
Abstract
As the population is aging, strategies for helping older people to maintain and promote good health and well-being are needed. This study aims to assess whether depressive symptomatology and spirituality are associated with subjective well-being in older adults when controlled for sociodemographic variables. Furthermore, the mediating role of spirituality in the association between depressive symptomatology and subjective well-being was examined. A total of 250 participants (mean age 75.91 ± 7.60) in this cross-sectional study completed the Daily Spiritual Experience Scale, the Zung’s Self-rating Depression Scale, and the Personal Wellbeing Index. Multiple linear regression and mediation analyses were used to analyze the data. Subjective well-being was negatively associated with depressive symptoms and positively associated with spiritual experiences. The indirect effect of depressive symptomatology on subjective well-being via spirituality was 28.7%. The enhancement of spirituality seems to represent one of the relevant interventional strategies in prevention and treatment of depressive symptoms and well-being improvement.
Introduction
The world is currently facing a global increase in aging population (World Health Organization, 2011). Older adults usually suffer from a variety of chronic diseases and disability that increase their vulnerability and reduce their social activities, mental health, and reduce their quality of life (QOL), and well-being (Abdi et al., 2019; Ćwirlej-Sozańska et al., 2018; Gobbens, 2018; Gobbens & Remmen, 2019). These changes are also associated with increased costs spent on health and social care (World Health Organisation, 2011). Consequently, global aging implies the need to develop strategies to keep older people active for as long as possible, promote their physical, mental, social and spiritual health, and improve their well-being (Steptoe et al., 2015; World Health Organisation, 2002).
Well-being is a complex term that integrates physical, psychological, and social dimensions of life. At present, research in this area focuses on two main approaches. The first, referred to as a subjective well-being (SWB), is based on hedonistic aspects of life, such as life satisfaction, experiencing happiness, and joy. The second approach, known as eudemonic well-being, emphasizes the importance of personal growth, meaning of life, and self-actualization (Diener et al., 2018; Gurková, 2011; Steptoe et al., 2015) According to Diener et al. (2018) SWB is a multidimensional construct constituted of two dimensions: cognitive and affective. The cognitive component reflects judgments of life satisfaction, for example, with relationships, family, finance, safety, health. The affective component refers to the experience of positive and negative emotions. Based on biological and genetic theory (Cummins & Wooden, 2014; Cummins et al., 2003, 2014; Diener et al., 2018), SWB is maintained by a homeostatic system, therefore it is relatively stable over time and relatively resistant to life changes. However, serious events or critical situations can disrupt the homeostatic system and it consequently results in reduction in SWB. This study is aimed to focus on cognitive SWB.
Optimizing well-being is one of the main goals in all areas of health care, including gerontological care. Previous studies have shown that well-being in the elderly is influenced by selected socio-demographic (Carmel et al., 2017; Enkvist et al., 2012; Freedman et al., 2017) and clinical characteristics, such as overall health status and disability (Carmel et al., 2017; Freedman et al., 2017). Earlier research has also shown that well-being in the elderly may be related to personal resources, such as coping behaviors (Carmel et al., 2017; Kahlbaugh & Huffman, 2017), size of social network and the level of social support (McHugh & Lawlor, 2012; Tian, 2016; Wang, 2016), mental health (Enkvist et al., 2012; Vitorino et al., 2018), and spirituality or religion (Lifshitz et al., 2019; Schuurmans-Stekhoven, 2019; Thauvoye et al., 2018; Villani et al. 2019).
Depression is a frequent mental disorder. Prevalence of depression has been estimated at 4.4% of the world-wide population with a higher incidence in women and an increasing age (World Health Organisation, 2017). Depression is one of main causes of disability worldwide and is a significant factor in the global burden of illness (GBD 2016 Disease and Injury Incidence and Prevalence Collaborators, 2016; World Health Organisation, 2017). Depression is widespread in older adults living in the community and its prevalence increases with comorbidity of chronic diseases, reduced cognitive functions, and in hospitalized and/or institutionalized older adults (Lotfaliany et al., 2018; Sivertsen et al., 2015). According to research studies (GBD 2016 Disease and Injury Incidence and Prevalence Collaborators, 2016; Han et al., 2018; Lotfaliany et al., 2018; Sivertsen et al., 2015; World Health Organisation, 2016), depression has a negative impact on health-related outcomes, quality of life, well-being, and on health care utilization and costs.
As the population is rapidly aging, strategies for helping the elderly to maintain and promote good health and well-being are needed. The need for developing and delivering useful and effective strategies to help elderly people prevent and delay the decline of functional abilities and intrinsic capacities require identification of key factors that may negatively affect health and well-being (World Health Organisation, 2011, 2017), including depression (GBD 2016 Disease and Injury Incidence and Prevalence Collaborators, 2016; Han et al., 2018; Lotfaliany et al., 2018; Sivertsen et al., 2015). The present research and clinical practice should also focus on identification of adequate internal resources which may improve well-being in the elderly population.
