
Abstract
The purpose of this study was to examine the level of loneliness and its relationship with socioeconomic and health conditions, social support, family functionality, and depressive symptoms in patients undergoing hemodialysis. This cross-sectional study involved analysis of a secondary data, collected in 2019 among 80 patients with CKD on hemodialysis. Participants completed the following instruments: socio-demographic, economic, and health condition characterization, UCLA Loneliness Scale, Medical Outcomes Study Social Support Scale, Patient Health Questionnaire-9, and the Family APGAR. On average, the sample was mostly female (55%), white (65%), and the mean age was 59.63 years. In the perception of loneliness, the highest index was (55%), moderately high. Social support scored the worst in the Positive Social Interaction domain. The prevalance of severe depression was approximately 29%. Family functioning was positive, with a good score (69%). There was a weak negative correlation between loneliness and all domains of Social Support, besides Family Functioning.
Introduction
Chronic Kidney Disease (CKD) is recognized as a global health problem, which after its diagnosis affects a series of adaptations in the patient’s life. Complications such as hypertension and diabetes mellitus associate this disease with high rates of morbidity and mortality (Malta et al., 2019).
CKD is defined by the appearance of progressive and irreversible abnormalities in the structure and/or function of the kidneys for more than 3 months, with implications for health (Kidney Disease Improving Global Outcomes [KDIGO], 2013). Thus, the diagnosis is made by analyzing the Glomerular Filtration Rate (GFR) in which values lower than 15 L/minute/1.73 m² establish renal functional failure (FFR) and by urine test (change in albumin) (KIS, 2013; Porto et al., 2017).
There are different possibilities of renal replacement therapy (RRT) available in the clinic for CKD, the treatments Conservative, Dialysis which is subdivided into hemodialysis and peritoneal dialysis, and Renal Transplantation.
The Conservative method has a preventive character and aims to avoid complications and worsening of kidney function, through lifestyle changes (KIS, 2013). In Hemodialysis, the treatment is extracorporeal and the toxins in the blood are filtered by a machine, while in Peritoneal Dialysis, the filtration process is internal with the help of a natural filter (peritoneum). In Renal transplantation a renal graft is placed in the patient’s lower abdomen without necessarily requiring the removal of the organ (Rocha et al., 2020; SBN, 2021).
It is emphasized that no treatment is considered a curative measure, thus, concerns with the biopsychosocial scope of the patient should be evaluated to provide him/her with less physical, emotional, financial, and social harm (Fernandes et al., 2017; Rocha et al., 2020).
Hemodialysis is performed three to four times a week, with dedicated time of 3 to 5 hours, in addition to all multidisciplinary monitoring and nutritional adaptation that the patient starts (Santos et al., 2017). The socioeconomic condition is a complication of the patient that puts him in a stressful situation, so the provision of treatment and medications for CKD requires greater funding and better management of services at the hospital level, so that there are no disparities in access to treatment (Crews et al., 2019).
A recent study developed by O’Hare et al. (2018), describes the emotional, social, and health impact that CKD patients face in making sense of their daily struggle with feelings of abandonment, isolation, and alienation during the hemodialysis period. These feelings directly affect patients’ quality of life and highlight the importance of good social monitoring, the need for good hospital service, and increased attention from the health care team to result in improved health conditions.
Finally, possible negative outcomes that can be prevented are highlighted in studies, as also presented in the study of Shi et al. (2020), in which it was confirmed that good social interaction and minimal loneliness are associated with positive emotions, while less social support and greater loneliness are associated with insufficient self-care and reduced social interaction. Thus, studying the impact of loneliness and associated factors on the lives of hemodialysis patients becomes essential for the non-development and non-mortality of CKD.
The webs of social relationships including the closest relationships (family and friends) and those more formal (work) refer to the individual’s social support, important for the patient’s sense of independence and autonomy in cognitive functions, which drive well-being and health (de Brito & Pavarini, 2012; Silva et al., 2016).
Loneliness is defined as “a subjective feeling of dissatisfaction with social relationships” (Gale et al., 2018). The assessment of loneliness is beyond the objective aspects of physical health, it incorporates subjective aspects of the individual’s perception, and its symptoms can lead to a mental decline and be linked to depressive conditions, consumption of illicit substances and also, of suicide attempts (Carmona et al., 2014).
