3. Details and supporting quotations are described in the following sections.
Expectations of Patients With Rheumatoid Arthritis (RA) and Healthcare Professionals About the Content and Format of an Online Self-Management Program for Patients With RA.
Expectations About Content of the Program
Information About How RA Would Impact Future Health Status
The first category addressed expectations that the program would provide information about what might happen in the future for patients with RA. Patients and experts agreed that knowledge of the disease trajectory of RA could be an incentive for incorporating self-management skills. Patient #16 said, “To me, the most important thing is to know what will happen in the future, and then I will know how to respond and cope.” Importantly, patients also commented that information provided by the online program should include information they need, but that healthcare staff are unable to provide because of time constraints. Patient #12 said, “My doctor and nursing staff seem too busy and look as if they are in a hurry. I don’t dare to ask what’s next for my disease.”
The expert participants also suggested that patients with RA need to have adequate information about the whole picture of RA which can enable the patient to be more cognizant of worsening of symptoms. Expert #4 suggested, “Patients should know the possible prognosis of their RA, and the problems they may face, so they will be more able to perform self-management of their disease.” Expert #2 said that information could help patients adjust their living environment in advance: “If patients realized how the disease can progress, then they can adjust their environment appropriately, for example, preparing barrier-free and safe arrangements of their living environments.”
Opportunities for Self-Monitoring
Patients described having expectations that the program would allow them to record changes in symptoms of RA, such as the condition of their joints. An 82-year-old female (Patient #9) said: “I would like to record the condition of my joints.” Another patient (#16) also had similar expectations: “I would like to record my condition, and then I will know if a strategy is or is not working for me.” A female patient expressed a desire share her progress with her physician: “When I go to the outpatient clinic, my doctor always asks me, ‘How you have been since your last visit?’. If I can use this online program for recording, I can show it to the doctor directly” (#12). Some patients were not interested in recording their progress for themselves, but in order to provide their physician with evidence of how hard they were working to manage their disease. Patient #9 (the 82-year-old female) said: “If I can show my record to my doctor, he will know my condition completely, and know that I care and work hard to manage my disease.”
Opportunities for self-monitoring were also expectations of the experts because they believed it would encourage patients take responsibility for their disease. Our nursing professional (Expert #7) said, “Self-monitoring is very important for building the self-management skills because it allows patients to do something for themselves and take responsibility for their own health.” Another expert in clinical nursing (Expert #3) provided the following example: On the one hand, self-monitoring allows patients to become aware of areas needing strengthening. On the other hand, improvements in self-management behaviors will be even greater, because the satisfaction they will feel when they evaluate their progress will allow them to experience a sense of achievement.
Opportunities for Interactions
Most patients with RA reported an online program should provide opportunities to interact with fellow patients as well as healthcare providers. They wanted to know about the disease status of other patients, learn about and discuss others’ experiences with RA, and hear about how they dealt with RA. We found the older the patient, the more likely they were to mention wanting to interact with fellow patients. Two participants, a 77-year-old (Patient #3) and an 82-year-old (Patient #9) said: “. . . hope to have the opportunity to share my own experiences of RA with other patients and to know how they deal with this disease.”
Patient expectations of the program also included having more opportunities to interact with their doctor. This was partly due to feeling stressed and uncomfortable during face-to-face interactions with their doctor, which was described by a 58-year-old female (Patient #8), who said, “I am afraid of talking with my RA doctor because I worry about whether my questions make sense.” A second participant (Patient #3) reported feeling she could not reliably count on having time to talk with her doctor during office visits, and hoped the online program would increase interactions, saying, “There is not much time to sit and talk with my doctor. If the program gives me more opportunities for discussions with my doctor, I will use them.”
Most of our experts also expected the online program could strengthen opportunities for interactions with patients and healthcare providers compared with traditional programs because patients would view the online program as user-friendly technology. One expert (#1) said, “Providing an interactive mode allows patients to feel that this program is human-focused.” Another expert (#5) said, “This program can be similar to an online group, making patients feel that they are not alone.” One nurse (Expert #3) suggested: “Interactions between patients is important; they can share what we can’t give them, and they can learn from and help each other.” Another expert (#7) provided details for how patients could obtain feedback from their healthcare providers: “The program needs to build an interactive platform available on a 24-hour basis, to manage and answer patients’ questions. This would be similar to an online consultation.”
