
Abstract
This study aims to analyze the effectiveness of nurse-conducted telephone guidance for bowel preparation before a colonoscopy after patients have received routine recommendations. A randomized, controlled, colonoscopist-blinded clinical trial was conducted at a Brazilian teaching hospital. Participants included patients aged ≥ 18, who were available via telephone (the intervention group was given guidance over telephone). Of the 109 total participants, 55 were placed into the intervention group (IG) and 54 into the control group (CG). Outcomes included Boston Bowel Preparation Scale (BBPS) scores, adenoma detection, and cecal intubation. Total BBPS scores showed a statistically significant reduction for the IG when compared to the CG (p < .001) (all colon segments were evaluated thus). Cecal intubation occurred in all exams for those in the IG (p = .027). No significant differences were found regarding adenoma detection. The examined educational intervention was an effective strategy for reeducating patients about bowel preparation.
Introduction
It is important to educate patients about bowel preparation prior to colonoscopy procedures in order to ensure their compliance with medication intake and dietary restrictions, thereby increasing the quality of the procedure (Guo et al., 2017; Hernández et al., 2019; Kastenberg et al., 2018; Quaresma et al., 2018). Patients require such guidance not only to ensure effectiveness, but also to avoid complications that could occur during preparation (Kastenberg et al., 2018; Quaresma et al., 2018). This guidance entails procedural instructions, information regarding how the examination will be conducted, associated risks, potential complications, benefits, discomforts, and preparatory factors, such as required medications and dietary considerations (Guo et al., 2017; Hernández et al., 2019; Kastenberg et al., 2018; Quaresma et al., 2018).
Ideal bowel preparation involves the complete elimination of fecal material without causing damage to the mucosal surface. Ingested medications must, therefore, be low-cost, have a pleasant taste, require a minimal period of time between ingestion and elimination, and be designed to minimize discomfort and/or avoid significant changes in fluid/electrolyte levels (Guo et al., 2017; Hernández et al., 2019; Kaiser-Júnior et al., 2018). Inadequate preparation can lead to unsuccessful examinations, impaired polyp detection, increased examination time, complications, an increased probability of procedural repetition, delayed patient treatment, and increased colonoscopy-related costs (Guo et al., 2017; Hernández et al., 2019; Kastenberg et al., 2018). However, current literature shows that nurse-led guidance on bowel preparation prior to colonoscopy is associated with significantly improved results (Andrade et al., 2017; Carvalho et al., 2012). When combined with regular in-person guidance provided by health professionals, a meta-analysis also discovered that elements such as educational leaflets, telephone calls, text messages, and phone applications significantly improved bowel preparation results and increased patient availability when repeat preparations were required (Guo et al., 2017). The authors ultimately concluded that factors related to patient instruction were as important as the chosen preparation method.
Contact via telephone is often an attractive, low-cost method for motivating ongoing health care (Nicolau et al., 2017). In Brazil, telephone interventions are important nursing tools for achieving and maintaining closer contact with patients. As such, they have been used for post-discharge follow-up strategies in different contexts (de Sousa et al., 2017), including assessments of discharge guidance and behavioral interventions in therapeutic compliance, rehospitalizations and mortality in patients with heart failure (Oscalices et al., 2019), programs designed to reduce absenteeism for return appointments to receive examination results (Nicolau et al., 2017), and assessments of the self-efficacy among puerperal women in regard to the duration and exclusivity of breastfeeding (Chaves et al., 2019). While no national studies have examined the use of telephone interventions for guiding colonoscopy patients in the process of bowel preparation, a Chinese study showed that reeducation of patients in colonoscopy preparation via telephone significantly improved the quality of bowel preparation (Liu et al., 2014).
Although the use of a telephone re-instruction approach is considered, an evidence-based approach is important to analyze whether this educational intervention can be beneficial to patients with low levels of education, such as in Brazil, where 6.4% of the population over 25 years have no schooling and 40.2% have not completed elementary school (IBGE, 2020).
In most cases, colonoscopy patients receive educational instructions regarding bowel preparation only once; that is, when scheduling their colonoscopy exams. Notably, however, the lack of understanding about proper bowel preparation (Hayat et al., 2016) can result in patients’ cancellation of the procedure, thus resulting in negative impacts to service quality, the health system, and the life of the patient. Researchers have expressed that inadequate preparation occurs in up to 30% of cases (Hernández et al., 2019), which creates a significant challenge for health professionals. Based on Hernández et al. (2019)’s research, this present study analyzed the effectiveness of nurse-led telephone guidance for bowel preparation among colonoscopy patients who had previously received routine recommendations, verbal guidance, and explanatory leaflets during their preoperative assessment.
