
Abstract
Jordanians are more at risk for heart failure now than in years prior. However, there are few studies addressing heart failure self-care in Jordanians. Identifying predictors that promote heart failure self-care among Jordanian patients is crucial in providing comprehensive care. This study aimed to identify predictors of self-care behaviors among Jordanians with heart failure. A cross-sectional study with a convenience sample of 300 Jordanian patients was performed in an educational hospital in the north of Jordan. Differences in the level of self-care between selected sociodemographic and clinical variables were identified using univariate statistics, and multiple regression was used to adjust estimates for covariates. The predictors of self-care were insomnia (p ≤ .001) and marital status (p = .018). Identifying factors influencing self-care can assist with addressing the causes of insomnia to ensure effective treatment, providing patients with social support, and eventually promoting heart failure self-care.
Introduction
Heart failure (HF) is “a clinical syndrome with symptoms and or signs caused by a structural and/or functional cardiac abnormality and corroborated by elevated natriuretic peptide levels and or objective evidence of pulmonary or systemic congestion” (Bozkurt et al., 2021, p. 387). It is a complex clinical syndrome with typical symptoms (e.g., dyspnea, fatigue) that can occur at rest or on effort, and is characterized by objective evidence of an underlying structural abnormality or cardiac dysfunction that impairs the ability of the ventricle to fill with or eject blood (particularly during physical activity) (Inamdar & Inamdar, 2016). Described as a global pandemic, HF affects 26 million people worldwide (Ponikowski et al., 2014). Furthermore, there have been dramatic increases in HF risk factors in both developed and developing countries including coronary artery disease, hypertension, diabetes, smoking, and obesity (Callender et al., 2014; Celermajer et al., 2012; Gaziano et al., 2010; Gong et al., 2018; Page et al., 2014; Teo & Rafiq, 2021; Yusuf et al., 2020). According to the World Health Organization (WHO, 2015) in the prevalence of diabetes in Jordan was 14.9%, hypertension was 19.3%, tobacco smoking was 38.4%, insufficient physical activity was 15.6%, overweight was 65.9%, and obesity was 30.5%. The high prevalence of HF risk factors can be attributed to increasingly sedentary lifestyles, higher levels of stress, and a shift in diet to high fat “fast” foods (Abu-Mweis et al., 2014; Abu-Zaiton & Al-Fawwaz, 2013; Elhneiti & Al-Hussami, 2017; Hammoudeh et al., 2006; Harris et al., 2020; Khader et al., 2019; Lavie et al., 2019; Sharkas et al., 2016).
Improvement in self-care is one of the major aims of HF management programs (Cowie et al., 2014; McGreal et al., 2014). Self-care includes activities performed intentionally by individuals, families and communities to promote health and prevent disease (Harkness et al., 2015). Self-care can reduce health problems, improve healthcare outcomes and quality of life (QOL), and reduce hospital readmissions and lower costs for patients with HF (Bidwell et al., 2015; Jaarsma et al., 2017; Moser et al., 2012; Toukhsati et al., 2019). Boyde et al. (2018) demonstrated that self-care education led to a 30% reduction in unplanned hospital readmissions at 12 months (relative risk [RR] 0.703; 95% confidence interval [CI], 0.55, 0.90).
Self-care can be influenced by several factors. A recent review demonstrated various influencing factors on self-care including clinical characteristics of patients (severity of HF, comorbidity, New York Heart Association [NYHA] functional classification), sociodemographic characteristics (e.g., age, level of education, self-efficacy), environment (e.g., social support, location). For example, a lower educational level correlates with lower self-care, and people with higher educational levels are more likely to understand health-related information, and to read educational material, which ultimately assists with improving knowledge and self-care (González et al., 2014; Tawalbeh et al., 2017). In addition, people with a low level of education have difficulties in comprehending educational content, and this may worsen their health physically and emotionally, increase negative health-related consequences (Wu et al., 2013), and therefore negatively affect self-care (Barbareschi et al., 2011; Zeng et al., 2017).
Despite the importance of engaging in self-care for HF management, few studies targeting factors to influence self-care have been conducted in Middle Eastern countries and none in Jordan (Akbari Kamrani et al., 2018).
Identifying the clinical factors, demographic characteristics, cultural differences (geographical area, religion, beliefs, attitudes, norms, values, and thoughts), and culturally-specific practices that influence self-care can be crucial for developing and tailoring the most appropriate and personalized self-care interventions for patients with HF in Jordan (Koirala et al., 2020; Osokpo & Riegel, 2021). Additionally, performing a comprehensive and thorough assessment for patients over the duration of education programs can facilitate adopting personalized HF interventions that conform to patients’ needs and preferences (Koirala et al., 2020; Osokpo & Riegel, 2021).
Therefore, this study aims to identify these factors in order to tailor suitable interventions and improve HF management in Jordan.
