
Abstract
In this study was to determine knowledge of cardiovascular disease (CVD) risk factors and to explore related factors among adults with type 2 diabetes mellitus (DM) who have not been diagnosed with CVD. This descriptive study was conducted with 175 adults. Data were collected individual identification form and Cardiovascular Disease Risk Factors Knowledge Level (CARRF-KL) scale. A negative correlation was found between age and CARRF-KL score. A significant difference was found between educational status and CARRF-KL score. The individuals described their health status as good, managed their condition with diet and exercise, received information from nurses, adults with DM in their family and those with no DM complications had significantly higher scores in CARRF-KL. The knowledge of an individual with DM about CVD risk factors should be assessed, CVD risks should be identified at an early stage, and individuals at risk should be subjected to screening.
Introduction
Cardiovascular diseases (CVD) are increasing internationally and are the leading cause of death around the world (WHO, 2021). However, management of CVD risk factors has the potential of decreasing mortality by half. Although there are many risk factors that are cited with respect to CVD, the most important one is reported to be diabetes (International Diabetes Fedaration [IDF], 2021). Diabetes Mellitus (DM) is a chronic metabolic disease with increasing prevalence internationally (WHO, 2021). Over time, individuals with DM develop various microvascular and macrovascular complications. CVD is one of the most serious complications of DM (American Diabetes Association [ADA], 2020). The complications of DM are generally an indication that individuals are not managing their condition satisfactorily (Yılmaz et al., 2018). The frequency of CVD is two to four times more in individuals with diabetes, and the mortality risk in these individuals is higher than in non-diabetics (IDF, 2021). Moreover, type 2 DM is responsible for more than half of deaths due to CVD. With the rapid increase in type 2 DM, the concern lies in both the vast prevalence as well as the major complications that accompany diabetes, especially CVD (Glovaci et al., 2019).
Although there are many factors that cause CVD in individuals with diabetes, The most important factors are endothelial dysfunction and atherosclerosis (Glovaci et al., 2019). By ensuring control over the risk factors of CVD and making sure a normal glycemic level is reached, atherosclerotic progress in the arteries, is slowed which helps to prevent thrombotic events, as well as reduces death rates (Bertoluci & Rocha, 2017; Keskin & Balci, 2011). Due to the strong correlation between DM and CVD and in light of the new mortality risk involved, robust DM health management should be provided (ADA, 2020). One of the fundamental treatment goals of DM management is to keep CVD risk factors under control (TC. Ministry of Health, 2020). The major strategy to be used in achieving this goal is to ensure that individuals are aware of CVD risk factors and protect themselves from the disease. It is of vital importance that individuals become sufficiently knowledgeable about CVD risk factors. Non-modifiable risk factors for CVD are considered to be age, gender, and a history of CVD at an early age in a close relative, while modifiable risk factors are believed to be smoking, DM, dyslipidemia, hypertension, abdominal obesity, psychosocial factors, insufficient intake of fruit and vegetables, excessive alcohol consumption, and inadequate physical activity (Ayraler et al., 2018; Bartels et al., 2007; Bertoluci & Rocha, 2017; IDF, 2021). It is beneficial for adults with DM to increase their levels of knowledge about CVD risk factors to be better equipped to protect themselves from CVD and to adopt and implement healthy lifestyle behaviors. Favorable CVD risk factor knowledge levels have a positive effect on DM management (Yılmaz et al., 2018).
Various studies from different communities about CVD risk components were evaluated (Andsoy et al., 2015; Baysal et al., 2014; George & Andhuvan, 2014). Such studies typically focus on risk data or on identifying individuals’ CVD risk factors (Ayraler et al., 2018; Bartels et al., 2007; Bertoluci & Rocha, 2017; Lorber, 2014). However, the number of studies on CVD risk factors in individuals with type 2 DM is limited in Turkey (Yılmaz et al., 2018; Zehirlioglu et al., 2020). There are few studies regarding this subject in other countries as well (Patneik et al., 2013; Saeedi et al., 2020; Tovar & Clark, 2015; Wagner et al., 2006). Several studies have shown a significant relationship between the level of knowledge about CVD risk factors and weight control, nutrition, physical activity, stress management, and other positive behavioral changes (Çürük et al., 2018; Tovar & Clark, 2015; Yılmaz et al., 2018). Individuals with DM and other high-risk individuals in the community must be identified and priority should be given to determine these individuals’ level of knowledge about CVD risk factors so that they can be protected from cardiovascular events (Arıkan et al., 2009; Howard, 2014).
