
Abstract
The aims of the present study were to investigate changes in QOL in post-stroke patients during the first 3 months of rehabilitation treatment. We estimate minimal detectable changes (MDCs) and minimal clinically important differences (MCIDs) of the eight dimensions of QOL and assess the proportion of patients’ change scores that exceed MDCs and MCIDs in stroke survivors who receive rehabilitation in a hospital ward. This prospective cohort study enrolled 40 stroke survivors (57.5% male; Mage = 58.3 years) who received in-hospital rehabilitation for a total of 3 months. The Stroke Impact Scale 3.0, which has eight subscales—strength, activities of daily living (ADLs)/instrumental ADLs (IADLs), mobility, hand function, communication, memory and thinking, emotion, and social participation—was used for assessment on the third day of rehabilitation (Time 1), 1 month later (Time 2), and 3 months later (Time 3). Our findings indicated that the MDC95 and MCID proportions varied from 7.5% to 30% and 7.5% to 65%, respectively, of individuals who exhibited change based on individual change scores. The findings show compliance with MDC and MCID values in physical function, with the lowest proportion in hand function.
Keywords
Introduction
The World Health Organization (2021) reports that cardiovascular diseases (e.g., heart attack and stroke) are the number one cause of death worldwide, and, of these deaths, 85% were due to heart attack and stroke. Stroke affects nearly all quality of life (QOL) functions, resulting in deficits in motor and sensory functions as well as cognitive impairment (Cinnera et al., 2020), and may lead to post-stroke emotional responses (e.g., depression and anxiety). Thus, QOL is an important indicator of stroke rehabilitation (Sadlonova et al., 2021; Schindel et al., 2021).
Changes in QOL are an ongoing challenge for stroke patients during the rehabilitation period, and improvement in the indicators of physical and mental function inspire confidence in rehabilitation. Most methods to determine whether a patient is progressing are based on the statistical significance of the findings, but the clinical importance of these findings is overlooked. Bernstein and Zalinski (1983) make the distinction between the magnitude of “statistically” and “biologically” significant changes and note that, although sample size may affect statistical significance, a small, statistically significant difference may not have biological or practical significance (Spooner et al., 2011).
Therefore, use of minimal detectable changes (MDCs) and minimal clinically important differences (MCIDs) can provide health professionals with a means to identify patients who have experienced clinically significant improvement (Sedaghat, 2019). MDCs refer to the minimal amount of change that falls outside of measurement error in the score of an instrument used to measure a symptom and that reflects true change in a patient between two time points (Kovacs et al., 2008; Nair et al., 2012). Spooner et al. (2011) notes that MDCs represent an expectation of detection, given sample variability, number of samples, monitoring design, statistical trend tests, and significance level. MCIDs can be defined as the smallest difference in the score in the domain of interest that is meaningful for patients (Jaeschke et al., 1989; Kovacs et al., 2008); MCIDs represent “the smallest amount of change in an outcome that might be considered important by the patient or clinician” (Shirley Ryan AbilityLab, 2016, p. 7).
In addition, there are many instruments that assess QOL, including the Stroke Impact Scale (SIS), which is widely used to evaluation stroke patients’ QOL (Pucciarelli et al., 2021). The SIS includes eight dimensions of quality (strength, activities of daily living (ADLs)/instrumental ADLs (IADLs), mobility, hand function, communication, memory and thinking, emotion, and social participation), and the multidimensionality of the SIS may allow health professionals to track patient progress in terms of physical, psychological, and social aspects of life in the rehabilitation setting (Richardson et al., 2016). Thus, the aim of the present study was to investigate changes in QOL in post-stroke patients during the first 3 months of rehabilitation in a hospital ward. We estimated MDCs and MCIDs of the eight dimensions of QOL using the SIS and then assessed the proportion of patients’ change scores that exceeded the MDCs and MCIDs.