Methods
A cross sectional survey of a convenience sample of patients with HF attending a cardiac clinic in an educational hospital in the north of Jordan was conducted. The inclusion criteria were: patients aged 18 years or older diagnosed with HF by a cardiologist through the NYHA criteria, signs and symptoms of HF, and echocardiograph. The exclusion criterion was inability to complete the survey due to conditions such as severe dementia. Illiterate participants were included if they had a consenting companion who could complete the survey with them.
The minimum sample size needed for this study was calculated by the “rule of thumb,” which implies that at least “ten observations are needed per category of predictor variables”(Austin & Steyerberg, 2015). Twenty predictors (demographic characteristics and clinical factors) were measured in the study, therefore, a minimum of 200 patients were needed to be enrolled. To allow for non-participation and potentially greater precision of estimates, a total of 333 patients were invited to participate. Seven patients refused to participate, three withdrew, and 23 were unavailable. The final total sample was 300 participants, with a response rate of 91%.
The study was approved by the research committee of the hospital, where the study was conducted (H-2017-025). The privacy and confidentiality of participants were protected during the data collection. Participant identifiers such as names and dates of birth were not collected, and the survey was completed anonymously.
Study Instruments
The European Heart Failure Self-Care Behavior Scale was used to assess the level of self-care, identify whether patients are performing recommended self-care behaviors, and evaluate the effectiveness of HF management programs (Jaarsma et al., 2009; Vellone et al., 2014). The scale consists of 9 items relating to self-care behavior in patients affected with HF (Jaarsma et al., 2009). Each item is rated from 1 (I completely agree) to 5 (I completely disagree), with the total score ranging between 9 and 45. A low score indicates better self-care (Vellone et al., 2014). The scale has been used to evaluate the effectiveness of education and other management strategies on patients affected with HF (Sedlar et al., 2017; Vellone et al., 2014) and has been translated into 14 languages, with reliability ranging from 0.77 to 0.95 and Chronbach’s α from .68 to .87 (Lee et al., 2013; Vellone et al., 2014). However, the tool has not previously been used in Arabic, which is Jordan’s official language. Therefore, we adapted the European Heart Failure Self-Care Behavior Scale for use in Jordan through the forward and back translation method (Beaton et al., 2000; Gudmundsson, 2009; Sousa & Rojjanasrirat, 2011). An experienced bilingual nursing academic with a master’s degree and doctorate from the United States first translated the scale from English to Arabic, and a second then independently translated it back to English. Study authors then confirmed the coherence between the original and back-translated English versions. The Arabic version of the tool was piloted on seven HF patients (two females and five males) who met the eligibility criteria for the larger study and regularly visited the cardiac clinic. These patients reported that the items were clear and readable, and the language was simple and understandable and culturally appropriate.
The demographic tool included clinical and demographic variables. The clinical variables were: body mass index (BMI), ejection fraction (EF), insomnia, and New York Heart Association (NYHA) classification. The EF was measured through echocardiography and classified as HF with reduced ejection fraction when LVEF <40%; HF with mid-range EF when LVEF 40%–49%; and HF with preserved ejection fraction when LVEF ≥50 (Ponikowski et al., 2016). The NYHA classification is comprised of four categories from class I to class IV to classify the impact of HF symptoms on patients’ ability to walk or exercise, and the level of limitation occurring when performing any physical activity (Raphael et al., 2007). Translation of the study tools into Arabic was performed by an experienced bilingual nursing academic, followed by back translation into English by another experienced academic, blinded to the original version.
Statistical Analysis
Means and standard deviation (SD) were used to describe the levels of self-care. Continuous sociodemographic characteristics and item analysis was used to measure the corrected item scale correlations and Chronbach’s α. An independent sample t-test and one-way ANOVA tested for differences in the level of self-care between selected sociodemographic and clinical variables. All assumptions of ANOVA and multiple linear regression were examined and met. Levine’s test was used to assess the equality of variances between groups. Stepwise backwards multiple linear regression analysis was used to determine the predictors of self-care. The variables included in the multiple regression were derived from univariate analysis (p ≤ .20). SPSS Version 22 was used to analyse the data.
Results
Sample Characteristics
The mean age of patients was 61.9 ± 12.6 years, two thirds were male (n = 202), most (40.0 %, n = 120) were retired or unemployed (37.3%, n = 113); most were married (79.0 %, n = 237) (Table 1). While 24% were illiterate and 40% of patients had low education, 22% had a bachelor’s degree. Nearly a third required assistance with activities of daily living. The mean monthly income was $495 US.
Sample Characteristics and Clinical Factors; Mean (M), Standard Deviation (SD), and Percentage (%) for 300 Patients With Heart Failure in Jordan.
