
Abstract
To explore the association between frailty and self-care in older adults with congestive heart failure and analyze their influencing factors. The cross-sectional study was conducted at the department of cardiology of a hospital in China from March 2018 to November 2018. A total of 165 participants were recruited. Frailty and self-care were measured by the Tilburg Frailty Indicator, and the Self-care of Heart Failure Index (V6). The physical, psychological, and social frailty exerted a significant negative association with self-care. Exercise, income, comorbidities, and times of congestive heart failure-related hospitalizations were independent risk factors for frailty; surgical treatment, comorbidities, and income were independent risk factors for self-care. These findings help to fill the need for new approaches to identify the high risk of frailty individuals in the acute care setting for targeted intervention and tailored transitions in care to promote optimal patient quality care and biopsychosocial well-being.
Introduction
Congestive heart failure (CHF) has become a primary and growing global public health issue as its incidence and prevalence increase significantly with age (Dharmarajan & Rich, 2017; Snipelisky et al., 2019). The prevalence of CHF is about 1.5% to 2.0%, and it may reach 6% to 10% among people over 65 years old (Roger, 2013), which makes CHF the most common cause of hospitalization in older adults (Benjamin et al., 2018). It constitutes unprecedented cost burdens to the healthcare system due to its high treatment costs combined with an unfavorable prognosis (Dharmarajan & Rich, 2017; Snipelisky et al., 2019).
Frailty is common in older adults with CHF and its prevalence is also strongly correlated with age (Hoogendijk et al., 2019). Frailty is the result of the decline in function and reserve of physical, psychological, and social systems, which increases vulnerability and sensitivity to adverse outcomes such as falls, disability, decreased mobility, frequent hospitalizations, and delirium (Chen et al., 2014; Clegg et al., 2013; Eeles et al., 2012; Gobbens et al., 2012; Pandey et al., 2019). A systematic review of community-dwelling older people in China showed that the potential risk factors correlated with frailty included increasing age, female sex, three or more chronic diseases, and activities of daily living disability (He et al., 2019). Frailty commonly coexists with CHF, which may be caused by the similar pathogenesis of frailty and CHF (Marengoni et al., 2020). Chronic inflammation may be the core pathophysiological basis of frailty and CHF. The underlying processes of frailty and CHF may perturb homeostasis, leading to low levels of chronic inflammation (Bellumkonda et al., 2017).
Background
The incidence of frailty in patients with CHF is approximately 15% to 74% (McDonagh et al., 2018). Meanwhile, frailty and CHF are both associated with worse clinical and patient-reported outcomes (Pandey et al., 2019). Frailty is also an independent predictor of a worse prognosis in people with CHF and increases CHF-related hospitalization rates and all-cause mortality (Cheng et al., 2017; Davis et al., 2021; Uchmanowicz et al., 2020). It has even been hypothesized that undiagnosed cases of CHF in older persons may be discovered by frailty assessment (Fung et al., 2018). Therefore, it is essential to identify the high-risk groups of frailty in CHF.
Self-care is considered essential to improve the prognosis of CHF (Kessing et al., 2019). Behaviors related to CHF self-care include symptom monitoring and management, medication administration, fluid intake management, exercise, dietary choices, and behaviors requiring lifestyle changes (Riegel et al., 2011). These are effective means to control and reduce the recurrence and deterioration associated with CHF (Toback & Clark, 2017). Adequate self-care behavior can not only reduce the readmission rate and emergency admission rate but also be a protective factor for the quality of life in people with CHF (Auld et al., 2018; Jones et al., 2012; Kessing et al., 2017), which may ultimately reduce all-cause mortality related to CHF (Lee et al., 2011). However, the self-care behavior of patients is inadequate and it gradually decreases after leaving the hospital (Seid et al., 2019). A study has revealed that only 22.3% of patients (310 participants) reported that they followed self-care recommendations with good adherence (Seid et al., 2019). Failure to achieve optimal compliance with self-care behavior may limit its effectiveness (Jones et al., 2012).