In summary, CVDs are the number one cause of death globally (IDF, 2021). The risk of developing CVD is higher in individuals with DM compared with those who do not have DM and CVD is a leading cause of death in those living with type 2 DM (Saeedi et al., 2020). Therefore, it is important for individuals with DM to be aware of CVD and related risk factors. The purpose of this study was to identify the knowledge of CVD risk factors and to explore related factors among adults with type 2 DM.
Methods
Research Design and Sample
This descriptive study was conducted with adults with type 2 DM who had applied to an internal medicine clinic at a university hospital located in the western part of Turkey between May and August 2019. The population of the study consisted of 500 with adults with type 2 DM. The sample was selected randomly by the multiclustered stratified sampling method. We used the formula: n = N · t2 p q/d2 (N + 1) + t2 · p q, to determine the size of the sample. The minimum size of the sample was determined to be 165. Adults with type 2 DM diagnosed with CVD, under the age of 18, with a communication disability or those not willing to participate in the research were excluded. During the data collection period, 238 adults with type 2 diabetes were reached. Those adults who did not want to participate in the study (n = 26) and could not fully answer the research questions (n = 14) were also excluded from the study. Adults with type 2 DM diagnosed with CVD (n = 53) were not included in the study. Thus, 175 adults with type 2 DM composed the final sample.
Data Collection and Instruments
Data were collected using the individual identification form and the Cardiovascular Disease Risk Factors Knowledge Level (CARRF-KL) scale.
The individual identification form
This form was developed by the researchers and included five questions about socio-demographic characteristics such as age, gender, marital status, educational level, economic status, three questions about health status (health perception, diabetes treatment, compliance with treatment), and seven questions about CVD risk factors such as duration of DM, body mass index, history of DM in the family, DM complications, presence of other chronic diseases, smoking, and physical activity levels (ADA, 2020; Calti Gur et al., 2013; Howard, 2014; Uçar & Arslan, 2017; Yılmaz et al., 2018). The adults’ metabolic parameters, such as fasting plasma glucose (FPG), 2-hour post-prandial plasma glucose, estimated average glucose (HbA1c), high density lipoprotein (HDL), low density lipoprotein (LDL), triglycerides, and total cholesterol were obtained from the individuals’ latest laboratory test result reports. Height and weight measurements were recorded based on self-reports and Body Mass Index (BMI) was measured a person’s weight in kilograms divided by square of height in meters. The researcher took the participants’ blood pressure and reported as systolic blood pressure (sBP) and diastolic blood pressure (dBP). For assessing physical activity levels, individuals were asked whether they did regular exercise by explaining what is meant by regular exercise.
The Cardiovascular Disease Risk Factors Knowledge Level (CARRF-KL) Scale-Turkish Form
This Turkish scale was developed and tested for validity and reliability (Arıkan et al., 2009). The scale comprises 28 items. The first 4 items are related to the characteristics the CVD, regarding, prevention and age; 15 items pertain to risk factors, and 9 items query the changes occurring in risk behaviors. The items on the scale are formulated in the form of complete sentences that the participants identify as correct or incorrect; their responses are expressed as “Yes,” “No,” or “I don’t know. Every correct answer on the scale is scored as 1; six questions are reversely scored. The total possible score on the scale varies between 0 and 28 with no cut points for knowledge levels. The higher the score, the higher the level of knowledge. Cronbach’s alpha value on the original scale was 0.76 (Arıkan et al., 2009). The scale has also been used for individuals with DM (Yılmaz et al., 2018; Zehirlioglu et al., 2020). The alpha coefficient of the scale found in this study was 0.87.
Data were collected by the researchers via one-to-one interviews with the adults and notations were made with pen and paper. The questionnaire took 15 to 20 minutes for every individual to complete.
Ethical Considerations
Written approval and permission for the study were obtained from the University Ethics Committee (19-9.1T/58-09.18.2019) and from the university hospital prior to implementation. And also, each adult was informed about the content of the study and written consent was acquired.
Data Analysis
Data were analyzed using SPSS 23.0 for Windows (SPSS Inc., Chicago, IL, USA). Descriptive statistics (numbers, percentage distribution, means, and standard deviation) were used to describe the adults’ socio-demographic characteristics, health status and scale scores. The independent sample t-test, ANOVA test, Kruskal Wallis analyses, post hoc test (Tamhane’s), Mann Whitney U-test, and Pearson’s product moment correlation were used to assess associations between scores and variables. Multiple regression analysis was used to identify the factors contributing to CVD risk factors knowledge of adults with Type 2 DM. Statistical significance was defined as p < .05.
Results
Socio-Demographic Characteristics of the Adults
The mean age of the adults with DM was 65.35 ± 10.75 years (min: 31, max: 91); 53.7% of the adults were females. The other sociodemographic characteristics of the adults are shown in Table 1.