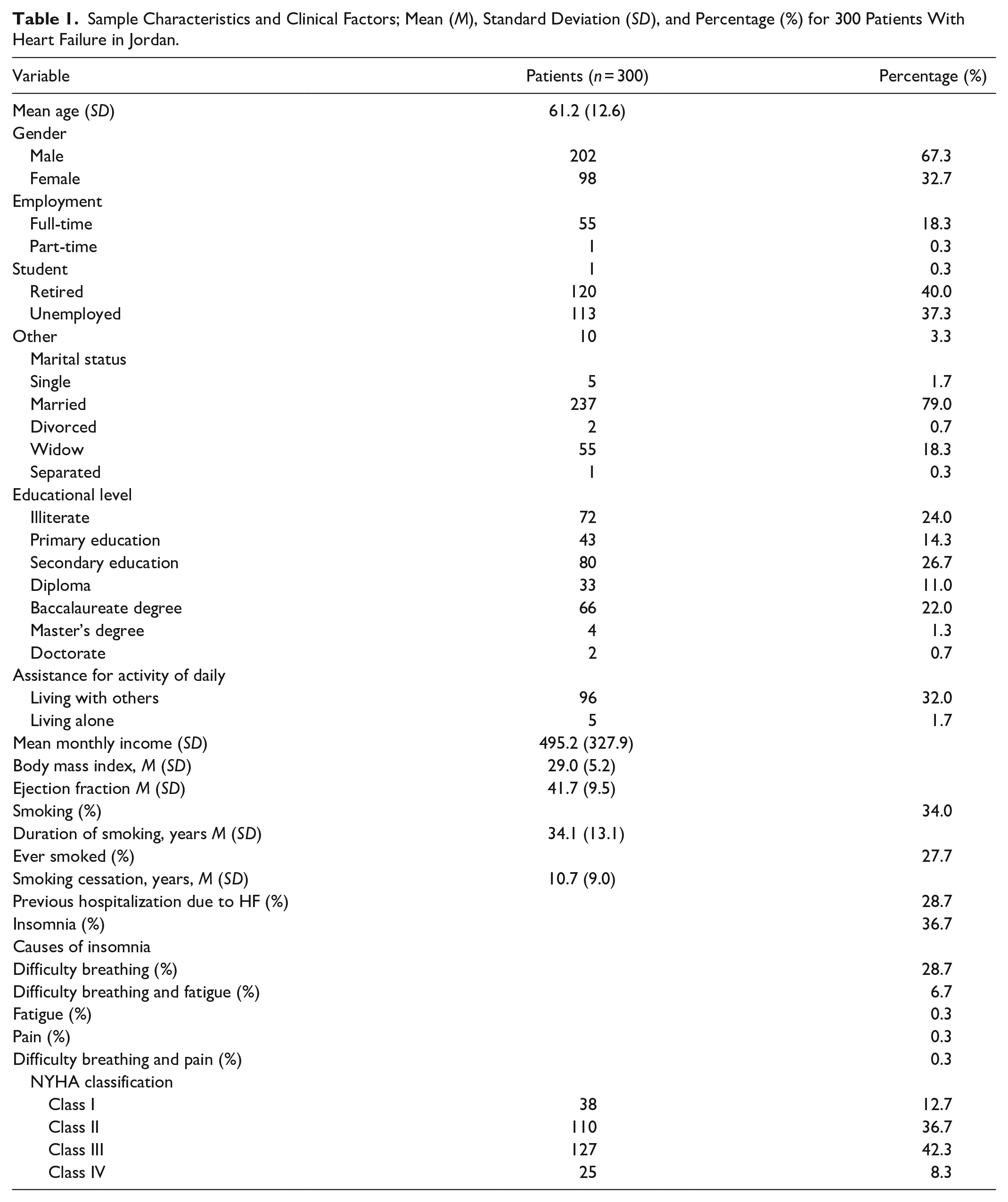
Clinical Factors
The participants’ mean body mass index (BMI) was 29.0 ± 5.2 (Table 1). The mean ejection fraction was 41.7% ± 9.5. Slightly more than quarter (34%, n = 102) of the patients were current smokers, with a mean smoking duration of 34.1 ± 13.1 years. A third of patients complained of insomnia (n = 110), the major cause of which was difficulty breathing (28.7%). The majority had been classified in NYHA class II (36.7%) or III (42.3%).
Participant’s demonstrated a moderate level of self-care (27.5 ± 4.7). The aspects of self-care with highest levels of agreement were: contacting their doctor or nurse if their shortness of breath increases (73% agreement) and if their feet/legs become swollen (62% agreement), and taking their medication as prescribed (92.4% agreement) (Figure 1). Aspects with lowest agreement were: contacting their doctor or nurse if they gain 2 kilos in 1 week (1.7 % agreement), monitoring weight every day (4 % agreement), and performing exercise regularly (14 % agreement) (Figure 1).
