
Abstract
The purpose of this study was to evaluate the psychometric properties of the Brazilian Scale for the Assessment of Self-Care Behaviors with Arteriovenous Fistula in Hemodialysis. Cross-sectional validation study, followed the recommendation provided by Sousa and Rojjanasrirat. Content validity, explanatory and confirmatory factor analyses used to check validity and Cronbach’s alpha was the reliability measure. Three hundred hemodialysis patients with arteriovenous fistula were included in the study. The expert committee assessed the content validity. Exploratory factor analysis confirmed the same two-factor structure found for the original scale, explaining 60.10% of the variance. Such solution was checked by confirmatory factor analysis with Cronbach’s alpha equal to 0.920, 0.810, and 0.884 for the overall scale, the self-care in management of signs and symptoms and the self-care in prevention of complications subscales respectively. The scale has good psychometric properties to assess self-care behaviors and can be used with Brazilian patients on hemodialysis with arteriovenous fistula.
Introduction
End-stage renal disease (ESRD) is a public health problem in several regions of the world, most often associated with the United States of America and Europe (Clementi et al., 2020). However, evidence shows that this disease is increasing in developing countries, especially in India, Mexico, Asian countries, Chile, and Brazil, among others (Neves et al., 2020).
The overall prevalence for patients with ESRD in Brazil was 640 pmp in 2018. In the last decade, prevalence increased 58%, with an average growth of 6.4% per year. The number of dialysis patients was 133,464 in 2018, an increase of 42,546 new patients (Neves et al., 2020). Dialysis patients need a vascular access to undergo hemodialysis and the arteriovenous fistula (AVF) is considered the best one when compared to other access types (grafts or central venous catheter).
AVF dysfunction is one of the most important causes of morbidity and mortality in hemodialysis (HD) patients and can account for up to a third of hospitalizations, representing an important part of such patients’ health costs (Kukita et al., 2015;Ibeas et al., 2017; Lok et al., 2020).
Dialysis units must be able to develop and implement vascular access monitoring programs which includes enabling patients to carry out self-care behaviors with that access in order to prevent and identify complications (Sousa, 2012; Sousa et al., 2017). Evidence suggests that effective programs in the development of self-care behaviors with AVF are important to improve hemodialysis patients’ quality of life and clinical results (Pessoa et al., 2020) (Sousa et al., 2020a). Furthermore, valid and reliable measures are required to assess such self-care behaviors and clinical evolution and to enable research on this issue.
Background
The European Association of Dialysis Transplant Nurses emphasizes that the nephrology nurse must promote both the adaptation of the patient and his/her family to ESRD and self-care capacity development, in order to enhance independence and well-being (Woodcock, 1999). Self-care is the practice by the patient of activities that enable him/her to maintain his/her health and welfare (Orem, 2001). Literature shows that patients with ESRD need to develop a number of self-care behaviors, namely concerning: factors that can worsen kidney disease; diet; fluids (Sagawa et al., 2001; Tsay, 2003); medication (Pagels et al., 2008); dialysis techniques (self-care HD and HD at home or peritoneal dialysis) (Meers et al., 1996; Honkanen et al., 2002; Moran, 2007; Pagels et al., 2008); or vascular access (Sousa et al., 2014, 2017, 2020a, 2020b).
Several vascular access guidelines recommend nurses to teach patients on how to take care of their own AVF (NKF-K/DOQI, 2006; Kukita et al., 2015; Ibeas et al., 2017; Lok et al., 2020) which provides them with the knowledge and skills required to carry out their own self-care. In this context, self-care with AVF must be considered “as the behaviors intentionally performed by the person to maintain health and well-being, which aim to promote the patency of the AVF” (Sousa et al., 2015). Self-care behaviors with AVF concern the prevention of complications and the management of signs and symptoms of such complications (Ozen et al., 2017; Teixeira et al., 2017; Sousa, 2012, 2020b). Several studies have found a large number of patients with very low frequencies of self-care behaviors with AVF (Pessoa & Linhares, 2015; Ozen et al., 2017; Sousa et al., 2017; Yang et al., 2019). A Brazilian study found 97.7% of patients with inappropriate attitudes towards AVF care (Pessoa & Linhares, 2015).