Methods
This study conducted a randomized, controlled, parallel, two-arm, evaluator-blinded clinical trial. All research was approved by the Research Ethics Committee. This study was also registered with Brazilian Registry of Clinical Trials (ReBEC). Based on norms established by the Consolidated Standards of Reporting Trials (CONSORT; Martins et al., 2009), a 22-item checklist and diagram were used to outline participant procedures during each study stage, to standardize the randomized clinical trial report. All procedures were conducted in the endoscopy clinic.
The inclusion criteria were as follows: patients who required colonoscopies must be (1) over 18 years, and (2) available via telephone based on information in their electronic medical records. An intervention group (IG) and a control group (CG) was established. Additionally, participants in the IG were required to answer their phones on at least one of the three calls placed by the researcher during previously established time periods; that is, from 8 am to 7 pm, Monday through Friday. Patients were excluded from study if they had undergone total or partial colectomies, intestinal loop stenosis, experienced diarrhea, or chronic constipation, had been diagnosed with Chagas disease in the intestinal tract, and/or suspected or diagnosed intestinal sub occlusion. Recruitments were conducted sequentially at the endoscopy clinic at the time of scheduling the colonoscopy. Patients who met the inclusion criteria were selected and randomized until the required sample was met.
The study protocol and data collection consisted of three moments: (1) included both CG and IG; (2) included only IG, and (3) included both CG and IG.
1) The common protocol for IG and CG was as follows: On the day of the scheduled colonoscopy at the endoscopy clinic, routine instructions (verbal instructions and explanatory leaflets) were given by the nurse and one study author. The protocol instructed patients to adhere to a light-colored liquid diet without residues (with examples) the day prior to their examinations and take three 15 mg bisacodyl® pills and 50 mg dimenhydrinate with 10 mg of pyridoxine hydrochloride (vitamin B6). On the morning of their examination, patients were instructed to drink 750 mL of a 20% mannitol solution and start fasting. This is a routine recommendation of the endoscopy clinic.
2) The protocol for IG was as follows: The intervention consisted of individualized bowel-preparation instructions that were given to participants via telephone. Specifically, 1 day prior to each respective examination, the nurse repeated all steps related to the bowel preparation protocol used by the clinic, the elements of which were previously explained in-person to patients in both the CG and IG when scheduling their colonoscopies (moment 1). Participants for IG were also given opportunities to ask questions during each guided stage.
3) Colonoscopy Day: On the day of the exam, one study author (i.e., the process manager) collected data on the study variables—sociodemographic variables (i.e., sex, age, city of residence, and education level) and patient bowel preparation prior to the exam (i.e., previous preparations, difficulties with preparation, gastrointestinal symptoms during preparation, and interference with the daily routine). Next, we included BBPS scores, adenoma detection and cecal intubation, which were obtained by one of the colonoscopists working at the clinic at the time of examination. The colonoscopists had extensive experience in performing the exam and administering the BBPS and had no knowledge of groups to which patients were assigned, thus guaranteeing evaluator blinding.
The outcome was established by Boston BBPS scores and secondary outcomes were determined by adenoma detection and cecal intubation. For the colonoscopy to be considered an effective exam, it is essential that the entire mucosa of the organ, that is, from the anal margin to the ileocecal valve, is visualized and examined. Adequate preparation also aids in the detection of adenomas, which are polyps most commonly found in asymptomatic individuals who may or may not belong to a risk group (Tariq et al., 2019). Bowel preparation was assessed using the BBPS (Lai et al., 2009; Mendez et al., 2011), which consists of three segments, including those on the right colon, transverse colon, and left colon (descending–sigmoid–rectum). Patients were given scores ranging from zero to three for each segment, which were totaled to obtain global BBPS scores ranging from zero to nine. In this regard, zero indicated an unprepared colon, while nine indicated excellent preparation without residue. To conduct the examination, it is recommended that patients receive scores of at least two for each segment. Adequate bowel preparation enhances subsequent procedural quality.