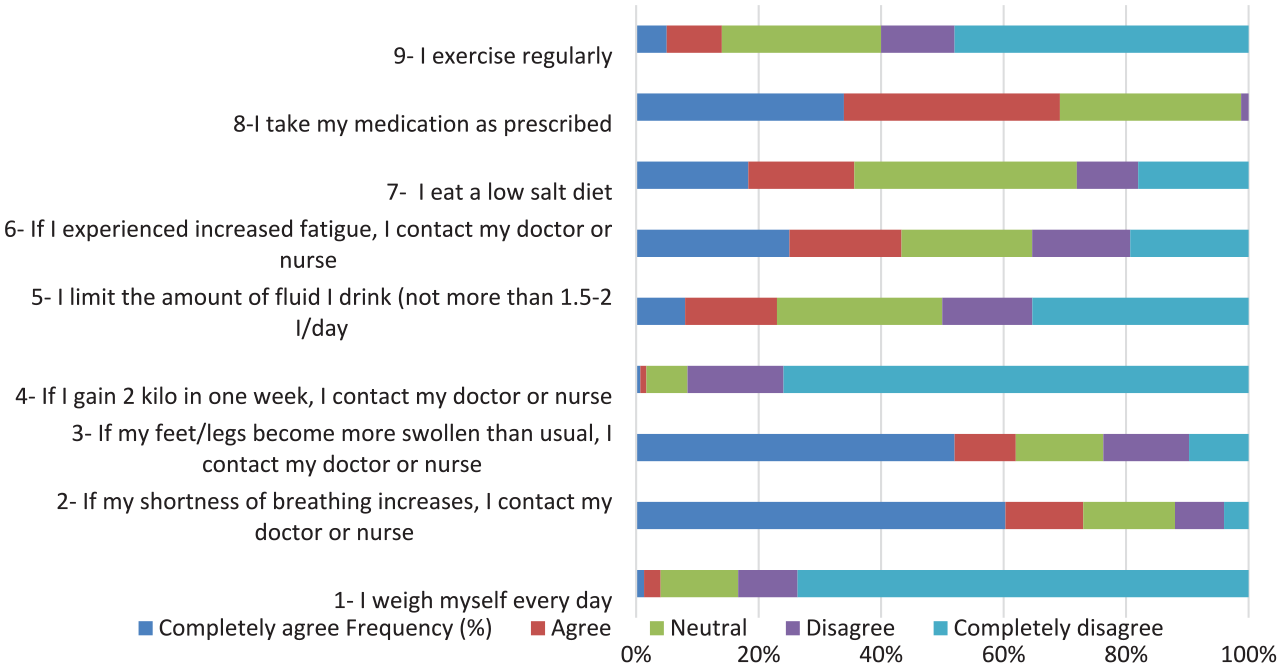
The percentage of agreement with nine statements about self-care behaviors.
Item Analysis
Chronbach’s α for self-care was .55 and the item-total correlation ranged from −.05 for item 5 to .55 for item 3. Three items demonstrated acceptable item-total correlations ≥ .4 (items 2, 3, and 6). Possible reasons for low Chronbach’s α were investigated by comparing item analysis between different demographic variables. This demonstrated a large difference in Chronbach’s α between patients who had previously been admitted for heart failure (α = .68) and those who had not (α = .49) (Table 2). Chronbach’s α improved most in both groups if item 5 (“I limit the amount of fluid I drink [not more than 1.5–2 L/day]”) was deleted.
Item Analysis for the Self-Care Scale Presented for Previously Admitted Patients (n = 86) and Non-Admitted Patients (n = 214).