Methods
Setting
This study was performed in the rehabilitation ward of a medical university hospital, where patients were recruited from March 18, 2019, to March 17, 2020. Stroke survivors were invited to participate by a clinical researcher. A total of 53 patients met the study criteria and agreed to participate. A total of 40 stroke survivors completed data, collected over the 3-month period.
Study Design and Participants
We used a prospective cohort study design with data collection on the third day (Time 1), 1 month (Time 2), and 3 months (Time 3) after stroke survivors were transferred from the acute ward to the rehabilitation ward. Inclusion criteria were (1) first stroke and admitted to the rehabilitation ward for treatment after the acute phase; (2) no serious cardiovascular disease, cancer, or other major diseases that may affect the measurement of QOL; (3) no severe cognitive impairment or communication impairment; and (4) willing to participate in this study and sign a consent form after the researcher has explained the aims and procedural of the study. Exclusion criteria were (1) patient is less than 18 years old and (2) patient had been admitted to the rehabilitation ward for more than 3 months.
Measures
Patients were assessed on their first visit during the third day in the hospital (Time 1: baseline assessment), 1 month later (Time 2), and 3 months later (Time 3). At each assessment, patients rated their own QOL. The clinical condition of each patient (e.g., National Institutes of Health Stroke Scale, NIHSS) was evaluated by the researcher at the rehabilitation ward. At the 3-month follow-up, patients scored the change in their QOL on the SIS. All measurement instruments were reviewed for content validity by four experts (two rehabilitators and two nurses), and the content validity index (CVI) was above 0.8. Each measurement instrument is described below.
Demographic questionnaire
We collected stroke survivors’ demographic data, including age, gender, marital status, and education level. In addition, stroke survivors’ clinical data (e.g., type of stroke and site of paralysis) were extracted from their medical records.
National Institutes of Health Stroke Scale (NIHSS)
The NIHSS was used to measure patients’ disease severity. It includes 11 items to assess patients’ level of consciousness, horizontal extraocular movements, visual fields, facial palsy, left or right arm motor, left or right leg motor, limb ataxia, sensation, language/aphasia, dysarthria, extinction, and inattention. Each item is scored 0 to 2 or 0 to 3, with a total score that ranges from 0 to 42 and higher scores as representing more severe nerve damage (Sucharew et al., 2013; Williams et al., 2000). Stroke severity can be categorized as follows: 0 = no stroke symptoms, 1 to 4 = minor stroke; 5 to 15 = moderate stroke; 16 to 20 = moderate-to-severe stroke; and 21 to 42 = severe stroke (Kogan et al., 2020; Samuel et al., 2017). In this study, the Cronbach’s alpha across the three time points were .95, .96, and .96, respectively, which indicates acceptable reliability (George & Mallery, 2020).
Stroke Impact Scale (SIS)
The SIS (Version 3.0; Duncan et al., 2003) captures the multidimensional effects of a stroke from the perspective of the patient and was used to assess patients’ disease-specific QOL. It consists of 59 items grouped into eight dimensions of quality (strength, activities of daily living (ADLs)/instrumental ADLs (IADLs), mobility, hand function, communication, memory and thinking, emotion, and social participation). The four dimensions of strength, hand function, ADLs, and mobility comprise the physical function domain, and the two dimensions of memory and thinking, and communication can be clustered together as a cognitive dimension (Coppers et al., 2021; Vellone et al., 2015). Each item is scored on a scale of 1 to 5, and a normalized score of 0 to 100 is calculated from each dimension, with higher scores as meaning that the dimension functions better. A visual analog scale, scored from 0 to 100, was used to measure patient’s global perception of recovery, with 100 as indicating full recovery and 0 as indicating no recovery (Duncan et al., 2003). In this study, the full-scale Cronbach’s alpha across the three time points were .95, .96, and .97, respectively. The subscale Cronbach’s alpha across the three time points ranged from .85 to .86 for strength, .92 to .93 for ADLs/IADLs, 096 to .97 for mobility, .97 to .98 for hand function, .96 to .98 for memory, .96 to .97 for communication, .72 to .79 for emotion, and .93 to .95 for social participation, which indicates acceptable reliability (George & Mallery, 2020).
