
Abstract
Many Zimbabwean immigrants have settled in the US in the past 20 years. These immigrants originate from a country highly burdened with HIV and other non-communicable diseases. The health needs of these immigrants are not known. To determine the prevalence of health conditions, and healthcare utilization of Zimbabwean immigrants. A cross-sectional study of 98 Zimbabwean immigrants recruited at religious festivals, completed questionnaires and had blood pressure and weight measurements taken. Three quarters (74.4%) were overweight/obese, 34.7% had hypertension, 79.6% were health insured, 87% had regular PCPs. In the year prior 78.7% had seen a provider, and 25% had utilized the ER for care. Despite regular visits to providers participants, Zimbabwean immigrants utilized the ER more frequently than other populations and had high prevalence of preventable cardiovascular disease risk factors. Providers need to partner with this population to come up culturally appropriate prevention and management interventions.
Immigrants to the United States originating from sub-Saharan Africa (SSA) are a small but growing population. The SSA immigrant population increased from 574,000 in 2000 to more than 2 million in 2018, corresponding to a three-fold increase over an 18-year period (Echeverria-Estrada & Batalova, 2019). It is noteworthy that immigrants from SSA originate from a region with a high burden of both communicable and non-communicable diseases (NCDs). The World Health Organization (WHO) raised a concern over an increase in NCDs in Africa, with CVDs causing higher mortality in Africa than in developed countries (World Health organization [WHO], 2015).
The literature shows that health-related studies in this immigrant population tend to be focused on immigrants from regions with larger populations in the US such as West Africa (Blanas et al. 2015; Commodore-Mensah et al., 2016; Kaplan et al., 2015; Turk et al., 2015) and East Africa (Carroll et al., 2007; Chaumba, 2011; Devlin et al., 2012; Mohamed et al., 2014; Raymond et al., 2014). To our knowledge, and based on extensive literature searches, the state of health of Southern African immigrants in the US is not known, despite that they originate from countries with high burdens of both communicable (UNAIDS, 2019) and non-communicable diseases (NCDs) (WHO, 2016). Over the past twenty years, many Zimbabwean immigrants settled in the US fleeing political, social, and financial instability (Nkala et al., 2014). These Zimbabwean immigrants come from a country with one of the highest prevalence of HIV in the world (UNAIDS, 2019) as well as high prevalence of NCDs including diabetes, hypertension, and obesity/overweight. (WHO, 2016). Not much is known about health needs of this vulnerable population after they settle in US. An extensive literature review in CIHNAL, Pubmed, Ovid, and Google scholar did not yield any published studies on the state of health among Zimbabwean immigrants. Anecdotal evidence on social media (WhatsApp group chats and Twitter feeds) among Zimbabwean immigrants quite frequently announce deaths from stroke, heart attack, cancer, diabetes complications, and suicide. As more Zimbabwean immigrants migrate and become US permanent residents and citizens, there is a need to understand their health needs. Understanding the health needs is crucial in the development and implementation of culturally appropriate disease prevention and management measures. Therefore, the purpose of this pilot needs assessment was to determine the prevalence of self-reported diagnosed health conditions, determine prevalence of overweight and obesity, inactivity and health utilization patterns of Zimbabwean immigrants in the US.
Methods
Design and Setting
We conducted a community-based cross-sectional needs assessment study of Zimbabwean immigrants between June 2015 and September 201 using a convenience sample of volunteers.
Sample and Recruitment
Participants were recruited at four annual regional interdenominational church conventions (Boston, MA; Chicago, IL; Philadelphia, PA; and Orlando, FL), attended by immigrants from Zimbabwe. Such religious conventions serve as religious and networking events for many Zimbabwean immigrants in the US. The research team was granted permission to take the podium to announce the on-location health fair, goals, and purpose of the needs assessment study. Attendees were invited to participate in the health fair staged at a booth erected in the convention hall. A pamphlet describing the study was included in the convention registration packet. To be eligible to participate, the participant had to be born in Zimbabwe, between 18 and 80 years of age, had lived in the US for at least 12 months, and be able to speak, read, and write English fluently. Individuals not meeting these criteria were excluded.
Data collection and measures
Individuals who were interested in the study visited the health booth and were provided the study purpose and could ask any questions about the study. Written informed consent was obtained. Data was collected using a self-administered survey questionnaire written in English at eighth grade reading level. Approximately 30 minutes was required to complete the questionnaire.