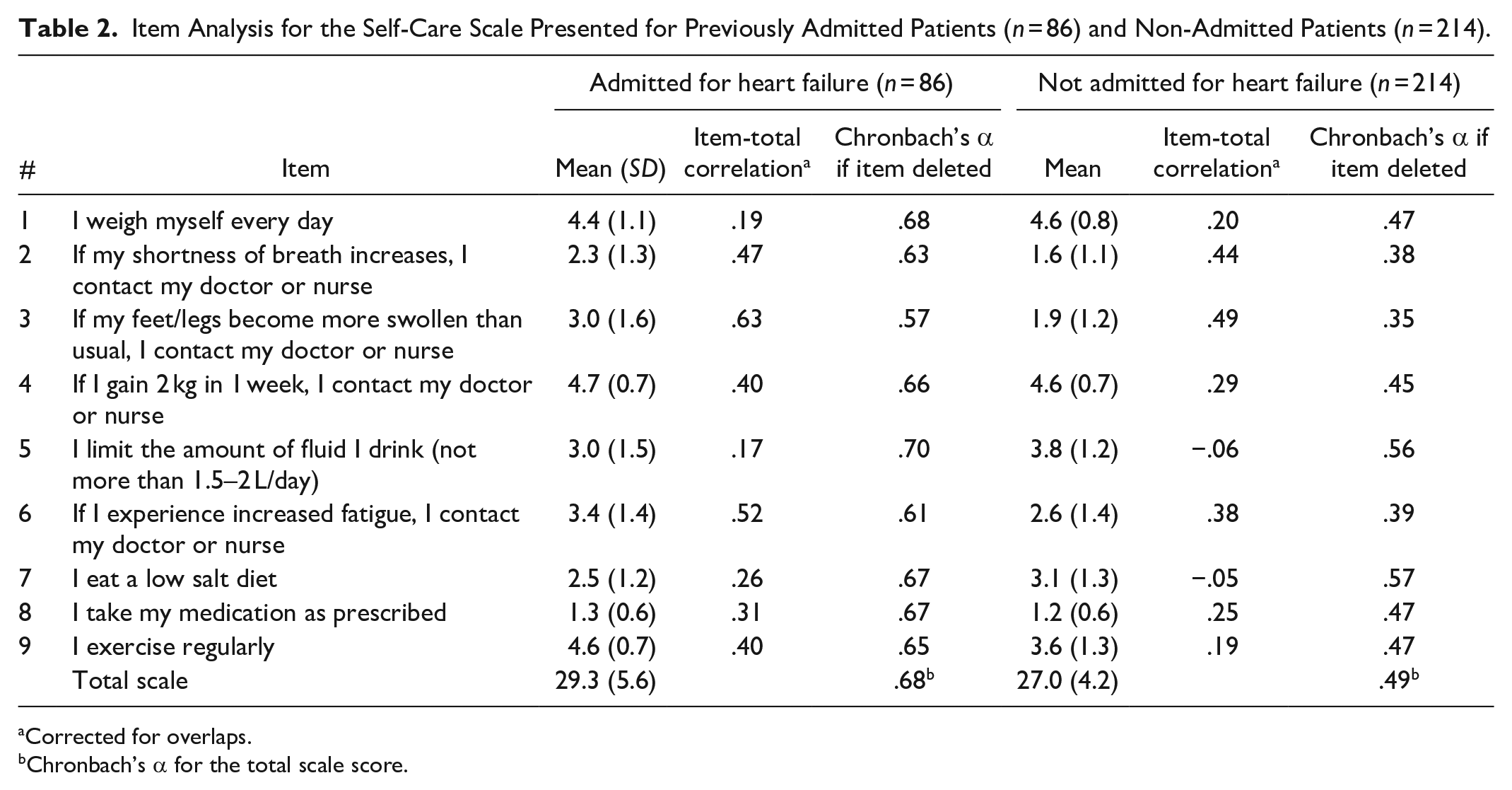
Corrected for overlaps.
Chronbach’s α for the total scale score.
Sociodemographic and clinical factors
Independent t-tests were used to test for differences in the level of self-care between sociodemographic and clinical factors (Table 3). Groups with higher self care scores were: males, married, employed, no previous hospitalization, and non-insomniacs. Self care scores tended to increase with education level and from higher to lower NYHF classification levels (Table 3).
Comparison of Self-care (Mean, SD) by Selected Sociodemographic (Gender, Marital Status, Occupation, Previous Hospitalization) and Clinical (insomnia, Hypertension (HTN), Diabetes Mellitus (DM), angina) Factors Among Patients With HF in Jordan (n = 300).
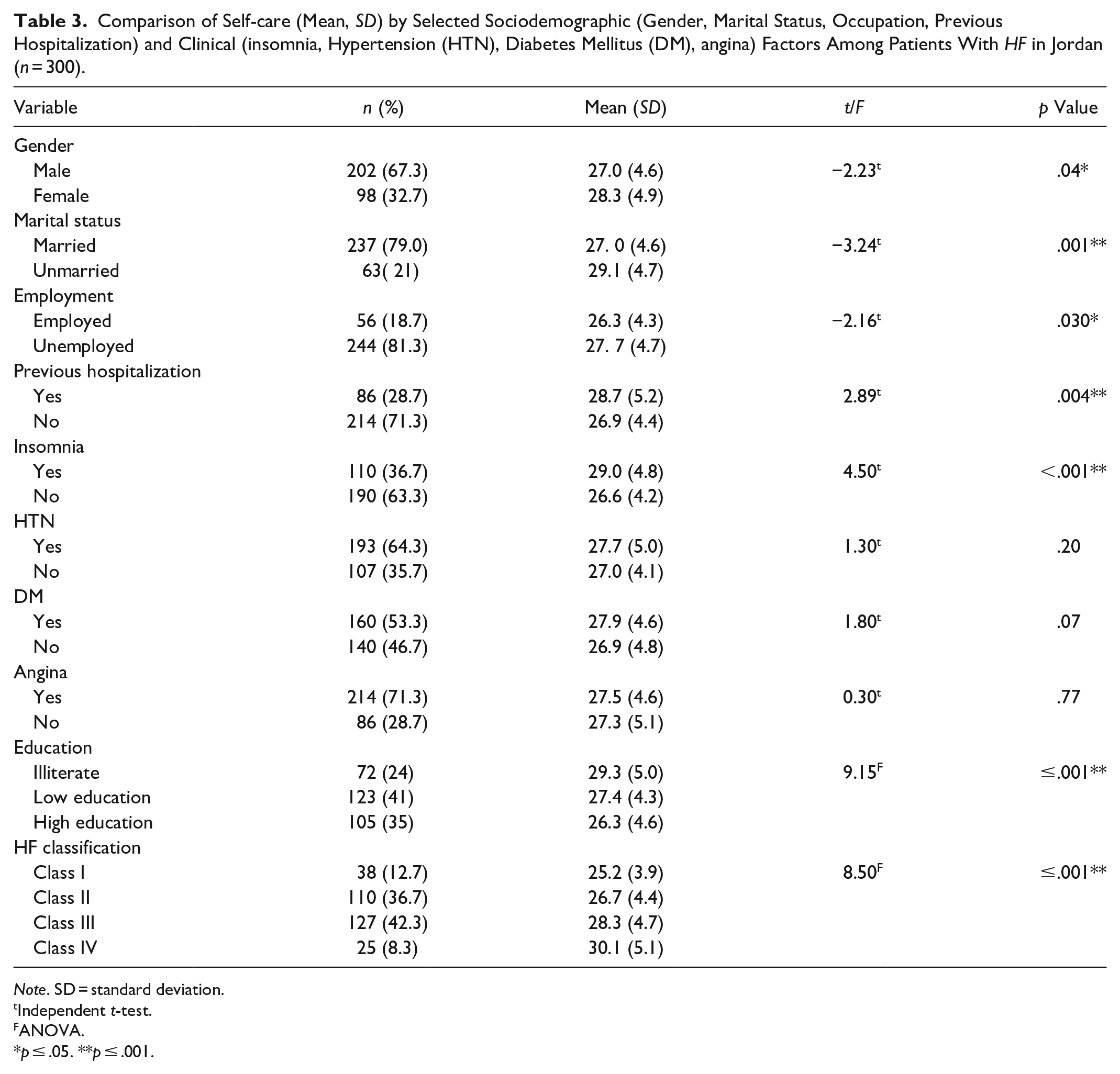
Note. SD = standard deviation.