CVD Risk Factors Knowledge According to Sociodemographic Characteristics and Health Status of Adults (n = 175).
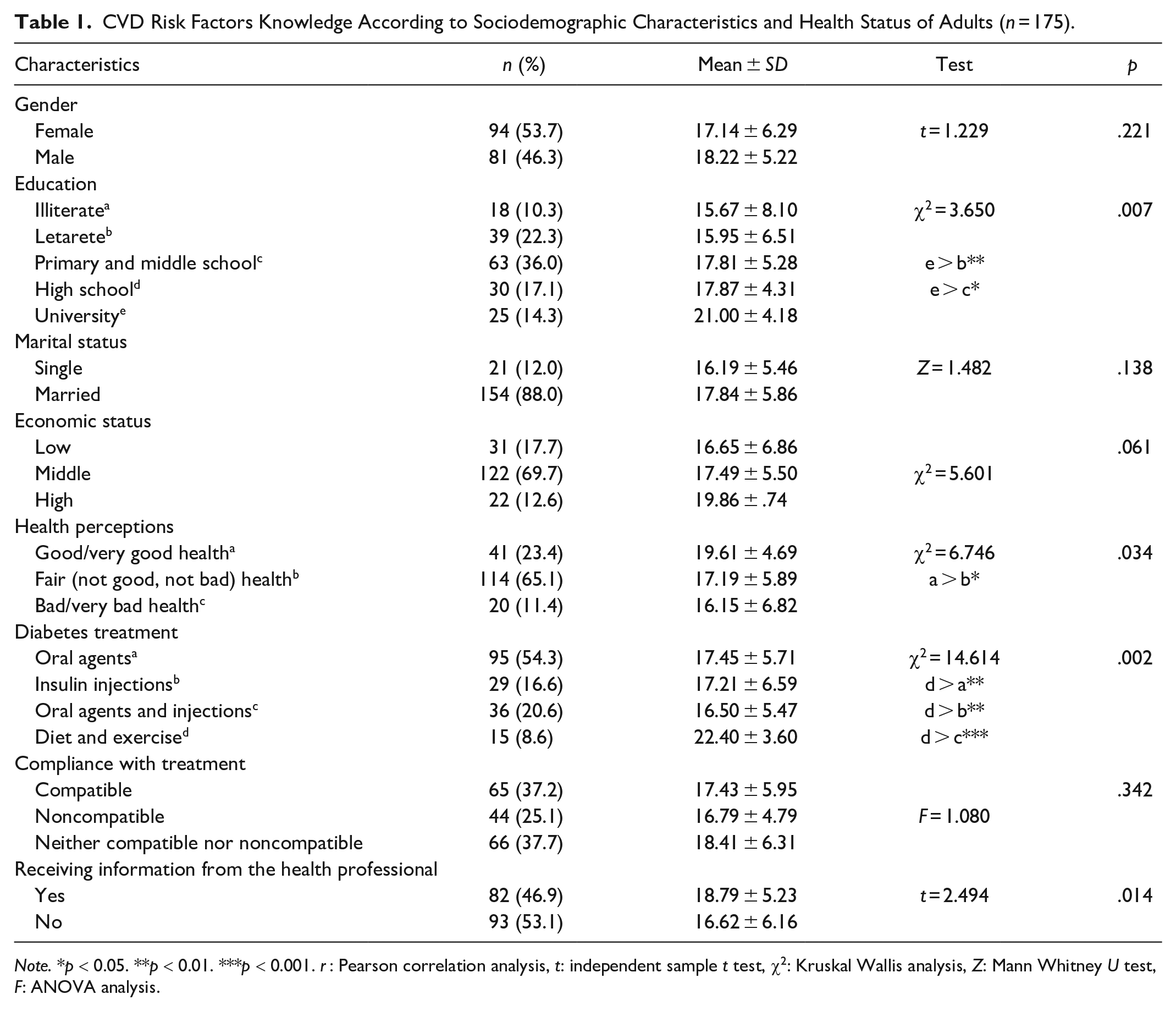
Note. *p < 0.05. **p < 0.01. ***p < 0.001. r: Pearson correlation analysis, t: independent sample t test, χ2: Kruskal Wallis analysis, Z: Mann Whitney U test, F: ANOVA analysis.
Health Status of the Adults
Adults (65.1%) described their general health to be average, 54.3% were on oral antidiabetic agents, 16.6% on insulin injections, and 20.6% on oral agents and injections. Of these adults, 8.6% were following a regime of diet and exercise for DM treatment, 25.1% did not comply with their treatment, and 53.1% had not received information from nurses about their condition (Table 1).