Studies have shown that frailty affects the self-care ability of community-dwelling older adults. Cramm et al. (2014) found that older adults with poor self-management ability had higher scores of physical frailty. A 2-year longitudinal study reported that strengthening self-care agency, self-management skills, and regular exercise for chronic illness may slow down the frailty progress among older adults (Tanimura et al., 2018). Therefore, we expect to explore the relationship between frailty and self-care ability in older adults with CHF in this study.
To date, a few studies have focused on the association between frailty and self-care in CHF, however, these available findings are mixed and inconsistent. Frailty syndrome and its various components (physical, psychological, and social) were differentially associated with individual self-care behaviors among people with CHF by combining these findings (Mlynarska et al., 2018; Uchmanowicz et al., 2015). Meanwhile, few studies have been found to clarify the relationship between self-care and frailty in CHF, especially in China. Moreover, it is of great clinical significance to explore the influencing factors that can be altered by interventions aiming to improve frailty or self-care behavior. Based on the above argument, the objectives of this study were to explore the association between frailty and self-care behavior and analyze influencing factors of frailty and self-care behavior in older people with CHF in China as a supplement and extension to existing research.
Methods
Design and Participants
The current study employed a hospital-based, descriptive and cross-sectional study design. A convenience sample of older adults was recruited from March 2018 to November 2018 in the department of cardiology of a hospital in China. Patients were incorporated in the study based on the following inclusion criteria: (a) age ≥60 years old (WHO, 2021); (b) diagnosed with CHF by a cardiologist through the New York Heart Association (NYHA) criteria, echocardiograph, and signs and symptoms of CHF. The population of people over 60 years old in China is considered to be older adults. The exclusion criteria were as follows: (a) identified by clinical experts as disturbance of body movement; (b) unconsciousness; and (c) cognitive impairment with no more than 17 points screened by the Mini-Mental State Exam (MMSE) scale.
The sample size required for this study was calculated according to the rule of thumb recommended by Austin and Steyerberg (2015), which implies that per category of predictor variables requires at least 10 observations. Fifteen predictors (socio-demographic and disease characteristics, frailty, and self-care) were measured in this study. Withdrawal and non-participation were allowed during the data collection period. It was estimated that the number of unqualified samples is 10%. A total of 165 participants who met the criteria were eventually approached to participate.
The survey was completed anonymously. After giving the participant a brief explanation of the study and obtaining the informed consent statement, two researchers collected the socio-demographic and disease characteristics data and the frailty and assessed the self-care behavior of patients within 3 days of admission. Participants were allowed to drop out and their privacy was protected during the data collection process. The collected data was collated and statistically analyzed by the other researchers.
The study was approved by the Institutional Review Board of the School of Nursing, Jilin University (HREC2018022601). The reporting guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology were followed (von Elm et al., 2007).
Measurement
Socio-demographic and disease characteristics
Socio-demographic data (sex, age, occupation, civil status, education level, living situation, income, exercise) were obtained through interviews with patients. Basic information on the disease was obtained by asking patients and doctors and checking medical records, such as admission mode, times of CHF-related hospitalizations in the last year, duration of CHF, NYHA, types of comorbidities, severity of comorbidities, CHF medications regularly before admission, types of surgical treatment.
Frailty
The Tilburg Frailty Indicator (TFI) scale is a standardized self-report questionnaire and is compiled based on the definition of frailty (Gobbens et al., 2012). It takes a short time to measure in the clinical setting and covers many domains of frailty assessment (physical, psychological, and social), which is suitable for measuring the frailty of patients with CHF in this study. The scale consists of 15 items, of which 11 items use a two-category scoring method (“yes”/“no”), and the remaining items use a three-category scoring method (“yes”/“no”/“sometimes”). “Yes”/“sometimes” answers are given a score of 1 point, while “no” answers are given a score of 0 points. The higher score indicated the more severe frailty of participants. The maximum points from the TFI scale are 15 and the minimum is 0 points (Gobbens et al., 2010). A previous study has shown good internal consistency reliability (Cronbach’s α = .71) and strong test-good retest reliability (r = .88) indices for the Chinese version of the TFI in measuring frailty (Dong et al., 2017).