Data Analysis
The standard error of measurement (SEM) is a reliability measure that assesses response stability and is calculated by the formula SEM = SD[(1 − ICC)1/2], where SD is the baseline standard deviation, and ICC (intraclass correlation coefficient) is the test-retest reliability coefficient (Nair et al., 2012; Schmitt & Di Fabio, 2004; Suriyaamarit & Boonyong, 2018). An ICC reliability value of >.75 is understood as excellent (Shirley Ryan AbilityLab, 2016; Suriyaamarit & Boonyong, 2018). SEM can be used to obtain the MDC, which is calculated in terms of confidence of predication. MDC95 indicates a real change, based on a 95% confidence interval, for individual patients and is calculated as follows: MDC95 = 1.96 × √2 × SEM (Badke et al., 2011; Nair et al., 2012; Spooner et al., 2011).
In regard to the estimates of MCIDs, distribution-based estimates (i.e., effect size and reliable change index [RCI]) were conducted to triangulate the ranges of MCIDs. Effect size is a standardized measure of change obtained by dividing the difference in scores from pre-test to post-test by the SD of the baseline scores (Copay et al., 2007). In this study, the change in scores that correspond to a moderate effect size is considered the MCID; thus, to calculate the change score equivalent to the MCID, one multiplies the SD of the baseline scores by 0.5. The RIC is calculated by the equation RCI = √2SEM2. Finally, the percentage of stroke survivors who exceeded MDC95 and MCIDs were calculated.
Ethical Approval