Loneliness and social isolation differ in the criteria of “having little contact and involvement in social activities and living alone”—social isolation refers directly to the absence of regular contact with family/friends and lack of involvement in social organizations (Schrempft et al., 2019). Both concepts are factors in high mortality rates in Chronic non-communicable diseases (NCDs) (Gale et al., 2018).
Another negative outcome that is quite relevant and prevalent in this group is depressive symptoms, which according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), involves disturbances in emotional, cognitive, behavioral, and somatic regulation, characterized by mood swings, feelings of sadness, loss of interest or pleasure, low self-esteem, etc.
In the context of patients with CKD, depression is associated with the recognition of the severity of the disease given by the diagnosis, the stress of continuous treatment and its consequences brought, the effect of medications, the new limits on diet, and the decline in the functional capacity of the individual (Costa et al., 2016; Tsutsumimoto et al., 2018).
Given the above, the present study aims to verify the level of loneliness and its relationship with socioeconomic and health conditions, social support, family functionality, and depressive symptoms in patients on hemodialysis treatment.
Methods
This cross-sectional study involved analysis of secondary data collect in 2019 among 80 patients who were recieving hemodialysis. In the renal replacement therapy service of the study, a total population was 180 patients, where 150 of whom met research eligibility criteria, thus the invitation was carried out and accepted with n = 80 participants. The study in question aimed to assess social frailty and its relationship with physical frailty in CKD patients on hemodialysis.
In this current study, the population consists of patients aged 18 years and older, with a diagnosis of CKD on hemodialysis, with the inclusion criterion defined by the medical diagnosis of Chronic Kidney Disease, being on hemodialysis treatment. The exclusion criterion was to present dementia verified in medical records, being under 18 years of age and not having a diagnosis of CKD.
There was a first contact with the patients for explanation and invitation to participate in the research and to those who agreed to participate in data collection signed the Free and Informed Consent Form, besides the opinion of the Research Ethics was respected. In the hemodialysis sessions, assessments were started through the instruments Sociodemographic, Economic, and Health Condition Characterization, UCLA Loneliness Scale (version 3), Medical Outcomes Study (MOS) Social Support Scale, Patient Health Questionnaire-9 (PHQ-9), and the Family APGAR.
The Sociodemographic, Economic, and Health Condition Characterization Instrument evaluates the Sociodemographic and Economic Characterization by gender, age, education, marital status, income, and housing; the Health Condition covers associated morbidities, treatment time, vascular access, medication use, and functional capacity.
The UCLA - Loneliness Scale was developed by Russel in 1996 and validated in Brazil with Brazilian elderly by Kuznier and collaborators, in 2016. This scale assesses subjective feelings of loneliness, and this study adopted its most recent version (version 3). It consists of 20 items (nine positively written and 11 negatively formulated) and its score can range from 20 to 80 points and the higher the score, the greater the degree of loneliness. The author of the scale assigned the score of 50 to 59 with a moderately high level of loneliness and 60 or more as indicative of high levels of loneliness. The author of the scale assigned the score from 50 to 59 with a moderately high level of loneliness and 60 or more as indicative of high levels of loneliness.
In the Medical Outcomes Study (MOS) Social Support Scale, the objective is to evaluate social support, it was developed by Shernoure and Stewart in 1991 and validated in Brazil in 2001 by Andrade. It consists of 19 items that are subdivided into five dimensions of social support, which are: material (four questions—provision of practical resources and material help); affective (three questions—physical demonstrations of love and affection); emotional (four questions—expressions of positive affection, understanding and feelings of trust); information (four questions—availability of people to get advice or guidance) and positive social interaction (four questions—availability of people to have fun or relax). For each item there are five response options that must be indicated by the person as the most appropriate, they are: never, rarely, sometimes, almost always and always (Andrade, 2001 ). The score of this instrument is obtained by scores for each domain ranging from 20 to 100 points, where the closer to 100, the higher the level of social support. In each dimension, the scores corresponding to the assigned answer are added: never (1), rarely (2), sometimes (3), almost always (4), and always (5). For the Affective Social Support dimension only, the score obtained must be divided by 15 and then multiplied by 100 (Sherbourne & Stewart, 1991 ).