The Scale of Assessment of Self-Care Behaviors for Arteriovenous Fistula in Hemodialysis (ASBHD-AVF) was developed in Portugal with the purpose of assessing patients’ self-care behaviors with AVF (Sousa et al., 2015). It comprises two sub-scales named self-care in prevention of complications and self-care in management of signs and symptoms. Its psychometric properties are good and it has been translated and validated in China (Yang et al., 2019) and Turkey (İkiz et al., 2021). The validation process is currently under way in Iran and Taiwan.
The purpose of this paper is to describe the process of ASBHD-AVF translation and validation in Brazil since no scale for self-care assessment was available in the Brazilian Portuguese language.
Methods
Sample, Setting, and Study Design
The sample involved 300 patients on hemodialysis with AVF registered in four dialysis unit in the city of northeast, Brazil. Data were collected between January and June in 2019. The same inclusion criteria as in the original scale were applied, that is, patients over 18 years of age, on HD with AVF for more than 6 months and with no cognitive impairment. Cognitive compromise was assessed by the Mini-Mental State Examination (Bertolucci et al., 1994; Brucki et al., 2003).
The Ethics Committee approved the project. Participants received information about the study and filled out the informed consent.
Instrument: Scale of Assessment of Self-Care Behaviors with Arteriovenous Fistula in Hemodialysis
The Assessment of Self-Care Behaviors with Arteriovenous Fistula in Hemodialysis (ASBHD-AVF) consists of 16 items distributed in two subscales: self-care in prevention of complications (10 items) and self-care in management of signs and symptoms (six items) (Sousa et al., 2015). The scale is self-completed by the patient but may also be filled out by the researcher in the case of patients with visual or osteoarticular problems.
The self-care behaviors in the prevention of complications subscale concerns the prevention of infections and those behaviors that can cause thrombosis in the access. The other subscale comprises self-care behaviors related to the management of symptoms and signs of vascular access complications.
Each item is scored according to a 5-point Likert scale ranging from 1 (Never carry out the self-care) to 5 (Always carry out the self-care). The final score is found by adding all the item scores, with a minimum of 16 and a maximum of 80. Next, the ratio between the final score and the maximum is found and such percentage is the patient’s frequency of self-care behaviors with AVF. Therefore, a higher percentage (closer to 100) reflects a higher frequency.
Cross-cultural Adaptation of the Scale of Assessment of Self-Care Behaviors with Arteriovenous Fistula in Hemodialysis
The ASBHD-AVF author allowed the translation and cultural validation in the Brazilian Portuguese language. The steps described by Sousa and Rojjanasrirat (2011) were followed in the translation and validation process. The procedures applied for cross-cultural validation were translation, comparison, back-translation, back-translation comparison, pilot test, and validity and reliability testing. The scale was translated into Brazilian Portuguese by two independent translators. A third independent translator compared both versions and proposed a first version, which was next back-translated into Portuguese by two other translators. Then, a multidisciplinary committee compared and analyzed the back-translation and proposed a new version, semantic and conceptually equivalent to the original scale, which was submitted for approval by the scale author in order to ensure instrument objectivity. The ASBHD-AVF Brazilian Portuguese version was tested on a sample of Brazilian patients with ESRD on HD (30 patients). A committee of experts analyzed the pilot test and proposed the Brazilian pre-final version of the scale or ASBHD-AVF-BR, which was applied to patients with ESRD on HD for validity and reliability testing.
Statistical Analysis
Face and content validity
To ensure face and content validity, we set up a committee of 11 experts (nephrology nurses, nephrologists, researchers, and methodological researchers) with experience on patients with ESRD on HD and/or experience on research and methodological research.
Construct reliability and validity
Exploratory factor analysis (EFA) was used to check whether the 16 items of the Brazilian ASBHD-AVF adapted to the Brazilian population had the same meaning as the Portuguese version. Bartlett’s test of sphericity (5% significance level) and the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy (acceptable if KMO > 0.6) were used. The EFA was run with extraction by principal component analysis and varimax rotation with Kaiser normalization. Two factors were extracted according to the ASBHD-AVF theoretical model (Sousa et al., 2015), discarding factor loadings less than 0.3.