Cardiovascular Risk Factors and Clinical Features of the Adults
Table 2 displays information on the metabolic parameters of the adults with DM. The mean sBP was 128.92 ± 18.71 mmHg; the mean dBP was 78.41 ± 14.08 mmHg. Mean FPG level was 136.59 ± 37.57 mg/dL; while mean total cholesterol level was 196.68 ± 41.86 mg/dL, mean HDL level was 50.23 ± 24.35 mg/dL, mean LDL level was 150.02 ± 58.57 mg/dL, mean triglycerides level was 185.22 ± 68.82 mg/dL, and mean HbA1c level was 8.12 ± 1.96 mg/dL.
CVD Risk Factors Knowledge According to Cardiovascular Risk Factors and Clinical Features of Adults.
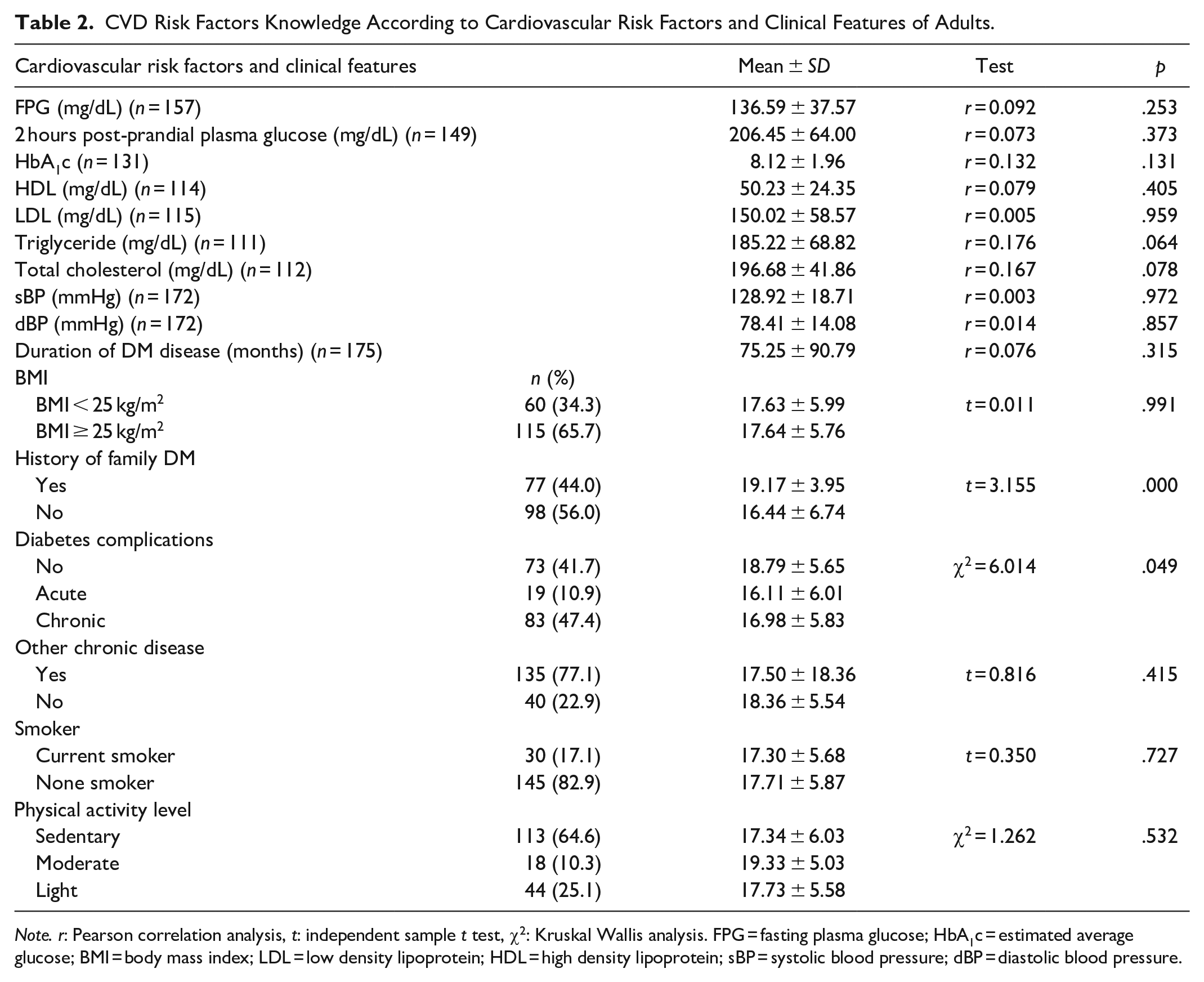
Note. r: Pearson correlation analysis, t: independent sample t test, χ2: Kruskal Wallis analysis. FPG = fasting plasma glucose; HbA1c = estimated average glucose; BMI = body mass index; LDL = low density lipoprotein; HDL = high density lipoprotein; sBP = systolic blood pressure; dBP = diastolic blood pressure.