The Patient Health Questionnaire-9 (PHQ-9) was validated by Kroenke, Spitzer, and Williams in 2001 and adapted in Brazil by Santos et al. in 2013. It is an instrument with nine questions based on the clinical diagnostic criteria for depressive episodes, DSM-IV, which corresponds to the evaluation module for depressive disorders of the Patient Health Questionnaire (PHQ). The symptoms evaluated are: depressed mood, anhedonia (loss of interest or pleasure in doing things), problems with sleep, tiredness or lack of energy, change in appetite or weight, feeling of guilt or worthlessness, problems with concentration, feeling if slow or restless and suicidal thoughts. The frequency of each symptom in the last 2 weeks is evaluated on a Likert scale from 0 to 3 corresponding to the answers “no day,” “less than a week,” “more than a week,” and “almost every day,” respectively. The questionnaire also includes a tenth question that assesses the interference of these symptoms in the performance of daily activities, such as working and studying. The final score scores are 5 for mild depression, 10 for moderate, 15 for moderately severe, and 20 or more for severe.
Finally, the Family APGAR was used, that verifies the existence of family dysfunction by assessing satisfaction with the dynamics of family functioning. It was created by Smilkstein in 1978 and adapted to Portuguese by Duarte in 2001. The instrument consists of five questions with four response options, which are never (0 points), rarely (1 point), sometimes (2 points), almost always (3 points), and always (4 points). The total score scores are 1 to 8 points (high family dysfunction), 9 to 12 points (moderate family dysfunction), and 13 to 20 points (good family functioning).
The database was coded and organized in a database with double entry and comparison of values, using the program Microsoft Excel® version 2013 program. The statistical treatment of data was carried out with the support of SPSS software, version 22.0. Descriptive analyses were performed, with the preparation of tables, including central tendency data (mean, minimum, and maximum) and dispersion measures (standard deviation). The distribution of the data was checked using the Kolmogorov-Smirnov Test, and parametric and/or non-parametric tests were adopted.
To verify the relationship between the continuous variables the Spearman (non-parametric) or Pearson (parametric) correlation coefficients were calculated. In this study, the magnitude of the correlations was classified according to Levin and Fox (2004) : weak (<.3); moderate (.3–.59); strong (0–6 to .9), and perfect (1.0).
Other statistical analysis may be performed as indicated by the statistical professional.
Results
Eighty patients participated in the study. Table 1 shows that the average age of the participants was 59.63 (±15.14) Years, the average education level was 6.66 (±3.91) years, and the average per capita income did not exceed one minimum wage (±666.45) in reais. The mean time on hemodialysis was equal to 4.53 (±5.69) years and the number of daily ingested medications was equal to 6.34 (±5.14)—Table 1.
Descriptive Statistics of Continuous Variables of Sociodemographic, Economic, and Health Condition Characterization. São Carlos, SP, Brazil. 2019 (n = 80).
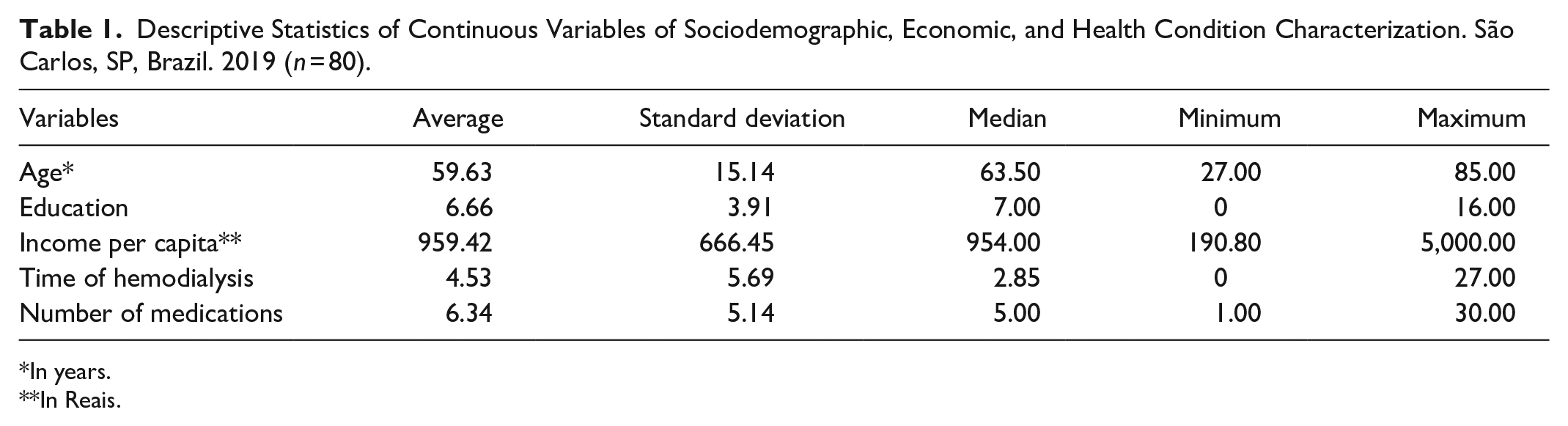
In years.