Self-care
The Self-care of Heart Failure Index (SCHFI) (V6) was adopted to assess the self-care behaviors of participants. Three subscales, self-care maintenance (10 items), self-care management (6 items), and self-care confidence (6 items), are included in the SCHFI (Riegel et al., 2004). These subscales, whose items include 4-response options (1–4 points) and 5-response options (1–5 points), can be used separately. The higher score indicated the more adequate self-care behavior. The score of each subscale can be converted into a standardized score from 0 to100, and ≥ 70 points indicate adequate self-care behavior. Kang et al. (2015) have indicated that the internal consistency for the Chinese version of the three subscales of SCHFI is adequate (self-care maintenance, Cronbach’s α = .66; self-care management, Cronbach’s α = .74; and self-care self-confidence, Cronbach’s α = .87), and the construct validity is supported (Kaiser-Meyer-Olkin = .811; Bartlett test of sphericity, χ2 = 1613.130, df = 231, p < .001).
Comorbidity
Comorbidities were evaluated using the Charlson Comorbidity Index (CCI). The Charlson index (1–6 points) was used to assign values to each comorbidity based on its relative risk, with a total score of 36 points (Charlson et al., 1987). The CCI has been widely used to assess the severity of CHF comorbidities. A high score represents more serious CHF (Fabbri et al., 2020). According to the index, comorbidities of CHF were divided into three different levels: mild (1–2 points), moderate (3–4 points), and severe (≥5 points). The weight value of Charlson comorbidities assignment was shown in Supplemental File S1.
Cognitive level
The MMSE scale was used to exclude CHF patients with cognitive impairment. It is composed of 19 items which measure cognitive function, including orientation, recall, calculation, language, and attention (Folstein et al., 1975). The total score ranges from 0 to 30, and a score of ≤17 was taken as the positive cut-off value for dementia screening (Li et al., 1989, 1991). And the Chinese version of the MMSE showed good validity (intraclass correlation coefficient = .998) and reliability (kappa = 0.72–1.00) indices (Li et al., 1991).
Data analyses
SPSS 23.0 (IBM Corp., Armonk, NY, USA) for Windows was applied for the statistical analysis of the data. The normality/distribution of the data was tested by the Kolmogorov-Smirnov test. Descriptive data, such as the means, standard deviations, percentages, and frequency, were calculated to describe the socio-demographic and disease characteristic variables and the scores of TFI and SCHFI for participants. The association between frailty and self-care was analyzed with Pearson correlations. The socio-demographic and disease variables affecting TFI/SCHFI scores were examined by Student’s t-test or one-way analysis of variance (ANOVA). The multiple stepwise regression analyses included the variables which were eventually identified as significant determinants of TFI/SCHFI scores on univariate analysis. p < .05 was regarded as statistically significant.
Results
Characteristics of Participants
Ten patients refused to participate, five patients withdrew, and 150 participants were eventually included for statistical analysis, with a response rate of 90.9%. The mean age was 71.03 ± 7.69 years (ranged from 60 to 87). Participants with an income of 1,001–5,000 RMB (a relatively low level of income) accounted for 69.3%. A high NYHA functional class, class Ⅲ for 41.3% of patients and class IV for 36.7%, was found in the participants. The other socio-demographic and disease characteristics of participants were shown in Table 1.
Demographic and Disease Characteristics of the Participants (N = 150).