The survey questionnaire was adapted from the validated National Health Information Survey questionnaire (NHIS) (National Center for Health Statistics, 2015a); the Behavioral Risk Factor Surveillance System (BRFSS) (Centers for Disease Control [CDC], 2015); and National Health Center for Health Statistics, 2015b); and. NHIS is the principal source of information on the health of the civilian non-institutionalized US population and is one of the major data collection programs of the National Center for Health Statistics, an arm of the Centers for Disease Control and Prevention. The BRFSS is an annual surveillance system designed to measure the behavioral risk factors for non-institutionalized US adults conducted by CDC’s Population Health Surveillance Branch (Centers for Disease Control [CDC], 2016).
The Global Physical Activity Questionnaire (GPAQ) (Armstrong & Bull, 2006) a WHO/CDC validated tool was used to assess energy expenditure. The tool has 16 questions focusing on physical activity participation at work, travelling, during recreational activities, and sedentary behavior. The tool measures moderate and vigorous physical activity (MVPA). GPAQ is used in over 50 countries and has been validated for use in several diverse populations (Cleland et al., 2014; Wanner et al., 2017). Blood pressure (BP) was measured using the Omron 6 monitor (Omran Healthcare) with the patient sitting on a reclining chair per published guidelines (Chobanian et al., 2003). Body weight was measured using a digital home bathroom scale (Yorkin et al., 2013), participants self-reported their height. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared (kg/m2).
Permission to use the BRFSS and NHIS items was obtained from the CDC. While the GPAQ was freely available on the internet. The designed study questionnaire was pilot-tested on a few individuals from the community. Their suggested edits and comments were incorporated into the final version.
Ethical Considerations
No personal identifying information was recorded. Study participants placed the completed surveys in a sealed collection box. At completion, study participants were given small gifts such as pens, lunch boxes, or $5 AT&T calling cards as appreciation for their participation. The study protocol was approved by the relevant Human Subjects Review Board.
Statistical Analysis
BMI was categorized as <25 (normal), 25 to <30 (overweight), and 30 or more kg/m2 (obesity). Age and duration of stay in the US on the date of the survey were calculated. Age was categorized into <40, 40 to <50, and 50 years or older categories. Duration in the US was coded as <5 years and >=5 years. Blood pressures were coded into AHA/ACC categories: <135, 135 to <140, 140 to <150 and 150 mm/Hg and higher for SBP, and <80, 80 to <90, 90 mm/Hg and higher for DBP (Chobanian et al., 2003). Total household annual income, employment status, marital status, educational attainment, medical insurance, and health utilization variables were recorded on the survey questionnaire. Prior to statistical analysis data was checked for consistency and to flag and correct implausible values. Descriptive statistics were computed using mean ± standard deviation (SD) for continuous/quantitative measures, and frequencies and percentages for qualitative variables. The prevalence of self-reported conditions (high BP/hypertension, heart disease and diabetes, high BMI) was computed for the whole sample and stratified by sex.
A two-sample t-test was used to compare quantitative measures between binary groups. Two-way contingency tables were used to compare proportions and prevalence between groups. The chi-squared test, or Fisher’s exact test where indicated, were used to assess statistical differences between groups. A p-value <.05 was used to indicate statistical difference.
Results
Our final sample size of 98 produces a two-sided 95% confidence interval with a width equal to 0.167, 0.189, 0.202 when the sample prevalence is 0.20, 0.30, and 0.40. Therefore, we had capacity to estimate a range of prevalence of CVD risk factors with good precision. (Newcombe, 1998).
Sample Characteristics
A total of 98 (75 women; mean (SD) age, 47.5 (11.1) years) participants completed the study. Fifty-eight, (59.8%) were in the 40 to <55 years age group, 62 (64.6%) were married or cohabiting, 78 (79.6%) had been in the US longer than 5 years, 57.7% had a graduate degree. Seventy-five participants, (76.5%) worked full time while 23 (25.3%) had total annual household income exceeding $100,000. Seventy-eight (79.6%) had health insurance, most of which was private insurance (Table 1).
Demographics Characteristics Overall and Stratified by Sex.