Sample calculations were conducted via simple random sampling. That is, according to a 1:1 allocation ratio, type I and II errors at 0.05 and 0.20, respectively, and mean BBPS scores equal to six (detection of one additional point on the mean in the IG when compared with the CG). Without considering confounding factors, 56 participants were thus required per group. The difference of one point was assumed considering that scores were given in units and with very few opportunities for variation (i.e., 0–9). Further, differences greater than one point would be clinically relevant, primarily for the detection of polyps (Lai et al., 2009).
Patients were randomized in a simple manner without blocking. A random sequence of zeroes (0) and ones (1) for a size of 200 was generated (therefore, more than 112 participants were required for execution) using the “runif” function in the Rv2.11.0 software. The code “0” represented the control group, while the code “1” represented the intervention group. This coding sequence was used to determine the order of patients receiving/not receiving the intervention.
All resulting information was stored in a database via the Excel program (©Microsoft, Redmond, WA, USA) and then analyzed using the SAS for Windows software, version 9.3 (©IBM, Armonk, NY, USA). Descriptive statistics were performed on all data to calculate frequencies and percentages for the qualitative variables and means, medians, standard deviations, and minimum/maximum values for the quantitative variables. A data normality test had been previously performed, thus finding an asymmetrical distribution. Further, Mann–Whitney and chi-squared tests were conducted to determine intergroup differences regarding age, sex, and educational level, while chi-squared, Fisher’s exact, and Mann–Whitney tests were conducted to determine any statistical differences between groups. Finally, the model included all sociodemographic variables, and a simple logistic regression was conducted to calculate the probability of occurrence of the binary dependent variables. In this study, p < .05 was considered as indicating significance.