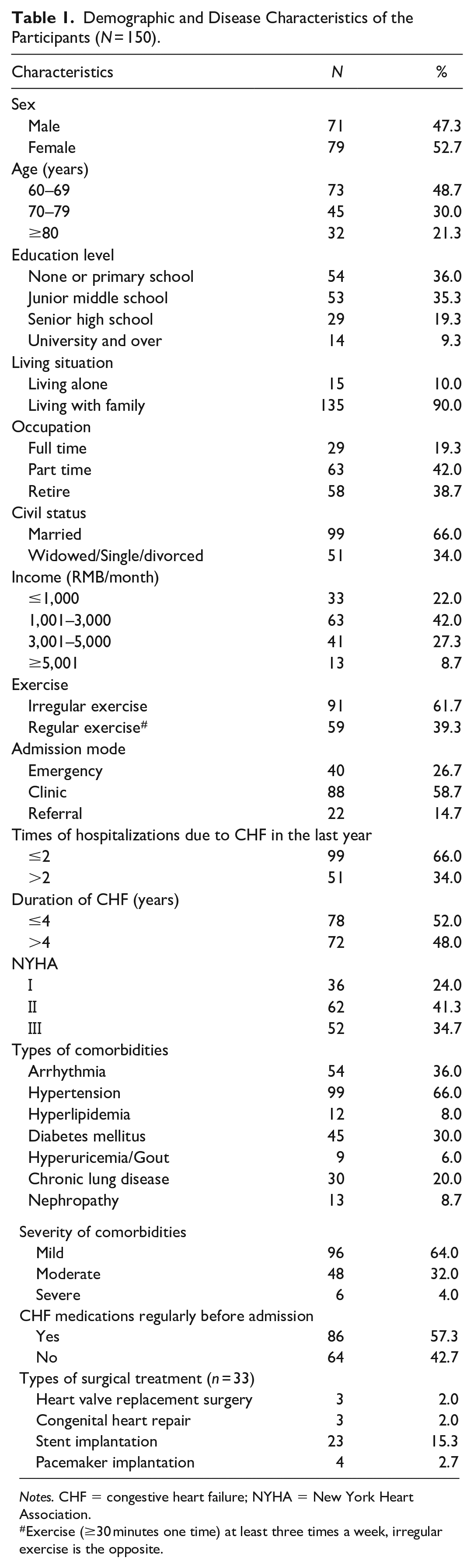
Notes. CHF = congestive heart failure; NYHA = New York Heart Association.
Exercise (≥30 minutes one time) at least three times a week, irregular exercise is the opposite.
Association Between Frailty and Self-Care Behavior
The global TFI score was 6.70 ± 2.59, the average value of physical dimensions was 3.86 ± 1.51 points, the average value of psychological dimension was 2.95 ± 1.27 points, and the average value of social dimension was 0.90 ± 0.69 points. The frailty prevalence was as high as 88% according to the critical value for the Chinese version of the TFI scale. The descriptive statistics of each item for the TFI scale was shown in Figure 1.
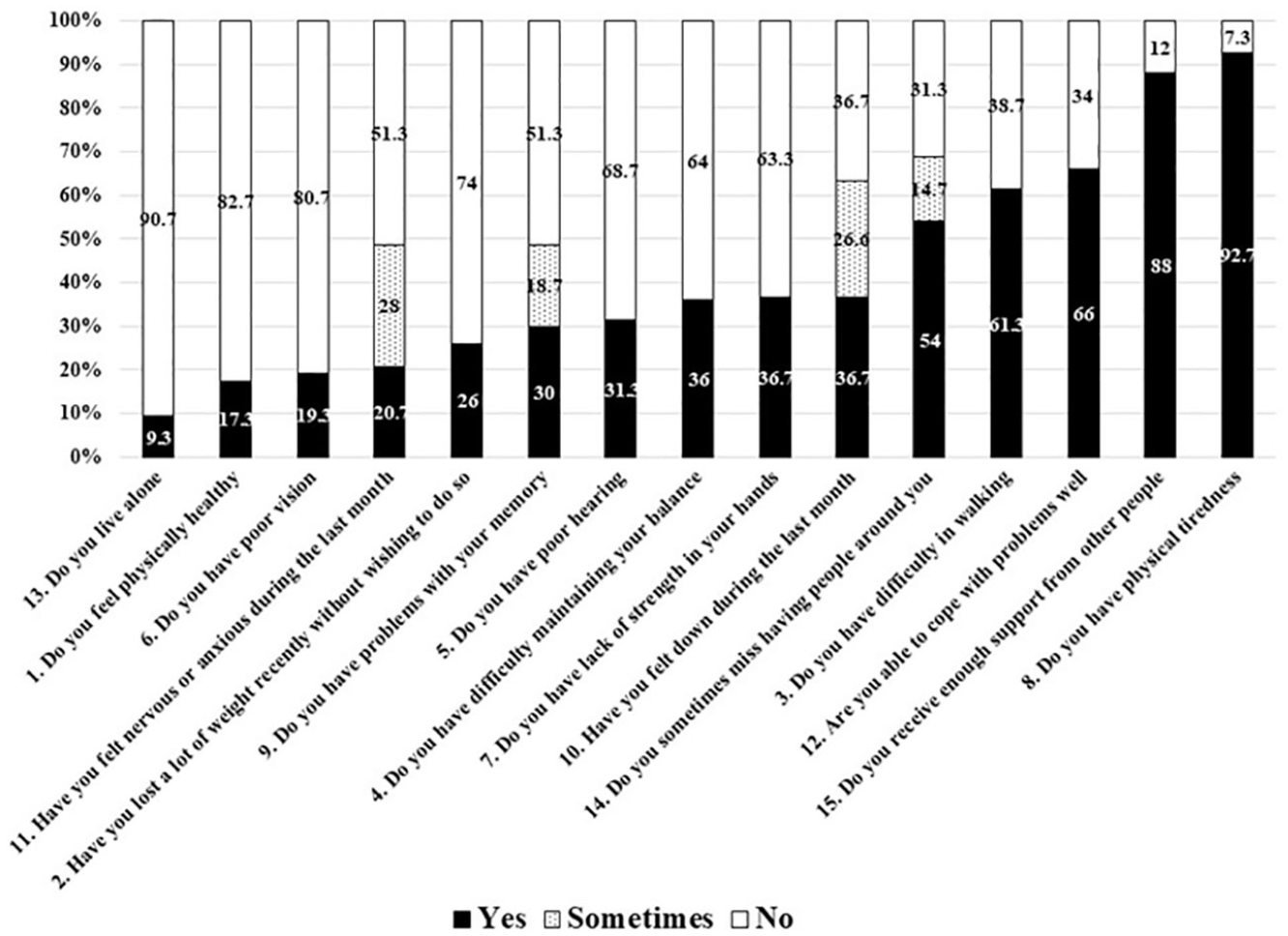
Description for the Tilburg Frailty Indicator (N = 150).