Independent t-test.
ANOVA.
p ≤ .05. **p ≤ .001.
Predictors of self-care among patients with HF in Jordan
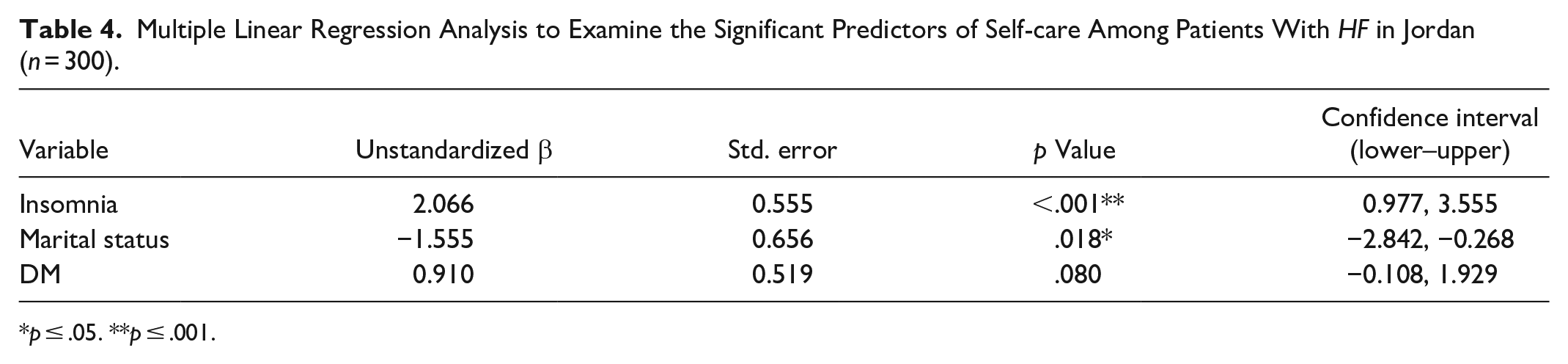
A multiple linear regression tested if previously identified variables (insomnia, marital status, HF classification, level of education, and DM) predicted the level of HF self-care. The assumptions of regression analysis were examined and met. Insomnia (p ≤ .001) and marital status (p = .018) were significant predictors of HF self-care (Table 4). The self-care score for patients with insomnia was 2.1 points higher than patients without insomnia, indicating inadequate self-care (Table 4). Unmarried patients scored 1.6 points lower than married patients, indicating better more adequate self-care. Diabetes was not a significant predictor of self-care (p = .08) (Table 4).