The study was approved by the Institutional Review Board (IRB) of Chung Shan Medical University Hospital (CSH-2019-A-002). The investigator explained the purpose and procedures of the study to eligible patients and invited them to participate in the study. All patients willing to participate in the study signed an IRB-approved consent form. In addition, based on the patient’s right to privacy, the collected data are kept confidential and coded, and participants had the right to withdraw at any time during the study.
Results
Demographics of Participants
The demographic and clinical characteristics of the 40 stroke survivors are presented in Table 1. The Mage of the patients was 58.3 years (SD = 12.2), with a range of 28 to 76 years, of whom 57.5% were male, 77.5% were married, and most (65%) patients’ education was senior high school or below. Nearly half of the patients had an ischemic stroke (47.5%) and left-side paralysis (50%). Most survivors had a moderate stroke (85%).
Demographic and Clinical Characteristics of Stroke Survivors (N = 40).
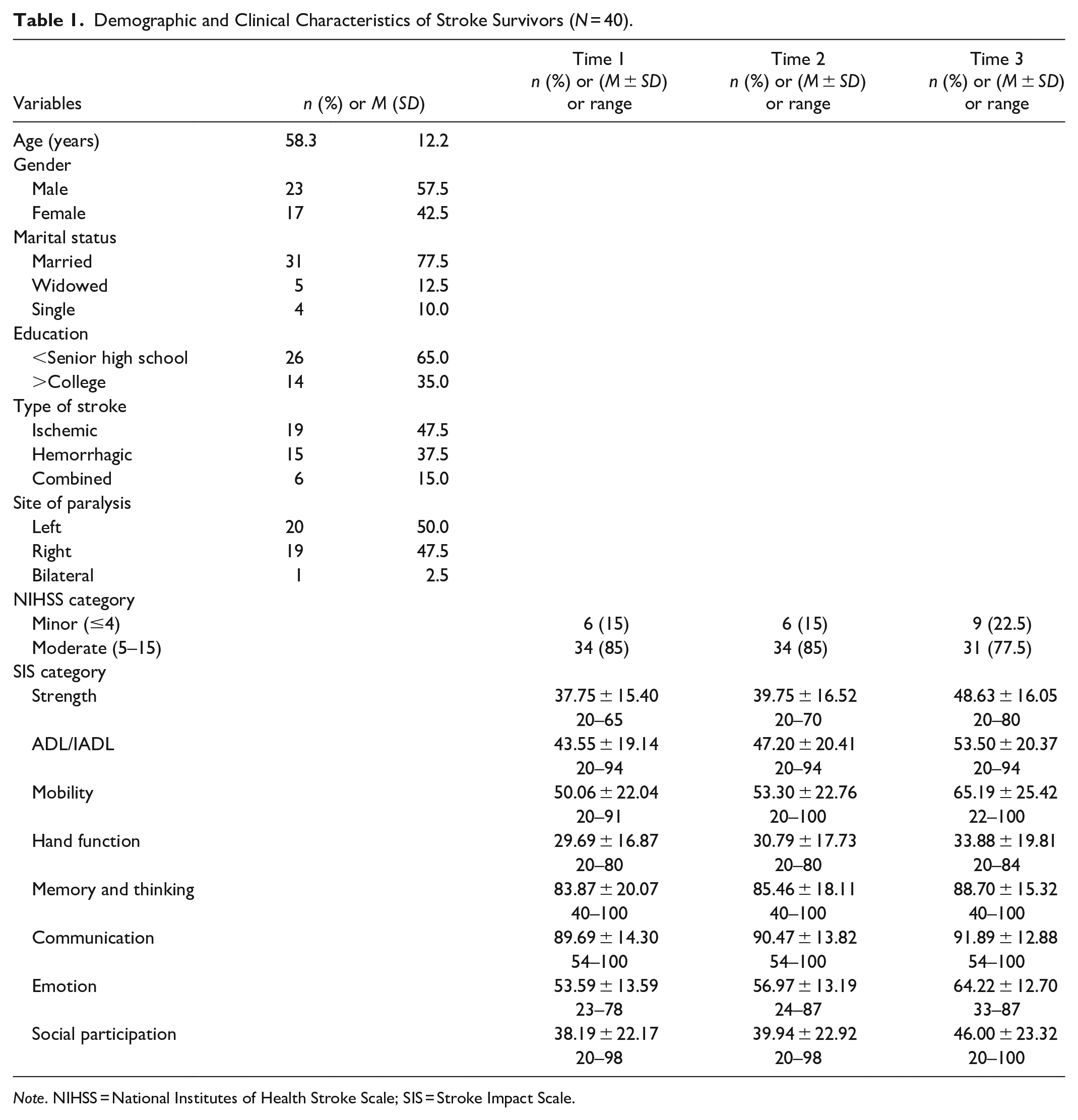
Note. NIHSS = National Institutes of Health Stroke Scale; SIS = Stroke Impact Scale.
Mean Scores in the QOL Domains Across the Three Time Points
Table 1 also shows the mean scores for the QOL domains across the three time points. As shown in Figure 1, of the physical domain scores (Group A), hand function had the lowest baseline values. In addition, communication and memory had higher baseline values among cognitive, emotion, and social participation domains (Group B) and was stable across the three time points. The social participation domain appears to have lower baseline values compared with the cognitive and emotion domains. In all QOL domains, however, change scores increased gradually over time.