Recently, spirituality and religiosity have been identified as important protective factors influencing physical, mental health, and well-being in the elderly (Koenig, 2012; Lucchetti et al., 2011; Zimmer et al., 2016). In health care context, growing interest in this area produced various definitions of spirituality and religion, but experts have still not reached a consensus. In contemporary health care literature, these terms are usually differentiated and are not considered synonymous. Connectedness with the sacred source (God, Higher Power) is a common feature of spirituality and religion. However, religion is described as a more organizational, institutionalized system of beliefs, practices, rituals, and outward expression of individual in relation to the sacred source. Spirituality is seen as more personal, individual human experience (de Jager Meezenbroek et al., 2012; Koenig, 2012; Rakošec et al., 2015; Thauvoye et al., 2018). Spirituality is considered to be the essence of human being, a personal experience and expression of the spirit and spiritual beliefs through the connection with the transcendent which is outside of self (connectedness with the sacred source, the nature, and others) but also within the self (connectedness with self) (Koenig, 2012; Rakošec et al., 2015; Thauvoye et al., 2018). Spiritual experiences can have the character of exceptional, ultimate experience (e.g., numinous experience, mystical experience, ecstasy, conversion) and/or ordinary everyday spiritual experience (e.g. experience of awe, love, hope, faith, trust, grace, gratitude, forgiveness, peace) (Rakošec et al., 2015; Říčan, 2007; Underwood & Teresi, 2002). Spirituality is a phenomenon that is universally experienced by all people, individually evolving and changing in the context of culture, ethnicity, religion, profession, personal experience, and other influences (Koenig, 2012; Rakošec et al., 2015; Thauvoye et al., 2018). Systematic reviews have showed that spirituality can decrease the recovery time and reduce the rate of morbidity and mortality (Koenig, 2012; Lucchetti et al., 2011), alleviate distress and improve coping with chronic diseases including cancer, pain, physical disability, and somatic symptoms (Koenig, 2012; Zimmer et al., 2016). Furthermore, there is strong evidence that spirituality may reduce symptoms of anxiety and depression (Abdi et al., 2019; Braam & Koenig, 2019; Chaar et al., 2018; Elham et al., 2015, You et al., 2009) and improve subjective well-being and quality of life, particularly in the elderly (Aglozo et al., 2019; Chaar et al., 2018; Lawler-Row & Elliott, 2009; Villani et al., 2019). To sum up, the evidence shows a generally positive influence of spirituality and religion on physical and mental health. Nevertheless, some people were found to experience a negative effect of spirituality and religion on their mental health outcomes (Lucchetti et al., 2019). Furthermore, so far, little is known about the interrelationships between depression, spirituality, and subjective well-being in the elderly population. To our knowledge, there are two studies aimed at the associations between depression, spirituality/spiritual self-care practices, and quality of life (Lee & Salman, 2018; White, 2016), though, not at associations with cognitive SWB. Thus, we aimed to assess whether depressive symptoms and spirituality are associated with cognitive subjective well-being (life satisfaction) in elderly people, when controlled for sociodemographic variables. Furthermore, we examined the mediating role of spirituality in the association between depressive symptomatology and cognitive aspect of subjective well-being.
Materials and Methods
Design, Procedures, Sample
The study had a cross-sectional design. Older adults from two hospitals and three residential homes in Slovakia participated in this study between December 2013 and January 2014. Convenience sampling method was used for the selection of study participants. Our sample consisted of older adults who were 65 years of age or older, with no major psychological disorders (e.g., major depression, psychotic disorders, dementia), and were willing to participate.
To estimate the sample size for regression analysis, “an a priori power analysis for linear multiple regression: fixed model, R2 increase” was conducted in GPower 3.1 (Faul et al., 2009). At conventional medium effect size f2 = 0.15, alpha level = 0.05, power = 95%, and six total number of predictors, optimal sample size was estimated not less than minimum 146 respondents. Three hundred questionnaires were distributed personally. The majority of participants completed the questionnaires alone, some were interviewed by trained administrators. The questionnaires were checked upon completion by the administrators to ensure they were fully completed. A total of 38 participants refused to participate in the study at the beginning or during the completion of the questionnaire, 12 were excluded due to more than 10% loss of data. Two hundred fifty participants were included in the study (response rate of 83%).
Measures
All participants completed the set of questionnaires consisting of the Daily Spiritual Experience Scale (DSES), the Zung’s Self-rating Depression Scale (SDS), the Personal Wellbeing Index—Adult (PWI-A), and a sociodemographic questionnaire.
The Daily Spiritual Experience Scale (DSES) was developed by Underwood and Teresi (2002) to measure daily occurrence of ordinary spiritual experiences of connection with the transcendent such as gratitude, awe, compassionate love, sense of connection with transcendent, sense of deep inner peace (e.g. “I feel God’s presence.,” “I feel God’s love for me directly.,” “I find strength in my religion or spirituality.,” “I am spiritually touched by the beauty of creation.”). Many items of this instrument use the term “God.” If respondents are not able to identify their spiritual experience with using the term God, the authors recommend replacing it with another term for a sacred source or divine. Given the fact that spiritual experiences are one of the most important aspects of spirituality, the DSES tool can be successfully used to assess spirituality (Rakošec et al., 2015; Underwood, 2011). The DSES measures only spiritual experiences with positive charge (e.g., love, mercy, desire for divine closeness), does not include experiences with negative charged features (e.g., feelings of ignorance, alienation from God, anger at God, rejection of the divine, disconnecting with transcendent, fear of punishment by God, loss of God’s love) (Kohls et al., 2009; Underwood, 2011). The instrument consists of 16 items. The first 15 are rated on a six-point Likert scale with response categories ranged from 1 (many times a day) to 6 (never or almost never). The 16 item—“In general, how close do you feel to God?”—is scored from 1 (not close at all) to 4 (as close as possible) and must be recoded. The total score is obtained by summing all answers and it ranges from 16 to 94. Lower total scores reflect higher frequency of daily spiritual experiences. The tool is reliable and valid, used in many languages, and applicable to people of different religions as well as atheists and agnostics (Underwood, 2011). The index of reliability of the Slovak version was high (Cronbach alpha: 0.98).