Results
Participants were recruited from February to September 2018, during which time a total of 955 colonoscopy exams were performed at the clinic. After searching electronic records, it was discovered that 238 patients were without telephone contact information, had incomplete information, or listed information that was not their own (e.g., message, neighbor, basic health unit). Only 502 patients initially met the inclusion criteria of this study. Of these, however, 390 were excluded for presenting one of the pathologies listed in the exclusion criteria, thereby resulting in 112 participants following the sample calculation. Ultimately, 109 patients were selected for participation and thus divided into the IG (n = 55) and CG (n = 54). Due to non-attendance on the exam day, participant follow-up loss was 1.8% in the intervention group and 3.6% in the control group. Please see Figure 1 for a sample flowchart of this procedure.
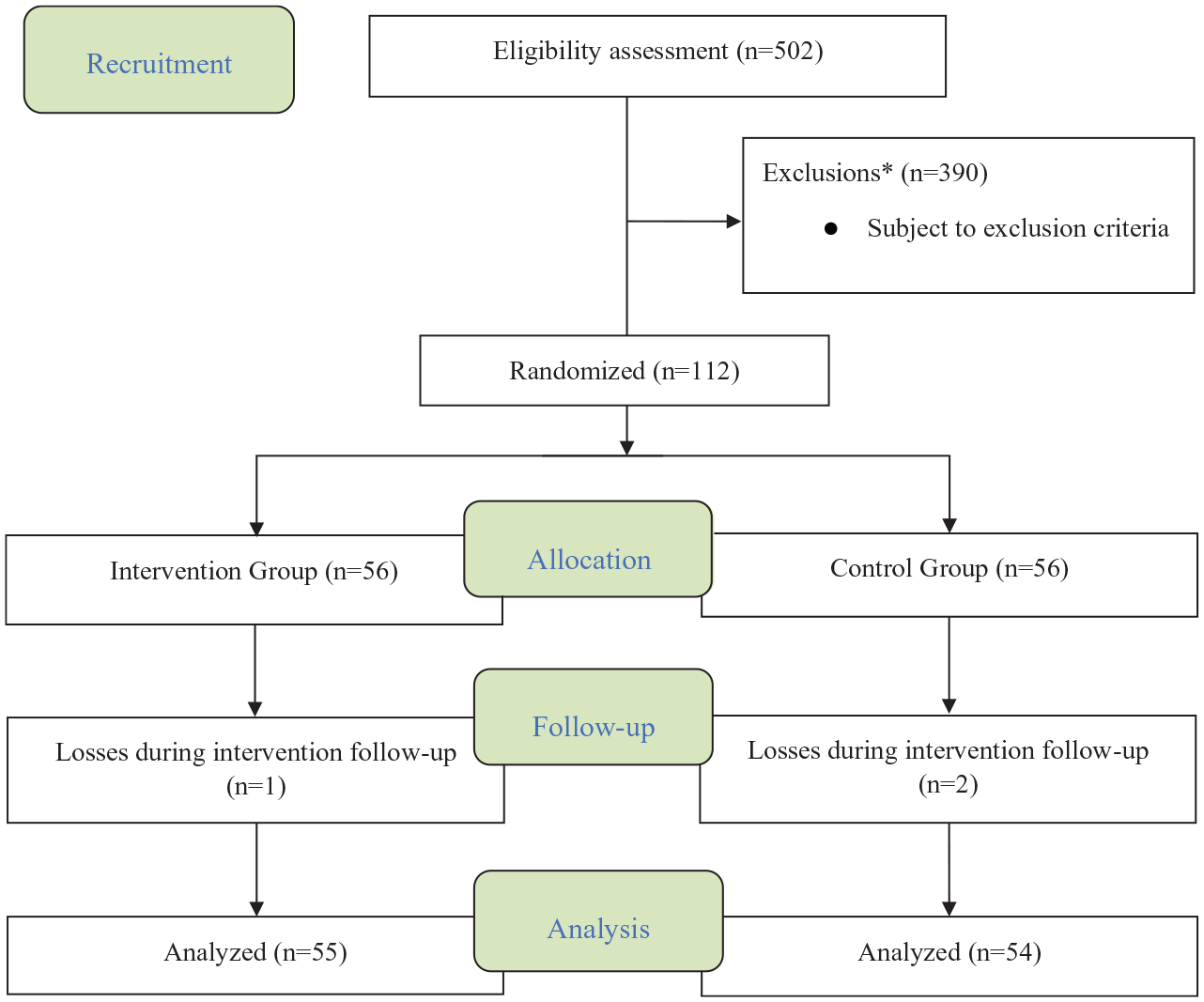
CONSORT allocation, follow-up, and analysis diagram.
Participant sociodemographic characteristics are shown in Table 1. As presented, the sample consisted mainly of women (56% and 63% for the CG and IG, respectively), while mean ages were 57 and 58 years in the CG and IG, respectively.
Participant Sociodemographic Characteristics at the Time of Colonoscopy.
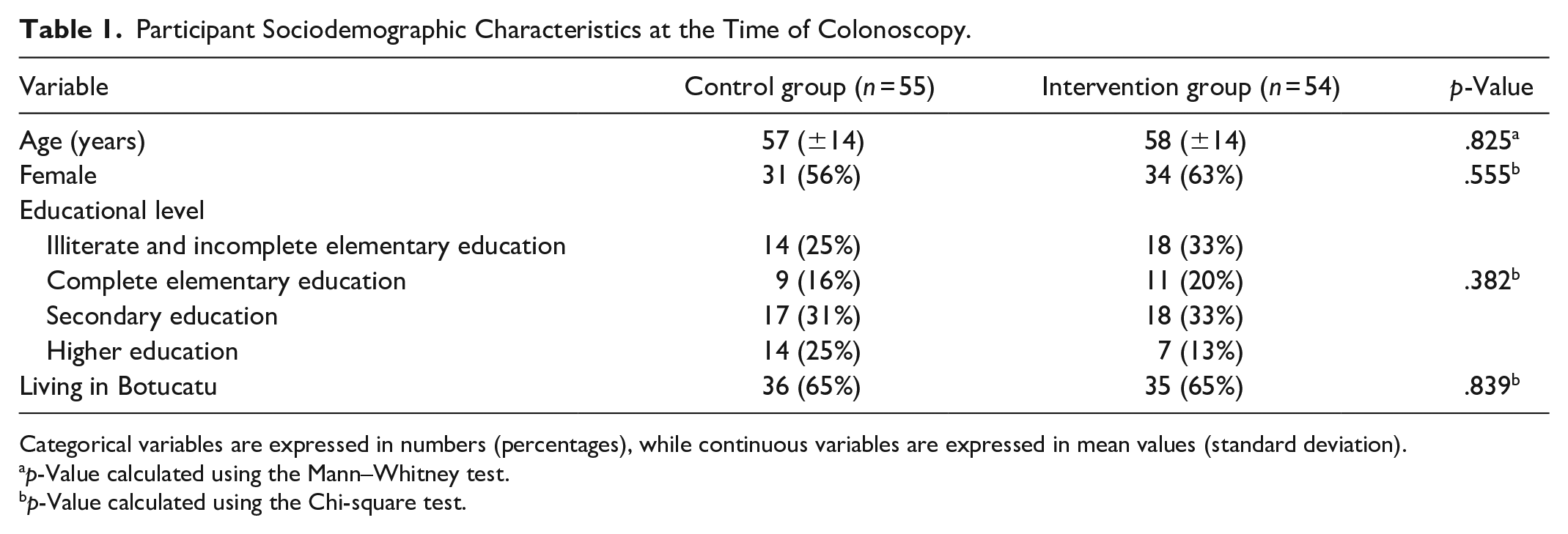
Categorical variables are expressed in numbers (percentages), while continuous variables are expressed in mean values (standard deviation).
p-Value calculated using the Mann–Whitney test.
p-Value calculated using the Chi-square test.