The mean duration of DM in the group was 75.25 ± 90.79 months (range: 1–91 months). The mean BMI was 28.32 ± 5.86 kg/m2; in 65.7% of the adults, BMI was ≥25 kg/m2. Of the adults, 44 % had close relatives with DM and 77.1% had close relatives with some other chronic illness. Among the adults with DM, 58.3% had developed diabetes-related complications, 17.1% were smokers, and 64.6% were sedentary (Table 2).
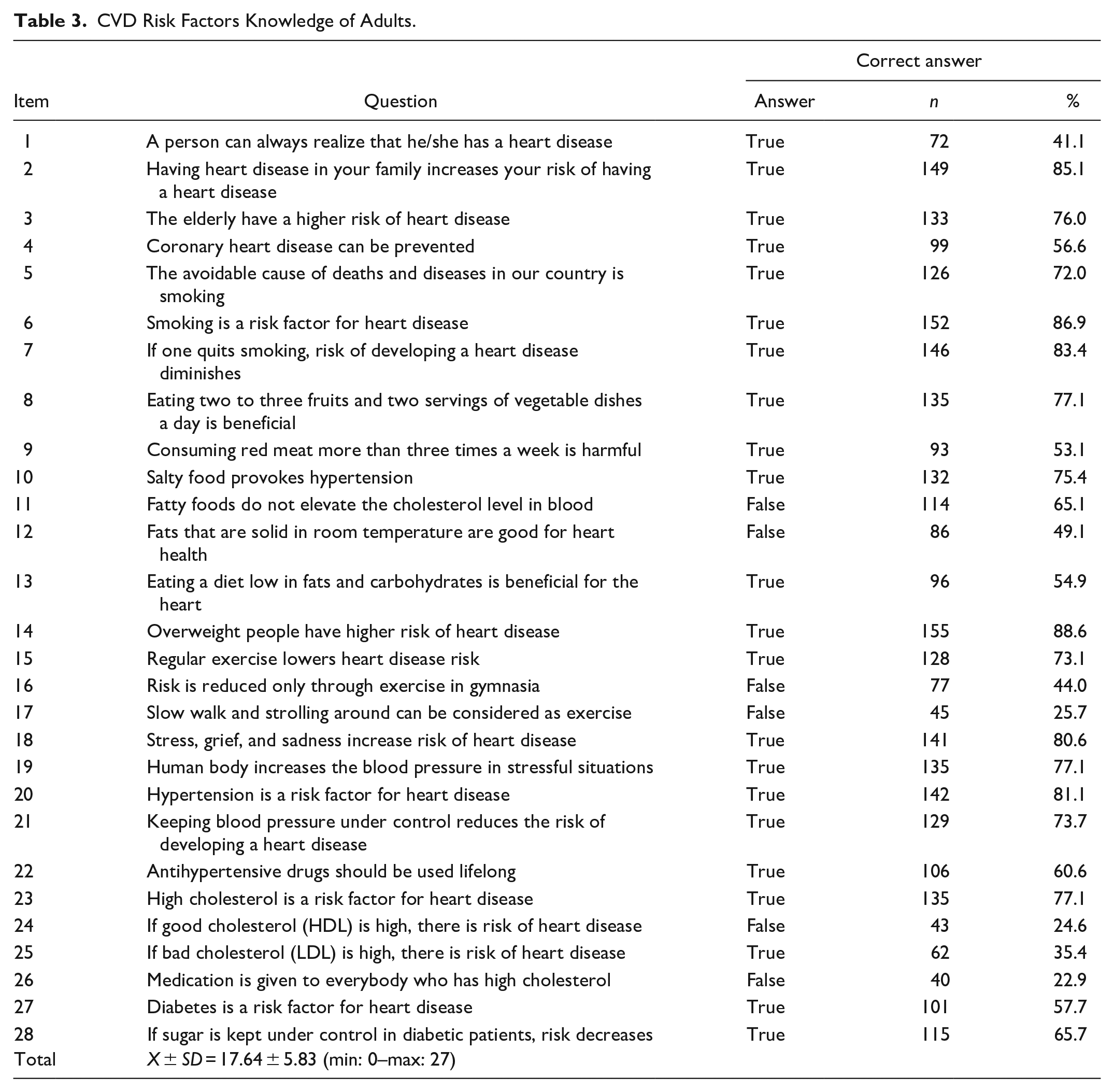
CVD Risk Factors Knowledge
The mean score of the adults on the CARRF-KL scale was 17.64 ± 5.83 (min: 0–max: 27; Table 3). Investigators found that overweight individuals (88.6%), smokers (86.9%), and those having heart disease in the family (85.1%) were the ones with the highest percentages of correct answers on the CARRF-KL. The items “Medication is given to everybody who has high cholesterol” (22.9%), “If good cholesterol (HDL) is high, there is risk of heart disease” (24.6%), “Slow walking and strolling around can be considered exercise” (25.7%) were the questions that revealed the lowest percentage of correct answers.