The Zung Self-rating Depression Scale (SDS) (Zung, 1965) has been designed to measure severity of depressive symptoms. The scale consists of 20 self-reported items with responses from 1 (a little of the time) to 4 (most of the time), higher score corresponds to a higher frequency of symptoms. Ten items are positively and 10 are negatively worded. Positively laid items are reverse-scored. Raw score is the sum of the scores of items, it ranges from 20 to 80. The raw score is converted to the SDS index score with the lowest score of 25 and the highest of 100. The scores are interpreted as follows: less than 50 without depression, 51 to 59 minimal or mild depression, 60 to 69 moderate-to-marked depression, and 70 and more severe depression. Total scores on the Zung SDS indicate the level of depressive symptoms which may be of clinical significance. This instrument has been recognized as reliable and valid in numerous studies in order to measure depressive symptoms (McDowel, 2006). Cronbach alpha reliability coefficient of SDS in this study was 0.83.
Personal Wellbeing Index—Adult (PWI-A) (International Wellbeing Group, 2013) has been designed to measure the cognitive dimension of subjective well-being in general adult population, aged not less than 18 years. The PWI-A consists of seven items of satisfaction. Each item relates to a specific domain, such as the standard of living, health, life achievements, relationships, safety, community, and future security. These domains represent the construct of global life satisfaction—cognitive dimension of SWB. Global life satisfaction is also evaluated by a separate item (“How satisfied are you with your life as a whole?”), prior to the seven domains, which is calculated solely. Respondents evaluate items on a scale of 0 (complete dissatisfaction) to 10 (complete satisfaction with life). Scores within each item are converted on a 0 to 100 scale. Total scores are calculated as the mean of the sum of individual items. The goal is to get the percentage of the scale maximum (%SM). Based on biological and genetic set-point theory of SWB, Cummins et al. (2014) and Cummins and Wooden (2014) state that individual values of SWB on a 100-point scale are usually normally distributed between 70 and 90 points (or %) on the PWI-A scale, with normal set-point range of plus-or-minus 20 points for each individual. The score between 50 and 70 on the PWI-A may reflect the lower limit of the set-point range, but may also indicate a decrease in cognitive SWB, as it is difficult to determine which case of cognitive SWB (normal or decreased) it is from one PWI-A measurement at one particular time. The score below 50 indicates a significant disruption in homeostatic system and worsening of SWB. The normative values of SWB in western countries reach 70% to 80% SM, while in non-western countries the values are lower by approximately 10% of the SM (Cummins et al., 2003). The PWI is a reliable and valid cross-cultural instrument (International Wellbeing Group, 2013). In this study, Cronbach alpha coefficient of seven-items PWI-A reached the value of 0.903.
Sociodemographic data relating to age, gender (male, female; male was set as reference), marital status (living with a partner, living alone; living with a partner was set as a reference), education (primary, secondary, university; primary was set as a reference), and religion affiliation were collected.
Statistical Analysis
The data were collected and calculated in MS Excel, G-Power 3.1, IBM SPSS Statistics 25, and Process for SPSS 3.5 software (Hayes, 2018).
Basic descriptive analysis (frequency, percentage, mean [M], standard deviation [SD]) was performed for the characteristics of sample, level of spirituality, depressive symptoms, and cognitive SWB. A z-test was applied for normality test of the DSES, SDS, and PWI-A using skewness (z = skew value/standard error of skewness value) with accepted z-value to 3.29 corresponding with a normal distribution in a medium-sized sample (50 < n < 300) (Kim, 2013). The z-test reached the value of 3.54 for the DSES (right asymmetric distribution), 1.54 for the SDS, and 1.94 for the PWI-A (symmetric distribution). Due to symmetric distribution of PWI-A and SDS we decided for parametric Pearson correlation.
A multiple regression analysis using Enter method was performed to determine the variables associated with subjective well-being. Sociodemographic variables (age, gender, marital status, and education level) were included in the first model, SDS was added in the second model and DSES in the third model. Multicollinearity was assessed by variance inflation factor (VIF) values of predictors. VIF value higher than 2.5 generally reflects substantial collinearity (Johnston et al., 2018). In this study, VIF values of independent variables ranged from 1.057 to 1.798 which excluded collinearity effect.
Finally, mediation analysis was performed to explore whether the association between depressive symptoms and cognitive SWB is mediated by spirituality. Socio-demographic covariates used in the mediation analysis were age, sex, marital status, and education level. We use Process for SPSS (model 4, 95% Confidence Interval [CI], number of bootstrap samples 5,000) to implement mediation analysis. Correlation analysis and a series of linear regression analyses were conducted. To support mediation, the subsequent conditions must be met (Baron & Kenny, 1986): 1. independent variable (depressive symptoms) must predict the dependent variable (subjective well-being), 2. independent variable (depressive symptoms) must affect the mediator (spirituality), 3. mediator (spirituality) must influence the dependent variable (cognitive SWB) in the third equation. In the third equation, independent variable (depressive symptoms) and mediator (spirituality) must be entered as predictors. When all of the above conditions are met, complete mediation exists, when the effect of the independent variable (depressive symptoms) on the dependent variable (cognitive SWB) drops to zero after the mediator (spirituality) has been included. Partial mediation occurs, when the influence of the independent variable (depressive symptoms) on the dependent variable (cognitive SWB) is reduced after the mediator (spirituality) is controlled. Direct and indirect effects were calculated. As a final point, the Sobel z-test was carried out to test the mediating effect of spirituality.