Table 2 shows the distribution of variables related to factors of patient bowel preparation. Although both groups had similar gastrointestinal symptoms, patients in the IG group reported greater interference (p < .001).
Distribution of Variables Related to Bowel Preparation by the Patient.

Categorical variables are expressed in numbers (percentages).
p-Value calculated via Chi-squared test.
Table 3 shows the effects of telephone guidance for bowel preparation in relation to the outcome variables. As presented, there was a statistically significant reduction among those in the IG when compared with the CG in all bowel segments evaluated via the BBPS scores, including the total score (p < .001). As for the other bowel assessment variables, cecal intubation occurred in all IG exams (p = .027), but there were no significant intergroup differences in adenoma detection (p = .337). Notably, there was a lower rate of exam rescheduling due to inadequate preparation among patients in the IG (p = .005) (Table 3).
Distribution of Patients Based on Boston Bowel Preparation Scale Scores and Number of Exam Cancellations.
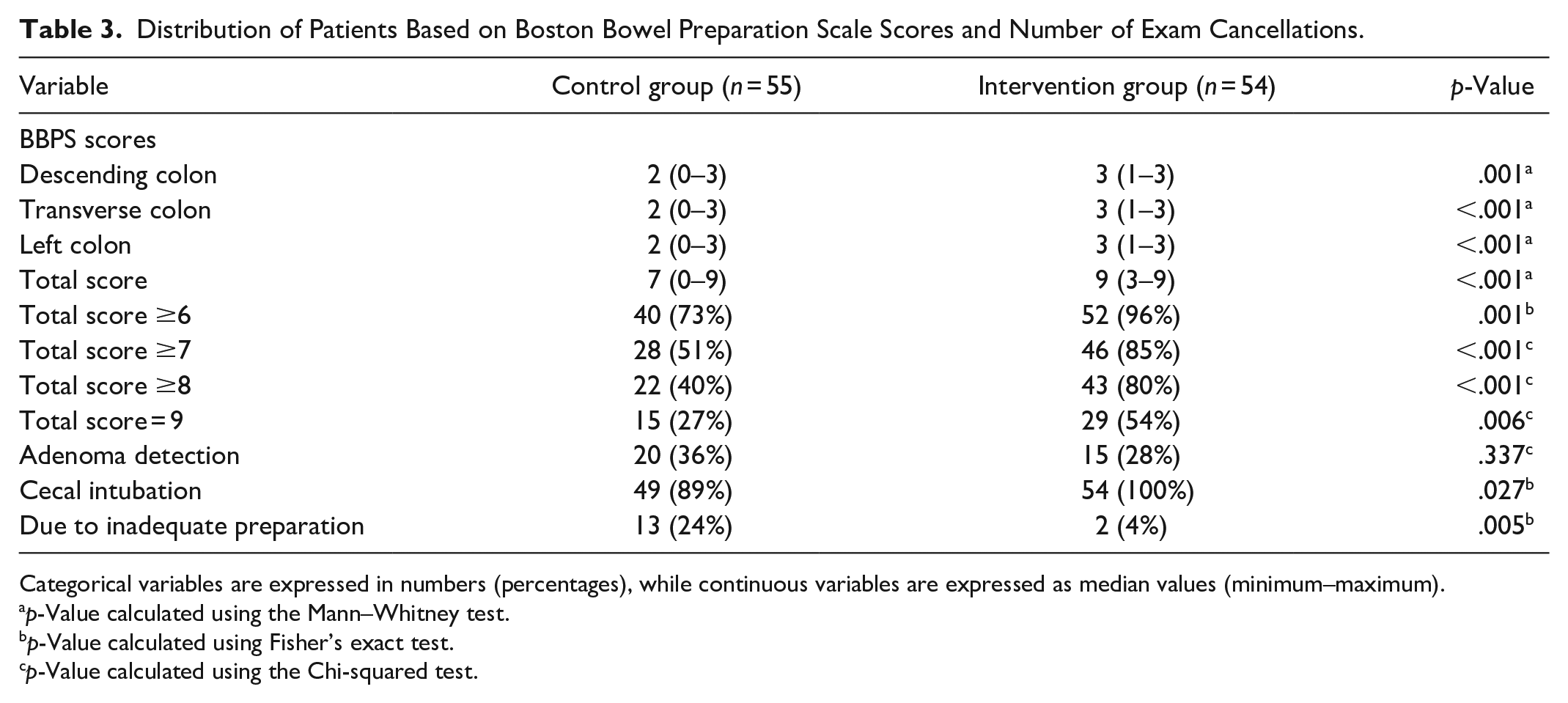
Categorical variables are expressed in numbers (percentages), while continuous variables are expressed as median values (minimum–maximum).