CVD Risk Factors Knowledge of Adults.
Related Factors: Sociodemographic Characteristics
A negative correlation was found between age and CVD risk factors knowledge score (r = −0.215, p = .004). A significant difference was found between educational status and the mean knowledge score. The adults’ mean knowledge score increased as the level of their education increased (F = 3.650, p = .007). There was no significant difference between the adults in their CARRF-KL scores in terms of gender, marital status or economical status (p > .05; Table 1).
Related Factors: Health Status
Those who described their general health as good/very good compared with those who described as bad/very bad (χ2 = 6.746, p = .034) and adults who managed their condition with diet and exercise had significantly higher scores than those who were being treated with oral antidiabetic agents and insulin (χ2 = 14.614, p = .002); those who received information from nurses (t = 2.494, p = .014) had significantly higher scores in Knowledge about CARRF-KL. There was no significant difference between CARRF-KL scores and DM treatment compliance (p > .05; Table 1).
Related Factors: Cardiovascular Risk Factors and Clinical Features
The CARRF-KL scores of adults with a family history of DM were found to be higher compared to those with no family history of DM (t = 3.155, p = .000). Risk factor scores of adults without DM complications were found to be higher compared with patients with complications (χ2 = 6.014, p = .049; Table 2).
No statistically significant difference was found between the adults in CARRF-KL score according to their clinical features (plasma glucose, HbA1c, HDL, LDL, triglycerides, total cholesterol, and blood pressure), body mass index, other chronic diseases, smoking, and physical activity level (p > .05; Table 2).
Variables Predicting CVD Risk Factors Knowledge of Adults
The multiple regression analysis performed with variables considered significant in paired comparison revealed that variables such as age, education, health perception, diabetes treatment, receiving information from the health professional, history of family DM, diabetes complications accounted for 17% of the CARRF-KL score of adults with Type 2 DM. (F = 4.703, p = .001, R2 = 0.17; Table 4).
Regression model Predicting CVD Risk Factors Knowledge of Adults (n = 175).
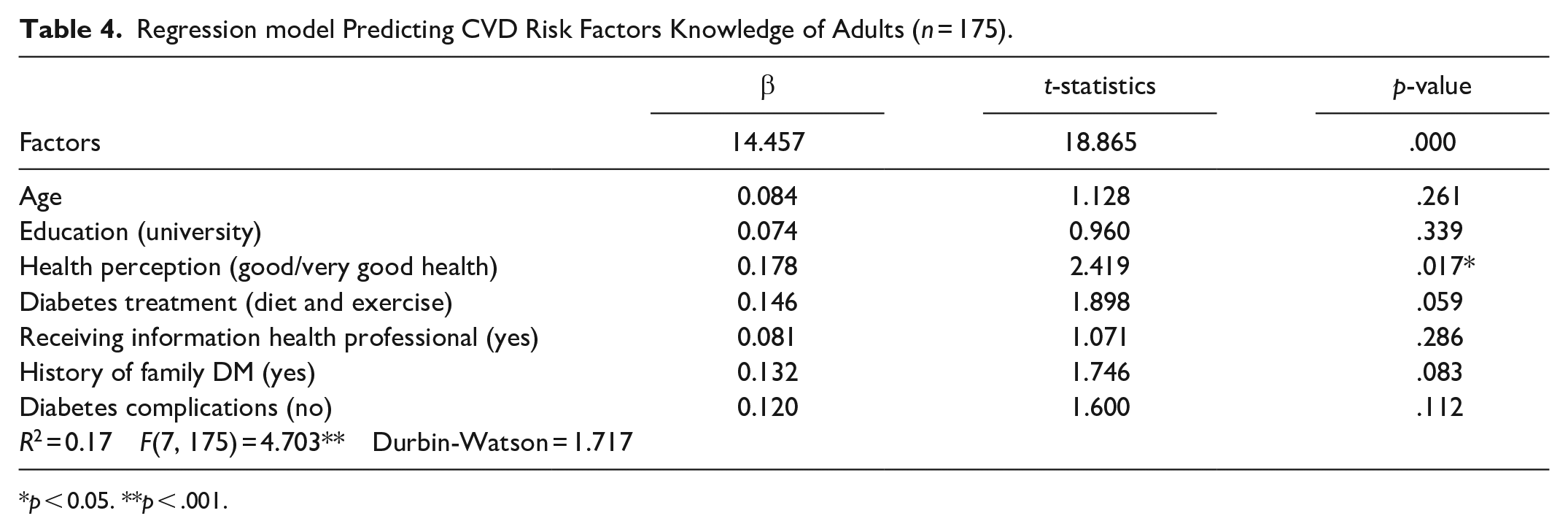
p < 0.05. **p < .001.