In Reais.
Table 2 shows the predominance of the females gender (55%), white ethnicity (65%), with a fixed partner (65%), and retired (71.3%). The prevalent religion was Catholic (62.5%), with the majority practicing (67.5%). Of the interviewees (n = 30; 37.5%) reported having diabetes, (n = 45; 56.3%) are hypertensive, and (n = 8; 10%) have other diseases associated with CKD. In addition, the most prevalent health status was regular (n = 80; 52.5%).
Distribution of the Percentage of Categorical Variables of Sociodemographic, Economic, and Health Condition Characteristics. São Carlos, SP, Brazil. 2019 (n = 80).
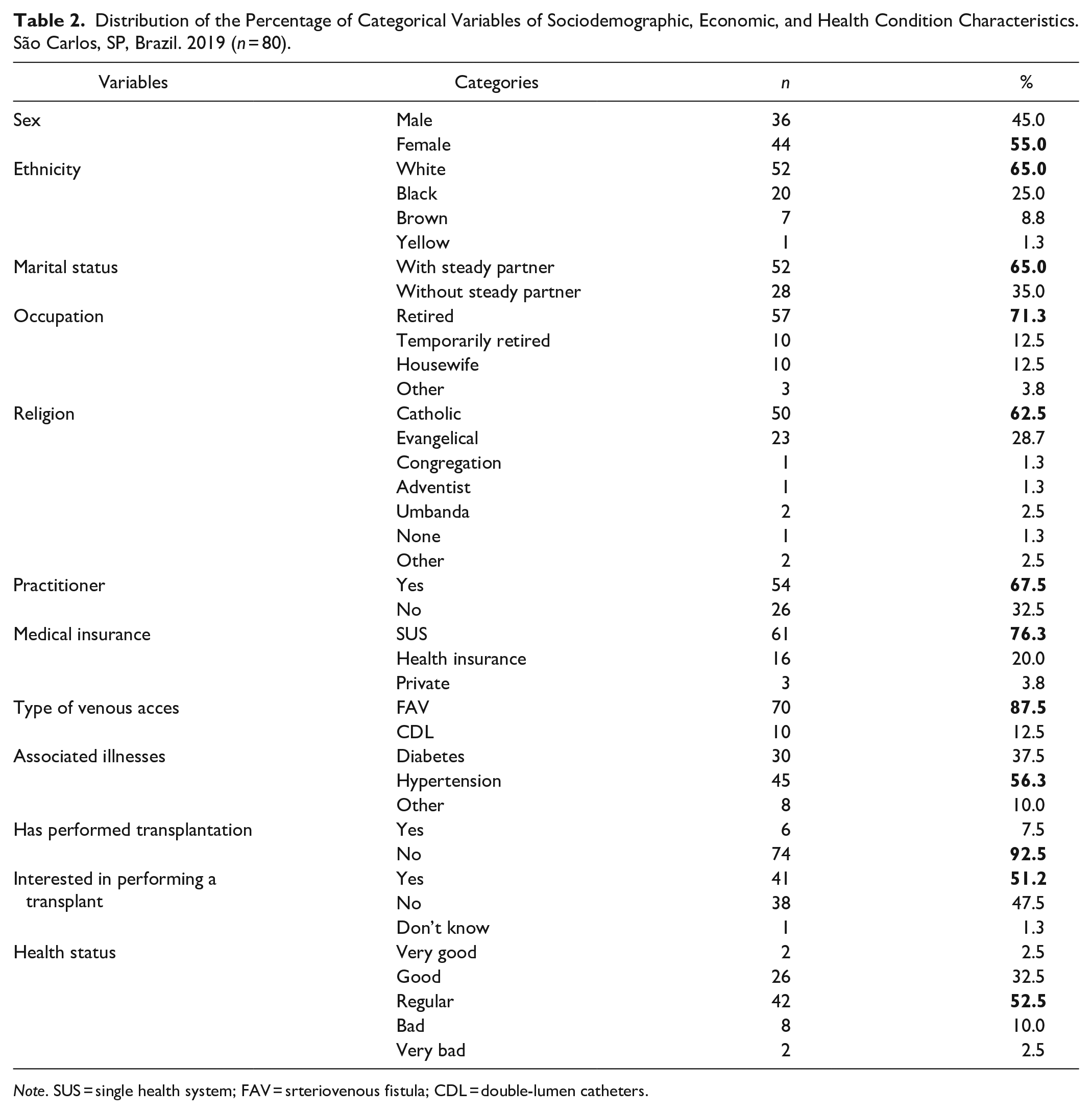
Note. SUS = single health system; FAV = srteriovenous fistula; CDL = double-lumen catheters.