p-Value calculated using the Mann–Whitney test.
p-Value calculated using Fisher’s exact test.
p-Value calculated using the Chi-squared test.
Simple logistic regression models were constructed to assess the binary outcome variables (Table 4). As shown, an odds ratio of 9.1 was obtained for BBPS scores above six, thus indicating the chance of patients in the IG obtaining this score was nine times greater than those in the CG. Odds ratios were also significant for the other tested scores, demonstrating the effectiveness of the intervention. There were no significant intergroup differences in adenoma detection (p = .437). The differences in cecal intubation were significant (p = .011), with and odds ratio of 4.0. Finally, patients in the IG had lower rates of exam rescheduling, due to inadequate preparation (p = .007), with an odds ratio of 0.12.
Logistic Regression Results for Outcome Binary Variables.
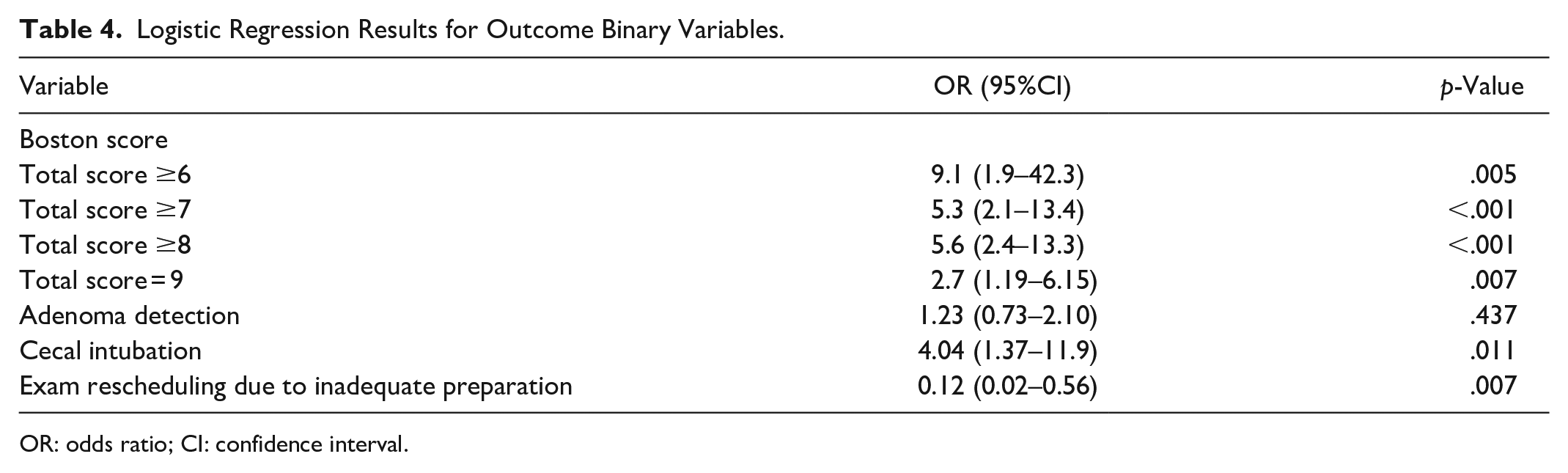
OR: odds ratio; CI: confidence interval.