Multiple Linear Regression Analysis to Examine the Significant Predictors of Self-care Among Patients With HF in Jordan (n = 300).
p ≤ .05. **p ≤ .001.
Discussion
The study showed a moderate level of self-care (27.5 ± 4.7, possible range 9–45) for Jordanians with HF. This study finding is supported by three studies conducted in Middle Eastern countries (two in Lebanon and one in Jordan). The first study from Lebanon, to identify determinants of self-care in 100 patients with HF, found suboptimal self-care in Lebanese patients with HF (Massouh et al., 2020). The second Lebanese study reported that cardiac patients were not sufficiently aware of the meaning and concept of self-care although they carry out some self-care behaviors (Dumit et al., 2015). Another cross-sectional descriptive-correlational study of 226 Jordanian patients with HF showed that self-care was suboptimal, and the mean scores of self-care were less than the level of clinical target (≥70) for the Self-care of Heart Failure Index (Tawalbeh et al., 2017). The breakdown of responses for each item in the self-care tool showed suboptimal levels of some HF self-care behaviors such as contacting doctor or nurse if patients gain 2 kilos in 1 week and monitoring weight every day. The suboptimal levels of these aspects in Jordan can be linked to the lack of clear and structured HF management programs in Jordan, and inadequate educational/management strategies provided by health care providers (High Health Council, 2017; WHO, 2015) . Additionally, some factors influencing self-care such as low self-confidence, poor social support, and poor HF knowledge may explain the suboptimal levels of self-care (Massouh et al., 2020).
The results of the present study extends existing knowledge of demographic and clinical factors that impact on HF selfcare to a Jordanian context. Two key factors emerged. First, patients without insomnia had higher self-care than insomniac patients. This result is in line with numerous studies (Dickson et al., 2007; Riegel & Weaver, 2009) which showed that sleep disturbance is a leading factor for cognitive impairment, which negatively affects patients’ capability to self-care. In turn, poor self-care may result in impaired QOL, limited functional capacity and increased burden of symptoms (Riegel & Weaver, 2009). Furthermore, poor sleep has been found to be associated with anxiety, depression, impaired motor skills, social discomfort, lack of concentration, worsening functional performance and fatigue, which ultimately lead to poor self-care, adherence to a healthy lifestyle and QOL (Altevogt & Colten, 2006; Redeker et al., 2010; Riegel, Ratcliffe et al., 2012; Tsuchihashi-Makaya & Matsuoka, 2016). This indicates the importance of identifying and treating the cause of insomnia through utilizing the most appropriate and tailored interventions. Several interventions can be used to improve insomnia in patients with HF. These include taking diuretics as prescribed to reduce orthopnea, cognitive behavioral therapy (breathing exercises, mindfulness meditation, sleep consolidation, identifying maladaptive beliefs relating to sleep), limiting bed activities (sex, phone, laptop, TV), regulating sleep patterns, going to bed when patient feels sleepy, avoiding sleep during the day, cutting down caffeinated drinks, performing tolerable exercise during the day, and ensuring that patient’s room is quiet, dark, and a comfortable temperature (Edwards, 2020). Additionally, educating patients to perform exercise, quit smoking, and follow low fluid and salt diet can help improve patients sleeping (Edwards, 2020; National Library of Medicine, 2020). Therefore, an effective strategy to treat insomnia and improve self-care can be to address the causes of insomnia, managing mental and psychological HF-related symptoms, and establishing effective collaboration between healthcare providers (Tsuchihashi-Makaya & Matsuoka, 2016).
Marriage was the second key factor impacting of HF self-care, with higher self-care levels reported for married patients.This finding can be supported by social causation theories (Quinones et al., 2014) and other studies (Kitko et al., 2020; Koirala et al., 2020; Tawalbeh et al., 2017) which show that married people are more likely to receive social support, psychological spousal support, and care from their partners which can lead to better self-care and clinical outcomes. A study reported that social support from a spouse has been associated with lower hospital readmissions and healthcare costs (Dunbar et al., 2008). Other studies from the United States and Netherlands, found that unmarried patients are at higher risk of depression, lower QOL, and poorer self-care (Havranek et al., 2004; Luttik et al., 2006). The result indicates patients’ need for additional social, emotional, and physical support in order to improve their self-care and adherence to healthy HF recommendations. Social support can also be provided by other family members and/or friends who may significantly assist patients with HF by reinforcing the information provided, and improving self-care (Cowie et al., 2014). The health promotion model postulates that adequate social support, reflected by the presence of family members and friends, is a vital source of interpersonal influence that increases health-promoting behavior and ultimately improves patients’ self-care and QOL (Pender et al., 2006). A finding of systematic review of 45 qualitative studies targeting HF self-care (Strachan et al., 2014) emphasizes the health promotion model assumption, which indicated that social support provided by family members or friends was one of the main contextual factors that promote self-care.