For the levels of loneliness, there was a predominance of respondents with moderate level of loneliness (n = 44; 55%), with low level of loneliness there (n = 19; 23.8%) and high level of loneliness (n = 17; 21.3%). Depression, evaluated by means of the PHQ-9 instrument, showed 83.7% with depressive symptoms, according to the final score of the instrument, in which they were classified into four levels (mild, moderate, moderately severe, and severe). In the evaluation of Family Functionality, carried out by the APGAR Family instrument, it was identified that most participants have good family functionality (n = 55; 68.8%). Social Support was evaluated through the MOS Social Support Scale, with the worst result in the Positive Social Interaction domain (average of 74.31). However, the averages found in Material Support, Affective Support, Emotional Support, and Information Support, were relatively high—Table 3.
Percentage of the Levels of Loneliness Assessed by the UCLA Instrument, Percentage of the Levels of Depression Assessed by the PHQ-9 Instrument and Percentage of Family Functioning by the APGAR Instrument and Distribution of the Percentage of Social Support Assessed by the MOS Instrument. São Carlos, SP, Brazil. 2019 (n = 80).
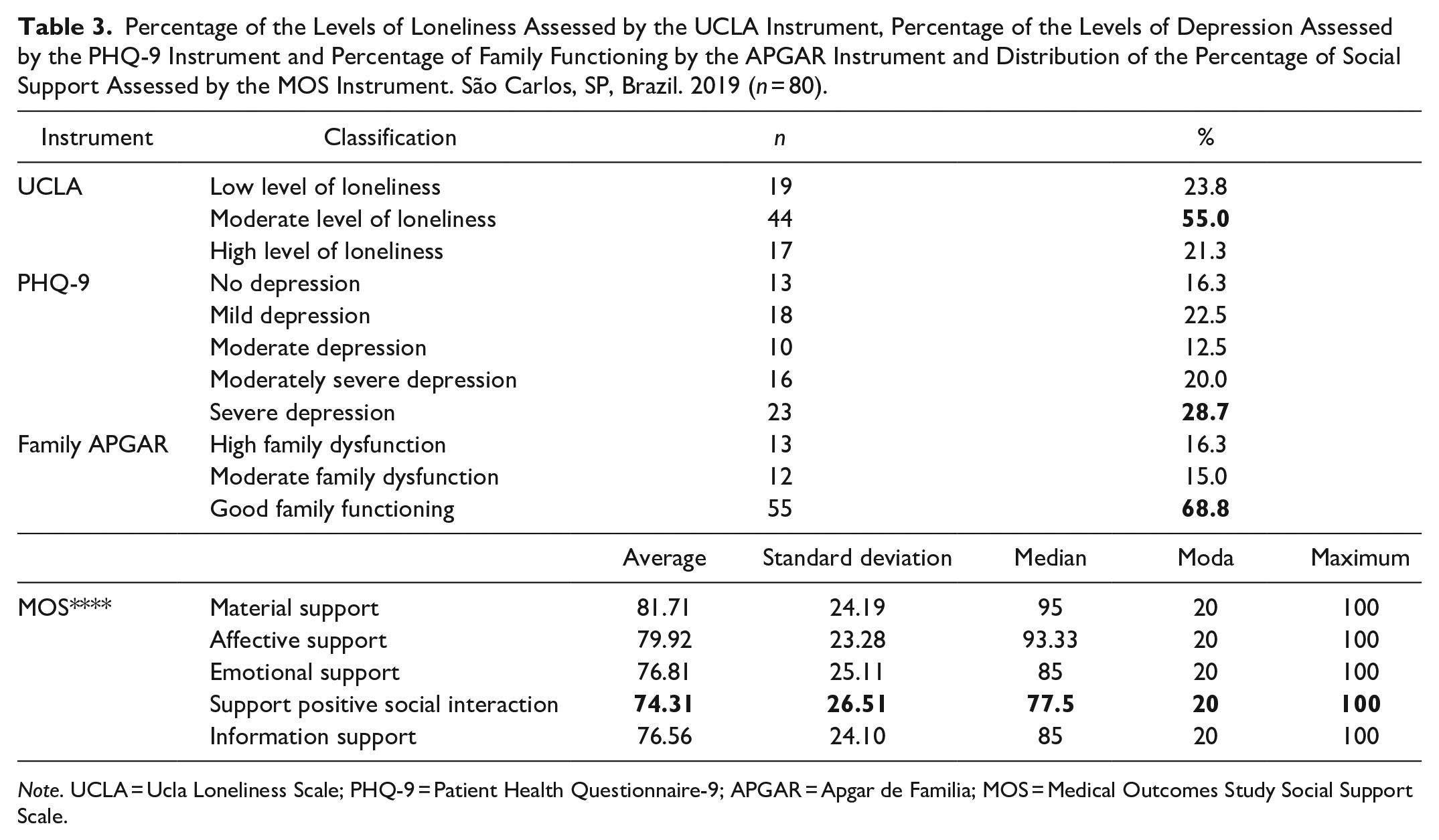
Note. UCLA = Ucla Loneliness Scale; PHQ-9 = Patient Health Questionnaire-9; APGAR = Apgar de Familia; MOS = Medical Outcomes Study Social Support Scale.
Loneliness, assessed through the UCLA instrument, there was statistical significance with the variables depression (PHQ-9), Material Support (MSA), Emotional Support (ESA), and Positive Social Interaction Support (PSA)—Table 4.
Spearman’s Correlation of UCLA and PHQ-9 with APM, APA, APE, APISP, API, and APGAR. São Carlos, SP, Brazil. 2019 (n = 80).
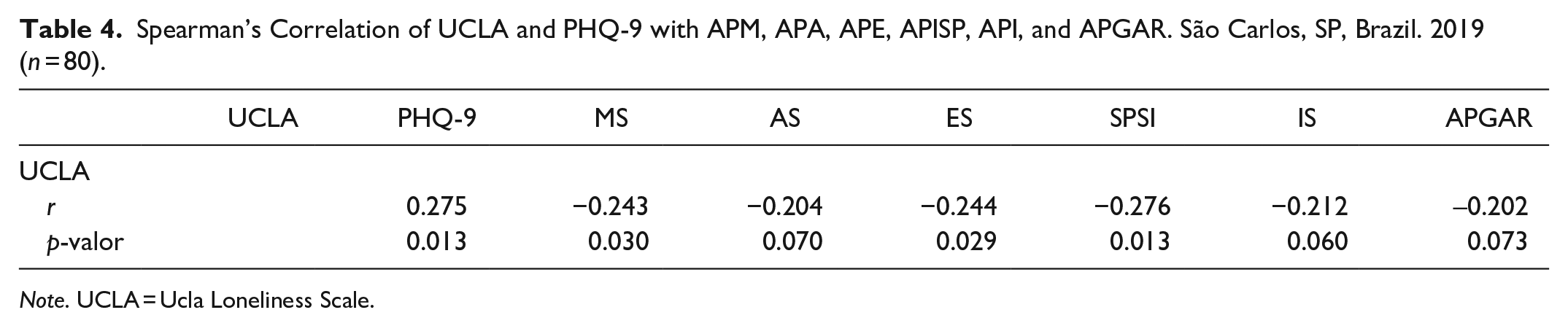
Note. UCLA = Ucla Loneliness Scale.
Discussion
In this research, patients with chronic kidney disease were interviewed, and the prevalent age was 59.63 years, consistent with other studies (Andrade et al., 2021; Costa et al., 2016). The female gender represented 55% of the participants and in other studies conducted previously also presented the same group with the highest rate (Barbosa et al., 2019; Nogueira et al., 2018).