Expectations About Format of the Program
Simplicity and Ease-of-Use
Most patients were emphatic about their expectation that the program needed to be simple and easy-to-use because their knowledge of technology was limited. One patient (#14) said, “We are getting older, and we are not good at high-tech things. If it is easy to use, I think I will like it.” In addition to simple technology, patients also expected the online program should be easy to use. Patient #9 said, “I suggest it should be simple and easy to operate.” In order to facilitate the use of this online program, participants suggested someone be available to provide technical support, if and when problems are encountered, to help with problem-solving.
The format of the online program being simple and easy to operate was one of most important expectations of our experts. They provided specific suggestions to achieve this goal of simplicity and ease-of-use, which included the use of large icons and text, wording that was easy-to-read and understand, and descriptions that were brief. A noteworthy finding was provided by three experts, who emphasized the importance of considering issues surrounding finger joints for patients with RA. One nursing professional (Expert #1) said, “Most patients with RA have deformed fingers. Therefore, this online program should reduce the fine movement of the joints in the hand as much as possible.” A nurse practitioner (Expert #5) echoed this suggestion saying, “The joints of the hands of patients with RA may be stiff and painful. Therefore, the design of all facets of the online program should take into account joint limitations as a primary consideration.” To achieve the goal of simplicity and ease-of-use, one nursing professional (Expert #7) suggested: “use pictures, symbols, and videos, and reduce the amount of descriptive text.”
Strategies to Facilitate Motivation
Several patients were concerned that they might be reluctant to enroll or fully participate in an online program. We found these issues to be noteworthy indications that facilitation of patient motivation might be required. For example, one 53-year-old female patient (#16) said: “I usually go online for daily needs, such as shopping, but I don’t think I can use it for my health.” Although many patients were used to using the Internet, these tended to be searches for health resources for family members, not themselves. One patient (#8) said, “Usually, I go online to check my family’s health problems, shopping, or just for fun, but I do not check my own [health problems].” Participants were uncertain they would use an online program for their health and concerned the online program would interfere with the care they needed from their doctor. Patient #8 said, “I need my doctor to take care of me. If I use the online program, will he continue to provide my care?” Another patient (#16) worried their doctor would no longer be available to assess their symptoms of RA: “If I use the online program, I worry that my doctor or my nurse will not try to figure out how swollen my joints are, or the pain level I have.”
The experts in RA commented that online healthcare was not like in-person care or self-management programs, which might make it difficult for patients to maintain their enthusiasm. A nursing professional (Expert #3) said: “I think the big issue for online program is motivation, because it is difficult for patients to be diligent about participating consistently with this type of program. Patients might discontinue use of the app.” The experts suggested several strategies patients could use to facilitate motivation to enroll in the program and maintain participation. One expert (#7) offered this solution:
Build a wishing well and encourage patients put their wish or idea into the well as a question/comment. Then, provide a link to wishes/ideas with responses. This could help patients’ feel they are contributing to the program and also provide recognition from their healthcare provider.
Expert #1 suggested providing incentives for continuous participation, such as earning a gift card or earning credits toward a reward, saying, “Developing a rewards incentive will let patients know of our [healthcare providers’] concern, which will indicate they [the patients] are not alone.” The incentives would not only facilitate patient motivation, but also indicate the healthcare providers were aware of the patients’ hard work. Expert #1 also made an additional suggestion: “Another strategy to help patients continue to use an online program is to take advantage of interactions with other fellow patients. This would foster a sense of comradery and the feeling that all patients are working together.”