Discussion and Conclusion
Discussion
This study highlighted the overall quality of bowel preparation among patients who received the nurse-led educational intervention via telephone prior to undergoing colonoscopy. Consequently, shorter waiting times between preparational instructions and exam dates are recommended. Here, it must be emphasized that interim instructions should be provided via telephone, e-mail, or text message when waiting times cannot be reduced, thus reminding patients about the necessary preparatory procedures (Cremers, 2012). In addition to telephone reeducation the day prior to colonoscopy (Liu et al., 2014), the literature also shows that other interventions can effectively improve the quality of colonoscopy preparation when compared with usual treatment conditions. This includes cellphone applications (Guo et al., 2020), educational booklets (Ergen et al., 2016), videos via SMS (Jeon et al., 2018), reeducation with reminders via telephone or SMS (Lee et al., 2015), and videos/3D animations (Veldhuijzen et al., 2017).
Mean participant age was approximately 60 years (slightly higher among women). Notably, it is recommended to complete screening and rectal cancer prevention efforts among all patients aged 50 years and older regardless of their family history or signs and symptoms (Guinhazi et al., 2019). It is therefore crucial to obtain patient sociodemographic characteristics prior to implementing any educational strategy. Previously, endoscopists conducted a randomized, controlled, and blinded study among 281 patients in Korea for the purpose of evaluating the effectiveness of sending them short educational videos in bowel preparation, via smartphone, prior to colonoscopy. It was found that the strategy was successful, especially among participants aged 30 to 40 years (Jeon et al., 2018). The authors believed this may have been due to how younger populations tend to use smartphones more frequently.
As for educational levels in this study, 25% and 33% of participants in the CG and IG were illiterate or had completed elementary education, respectively, which is consistent with the region where the research was conducted. However, these individuals deserve the attention of health professionals, since the quality of bowel preparation and procedural success not only depend upon the skill of the examining physician, but also upon the understanding of the patient who must follow the provided instructions (Ergen et al., 2016; Guo et al., 2020; Jeon et al., 2018). A previous randomized, blinded study conducted among 125 patients in Portugal showed that 69.2% of participants with education levels higher than elementary schooling exhibited good to excellent bowel preparation, while only 37.5% of those with lower education levels exhibited adequate preparation (Carvalho et al., 2012). Further, researchers have stated that individuals who are illiterate, from lower socioeconomic classes, have mobility difficulties, are elderly, take opiates, or are hospitalized tend to have greater difficulties in conducting good bowel preparation (Rembacken et al., 2012).
As for bowel preparation results in this study, gastrointestinal symptoms were similar in both groups. However, patients in the IG reported greater intensity and interference in this regard (p < .001). This intergroup difference is likely because patients in the IG prepared for their colonoscopies with greater rigor. It can also be inferred that those who received telephone guidance established bonds with the nurse, thus developing a trusting relationship when reporting interferences during bowel preparation. Indeed, there are several ways to build the nurse-patient bond, one of which is effective communication.
Previously, a Canadian study traced quality indicators from the perspective of individuals undergoing colonoscopy, reporting three issues that influenced the quality of care that patients received, including communication, comfort, and the service environment. When considering quality indicators, patients focused more on what occurred prior to colonoscopy than on potential complications (Sewitch et al., 2013). In this regard, more than 80% of participants assessed several factors as highly important, including four communication items (i.e., clear instructions, detailed information, knowing what to expect, and getting timely results) and five comfort items (i.e., dignity, being treated with respect, team attitude, being treated as an individual, and pain control; Sewitch et al., 2013).
This present study analyzed the outcomes of colon cleansing based on BBPS scores, the presence of adenoma, and cecal intubation. A previous related study proposed necessary procedures and indicators of structure, process, and results when applying and evaluating colonoscopy quality, thus finding 13 specific indicators; of these, the quality of intestinal cleansing was characterized as a process indicator because it facilitates the detection of a colon adenoma—an outcome indicator (Sánchez-del-Río et al., 2018). Cecal intubation was also considered an outcome indicator because it enabled the quantification of colonoscopies resulting in complete colon exploration (Sánchez-del-Río et al., 2018).