Results of statistical tests were considered statistically significant at the alpha level ≤0.05.
Ethical Aspects
Prior completing of the questionnaires, participants were informed about the purpose of the study, assured that completing the questionnaire is voluntary and anonymous, that no risks are associated with participation in the research, they may withdraw their participation in the research at any time, and the data obtained shall be confidential and used only for scientific purposes. All participants had to sign a written consent prior to participation in the study. The study was performed in accordance with the Declaration of Helsinki. The Ethical Committee of the Faculty of Medicine, Pavol Jozef Šafárik University in Košice (no. 9N/2020) and ethical committees or institutional review boards from two hospitals (General Hospital Rimavská Sobota, Gemerclinic, Hnúšťa) and three residential homes (Residential Homes and Social Services Homes in Rimavská Sobota, Tisovec, Klenovec) in Slovakia approved this study.
Results
Sample Characteristics
The study enrolled 250 older adults with a mean age of 75.91 (±7.60) years. The research sample involved predominantly women (64.8%), living alone (77.8%), with completed secondary education (52.4%), followed primary education (35.6%) and university (12.0%). Almost all study participants claimed to be religious (97.2%). Majority of the study sample was Roman Catholic (49.6%) and Lutheran (34.0%), then Reformed (6.8%), Greek Catholic (4.0%), and Baptist (2.8%).
The mean score of daily spiritual experience was 44.00 (±21.55), with minimal score 16 and maximal 90 (lower scores indicate higher spiritual experiences). The mean score of depressive symptomatology reached the value of 58.23 (±10.68), indicating minimal to mild depressive symptoms; the minimal value was 28.75 and maximal 93.30. The mean score of subjective well-being was 59.29 (±19.12) with minimal value 8.57 and maximal 97.14.
Correlation Analysis
Bivariate correlation analysis between variables is shown in Table 1. Outcomes indicated statistically significant associations between depressive symptoms and socio-demographic variables (age, marital status, education), with spirituality, and cognitive SWB. With regard to control variables, higher levels of depressive symptoms were associated with higher age, living alone without partner, and lower education level. Overall, higher levels of depressive symptomatology were associated with lower frequencies of spiritual experiences and poorer cognitive SWB. Higher frequency of spiritual experiences (lower score value of the DSES means higher frequency spiritual experiences) was associated with a lower incidence of depressive symptoms and with higher cognitive SWB (higher life satisfaction). We also found that higher frequency of spiritual experiences were associated with higher age and female gender. Higher level of cognitive SWB was associated with lower occurrence of depressive symptomatology, higher frequency of spiritual experiences, female gender, living with partner, and higher education level.
Correlation Analysis Between Variables.
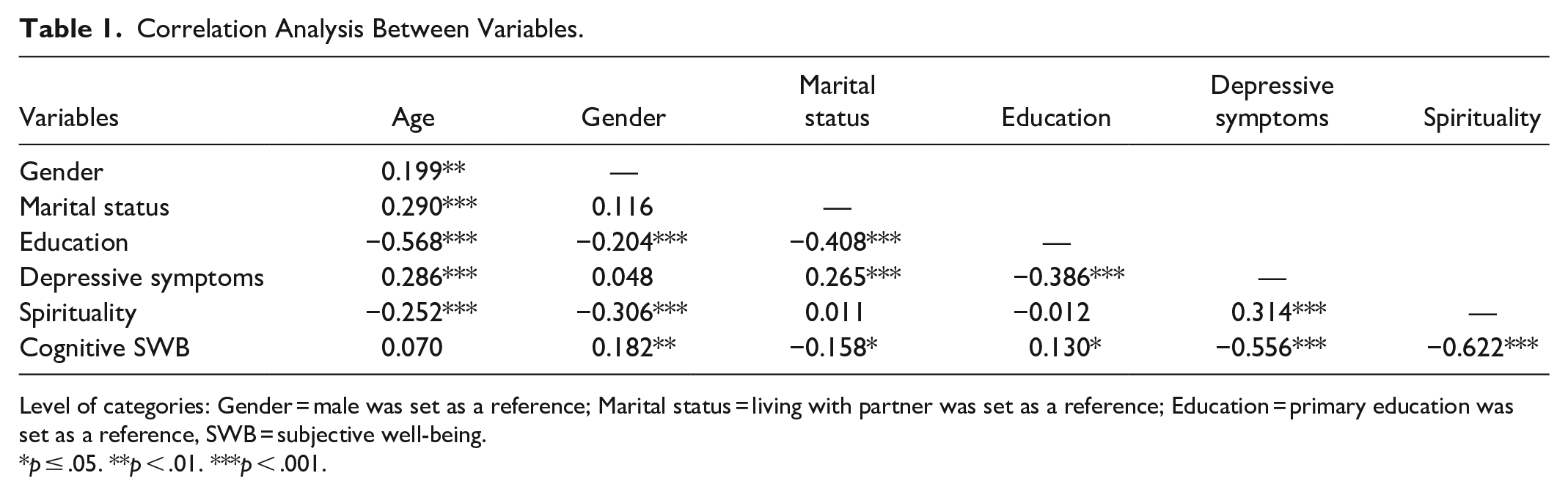
Level of categories: Gender = male was set as a reference; Marital status = living with partner was set as a reference; Education = primary education was set as a reference, SWB = subjective well-being.
p ≤ .05. **p < .01. ***p < .001.