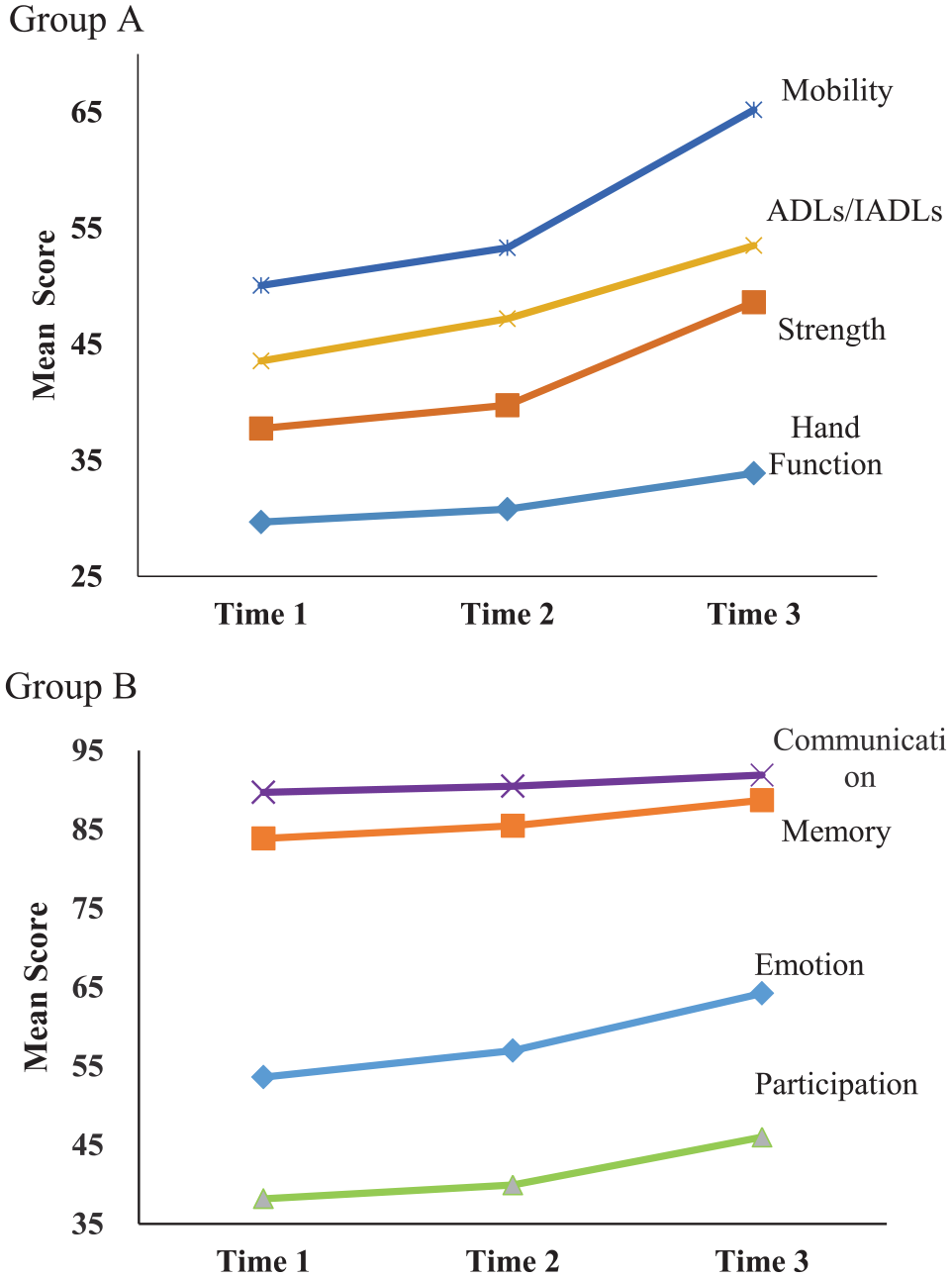
Trend of stroke disease-specific quality of life during the first 3 months of rehabilitation.