The BBPS has widely been used as a bowel-preparation quality indicator, with the literature showing that scores of 6 are the minimum expected for conducting the exam; repetition is suggested for any lower scores (Adike et al., 2018; Kastenberg et al., 2018; Lai et al., 2009). In this study, telephone guidance was found to improve colon cleansing results among participants in the IG. This included all colon segments assessed via BBPS scores, including the total score. An intergroup comparison conducted via logistic regression also showed that the intervention was effective when considering all scores. These results support those of a clinical trial conducted among 258 patients to evaluate the effectiveness of text messages informing patients about the date of the procedure, laxative medications, and dietary requirements (Adike et al., 2018). That is, the intervention group had higher BBPS scores, better cecal intubation, and enhanced polyp detection (Gálvez et al., 2017). Another randomized, controlled study among 390 participants compared the relevance of traditional instructions given at the service location versus traditional instructions with reminders via telephone or SMS 2 days before colonoscopy, thus finding a significantly higher total BBPS score among participants in the reinforced education group (Lee et al., 2015). Further, a randomized, controlled endoscopist-blind study conducted among 283 patients in order to compare the impact of reeducation via smartphone concerning the quality of bowel preparation for colonoscopy found a mean BBPS score of 7.53 among intervention recipients versus 6.29 in the control group (p < .001; Back et al., 2018).
Although the literature proves a relationship between bowel cleansing and adenoma detection (Gálvez et al., 2017; Sánchez-del-Río et al., 2018), this study found no significant intergroup differences in that regard. Our data were consistent with studies (Gálvez et al., 2017; Rembacken et al., 2012) that included patients undergoing their first colonoscopies, and which found that an educational video on bowel cleansing was effective. The researchers found improved bowel preparation among the intervention group, but with similar adenoma detection rates between groups (Hayat et al., 2016). Other researchers who found no associations between BBPS scores and adenoma detection believed the discrepancy could be related to better visualization of the mucosa when cleaning and aspiration are necessary during the exam; that is, in regard to cases of inadequate preparation (Adike et al., 2018).
A second important aspect is that telephone guidance was found to be extremely relevant based on the decreased need to reschedule exams due to inadequate preparation among participants in the IG (p = .005). The literature also reveals that there are additional benefits to improved educational strategies, including lower patient anxiety, better tolerance to medication and diet (Lee et al., 2015), greater service satisfaction (Back et al., 2018; Gálvez et al., 2017) and greater availability to repeat exams when necessary (Gálvez et al., 2017).
This study’s findings should be highly relevant to the nursing profession in the context of endoscopy. Specifically, it was determined that the telephone is an accessible, inexpensive, and widely available resource that nurses can use to conduct appropriate health education prior to colonoscopy, thus contributing to improved bowel preparation. This is significant because colonoscopies are invasive and costly but essential for diagnosing numerous diseases.
Finally, although bowel preparation was better, there were no differences in adenoma detection in the groups. Regarding this, we suggest further studies should be conducted with a different research design. Therefore, it will be possible to verify whether the telephone can indeed be a useful tool used by a nurse for patient education. It is recommended that the research be repeated with other outcomes to consider, such as pre versus procedural anxiety or discomfort, which would be significant in the context of the nursing process in endoscopy assistance.
This study had some limitations. Although the BBPS was developed to limit interobserver variability when classifying bowel preparation quality and is used in the context of both care and research in several countries (Kastenberg et al., 2018), grading can vary depending on the unique experiences of the administering physicians, even when they correctly follow protocol. However, a previous study found that objective and automated bowel cleansing assessments would help reduce these inequalities (Hernández et al., 2019), meaning that future research should investigate the optimization of relevant medical resources. Additionally, this study did not control for waiting time intervals between scheduling and preparation instructions for routine colonoscopies or for procedural conduct, both of which require future investigation.
Conclusion
Nurse-led educational interventions via telephone effectively reorients patients about bowel preparation prior to colonoscopy. In addition to current educational practices, this constitutes an effective strategy that nurses can incorporate into care provisions for patients requiring the procedure.
Practice Implications
This study resulted in vital practical implications for the nursing field, most particularly in reducing costs while ensuring better quality of care and decreasing instances of colonoscopy rescheduling based on patient reeducation during gaps between scheduling and examination days.
Research Data
sj-pdf-1-cnr-10.1177_1054773821995015 – Supplemental material for Telephonic Nurse Guidance for Colonoscopy: A Clinical Trial
sj-pdf-1-cnr-10.1177_1054773821995015 for Telephonic Nurse Guidance for Colonoscopy: A Clinical Trial by Tatiane Santa Rosa Diniz, Suzimar de Fátima Benato Fusco, Maria Elizandre Camilo de Oliveira, Hélio Rubens de Carvalho Nunes and Marla Andréia Garcia de Avila in Clinical Nursing Research
Footnotes
Acknowledgements
TIKINET and Editage by translation
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior e Conselho Federal de Enfermagem – Project CAPES/COFEN.
Author Biographies
References
{kind=link}
{kind=link}
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.