Discussion
This study explored expectations of an online self-management program for patients with RA, which was from the perspective of patients with RA and experts in RA healthcare. The main themes and subthemes identified when interview data from patients and experts were analyzed were comparable. Both groups described expectations of the content and format when designing an online program for self-management of RA. Findings showed there were consistent expectations but different perspectives among patients and experts, including providing sufficient disease information, having the function of self-monitoring, being able to interact with follow-patients and healthcare providers, and being simple and easy. Moreover, experts emphasized the importance of an online program including strategies to enhance motivation of patients.
Patients expected the online program to function as a self-monitoring device. Experts also thought opportunities for self-monitoring were important because it could improve a patient’s ability to take responsibility for their own health. Nguyen et al. (2018) surveyed patients with gout to determine what they might desire in a disease self-management app; most were attracted by the ability to self-monitor using online tracking with a built-in diary. Other studies have shown the use of an online diary increases a patient’s awareness of their progress in self-management and provides results that can be discussed with their healthcare team, which allows patients to better cope with their disease (van Kruijssen et al., 2015), and recognize their strengths and limitations (Prothero et al., 2017).
Patients wanted the online program to offer opportunities to interact with fellow-patients and healthcare providers. The experts agreed fostering these interactions were important to include in the content of the program and also one of the strengths of online program compared with traditional programs. Interactions with fellow patients have the benefit of providing a sense of comradery as a member of a group, which can help patients realize they are not alone with their disease (des Bordes et al., 2018; Dwarswaard et al., 2016). Rask et al. (2021) also found that patients with chronic disease expressed a need for seeing other patients to learn how they successfully managed their daily life. Rask et al. (2021) commented that it was of utmost importance to the patients that the online program offer hope, positive experiences, and effective strategies through interactions with their fellow patients.
Interactions with healthcare staff increase communication between the patient and their medical staff, which can facilitate problem solving and enhance confidence in self-management (Bywall et al., 2019; Dwarswaard et al., 2016). Most patients in our study reported they had few opportunities or were reluctant to talk with their doctor or medical staff during in-person visits. However, their expectation was the online program would allow them to interact with their doctor and they would feel more comfortable sharing their concerns online rather than in-person. The development and use of an online RA self-management program could increase these interactions. Therefore, development of online self-management programs for patients with RA with should be encouraged.
Patients and experts were aware of the need for simplicity and ease-of-use for the format of the online program. Patients admitted they had limited “high-tech skills.” In Taiwan, 32% of patients with RA have an educational level that is less than sixth grade (Shao et al., 2021). Therefore, an online self-management program for patients with RA in Taiwan should be easy to use. It was also suggested support be available around the clock for troubleshooting, should any problems arise. The experts suggested that limitations of finger dexterity, which diminish as fingers become swollen, stiff, and painful, would require keyboards also be easy to use. A Swedish study by Bywall et al. (2019) reported patients with RA preferred to participate an online program because it was easier than painfully grasping a pen to write (Bywall et al., 2019). Moreover, the experts agreed that providing patients with easy access to self-management tools will promote their motivation (Rask et al., 2021).
It is noteworthy that some patients in our study had a relatively negative or passive attitude toward using an online program. Reasons included lack of interest in personal online health information, concern that participation might negatively affect their relationship with healthcare staff including what their doctor thought of them, and worry their doctor might be inattentive about assessing their health status. Other patients reported their interest in participating was not to improve self-management of RA, but to demonstrate to their doctor how hard they worked to manage their disease. These issues might not only prevent patients from using an online program, but also might also prevent them from sustained participation.
The demographic characteristics need to be considered when developing an online self-management program. Many patients with RA in Taiwan have been reported to have an educational level less than sixth grade (32%) and most practice Buddhism or Taoism (67%, Shao et al., 2021), these factors may contribute to poorer attitudes toward health (Chen & Shao, 2012; Chen et al., 2016). These characteristics can also make it difficult to incorporate changes in behaviors due to cultural influences (Chen & Shao, 2012). Individuals in Chinese cultures often adopt a fatalistic attitude toward their health condition, which is often reflected in a passive attitude about taking control of a disease because health is subject to the will of God or fate (Chen & Shao, 2012). This passivity was described by a participant in a qualitative study of patients with heart disease: “We have an old saying that to keep our health, the first priority is God, and the second is the doctor” (Chen et al., 2016, p. 809).