Improvement in QOL Domains From Time 1 to Time 3
We calculated the change score of all QOL domains from Time 1 to Time 3. Table 2 presents the ICC values for QOL domains, which ranged from .81 to .97 between Times 1 and 3, indicating excellent reliability (Shirley Ryan AbilityLab, 2016; Suriyaamarit & Boonyong, 2018). The results for SD, SEM, MDC95, and MCID of the QOL dimensions are presented in the table. The MDC95 estimates for the physical dimensions of QOL, that is, strength, ADL/IADL, mobility, and hand function dimensions, were 18.61, 18.38, 25.19, and 11.45, respectively. Approximately one-fourth to one-half of the patients had a positive change that exceeded the MDC95 of the strength (27.5%), ADL/IADL (17.5%), mobility (20%), and hand function (15%) dimensions. For the other QOL domains, the MDC95 values were 14.73 for memory, 13.94 for emotion, 6.87 for communication, and 18.44 for social participation. Of the patients, 7.5% to 30% had a positive change that exceeded the MDC95 values for memory, emotion, communication, and social participation.
ICC, SEM, MDC, and MCID for all Quality of Life Domains (Time 1–Time 3).
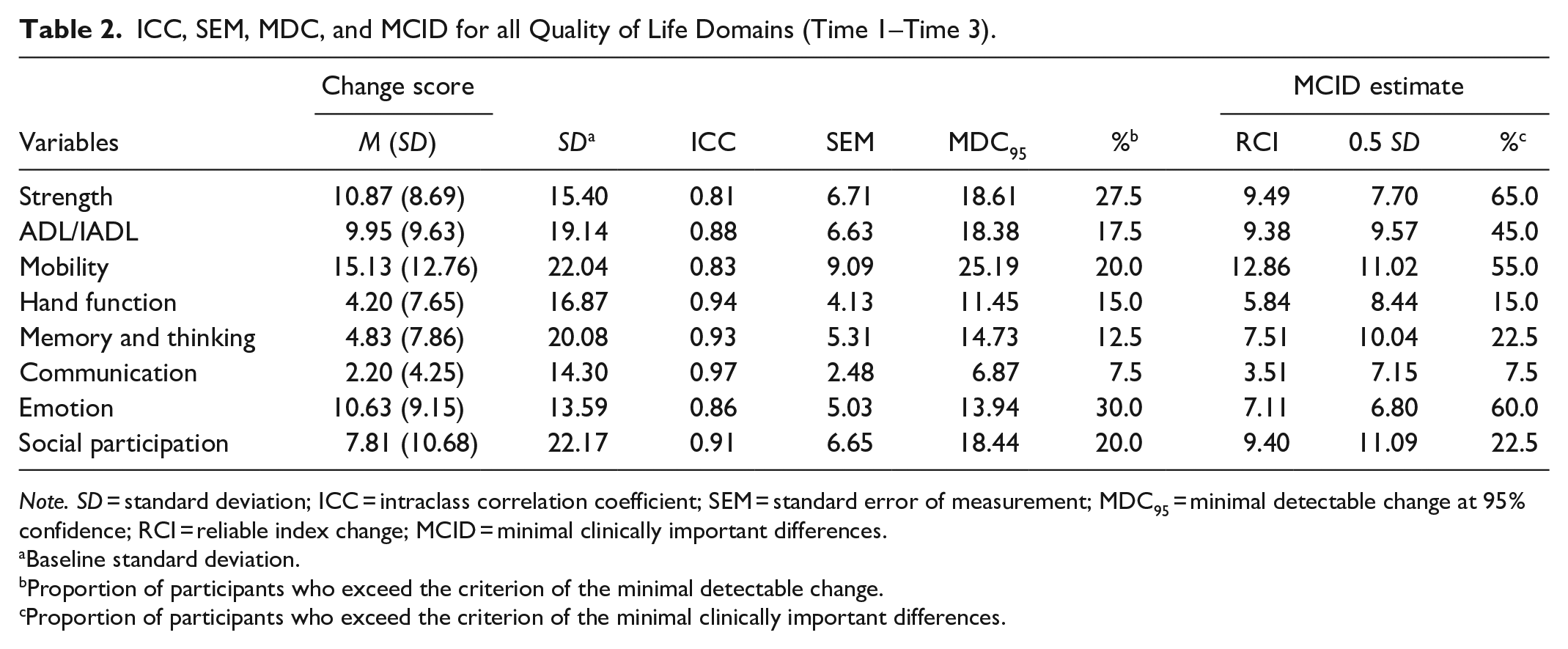
Note. SD = standard deviation; ICC = intraclass correlation coefficient; SEM = standard error of measurement; MDC95 = minimal detectable change at 95% confidence; RCI = reliable index change; MCID = minimal clinically important differences.