The average self-care maintenance score was 53.11 ± 20.35, and the mean self-care management score was 56.67 ± 12.69. The scores of two subscales for the SCHFI showed that 76.7% of patients scored less than 70% of the standard score for self-care maintenance, and 86% of patients scored less than 70% of the standard score for self-care management. “Exercise 30 minutes” was the lowest score of self-care maintenance behavior, and “using the effective methods patients have used” was the lowest score of self-care management behavior in the SCHFI.
The results of Pearson correlations showed that the global frailty score and each dimension score of the TFI scale were all significantly negatively associated with self-care maintenance score and self-care management score (p < .01) (Table 2).
Association Between Frailty and Self-Care Behavior (N = 150).
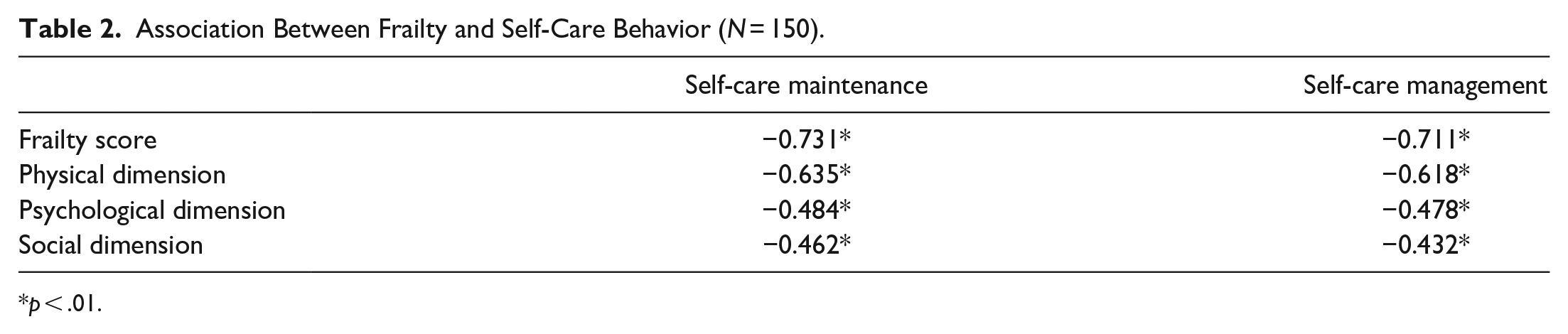
p < .01.