In order to assess the two-factor construct reliability, validity and goodness-of-fit, a confirmatory factor analysis (CFA) was run. Reliability analysis involved two checks: test-retest reliability run on the same patients with a one-month interval and given by the intraclass correlation coefficient and by the Pearson correlation coefficient; internal consistency, measured by coefficients such as Cronbach’s alpha, composite reliability, Guttman split-half reliability coefficient and Spearman-Brown coefficient. Goodness-of-fit was given by the coefficients
Results
Sociodemographic, Clinical and Self-care Descriptive Measures
Sociodemographic descriptive measures of the 300 patients with ESRD on HD with AVF are displayed in Table 1. Most patients are male (63.7%), retired (77.3%) and married (56.7%). The mean (SD) age is 55.3 (15.4) years, the main ESRD etiology is arterial hypertension (39.3%) and the mean (SD) AVF duration is 47.1 (47.5) months. Information on care with the AVF was mostly provided by the nurse (58%).
Sociodemographic, Clinical and Self-Care Descriptive Measures (n = 300).
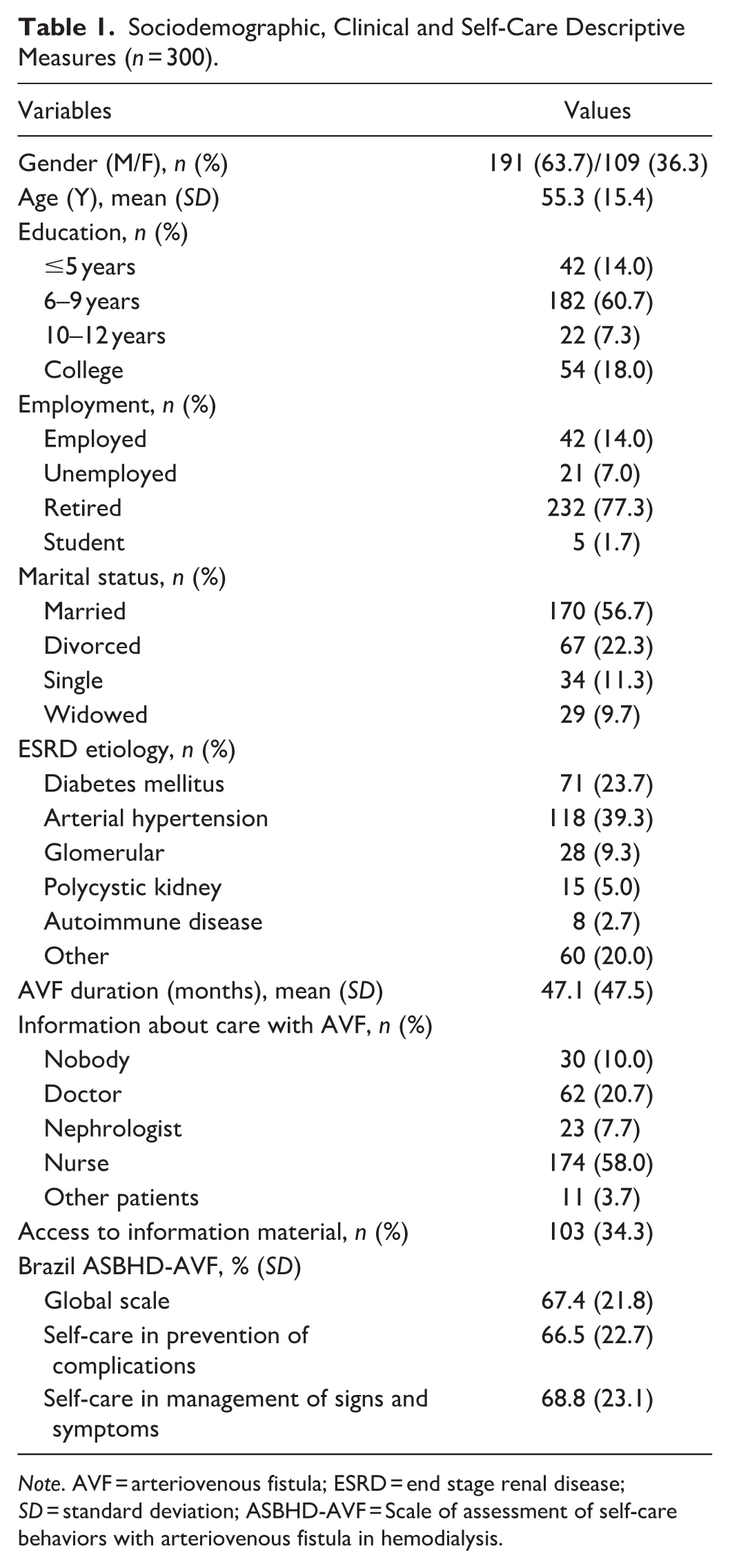
Note. AVF = arteriovenous fistula; ESRD = end stage renal disease; SD = standard deviation; ASBHD-AVF = Scale of assessment of self-care behaviors with arteriovenous fistula in hemodialysis.