Baseline standard deviation.
Proportion of participants who exceed the criterion of the minimal detectable change.
Proportion of participants who exceed the criterion of the minimal clinically important differences.
The distribution-based MCID estimates (0.5 SD) for the strength, ADL/IADL, mobility, hand function, memory, communication, emotion, and social participation dimensions were 7.70, 9.57, 11.02, 8.44, 10.04, 7.15, 6.80, and 11.09, respectively. RCI values ranged from 3.51 to 12.86. We used 0.5 SD as the MCID to calculate the percentage of stroke survivors who exceeded MCIDs due to its value being mainly higher than that of RCI. Overall, changes in nearly one-half to two-thirds of the patients achieved the MCID estimates of the strength (65%), ADL/IADL (45%), and mobility (55%) dimensions; however, hand function was only 15%. In addition, the estimation results indicated that 7.5% to 60% of patients had positive changes that exceeded the MCID of memory, emotion, communication, and social participation.
Discussion
The SIS is widely used to evaluation stroke patients’ QOL. Most studies focus on investigating QOL at 3 to 6 months (Guidetti et al., 2014; Lin et al., 2010) or 1 year or more after stroke rehabilitation (Carod-Artal et al., 2009; Chiu et al., 2021; Sadlonova et al., 2021; Schindel et al., 2021; Wu et al., 2019). Our findings concerned changes in QOL of stroke patients in the first 3 months of rehabilitation, using the SIS. Our findings indicate that the values of MCID for the QOL subscales were 7.70 for strength, 9.57 for ADLs/IADLs, 11.02 for mobility, 8.44 for hand function, 10.04 for memory and thinking, 7.15 for communication, 6.80 for emotion, and 11.09 for social participation. In a previous study, the MCIDs were 9.2 for strength, 5.9 for ADLs/IADLs, 4.5 for mobility, and 17.8 for hand function (Lin et al., 2010). Lin et al.’s (2010) study indicates that the minimum cutoff points that are perceived as beneficial are highest in hand function, whereas in our study, mobility and social participation have the highest cutoffs. These differences may be due to different rehabilitation stages as having different foci in terms of physical function for stroke survivors. In addition, Lin et al. investigated only physical function and did not include cognition, emotion, or social participation, which also may have an impact on the findings.
In this study, all QOL domains experienced a gradual increase from baseline across the three points. We find that the four physical domains had lower baseline values compared with the other domains (e.g., cognitive and emotion), with the exception of social participation. Among the physical domains, hand function had the lowest baseline value, whereas communication and memory had higher baseline values. The social participation domain appears to have lower baseline values compared with the cognitive and emotion domains. This finding is consistent with previous studies (Carod-Artal et al., 2009; Chiu et al., 2021; Pucciarelli et al., 2021), although the stroke survivors investigated in those studies were undergoing rehabilitation a year or more post-stroke. Pucciarelli et al. (2021) noted a significant linear increase in the SIS domains of stroke survivors discharged from rehabilitation hospitals. Our findings also indicated that, among the eight domains of QOL, the three domain of strength, hand function, and social participation had the lowest baseline scores. Thus, improvement of strength, hand function, and social participation during rehabilitation requires more attention (Guidetti et al., 2014).