Multivariate Stepwise Regression Analyses of Frailty Scores and Self-Care Scores
The frailty scores were taken as the dependent variable to establish multiple regression models for analysis. The factors that had a significant impact on the frailty scores in the univariate analysis (provided in Supplemental File S2) were considered as the first level of independent variables, and self-care maintenance and self-care management were considered as the second level of independent variables. Then, multiple stepwise regression models were established and introduced into equation analysis. The results showed that four independent variables (monthly income, times of CHF-related hospitalizations in the last year, exercise, comorbidities of chronic lung disease) were included in the regression model (see Table 3). 45.4% of the total variation for the frailty can be explained by these four independent variables.
Multivariate Stepwise Regression Analyses of Frailty Scores and Self-Care Scores (N = 150).
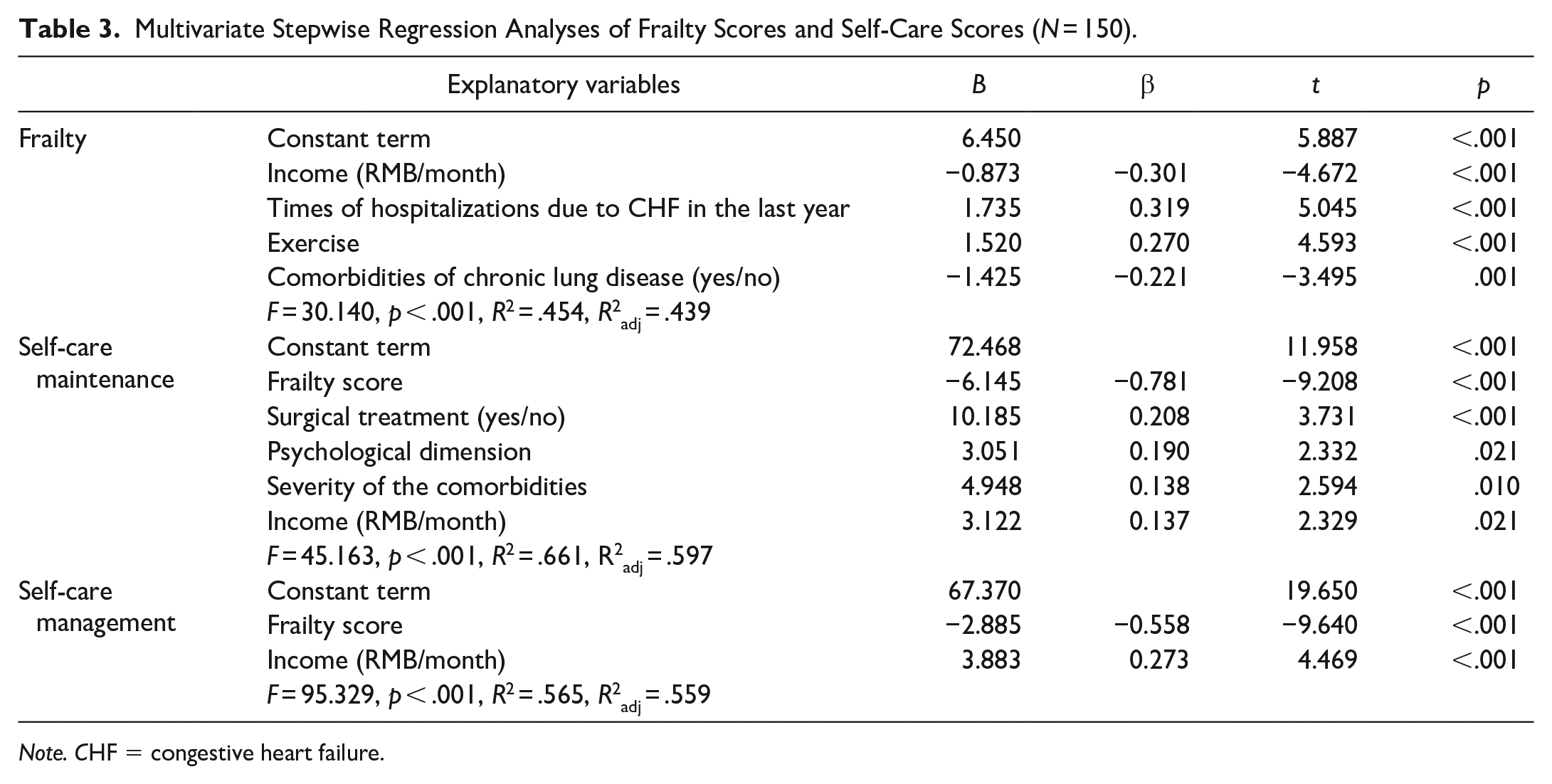
Note. CHF = congestive heart failure.