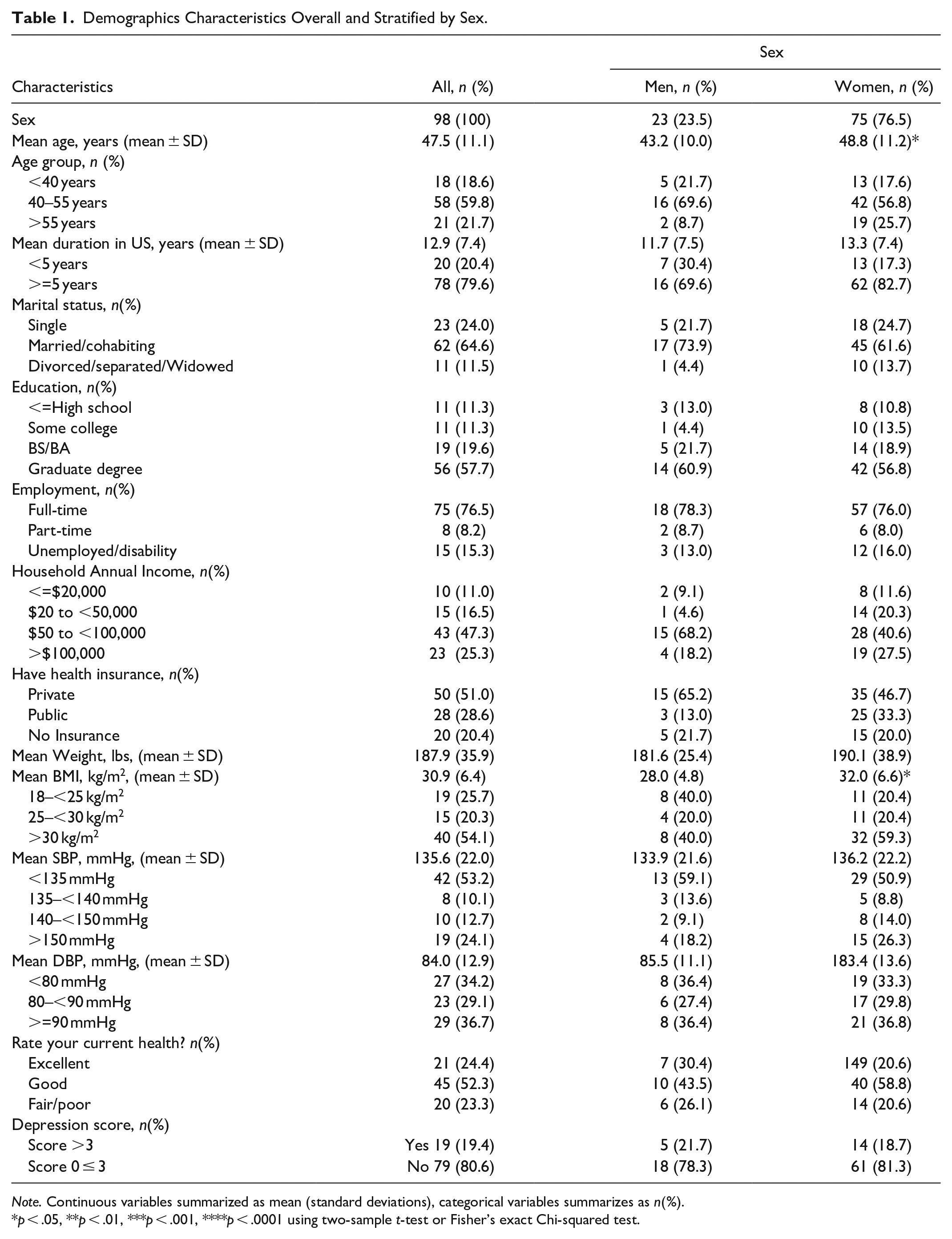
Note. Continuous variables summarized as mean (standard deviations), categorical variables summarizes as n(%).
p < .05, **p < .01, ***p < .001, ****p < .0001 using two-sample t-test or Fisher’s exact Chi-squared test.
Weight, BMI, and Blood Pressure Measurements
The mean weight was 187.9 lbs. (95% CI: 180.8–195.0), 54.1% were obese, while 20.3% were overweight. Of the participants whose BP was measured, 19 (36.8%) had Systolic BP > 140 mmHg; 29 (36.7%) had diastolic BP >90 mm/Hg.