Based on SEM, we found that the changes of at least 18.61 points on strength, 18.38 points on ADLs/IADLs, 25.19 points on mobility, 11.45 points on hand function, 14.73 points on memory and thinking, 6.87 points on communication and thinking, 13.94 points on emotion, and 18.44 points on social participation were significant, based on a 95% confidence interval, and represented real improvement in these QOL domains. This suggests that MCID scores are smaller than the MDC values (Lin et al., 2010). According to our findings for MCIDs, only the mean change scores of the communication and thinking domain did not achieve the MCID cutoff. This may be because, at baseline, communication and memory have the highest scores of the eight domains, so the scope of improvement is limited. This finding also may be related to the fact that the subjects included in this study did not have severe cognitive or communication impairments. Our current research found that the largest increase in perceived real improvement is mobility, which means that the patient is most able to feel progress in mobility.
We also assessed the proportion of patients’ change scores that exceeded the MDCs and MCIDs. If communication and memory are excluded, the findings show compliance with MDC95 and MCID values, with the lowest proportion of compliance for hand function (15%). These results are inconsistent with the findings of Lin et al. (2010), who report that improvement in hand function was easier to detect than any other SIS domain. This may be related to the different rehabilitation stages of stroke patients. Lin et al. investigated stroke patients who had their first stroke at least 6 months prior, while our participants were 3 months post-stroke. Our findings, however, are in keeping with those of Chiu et al. (2021), who report that no stroke survivors showed a score change higher than the MDC value of the hand function subscale during rehabilitation treatment; in other words, participants did not perceive a significant improvement in hand function. This also shows that an improvement in strength of hand function requires more time or higher priority. Our study showed that 27.5% of patients achieved improvement in strength in the third month. According to the MCID criterion, 65% of patients achieved MCID, indicating that improving strength is key for rehabilitation of hand function. In addition, we found compliance with MDC95 values, with the highest proportion of compliance for emotion (30%). This shows that, in the first 3 months of rehabilitation, in addition to changes in physical function, patients feel emotional changes. It is worth noting, however, that our participants’ extent of stroke hemorrhage was 37.5%, which is higher than that in Montaño et al. (2021), who find that hemorrhagic strokes comprise about 20% of all strokes. Further, right-hemisphere strokes may be associated with worsened emotions (O’Connell et al., 2021). Thus, future research should analyze the emotional responses of left- and right-hemisphere lesions separately.
Limitations
Several limitations warrant consideration. First, due to the impact of the COVID-19 pandemic, the sample size was small, and 25% was lost in follow-up. Nevertheless, our findings provide trends in regard to QOL of stroke survivors for whom stroke disease severity is minor to moderate in the first 3 months in the rehabilitation ward. Second, the study did not analyze data by demographic characteristics (e.g., age and gender). Large-sample studies and analyses by different demographic characteristics are needed to support the MCID values. Third, the participants in this study did not have severe cognitive impairment or communication impairment; therefore, our findings may not reflect stroke survivors with such impairments.
Clinical Implications
Despite the limitations of the present study, the MCID value estimated in this study may be useful in interpreting stroke disease-specific QOL scores in patients who participate in the first 3 months of rehabilitation. Estimates of this threshold can also be used by healthcare providers to assess the development of stroke survivors’ disease-specific QOL post-intervention. Our findings also can be used to calculate sample size and to assess the clinical value of the results in future research.
Conclusion
We established that, for the values of MCID for the QOL domains (SIS subscales), if the mean change scores were 7.70 for strength, 9.57 for ADL/IADL, 11.02 for mobility, 8.44 for hand function, 10.04 for memory and thinking, 7.15 for communication, 6.80 for emotion, and 11.09 for social participation, the changes can be considered clinically important. In addition, the improvement of strength, hand function, and social participation during rehabilitation is important and requires more attention, as these are the most affected part of patients’ perceived concerns.
Footnotes
Author Contributions
Hsiang-Chu Pai and Shu-Chuan Kao were responsible for the study conception and design. Shu-Chuan Kao performed the data collection. Hsiang-Chu Pai involved in data analysis, drafting of the manuscript, and made critical revisions to the paper for important intellectual content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the Chung Shan Medical University Hospital for their funding (CSH-2019-A-002).