Multivariate Stepwise Regression Analyses of Self-Care Scores
The self-care maintenance/management scores were taken as the dependent variable to establish multiple regression models. The regression model controlled the variables that had significant effects on self-care maintenance/management scores in the univariate analysis (provided in Supplemental File S3), as well as the total frailty score and its three-dimensional scores. The results showed that the total frailty score, psychological frailty score, presence or absence of surgical treatment, severity of comorbidities, and income were included in the regression model on self-care maintenance. 66.1% of the total variation for self-care maintenance could be explained by these four independent variables. The total frailty score and income were included in the regression model on self-care management (see Table 3). 56.5% of the total variation for self-care management could be explained by these four independent variables.
Discussion
This study described the current level of self-care behavior and the prevalence of frailty for older adults with CHF and clearly presented significant negative associations between frailty and self-care. Moreover, this study provided insights into factors that may affect frailty and self-care behavior.
The relationship between frailty and self-care is complex. An interesting observation of our study is that each dimension of frailty has a significant impact on the patient’s self-care behavior. A previous study performed in a cardiology clinic found that only a higher score in the social dimension of the TFI scale was associated with better self-care capability (Uchmanowicz et al., 2015). Uchmanowicz et al. (2015) evaluated self-care with European Heart Failure Self-care Behavior (EHFScB) Scale in Poland and the high score of this scale represented inadequate self-care behavior. Therefore, the inconsistencies may have been caused by the different measurement scales and regional differences. The physical frailty results in a deterioration of the self-care capability. The functional limitations related to CHF (such as fatigue and memory decline) are serious obstacles to self-care for patients (Bennett et al., 1998; Kessing et al., 2016), and these physical function limitations are usually caused by frailty (Chen et al., 2014; Clegg et al., 2013). It is worth noting that the impact of psychological and social frailty on self-care ability cannot be ignored either. Patients with social and psychological frailty experience a deterioration of CHF self-care in this study. Our finding emphasizes the importance of a multidimensional assessment of frailty. Some researchers have confirmed that CHF patients with multiple psychosocial problems may be more likely than other patients to have difficulty in self-care that can increase their risk of hospitalization. This usually includes symptoms of depression, anxiety, inadequate social support, and stress (Freedland et al., 2021; Müller-Tasch et al., 2018). Among them, the influence of social support on CHF self-care maintenance and management behavior is reflected by seeking treatment for CHF symptoms and by assisting with maintaining treatment regimens (Graven & Grant, 2014).
Findings of this study indicate that income, comorbidities, the hazard of hospitalization, exercise, surgical treatment play a role in enhancing the capability of self-care and alleviating frailty. Income, as an important factor in determining the living standards of patients, has a significant impact on CHF frailty and self-care (Siriwardhana et al., 2018; Tawalbeh et al., 2017). However, a previous study showed that there was no statistical significance between frailty and income (Uchmanowicz et al., 2015). Compared with high-income countries, Siriwardhana et al. (2018) have found that the prevalence of frailty was higher in upper-middle-income countries, but the epidemiological evidence of frailty was limited in low-income and lower-middle-income countries. In this study, the participants are all from China and the low-income groups accounted for 91.3% (income ≤5,000 RMB), which may lead to the majority of patients being unable to afford the high consumption caused by repeated hospitalization and long-term medication.