An additional influence may be due to gender and the role expectations for women in Taiwan. Nearly all patients with RA in our study were female. Taiwanese women are not expected to look after themselves, but to care for other family members (Chen et al., 2016; Shao et al., 2015), and tend to rely on their doctor rather than take personal responsibility for managing their health (Chen & Shao, 2012). Women with RA in Korea also prioritize their family’s health over their own and have reduced levels of self-care competence (Sok et al., 2019). This highlights the importance of enhancing the individual’s responsibility for their own health. The online program could play an important role in supporting patients in their own environment and reducing dependence on needing continuous contact with healthcare providers (Rask et al., 2021).
Our experts also agreed that patients might be reluctant to participate in an online program and maintain motivation to continue with the program. Unlike face-to-face traditional programs, online programs lack in-person interactions, which make it difficult to sustain enthusiasm, and rely much more heavily on the active engagement of the user (Whitehead & Seaton, 2016). Most online programs focus on providing educational information to participants, whereas many self-management programs in Taiwan have been conducted in an outpatient clinic (Chen et al., 2017; Shao & Chen, 2019; Shao et al., 2021) and thus, patients’ motivation is often a result of in-person contact with nurses and physicians. A systematic review of the literature on how self-management programs were offered for patients with a chronic disease included group therapy, one-on-one therapy, telephone interviews, and telehealth, which can assess motivation directly (Kuo & Wang, 2012). However, how motivation can be improved to maintain participation was not explored. Therefore, an important aspect of our online self-management program was including activities to increase motivation and sustain participation. Our experts suggested incorporating strategies that included encouraging patients to add wishes or ideas about their symptoms or progress to a site labeled as a “wishing well” and they received feedback from healthcare staff. Offering participants incentives for advances in goals, such as gift cards or points, and receiving support from fellow patients reinforced and strengthened participants’ motivation to continue with the program.
Limitations
The mean age of patients in this study was 56.3 years. Although ages ranged from 38 to 82 years, views of younger patients were not adequately captured, which might prevent generalizing our findings to a broader population of individuals with RA. Nearly all participants in our study were female (93.8%), and rheumatoid arthritis disproportionately affects more females than males (WHO, 2020). This uneven gender distribution prevents generalizing our findings to males’ experiences and future research should examine expectations of male patients with RA about an online program. A third limitation was the duration of time since receiving a diagnosis of RA (range = 5–26 years). We did not exclude patients with a lengthy disease duration, which may have increased the confounding effects of comorbidities usually associated with a longstanding disease. Lastly, our participants were recruited from only one medical center and data were collected only from participants with Internet access who were willing to share personal information about their expectations regarding an online RA self-management program. Patients with RA had no Internet access or were not interested in participating might have different opinions. Therefore, our findings may not be transferable to the general population of patients with RA in Taiwan.
Conclusion
This study brings a new perspective of understanding expectations of patients and experts regarding an online RA self-management program. Our qualitative study interviewed not only experts in RA but also patients with RA, which provided perspectives of what would be important for the end-users. Our research findings suggest the design of an online self-management program should consider the specific needs and cultural influences of patients with RA, for example, being aware of their hand joint problems, understanding the reluctance to reduce in-person time with their doctors, and recognizing fatalistic orientations. Strategies should be adopted to encourage and increase patient’s motivation and confidence, such as building a wishing well, delivering timely feedback, and providing support through connections with their fellow patients and healthcare providers. Nurses are well positioned to overcome those issues. The use of online delivery of a self-management program for patients with RA can readily be delivered by nurses in clinical care practices to help build lifelong disease self-management skills.
Footnotes
Acknowledgements
The authors wish to thank the director and staff of the Chang Gung Memorial Hospital at Linkou, Taiwan, for their friendly support, and to acknowledge the participants who provided invaluable data for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Technology, Taiwan (MOST 107-2314-B-255 -003-MY3).