As for financial condition, the minimum wage was the most affected with an average of 959.42 reais, thus exemplifying the specificity of this group of patients with CKD. Besides all the necessary adaptation from the beginning of treatment, they face barriers related to the high cost of treatment, which is justified by the transportation of at least 3 days a week, restriction in the work and study load, the early withdrawal from the labor market and access to daily medications that are of high cost (Harambat & Ekulu, 2016; Pretto, Winkelmann et al., 2020). In this same study an average of 6.34 units of numbers of medications purchased daily was presented. Both statistical data corroborate with other previously conducted studies (Ferreira, 2015; Sgnaolin & Figueiredo, 2012).
It was found an average of 4.53 years of hemodialysis time of these patients, also presented the same average in the literature (Gesualdo et al., 2020; Nogueira et al., 2018). There are data related to 100% of patients with some associated disease, in which 56.3% have Arterial Hypertension and 37.5% with Diabetes and the other 10% with other related diseases, these two results in relation to the treatment time and the associated disease respectively, reinforce the possibilities of the patient having a negative outcome in CKD (Costa et al., 2016; Palmierl et al., 2017).
In the data concerning the instruments, it was noted the predominance of patients with moderate level of loneliness (55%), with 23.8% of patients with low level of loneliness, followed by 21.3% of patients with high level of loneliness. This number is consistent with all the theory addressed in this study, characterizing CKD also as a social problem due to its necessary adaptation in the autonomy of basic activities of daily living and by social withdrawal after the beginning of treatment (O’Hare et al., 2018; Shi et al., 2020).
The webs of social relationships of the patient are significant, representing the direct social support of the individual with CKD, being fundamental to their sense of independence and autonomy in addition to psychological well-being. Reinforced in other studies, the family, along with the team of professionals in the nephrology service can favor with better acceptance of the same in relation to their new needs and treatment (Maia et al., 2016; Nogueira et al., 2018).
In the evaluation of social support, Applied by the MOS Social Support Ladder, it showed positive averages with 81.71% in the domain Material Support, 79.92% Affective Support, 76.81% Emotional Support and 76.56%, with the worst result in the domain Positive Social Interaction, with an average of 74.31%. In this same axis, there were positive results regarding Family Functioning, in which most participants presented Good Family Functioning (n = 55; 68.8%). Of this group, 16.3% had High Family Dysfunction and 15% had Moderate Family Dysfunction. According to this and others in the current literature, these two data (social support and family dysfunction) reflect the positive support of their families and are also justified by the majority of participants (65%) having a steady partner collaborating in the activities of daily living and in issues of physical dependence of the same (Silva et al., 2017 ).
Regarding depression, the PHQ-9 instrument showed that among the 80 participants, 83.7% presented depressive symptoms. In the classification of the levels of this illness, 12.5% had moderate depression, 16.3% had no depression, 20% had moderately severe depression, and 28.7% had severe depression. Percentage consonant with studies, in which more recent data demonstrate comprehensive prevalences of depressive symptoms in patients on hemodialysis treatment, whose rates are between 40% and 100% depressive (Pretto, Rosa et al., 2020). The fact that patients resize all their habits and customs makes for a biopsychosocial adaptation used to find new relationships and affairs. The haunts of hemodialysis treatment develop from the discovery of the disease, to the recognition of its severity, thus strengthening this possible negative outcome—depression (Coutinho & Costa, 2015; Pretto, Winkelmann et al., 2020).
It is expected that this study will help health professionals in the prevention and management of diseases, identifying the most prevalent problems in these populations at an early stage, allowing the planning of actions that improve the quality of life throughout the treatment and reduce the incidence of negative outcomes such as loneliness and depression.
Conclusion
The treatment of CKD requires such an adjustment of the patient to his new eating, social and physical habits, thus exposing him in a stressful situation that can negatively influence his quality of life. The scarce number of accessible Nephrology Services hinders the patient’s mental, physical and psychological well-being, since sociodemographic and clinical conditions are of high relevance for accepting and coping with the continuous and irreversible hemodialysis treatment.
It is concluded, therefore, that CKD patients had a significant level of loneliness. In addition, participants with higher level of loneliness had more depressive symptoms, family dysfunction, and reduced social support.
This present study has as a limitation the selection of the sample by convenience, with n = 80 patients with CKD. Future longitudinal studies with larger samples and investigation in the area of the level of loneliness and its associated factors are necessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Council for Scientific and Technologica (CNPQ).
Headquarters Institution
Federal University of São Carlos, Center for Biological Sciences, Department of Gerontology. San Carlos—San Paulo.