Discussion
Considering that in this study, the highest score possible on the CARRF-KL scale is 28, the participants’ knowledge level of CVD risk factors was moderate (17.64 ± 5.83). The moderate level of knowledge of adults with diabetes, a disease that increases the risk of CVD the most, is not at the desired level is an important finding. Another study for individuals with DM reported a low level of CVD risk knowledge (Wagner et al., 2005). In the a secondary study by Wagner et al. (2006), only approximately half of the participants could provide correct responses to the questions measuring their CVD risk knowledge. Another study conducted with adults who have DM indicated that more than half of the participants (68.5%) did not know that DM increased the risk of heart disease (Patneik et al., 2013). Saeedi et al. (2020) found that one-tenth of the participants with DM did not know about CVD risk factors and only one-sixth believed that they carried a high risk of developing CVD. In Turkey, Yılmaz et al. (2018) conducted a study for adults with DM and reported a CVD risk factors knowledge score of moderate, similar to our study findings. In another study and half of the participants with DM had heart disease, and their knowledge about risk factors was insufficient (Zehirlioglu et al., 2020). Kayaniyil et al. (2009) found that in individuals hospitalized due to coronary artery disease, it was shown that those with a history of DM had a lower level of knowledge about CVD compared to those who did not have the condition. According to the current literature, individuals with DM have an inadequate knowledge of CVD risk. This lack of knowledge about CVD among individuals with DM negatively affect their awareness and attitudes and constitutes a major barrier for disease control (Tan et al., 2013). Research emphasizes in the literature that individuals with a high level of knowledge about CVD risk factors acknowledge their risk in terms of CVD (Andsoy et al., 2015). Based on this knowledge, when individuals are aware of their condition and gather sufficient information about CVD risk factors, prevention and control of CVD is more likely to occur (Karakoç Kumsar & Taşkın Yılmaz, 2017; Sevinç, 2016).
This study revealed a negative correlation between CVD risk knowledge levels and age as. Similarly, Scalzi et al. (2008) found that age was a major determinant of CVD risk awareness and noted that awareness was at a better level in younger individuals. Although several studies report similar results (Tan et al., 2013; Zehirlioglu et al., 2020), there are also those that indicated that knowledge of CVD risk factors increases with age, etc., as well as studies that pointed out no correlation at all in this respect (Andsoy et al., 2015; Uçar & Arslan, 2017; Yılmaz & Boylu, 2016). Considering the decrease of knowledge levels in adults with increasing age obtained in this study and the different age knowledge level relationships in other studies, age alone is no determining factor. Researchers considered that individuals’ intellectual and educational levels may also be effective factors. Only 31.4% of the participants in this current study have an educational level of high school and above. In addition, the decrease in cognitive capacity with age and the acceptance of deviations from health as normal may distract individuals from seeking information to protect health.
The current study found that as the level of education increased, so did knowledge of CVD risk factors. Some studies about a correlation between educational level and CVD risk factor knowledge were also reported (Tan et al., 2013; Tovar & Clark, 2015; Uçar & Arslan, 2017; Wagner et al., 2006; Yılmaz & Boylu, 2016; Zehirlioglu et al., 2020). However Andsoy et al. (2015) did not find any relationship between knowledge of CVD risk factors and education. Higher education levels are accompanied by health literacy, cite which suggests that more educated adults have higher levels of knowledge about CVD risk factors.
Adults with DM who reported their general health as good had a higher level of CVD risk knowledge. In other studies, however, no difference was detected between adults’ general health and their CVD risk knowledge scores (Andsoy et al., 2015; Uçar & Arslan, 2017). This findings suggests that the relatively higher level of education of the participants in the study sample and their positive interest in their own health set the stage for a more positive self-perception of health and therefore was conducive to achieving a higher level of knowledge about CVD risk factors.