Men were significantly younger than women by 5.6 years (43.2 (10.0) vs. 48.8(11.2) years, p < .05). Men also had lower BMI than women (28.0 (4.8) vs. 32.0 (6.6), p < .05). There was a statistically significantly greater proportion of individuals >40 years with SBP >150 mm/Hg (30.2% vs. 0.0%, p < .01) and DBP >90 mm/Hg (42.9% vs. 12.5%, p < .05) (Table 1).
Prevalent Diagnoses
The prevalence of hypertension was 34.7% (95% CI: 25.2–44.3), diabetes 8.6% (2.5–14.8), heart disease 5.8% (0.9–10.8). Nearly one in five reported having been told that they had elevated cholesterol, 19.8% (11.8–27.8). Of the 32 participants who answered the hypertension-related questions, greater than half, 52.5% (39.9–65.0) reported taking anti-hypertensive medication; two-thirds, 66.7% (55.0–78.3) had ever been told to reduce salt intake, and having been told to lose weight through dieting, 50.0% (37.9–62.1) (Table 2).
Prevalence of Cardiovascular Conditions and Cardio-Metabolic Risk Factors Overall and Stratified by Sex.
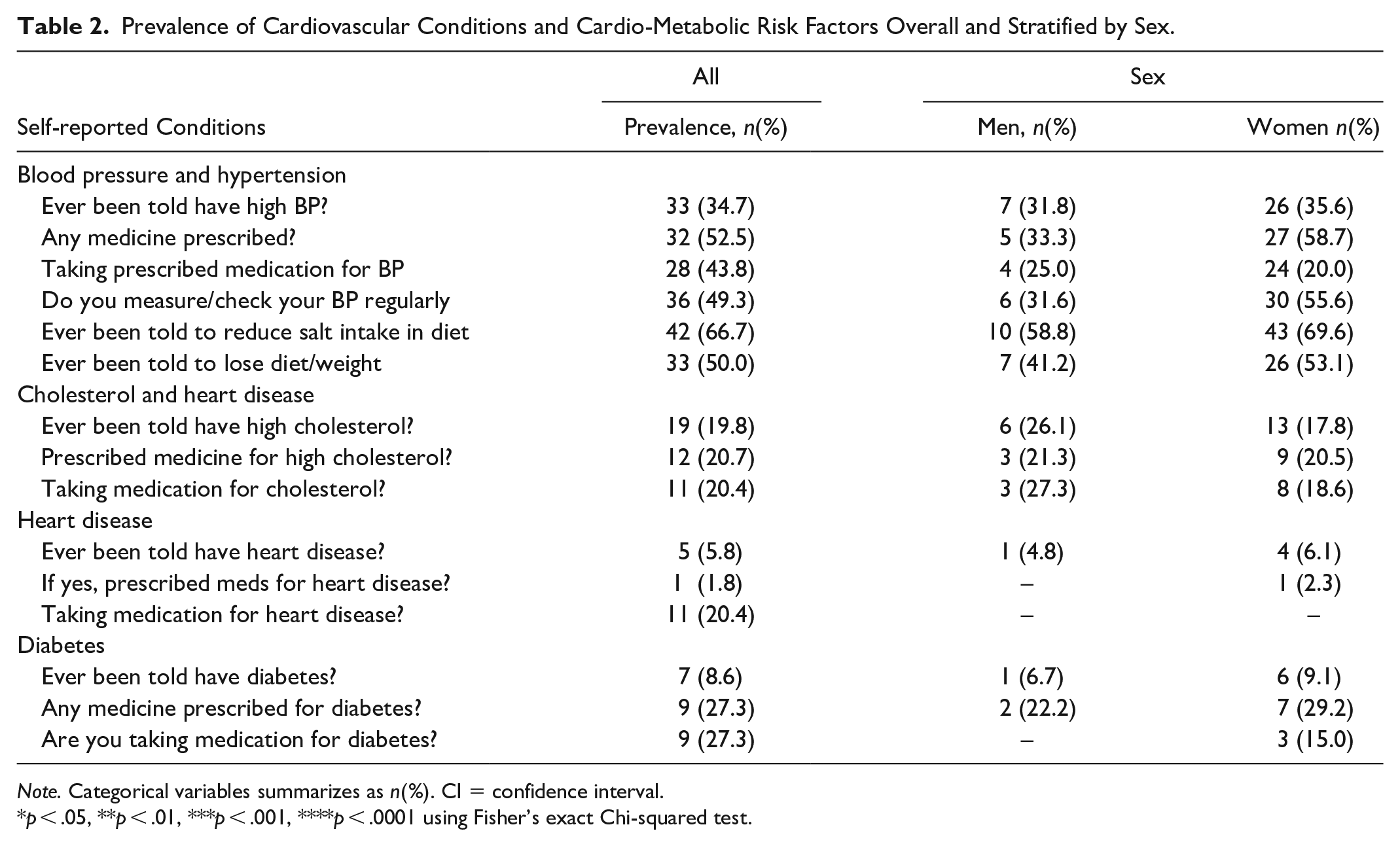
Note. Categorical variables summarizes as n(%). CI = confidence interval.