Linear Regression Analysis
We applied the Enter method in linear regression to assess the variables associated with cognitive SWB. (Table 2). In the first model, sociodemographic variables significantly predicted cognitive SWB and explained 8.2% variance of cognitive SWB. After depressive symptoms were added to the second model, marital status and level of education lost their significance in the association with cognitive SWB. Depressive symptomatology, age, and gender explained 38.9% variance of cognitive SWB. In the third model, only depressive symptoms and spirituality significantly predicted cognitive SWB; explaining 53.8% of its variance.
Regression Analysis of Depressive Symptoms and Spirituality on Cognitive Subjective Well-Being.
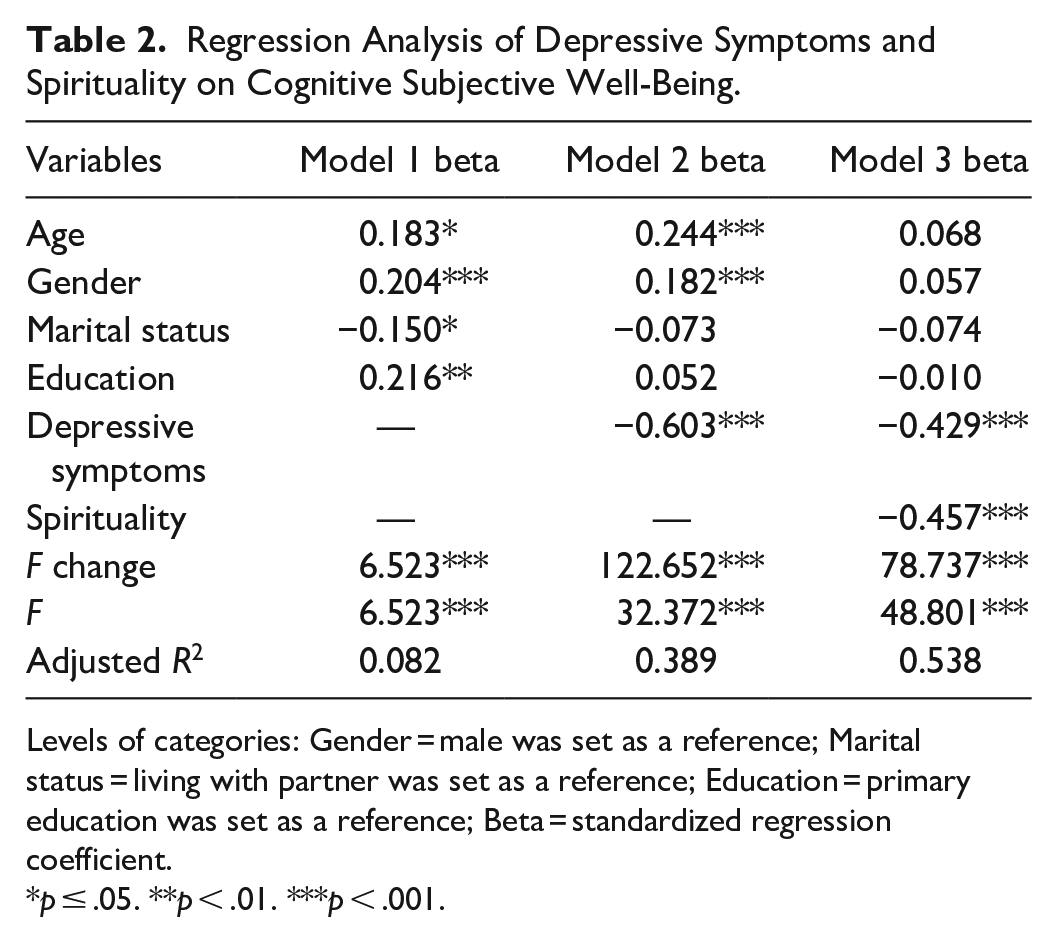
Levels of categories: Gender = male was set as a reference; Marital status = living with partner was set as a reference; Education = primary education was set as a reference; Beta = standardized regression coefficient.
p ≤ .05. **p < .01. ***p < .001.
Mediation Analysis
To test the mediation model, a series of regression models were estimated (Table 3). Mediating effect of spirituality was calculated on the associations between depressive symptoms and cognitive SWB when controlled for covariates: age, gender, marital status, and education. The total effect of depressive symptomatology on cognitive SWB was significant (c = −1.08, t = −11.08, [95%CI −1.27, −0.89], p < .001), as is the direct effect (c′ = −0.77, t = 8.38, [95%CI −0.95, −0.59], p < .001). The value of Sobel test (z = −5.05, p < .001) confirmed significance of indirect effect of depressive symptoms on cognitive SWB via spirituality (b = −0.31, [95%CI −0.48, −0.19], p < .001). The direct effect of the depressive symptoms on the cognitive SWB was 71.3% (direct to total ratio), the indirect effect of the depressive symptomatology on the cognitive SWB via spirituality was 28.7% (indirect to total ratio). In the tested model, partial mediation of spirituality on the association between depressive symptoms and cognitive aspect of subjective well-being was identified (Figure 1). Mediation analyses also showed that older age and female gender may explain additional variability in association between spirituality and cognitive SWB.