Chronic lung disease comorbidities exert a certain influence on the degree of frailty and self-care ability. The presence of a variety of cardiovascular and non-cardiovascular comorbidities affects the treatment and management of CHF patients (Paolillo et al., 2020). A previous study pointed out that the risk of frailty in COPD patients was significantly higher than that in patients with other chronic diseases and was twice as high as that in people with non-COPD (Marengoni et al., 2018). Meanwhile, the severity of comorbidities can have a substantial impact on self-care maintenance in the present study. A meta-analysis also demonstrated that individuals with multiple chronic diseases are vulnerable to inadequate self-care (Dickson et al., 2011).
Similar to a previous study (Uchmanowicz et al., 2020), frailty is associated with the increase in the hazard of hospitalization across clinical contexts in CHF patients. The guidelines of CHF management indicated that exercise could improve physical function and quality of life, and decrease rehospitalization and mortality (Takano et al., 2017). The participants with exercise (≥30 minutes one time) at least three times a week show a low prevalence of frailty in our findings.
Self-care may be affected by surgical treatment among older adults with CHF. The patients with CHF who underwent surgery had better self-care maintenance than those who did not undergo surgery in our study. Mlynarska et al. (2018) reported that patients with CHF who received conservative treatment had inadequate self-care behavior than those who underwent cardiac resynchronization therapy.
From a clinical standpoint, identifying the factors influencing frailty and self-care is necessary to promote HF management. The attention of these influencing factors can enable healthcare providers to employ targeted intervention and education programs to slow down the frailty and improve clinical outcomes. For example, healthcare professionals should question CHF individuals at each medical treatment appointment regarding the presence of social support sources. These sources may be from spouses, family members, significant others, and can be able to assist patients to carry out daily activities related to self-care maintenance and management. The identified social support sources of patients should be considered in constructing the multidisciplinary self-care interventions to promote the psychological and social support of patients. Meanwhile, reasonable, inexpensive, and effective interventions should be provided to alleviate the economic burden of lower-income CHF patients based on the patients’ financial affordability. It can further improve heart function by guiding patients to develop good living habits and appropriate exercise habits.
Limitations
Some potential limitations should be taken into consideration in examining the findings of this study. One limitation was that the present research was a cross-sectional study and did not explore the trend of frailty in old adults with CHF over time. Frailty is defined as a dynamic state, and it is necessary to dynamically track the frailty of patients. Another limitation was that the results of this study lacked objective evaluation indicators and were only based on subjective descriptions. Finally, our study only assessed the frailty of CHF patients in acute care hospitals, which may not be applicable to all patients with CHF. Longitudinal study and interventional study will be needed in the future to analyze and judge the predictive value of these factors in the prevalence of frailty and the level of self-care behavior. Meanwhile, the frailty and self-care of patients in different environments (e.g., communities and nursing homes) are also worth evaluating, and more scientific investigations on frailty in this population are needed.
Conclusions
The important conclusion from the data of this cross-sectional survey is that the physical, psychological, and social frailty affect the self-care capability in older adults with CHF. Frailty is significantly affected by chronic lung disease comorbidities, income, exercise, and the times of hospitalizations in the last year. Self-care behavior is significantly affected by surgical treatment, chronic lung disease comorbidities, and income. Therefore, interventions targeting these variable factors should be constructed and implemented, which may be fundamental to achieving effective self-care and improving the prognosis of CHF. Meanwhile, this study helps to fill the need for new approaches to identify the high risk of frailty individuals in the acute care setting for targeted intervention and tailored transitions in care to promote optimal patient quality care and outcomes and biopsychosocial well-being.
Supplemental Material
sj-docx-1-cnr-10.1177_10547738221075772 – Supplemental material for Frailty Affects Self-Care Behavior in Congestive Heart Failure
Supplemental material, sj-docx-1-cnr-10.1177_10547738221075772 for Frailty Affects Self-Care Behavior in Congestive Heart Failure by Jing Li, Jiaqi Han, Nan Luo, Xinxin Ding, Xiaonan Hao and Kun Li in Clinical Nursing Research
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Department of Science and Technology of Jilin Province (20190303170SF).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.