Brazil ASBHD-AVF average (SD) percentage scores were: global scale, 67.4% (21.8); self-care in prevention of complications, 66.5% (22.7); and self-care in management of signs and symptoms, 68.8% (23.1).
Face and Content Validity
The multidisciplinary committee analyzed the ASBHD-AVF Brazil after back-translation and suggested grammatical changes in a few items. The scale was applied to some patients who suggested changes to a few words for better item clarification. The expert panel analyzed the scale and suggested one grammatical change. The ASBHD-AVF showed an appropriate face and content validity for the assessment of self-care behaviors with AVF in Brazil.
Construct Validity
Exploratory factor analysis
The KMO measure was 0.848 and Bartlett’s test was significant (
Factor Analysis of the ASBHD-AVF Scale—Brazilian Version.
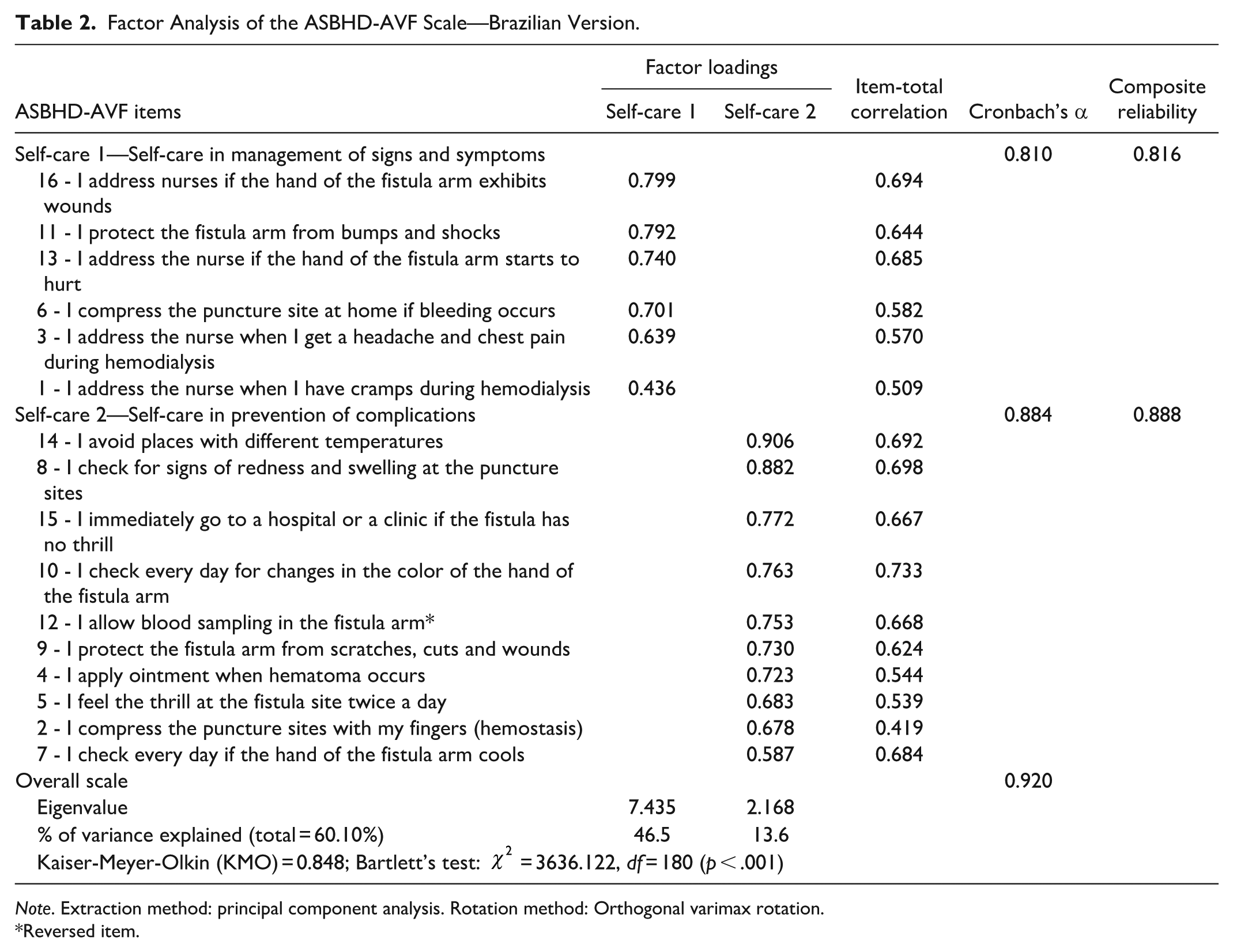
Note. Extraction method: principal component analysis. Rotation method: Orthogonal varimax rotation.
Reversed item.
Confirmatory factor analysis
Forty patients were retested a month later. The item correlation coefficients and the intraclass correlation coefficients are in the range 0.530 to 0.914 and 0.424 to 0.897, respectively. The correlation coefficient for the overall scale and for the two subscales is 0.928, 0.865, and 0.930, respectively; the intraclass correlation coefficient is 0.809, 0.797, and 0.811, respectively.