Regression Analysis for Presumptive Mediation Model with Age, Sex, Marital Status, and Education as Covariates.
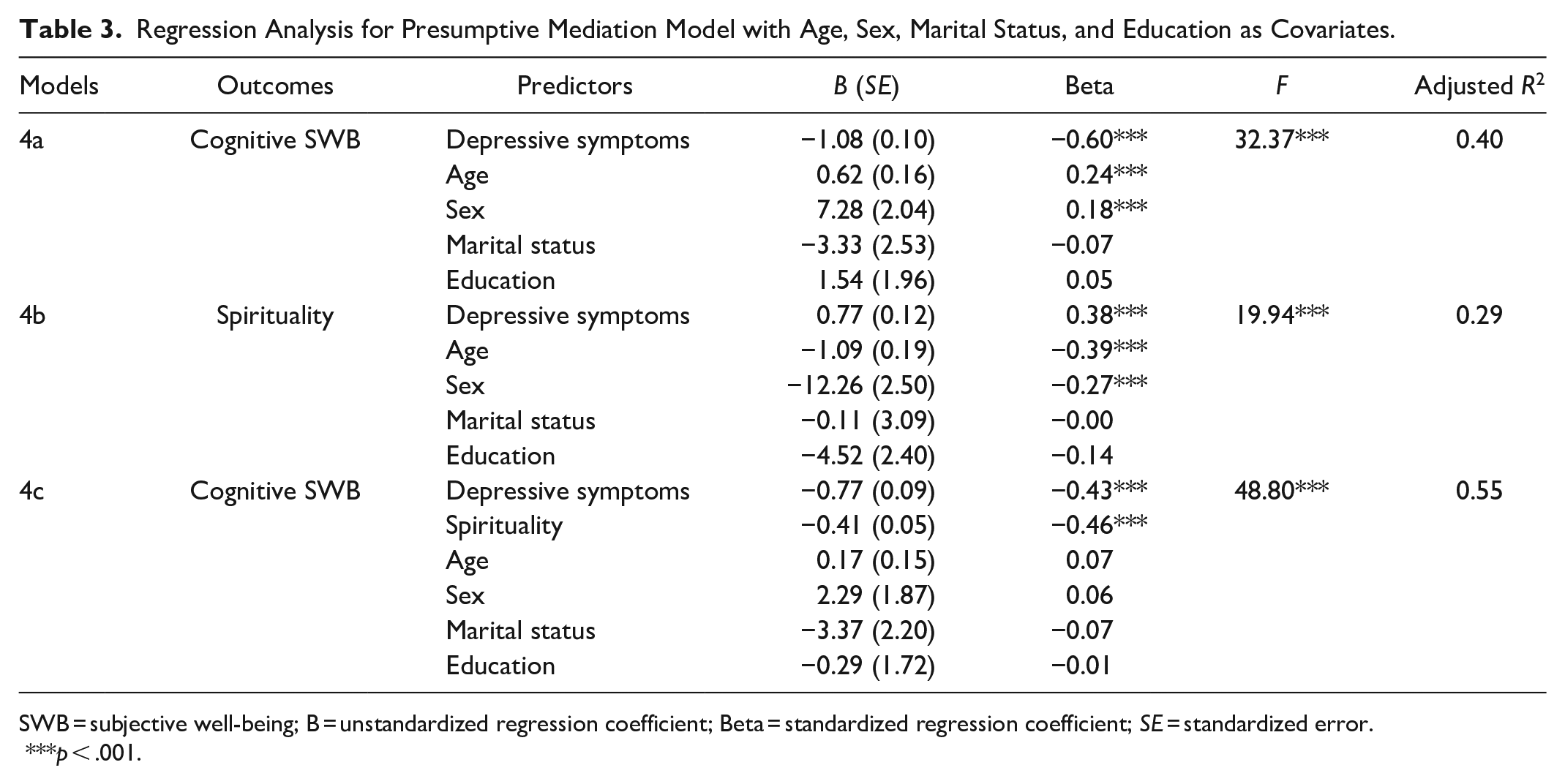
SWB = subjective well-being; B = unstandardized regression coefficient; Beta = standardized regression coefficient; SE = standardized error.
p < .001.