p < .05, **p < .01, ***p < .001, ****p < .0001 using Fisher’s exact Chi-squared test.
Health Care Utilization
The proportion of participants with medical insurance was 79.6% (72.1.6–87.6). Similarly, high were the proportions with a regular PCP in the previous 12 months, 78.7% (69.4–87.9), and had seen healthcare provider in previous 12 months, 87.6% (80.0–93.5). Thirty-three participants had been to the ER in the previous 12 months, 13 of these visits resulted in hospitalization (Table 3). A greater percentage of men than women (91.9% vs. 73.9%, p < .05) had seen a provider in the previous 12 months (Table 3). Participants who had been in the US for at least 5 years were more likely to have medical insurance (88.5% vs. 45.0%), more likely to have a regular PCP (96.1% vs. 55.0%, p < .001), and more likely to have seen a healthcare provider in the previous 12 months (93.5% vs. 65.0%, p < .01). Participants with health insurance were statistically significantly more likely to have a PCP whom they have seem in the previous 12 months. (subgroup analysis data not shown).
Healthcare Utilization Overall and Stratified by Sex.
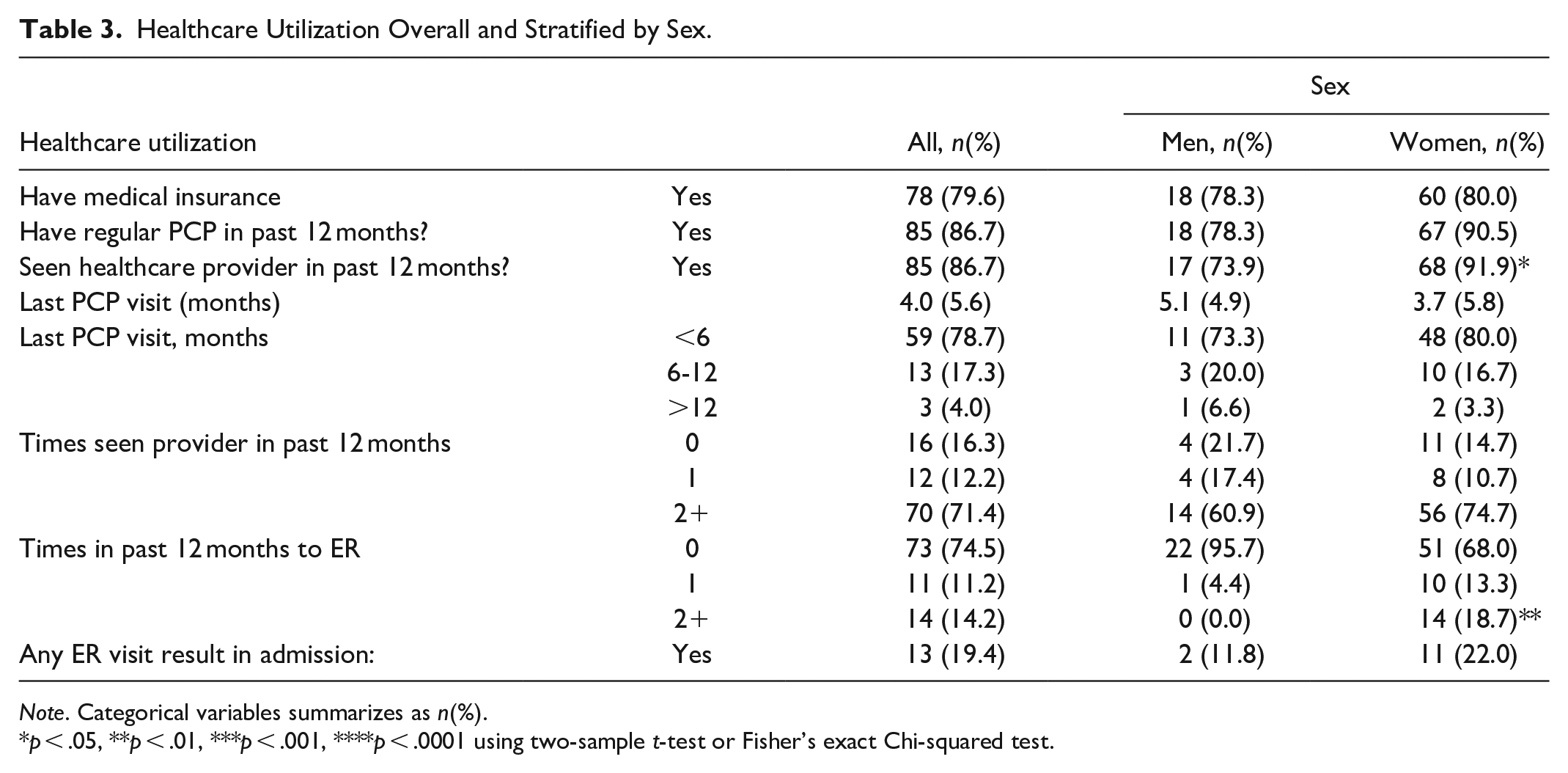
Note. Categorical variables summarizes as n(%).
p < .05, **p < .01, ***p < .001, ****p < .0001 using two-sample t-test or Fisher’s exact Chi-squared test.
Discussion
We conducted a needs assessment among Zimbabwean immigrants in the US. We examined the self-reported prevalence of diagnoses, health care utilization, weight, blood pressure Hypertension was the most commonly diagnosed condition. A significant majority of the participants were either obese or overweight. Most participants were medically insured and had visited their PCPs regularly. Despite visiting PCPs regularly, a significant minority reported receiving care at the ER.
Uncontrolled hypertension is a known preventable major cause of cardiovascular disease (Santos & Dhamoon, 2020; Whelton et al., 2017). Untreated or treated but uncontrolled hypertension in adults increases the risk for all cause and CVD mortality while effectively treated hypertension levels CVD risk to that of normotensive people (Zhou et al., 2018). The high prevalence of hypertension at 34.7% is higher than that the 30.0% in Zimbabwe, (Mutowo et al., 2015), and also higher than that from a meta-analysis of data from 90 countries (Mills et al., 2016), and other black immigrant populations (Brown et al., 2017; Turkson-Ocran et al., 2020). The longer the participants in our study had been in the US, the more likely they were to be diagnosed with hypertension. This finding is different from that reported by Brown et al. (2017) in