The scale’s internal consistency was assessed by Cronbach’s alpha with 0.920, 0.810, and 0.884 for the overall scale, the self-care in management of signs and symptoms and the self-care in prevention of complications subscales respectively (≥0.7 and ≥0.8 is considered as acceptable and good respectively). Furthermore, the subscales’ composite reliability is 0.816 and 0.888, respectively (≥0.7 is considered acceptable). Such large values show good consistency and reliability.
The goodness-of-fit is acceptable, since
The Figure 1 displays the path diagram with the items’ standardized regression weights whose squares are all at least 0.25 (square ≥0.25 is good) with a single exception (which is near that value). Thus, all but one item shows good reliability and both subscales have a good factorial validity.
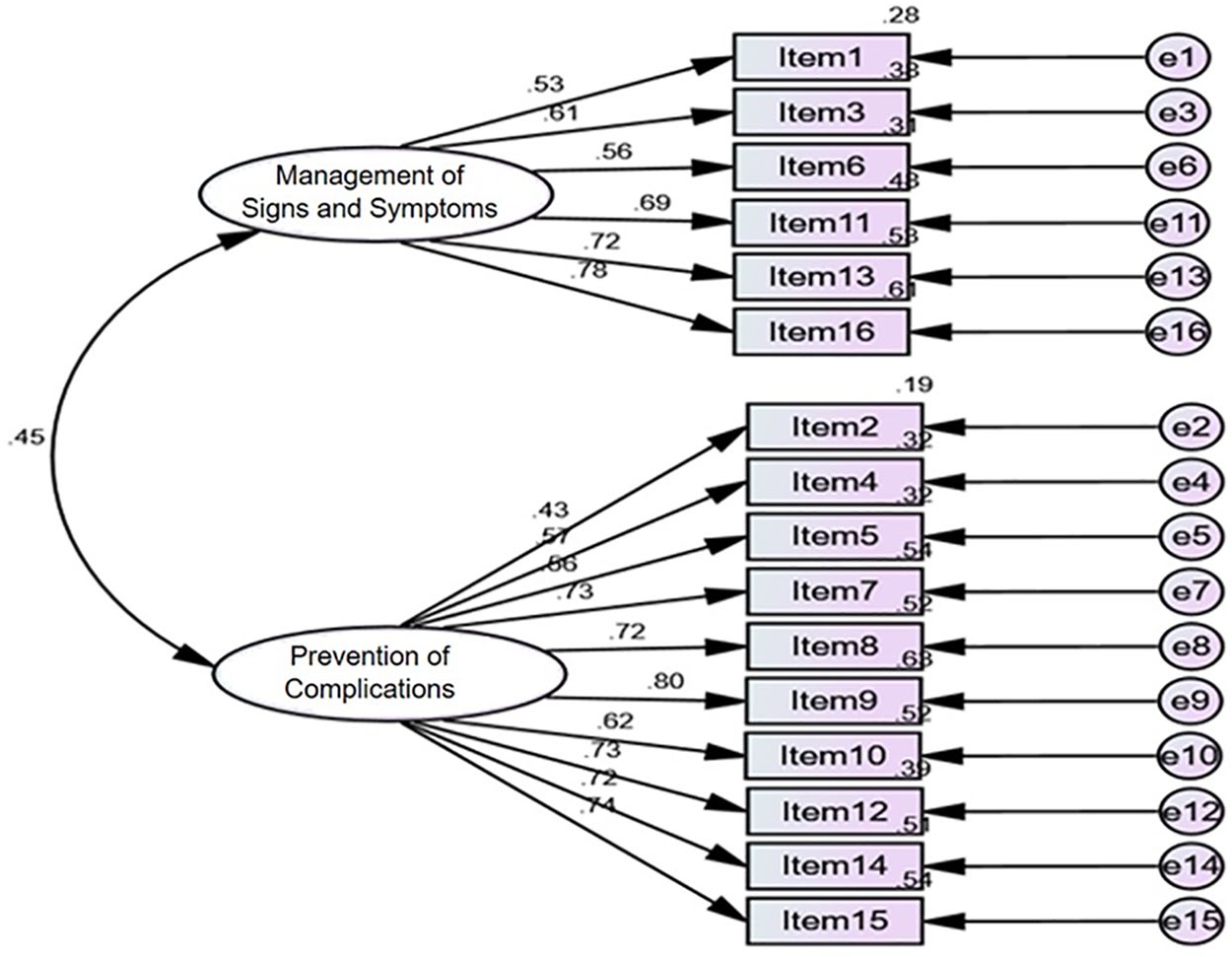
Path diagram with standardized estimates.
Discussion
The ASBHD-AVF scale showed good psychometric characteristics for the Brazilian population.
The translators selected for content validation had experience and knowledge on health and scale validation with the purpose of simplifying item translation. The multidisciplinary committee made grammatical suggestions and changes in a few item words, for example, the word “vibration” was changed to “emotion,” “swelling” to “edema” and “shock” to “injuries” in items 5, 8, and 11, respectively. After analyzing the pilot test applied to patients, a new expert committee proposed three changes: to add the term “vibration” in parentheses after the term “thrill” in items 5 and 15 and to replace the term “edema” with “swelling” in item 8.
Construct validation was based on an exploratory factor analysis. A two-factor solution was found explaining 60.1% of the total variance, larger than the original scale with 39.12% (Sousa et al., 2015), the Chinese version with 53.52% (Yang et al., 2019) and the Turkish version with 59.01% (İkiz et al., 2021).
The ASBHD-AVF Brazilian version exhibited the same structure as the original scale (Sousa et al., 2015) concerning the number of subscales (two subscales), the total number of items (16) and the item allocation to factors. Factor loadings were better than in the original scale in subscale 2, ranging from 0.587 to 0.906 and from 0.369 to 0.700, respectively (Sousa et al., 2015), but were lower in subscale 1 (0.436–0.799 and 0.511–0.805, respectively). Scale validation in Turkey kept the same number of items as the original and the Brazilian versions (İkiz et al., 2021), but only twelve items were retained in the validation process in China (Yang et al., 2019).