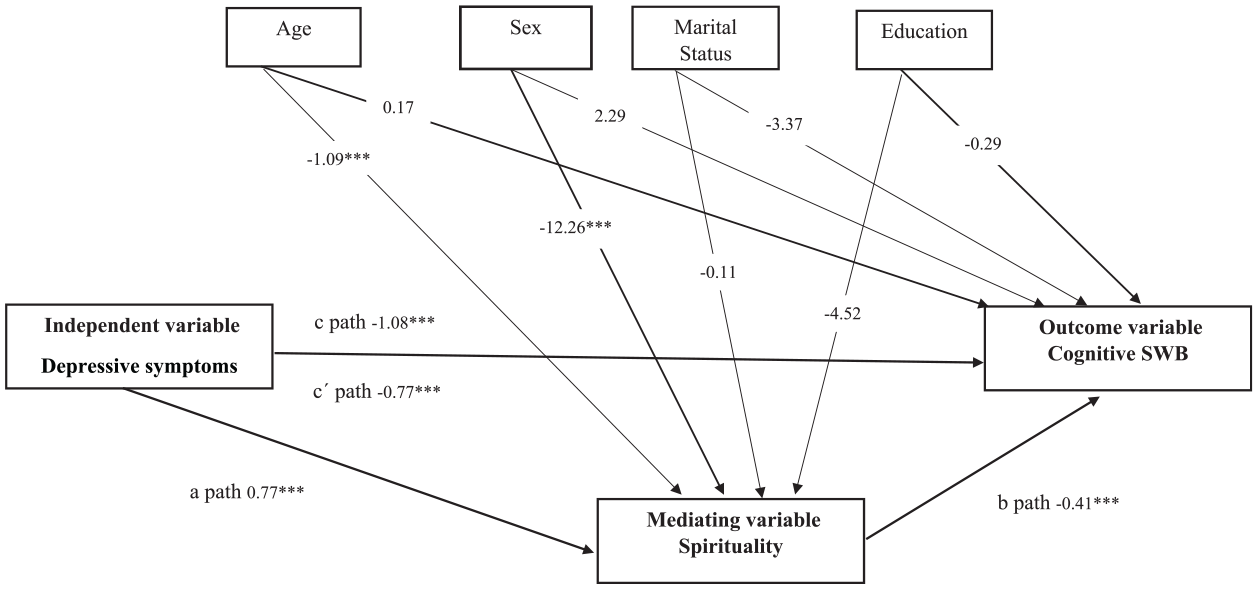
Mediating effect of spirituality on the association between depressive symptoms and cognitive subjective well-being with age, sex, marital status, and education as covariates.
Discussion
Our results provide suggestive evidence of the association between depressive symptoms, spirituality, and cognitive subjective well-being (life satisfaction) in older adults. Furthermore, spirituality mediated the association between subjective well-being and depressive symptomatology.
The cognitive SWB in the Slovak elderly people reached 59.29% of the scale maximum, that is below the normative value for non-western, post-communist Eastern European countries (60%–70% SM) (Cummins et al., 2003; Steptoe et al., 2015). We further revealed higher level of cognitive SWB in women, participants living with a partner, with higher education, and higher age. However, these associations attenuated and were no longer significant when depressive symptomatology and spirituality were added in the final model. Previous studies conducted in the elderly population (Enkvist et al., 2012; Steptoe et al., 2015) have shown different results between socio-demographic variables and cognitive SWB (life satisfaction). Enkvist et al. (2012) found no association between sex and SWB, however the level of life satisfaction decreased with increasing age, depressive mood, and physical symptoms. The review study of Steptoe et al. (2015) revealed that life satisfaction in high-income countries was found to increase with age. However, in Eastern Europe, countries of the former Soviet Union, Africa, and Latin Amerika, the level of life satisfaction was found to decrease with higher age. Furthermore, an association between, high level of stress, worry, poor physical health, and lower level of life satisfaction was also confirmed in elderly people (Steptoe et al., 2015). Life satisfaction may be affected by many factors such as socio-economic situation, regular retirement, family relationships, social support, and activities (Steptoe et al., 2015). We found that higher level of depressive symptomatology and lower frequency of spiritual experiences with positive valence were associated with lower level of cognitive SWB. Our study highlighted, that even mild depressive symptoms, as experienced by study participants, may significantly contribute to decrease in cognitive SWB. The results of our study are consistent with previous research conducted in various countries (Enkvist et al., 2012; Lawler-Row & Elliott, 2009). Depression is a prevalent mental disorder in older population, more common in women, older people, disabled people, and people suffering from physical comorbidities (Enkvist et al., 2012; Lotfaliany et al., 2018; Sivertsen et al., 2015), which implies the need for more intensive efforts for screening and detection of depression in elderly as well as its optimal treatment strategy. In line with our findings of the association between spirituality and cognitive SWB, previous studies also revealed positive association between spirituality and cognitive SWB (life satisfaction) (Lawler-Row & Elliott, 2009; Villani et al., 2019) and psychological well-being (Lawler-Row & Elliott, 2009; Thauvoye et al., 2018). An explanation for this phenomenon, may be that people who have a higher connection with the sacred source or have more positive spiritual experiences tend to evaluate their lives more positively (Kohls et al., 2009; Villani et al., 2019).
We further identified the mediating effect of spirituality on the association between depressive symptoms and cognitive aspect of SWB. Thus, it may be assumed that higher frequency of spiritual experiences with positive valence could help to alleviate depressive symptoms and improve cognitive SWB. Univariate analyses showed significant association between female gender, older age, and higher level of spirituality. Mediation analyses also indicated that older age and female gender may explain additional variability in association between spirituality and cognitive SWB. All in all, it needs to be considered that the mediating effect of spirituality on the association between depressive symptomatology and cognitive SWB may be especially profound in older people and female participants. Results of previous studies also showed that older people tend to be more spiritual, whereas older female participants reported higher levels of spirituality than older male participants (Forlenza & Vallada, 2018; You et al., 2009; Zimmer et al., 2016). Our findings are congruent with the current study by Lee and Salman (2018) who found the mediating effect of spirituality on the association between depression and mental component of quality of life in the elderly. Another study (White, 2016) revealed a mediating effect of spiritual self-care practices on relationship between depression and quality of life in patients with heart failure. The study of Aglozo et al. (2019) demonstrated an indirect effect of spirituality on subjective well-being (cognitive aspect measured as life satisfaction and affective component measured as positive and negative affect) through meaning in life and optimism in Ghanaian older adults.