which the length of stay in the US had no association with getting diagnosed with hypertension. Not only did the participants in our study have higher prevalence of diagnosed hypertension; participants with no health insurance, typically, had SBP and DBP classified in the Stage 1 hypertension; putting them at increased risk for CVD (Whelton et al., 2017; Zhou et al., 2018). A majority of participants with diagnosed hypertension reported taking medications as prescribed by their provider and yet, counterfactually, the mean systolic and diastolic BP were higher than ideal, indicating prevalence of uncontrolled hypertension.
A substantial majority had health insurance and had access to providers and followed the health instructions they were given. Despite significant number of visits to their PCPs and receiving instructions on managing their chronic conditions including hypertension, there was an increased use of the ER to get care. Our participants’ ER usage was higher than that of the general population (Sun et al., 2018) and that other immigrant populations (Tarraf et al., 2014). The high utilization of health resources, including the ER, did not necessarily translate to optimal health care. For example, for every five participants, two had at least two or more risk factors for CVD. The high usage of the ER might indicate participants substitute routine care with ER visits. If this is the case, then this population might be missing out on important preventive services patients receive in routine healthcare visits with their regular PCP. In a study based on 4 million US children and adolescents enrolled in Medicaid Burns et al. (2020) found that individuals who get care via urgent care centers or emergency department as opposed to PCPs may be missing out on important prevention services.
The high prevalence of obesity and overweight is a cause for concern since these conditions are closely associated with increased risk for CVD. A typical woman in our sample had a BMI of 32 kg/m2, a level classified as obese by both the World Health Organization [WHO] (1995) and the NHLBI Obesity Education Initiative Expert Panel on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults (1998), while the typical man had a BMI of 28 kg/m2, which is classified as overweight (National Heart, Lung, Blood Institute, National Institute of Diabetes, Digestive, Kidney Disease, 1998; WHO, 1995). The prevalence of obesity/overweight of 74.4% observed in our study is higher than the prevalence observed in the study by Turkson-Ocran et al. (2020) which reported 61% prevalence in African immigrants compared to 70% in African Americans.