Confirmatory factor analysis corroborated the number of subscales and the relationships among items and factors (factor loadings) of the original scale. Cronbach’s alpha of the Brazilian version is very high for the overall scale (α = 0.920) and high for both the self-care in management of signs and symptoms subscale (α = 0.810) and the self-care in prevention of complications subscale (α = 0.884). Such values are better than for the original scale whose alpha is 0.797, 0.797, and 0.722, respectively (Sousa et al., 2015), and similar to the Turkish and Chinese versions concerning the overall scale (0.910 and 0.865, respectively) (İkiz et al., 2021; Yang et al., 2019). The former version’s alpha is also close to the Brazilian one for both subscales (0.84 and 0.85, respectively) (İkiz et al., 2021).
Concerning goodness-of-fit, the CFI was 0.852, a nearly acceptable fit. On the contrary, the GFI and the AGFI are both 0.99, a very large value. The RMR and the RMSEA are 0.081 and 0.07, respectively, an acceptable fit.
Item reliability, given by the squares of the standardized regression weights, is good for every item, with a single exception. Therefore, both subscales have factorial validity. Such results support the model used in the construction of the ASBHD-AVF scale and confirm item association with their respective factors. This is the first time the scale is subject to a confirmatory factor analysis.
This study did not assess convergent and divergent validity which is a limitation. Such assessment is recommended for further research.
Implications for the Clinical Practice
The ASBHD-AVF scale was developed to be used in patients with ESRD undergoing hemodialysis, without memory problems. The instrument must be applied 30 to 60 minutes after connecting the patient, and can be completed by the patient or with the help of the nurse.
Conclusion
The ASBHD-AVF’s Brazilian version exhibited good psychometric properties to assess self-care behaviors with AVF in patients of that country. The overall scale, the Self-care in management of signs and symptoms subscale and the Self-care in prevention of complications subscale showed an internal consistency equal to 0.920, 0.810, and 0.884, respectively. This scale is an important step in the identification of self-care behaviors with AVF actually carried out by patients.
Supplemental Material
sj-pdf-1-cnr-10.1177_1054773821989800 – Supplemental material for Scale of Assessment of Self-Care Behaviors with Arteriovenous Fistula in Hemodialysis: A Psychometric Study in Brazil
Supplemental material, sj-pdf-1-cnr-10.1177_1054773821989800 for Scale of Assessment of Self-Care Behaviors with Arteriovenous Fistula in Hemodialysis: A Psychometric Study in Brazil by Marta Nunes Lira, Clemente Neves Sousa, Maria Carolina Medeiros Wanderley, Natália Ramos Costa Pessoa, Kelly Cristiane Rocha Lemos, Carlene Souza Silva Manzini, Andressa Garcia Nicole, Sheila Coelho Ramalho Vasconcelos Morais, Cecília Maria Farias de Queiroz Frazão, Vânia Pinheiro Ramos, Paulo Teles, Olga Maria Pimenta Lopes Ribeiro, Vanessa Filipa Ferreira Dias, Lara Helk de Souza, Rita Cássia Helú Mendonça Ribeiro, Anna Luiza Pereira Magalhães, Silvia Maria de Sá Basílio Lins, Maira Maria Trevisan Pressi, Polyana Bezerra Mendonça Dourado, Millena Freire Delgado, Ana Elza Oliveira Mendonça, Jacielly Andes Araújo Pinheiro and Nurten Ozen in Clinical Nursing Research
Footnotes
Acknowledgements
To the professionals, participants of the expert panel, who contributed to the face and content validation of the instrument. To the patients, who allowed the application of the instrument for further analysis of the results obtained.
Author Contributions
Study design: MNL; CNS; MCMW; NRCP; CSSM; AGN; LHS; AEOM; NO
Data Collection: MNL: MCMW; NRCP; KCRL
Data Analysis: CNS; PT; VFFD; OMPLR; NO
Study supervision: CNS; CSSM; AGN; SCRVM; CMFQF; VPR; RCHMR; ALPM; SMSBL
Manuscript writing: MNL; CNS; PL; CSSM; AGN; LHS; SMSBL
Critical revisions for important intellectual content: MCMW; MRCP; KCRL; SCRVM; CMFQF; VPR; OMPLR; ALPM; AEOM; NO
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.