In addition, many HF self-care behaviors and management activities are complicated and may be notoriously difficult for patients to perform autonomously, particularly in patients with cognitive impairments, functional limitations, and depression (Kitko et al., 2020; Riegel et al., 2011). This highlights the potential provision of social support in the home environment to unmarried patients, and/or the important caregiving role that friends and family members can play in assisting patients’ HF self-care activities and handle complex tasks requiring both coordination and skills (Dionne-Odom et al., 2017; Kitko et al., 2020). The caregivers can aid: (1) monitoring and recognizing any changes in HF symptoms, (2) following the recommended heart diet, (3) performing physical exercise, (4) taking prescribed medication, (5) performing daily activities (driving, going to hospital, participating in social events), and (6) providing emotional and social support) (Heart Failure Society of America, 2016). Family or friends can provide emotional/social support for patient through: (1) talking with them about their treatment plan, (2) avoiding critical criticism if the patient doesn’t adhere to treatment regimen, (3) allowing them to express their opinions, (4) encouraging them make their decisions regarding their lifestyle behaviors and treatment plan, and (5) recognizing and acknowledging their feelings (Heart Failure Society of America, 2016).
Additionally, patients can be supported by others to monitor their HF symptoms through: (1) informing them about any changes in symptoms that they may notice such as ankle swelling and increased breath shortness, and then encouraging them to go to the hospital; (2) reminding patients to self-weigh every day and document their daily weight; and (3) observing if the patient uses many pillows to reduce shortness of breath. Importantly, family members or friends should ask patients about what type of support/assistance they need, because each patient has different needs, preferences, capacities, and goals (Heart Failure Society of America, 2016). In addition to social and emotional support, family can help in teaching and empowering patients in performing health-related behaviors such as stress management, nutrition, and exercise (Khachian et al., 2016). Therefore, healthcare providers can develop effective management programs through involving patient’s family in the patients’ care plan (Khachian et al., 2016).
Culturally, family relations of Arabs are considered the most powerful social institution of the Middle East (Lipson & Meleis, 1983; Massouh et al., 2020). Additionally, family members have close relationships and links in which they may be over-protective of their patient and exchange roles of delivering care (Dumit et al., 2015). Therefore, married patients in Jordan are highly expected to receive social support. However, the influence of this cultural expectation on self-care has not yet been investigated in Jordan.
The Chronbach’s α for self-care in Jordanian HF patients was low (.55) compared to other studies. The causes of low Chronbach’s α here are unclear. In addition to simply indicating poor item inter-relatedness, a low α could indicate violation of the “tau equivalent model” that assumes that each test item in a tool measures the same latent trait on the same scale (Tavakol & Dennick, 2011). In this instance, factor analysis could be used to identify that there are actually multiple factors or traits being measured by the tool, whereas previous studies have reported unidimensionality (Tavakol & Dennick, 2011). Alternatively, our finding of Chronbach’s α differing for patients based on a previous HF hospitalization, suggests that greater uniformity of responses may be anticipated following the intense education and training in self care that may be permitted during a hospitalization.
The study has a number of limitations. First, data were collected in one healthcare setting using a convenience sample, which limits the representativeness of the study sample, generalizability of the results to other patients living in different settings and external validity of the results. Second, components of HF self-care including self-care maintenance and self-care management and their determinants were not addressed in this study. Lastly, the other factors that can influence HF self-care such as depression, impaired cognition, and age were not investigated in this study.
Implications for Practice
Identifying factors influencing self-care is necessary to promote HF management. The influence of marital status withdraws attention of health care providers toward the importance of providing patients with social support and involving family members in their care process. Identifying patients experiencing insomnia can enable healthcare providers to employ interventions and approaches to improve insomnia and minimize patients suffering. The results of this study could be used as a foundation for conducting education programs for patients to improve their HF self-care and to target factors that can potentially improve self-care, such as reducing insomnia and increasing social support in unmarried patients.
Conclusion
The study demonstrated moderate self-care level in Jordan. The insufficient knowledge of the factors influencing self-care increases the difficulty of identifying patents at risk for not performing appropriate self-care behaviors, and consequently leads to ineffective HF management. Married patients had better self-care than unmarried. Patients with insomnia had poorer self-care than those without insomnia. These findings indicate that identifying factors influencing self-care such as insomnia and marital status can assist healthcare providers to develop more health management interventions aiming at reducing patients’ insomnia and providing social support. The study findings also highlight the importance of performing comprehensive assessment of patients including socio-demographic and clinical characteristics, prior to starting treatment. This can help in tailoring the most appropriate, suitable, and needed health interventions for patients which can eventually improve patients’ health outcomes. The study results also highlight the importance of implementing patient-centered approach to produce better patient outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.