Similar to other studies in Africans around the world, immigrant women from Zimbabwe had a higher prevalence of obesity than their male counterparts. This pattern concurs with findings by Commodore-Mensah and colleagues who reported higher prevalence of obesity/overweight among in West African immigrant women (Commodore-Mensah et al., 2016). Our study findings are also consistent with the trend of overweight and obesity in Zimbabwe where obesity rates have increased by nearly 12 percentage points from 25.0% in 2005 to 36.6% in 2015 (Mukora-Mutseyekwa et al., 2019). In Zimbabwe where our study sample came from, an increasingly westernized diet consisting of large portions high in fats have been implicated in the increased prevalence of obesity/overweight states (Mangemba & San Sebastian, 2020). If Zimbabwean immigrants have continued with the westernized diet this might explain the high burden of obesity and overweight. The high burden of obesity/overweight states could also be explained by the low response rates on the physical activity questionnaire of our study. The lack of response could also be due to low levels of physical activity in the population. Other studies (Ilunga-Tshiswaka et al., 2018; Mohamed et al., 2014; Terasaki et al., 2017) reported that African immigrants were likely to be physically inactive as they tended to walk less and were embarrassed to exercise in public.
Relative to findings from other African immigrants, participants in our sample had higher prevalence of diagnosed diabetes (7.0% vs. 8.6%) and higher prevalence of hypercholesterolemia (4.0% vs. 19.8%). African Americans, on the other hand, had diabetes prevalence of 10.0%, and 5.0% hypercholesterolemia (Turkson-Ocran et al., 2020). The high burden of diabetes in the African immigrant population has been associated with acculturation (Mukaz et al., 2020). With high prevalence of overweight and obesity, diagnosed undertreated hypertension, and possible physical inactivity, the risk for CVD in this population is disproportionately high. Of note, these CVD risk factors are highly preventable. The fact that this highly educated, high income population where most participants reported having health insurance, regular primary care providers, and had seen a provider within the past year, and have high prevalence of CVD risk factors, utilized the ED more than other African immigrants is a major cause for concern. This alludes to a state of higher disease burden, requiring special attention from providers and researchers.
Limitations
Our study has some limitations. We conducted a cross-sectional study using convenience sampling. The estimates derived from convenience samples are often biased because the sample poorly represents the target population. Our sample had more women than men. This was because women tend to participate in religious conventions more than men. Views expressed by religious men and women are not necessarily representative of all Zimbabwe-born immigrants. Another limitation is that participants in our study might have underreported perceived vices such as smoking cigarettes and drinking alcohol as these behaviors are socially undesirable within their church groups. Our reliance on self-reports of current diagnoses and behaviors is also a potential weakness. Self-reports can be biased as they can be affected by recall and social desirability of responses (van de Mortel, 2009). We did not have the means to verify the veracity of the responses given by participants on the questionnaires. For example, we took it at face value that the self-reported cardiovascular diagnoses were accurate. Besides these limitations, we managed to successfully penetrate and study the health status of a hard-to-get population of immigrants.
Application
We were able to access a highly educated population with high utilization of healthcare as well as a high burden for CVD risk factors. Our findings revealed some contradictions, that is, participants reported being regularly connected to their PCPs, yet they had a high burden of uncontrolled BP, were mostly overweight or obese and utilized ERs more frequently than other immigrant populations. There seemed to be a disconnect between these participants and their healthcare providers. For providers working with this population, seeing the patients regularly, writing prescriptions, and providing health education is not adequate. It appears that healthcare access for this population might not be the issue, alluding to the inadequacy of the interaction between the provider and the patient. Providers need to “know” their patients so they can build meaningful relationships they can use to follow through with care and preventive measures.
Our study findings highlight the inadequacy of the care these immigrants receive. Follow up studies to interrogate some of the reasons for poor outcomes are needed. The data from the follow up studies will be essential in the development of targeted culturally appropriate health interventions to improve health by reducing the risk for CVD through behavior modification, disease screening and management.
Footnotes
Acknowledgements
Dr. Inge Corless who reviewed and edited the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.