Besides taking antidiabetic drugs, lifestyle changes in terms of nutrition and exercise are among the main steps taken by individuals with DM as part of their treatment (ADA, 2011; TEMD, 2018). When individuals are sufficiently informed about CVD risk factors, they are more likely to develop healthy lifestyles that include a nutritious diet and exercising (Arıkan et al., 2009; Lorber, 2014). The present study showed that those who followed a lifestyle change course about disease had higher CVD risk factor knowledge scores. Same studies point out a correlation between knowledge about CVD risk factors and forming healthy lifestyle habits (Abdo et al., 2019; Çürük et al., 2018; Kumsar et al., 2015; Yılmaz & Boylu, 2016). Similar to the results of our study, Yılmaz et al. (2018) found that favorable CVD risk factor knowledge levels have a positive effect on DM management.
Adults with DM who were informed about their condition by nurses had higher CVD risk factor knowledge scores. Andsoy et al. (2015) also found that adults who had knowledge about their illness had higher scores. However, Zehirlioglu et al. (2020), did not detect a difference between CVD knowledge scores and whether study participants received DM education. DM education includes training about health lifestyle behaviors, DM treatments, and information about DM complications. Diabetes self-management education improves diabetes consequences. However, unfortunately, most individuals cannot benefit from this service effectively (Nassar et al., 2019). Patient education, which is important in the management of diabetes, is one of the basic roles of the nurse. As found in the present study, individuals receiving information about DM from nurses become more knowledgeable about complications such as CVD caused by DM. Being informed in this way will reduce or delay the risk of developing complications such as CVD in individuals with DM.
Studies have found that adults with DM, who had close family members with a history of heart disease had higher CVD risk factors knowledge scores (Abdo et al., 2019; Andsoy et al., 2015; Kumsar et al., 2015; Tan et al., 2013). These findings suggests that the experience of having CVD in the family increases an individual’s knowledge and awareness about the illness and its risk factors.
This study showed that half of the participants experienced complications, and those with DM complications had a lower level of knowledge about CVD risk factors compared to those who did not have complications. This finding suggests that knowledge about CVD risk factors has a positive effect on awareness about DM complications, and about their prevention and management. Wagner et al. (2006) reported a different result, stating that experiencing DM complications is not a variable that has an effect on knowledge about CVD.
In this study, the sociodemographic variables of gender, marital, and economical status did not display any difference in terms of CVD risk factor knowledge. But, some literature indicated that individuals and women in particular (Andsoy et al., 2015; Wagner et al., 2006; Yılmaz & Boylu, 2016), and with those high-income (Çürük et al., 2018; Wagner et al., 2006), have demonstrated higher levels of knowledge about CVD risk factors.
In the current study, no difference was found in levels of CVD risk factor knowledge in terms of compliance with DM treatment, the duration of DM, and some CVD risk factors in adults with DM (obesity, smoking, chronic disease, exercising status). The literature revealed that knowledge of CVD risk factor is higher among individuals with obesity (Kumsar et al., 2015; Uçar & Arslan, 2017), hypercholesterol (Andsoy et al., 2015), high LDL levels (Yılmaz et al., 2018), low glucose and cholesterol levels (Kaya et al., 2019), low blood pressure (Çürük et al., 2018), other chronic diseases (Uçar & Arslan, 2017), and non-smokers (Tan et al., 2013).
Conclusion
We found that knowledge of CVD risk factors was not at the desired level among adults with DM and that the level of knowledge differed according to the adult’s age, education, perception of general health, mode of treatment, whether or not information about the condition was received from nurses, whether or not there was a history of DM in the family history or if the adult suffered from DM complications.
The study showed how important it is to have adults with DM receive education about their condition from nurses to ensure that they develop an awareness about CVD risk factors. The health education to be provided to adults with DM about their condition should be offered as a priority to the risk groups that consist of those who are older adults, less educated, perceiving their general health to be poor, taking oral antidiabetics or insulin, and also experiencing DM complications. The education should contain information about CVD risk factors, prevention, and management. Our recommendations are that the knowledge of an individual with DM about CVD risk factors should be assessed during medical examination, CVD risks should be identified at an early stage, and individuals at risk should be subjected to screening and education by nurses.
Limitations
The results from this research cannot generalize to the entire Turkish population as it was conducted in only one hospital. Future studies can be conducted with larger samples in multiple locations. Another limitation was the collection of data (weight and height, DM complications, and physical activity levels) being based on patients’ self-reporting.
Footnotes
Acknowledgements
We thank Ege University Institutional Development Planning and Monitoring Coordinatorship (EGE-PIK) and Ege University Library and Documentation Department for their editing service.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.