It is also known that the positive aspects of spirituality and/or religion can act as a buffer against stress and can help seniors cope with stressful life events such as loss of a partner, or limitation in physical, mental, and social functioning (Pargament et al., 2004; Zimmer et al., 2016). As indicated by previous research, we may assume that higher frequency of spiritual experiences with positive charge such as feeling of God’s presence, the joy of this connection, the feeling of God’s love, etc., evaluated by the DSES in our study are protective, may help to diminish depressive symptomatology and enhance cognitive aspect of SWB in older adults. On the contrary, results of some previous studies showed that negatively valenced spiritual experiences (such as to feel abandoned by God, punished by God) were associated with distress (Kohls et al., 2009), higher level of negative affectivity, and lower level of life satisfaction (S Dy-Liacco & Werdel, 2019). Therefore, future studies should assess the associations between subjective well-being and spiritual experiences with both positive and negative valence in order to fill gaps in the current knowledge.
In this study, we did not evaluate the impact of religion or religion denomination, however almost all participants in the study declared to be religious. The effect of spirituality in our sample could also be related to strong religious values in which seniors grew up and retained them into later life. The majority of Slovak population is considered to be religious (Majo, 2016), while Christianity is the predominant religion in Slovakia. According to the latest available population census in 2011, 75.97% of the population were identified to be religious, 13.44% have established themselves as irreligious, and 10.59% have not specified their affiliation (Ministerstvo kultúry Slovenskej republiky. [Ministry of Culture of the Slovak Republic], 2017).
Next, as some religious or spiritual activities (e.g., church attendance) represent source of social interaction that may decrease loneliness and increase well-being (Malone & Dadswell, 2018; Zimmer et al., 2016), future research should also include measures of social support and loneliness to shed more light on the association between spirituality, depression, and SWB. Finally, it would also be useful to assess the associations between spirituality, depression, and eudemonic well-being in different age groups including adolescents and adults.
Implications for Nursing Practice and Research
Our study showed that depressive symptoms and spirituality are associated with cognitive SWB in older adults. We further ascertained that spirituality was associate with higher scores of cognitive subjective well-being (life satisfaction). Promoting intrinsic and extrinsic spiritual and/or religious activities can be a valuable source of enhancing the cognitive SWB of older adults, better adaptation to old age, and successful aging. Thus, health care and social care professionals should be aware that interventions aimed at spirituality enhancement may help improve cognitive SWB of older people. Given that, older people should be treated in line with holistic care approach. Professionals dealing with elderly population should be aware of their spiritual beliefs in order to provide a more comprehensive care. Future studies should focus on applying and testing selected spiritual interventions on mental health and well-being of the elderly. Future research should also include a measure of spiritual experience with negative valence, religious coping, social support, loneliness, or religion denomination to shed more light on the association between spirituality, depression, and SWB.
Authors (Underwood & Teresi, 2002) of the DSES instrument considered it suitable for assessing spirituality of people from various religious and not religious backgrounds. However, De Jager Meezenbroek et al. (2012) in their review criticize the fact that many items in the DSES instrument contain the term God, making it more suitable for a religious population. Therefore, further studies should focus on testing the validity of the DSES instrument in populations of atheists and agnostics. Finally, future studies should also use different measures of spirituality to cover this human experience more fully.
Limitations
To our knowledge, this is the one of first studies examining the associations between depressive symptoms, spirituality, and cognitive SWB in elderly population. However, the study has several limitations. The cross-sectional character of the study does not capture causal relationships. Next limitation represents the convenience sampling as it may potentially lead to skewed results. Participants in our study were found to experience mostly mild to moderate depressive symptoms. Therefore, it is difficult to state to what extent the statistically significant findings are also clinically significant. Furthermore, it should be considered that no formal psychiatric diagnosis of depression was established in our participants, and depressive symptomatology was only self-reported. Further studies with participants reporting higher levels of depressive symptoms, or even with a diagnosis of depression, may shed more light on the mediating effect of spirituality on cognitive SWB. Furthermore, our sample consisted of Slovak participants; thus, our results may be less generalizable. Nevertheless, also other European countries such as Poland or Slovenia have high prevalence of the Roman Catholic religion. Furthermore, previous research also showed correlation between the Roman-Catholic religious affiliation and life satisfaction in eastern and central European countries (Bodogai et al., 2020). As the study sample consisted predominantly of female participants, our results may be less generalizable to male population. Finally, we did not assess the effect of confounding variables such as physical health, comorbidity, social support, loneliness, religious coping, etc., that may also potentially influence cognitive SWB.
Conclusion
The results of this study showed significant associations between depressive symptomatology, spirituality, and cognitive subjective well-being in older adults. Holistic and comprehensive care focused on enhancement of spiritual activities seems to represent a relevant interventional strategy for diminishing the level of depressive symptomatology and well-being improvement in elderly population.
Footnotes
Acknowledgements
The authors would like to express gratitude to Lynn Underwood, Ph.D., for her permission to use the DSES in this study, PaedDr. Karol Sovári Soós and PhDr. Radoslav Berecký for their support in the manuscript translation, and to older adults who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Slovak Research and Development Agency under Grant no. APVV-15-0719.