
Abstract
Nurses routinely assess pain in hospitalized patients; similar assessment of dyspnea is increasing. Most nurses start with a yes–no question when assessing pain or dyspnea; many record “no” as a zero rating, skipping the rating scale. We tested the hypothesis that recording “no” answers as “zero” fails to detect the symptoms that would have been detected with a rating scale. Nurses asked 60 patients yes–no questions about the presence of dyspnea and pain, then asked patients to rate the symptoms using a 0–10 scale. All “yes” answers were followed by a concordant rating (i.e., greater than zero). More than 25% of “no” answers were followed by a discordant rating (> zero). Documenting “no” as “zero” missed information potentially useful in care planning; patients who rate dyspnea above zero are at greater risk of adverse outcomes. This information can also provide opportunity to start a discussion with patients who may benefit from symptom management.
Introduction
Dyspnea (breathing discomfort), like pain, is a common source of suffering in hospitalized patients (Banzett et al., 2020; Stevens et al., 2018). Furthermore, even low levels of dyspnea are associated with inpatient mortality and other adverse events; there is a sharp increase in associated mortality between dyspnea ratings of “zero” and ratings as low as “1” in hospital inpatients (Stevens et al., 2021). Low ratings of dyspnea may also indicate unacceptable discomfort: 45% of patients surveyed considered breathing discomfort to be unacceptable when they rated it 1, 2, or 3 on a 0–10 scale (Stevens et al., 2019).
Routine dyspnea quantitation and documentation in all patients is not done at most hospitals. Nurses at our hospital began mandatory dyspnea assessment using a 0–10 scale in all patients, on the same schedule as pain assessment in April 2013 (Baker et al., 2017). We surveyed nurses 12–20 months after institution of routine dyspnea assessment (Baker et al., 2017); the survey revealed, among other things, that most nurses (60%) start with a yes–no question, and 37% of those routinely record a “no” answer as a zero rating, rather than proceeding with the rating scale—thus, we estimate that a quarter of answers documented as “zero” were recorded in the absence of a patient rating of zero.
Problem
We saw the documentation of “no” as “zero” as a potential problem because the decision to provide a “yes” response requires a threshold magnitude of sensation to decide that a “yes” response is appropriate; therefore, the patient may fail to report the existing sensation. It might seem intuitive that patients will respond “yes” if they feel any breathing discomfort at all, but individual response thresholds vary. An individual may be hesitant to say “yes” unless they are very sure the symptom is present; for example, a patient may respond “no” until the discomfort reaches a level of 3/10. There may be other reasons for elevated response threshold. For instance, the patient may have accommodated to a pre-existing background level of dyspnea or pain; the patient may be reluctant to “bother” the nurse, etc.
We hypothesized that in clinical practice, “no” answers that are directly recorded as “zero” often fail to detect the presence of dyspnea that would have been detected with a rating scale. The present pilot study tests the null hypothesis that all patients who respond “no” will also rate “zero.”
Although our primary interest is dyspnea, we also report data on pain responses as a comparison landmark. Rating breathing discomfort is unfamiliar to most patients, and the language of dyspnea is unfamiliar to many (Lansing & Banzett, 1996; Mahler & Baird, 2008; Schwartzstein, 1999)—this could lead to discrepancies between ratings and binary questions. In contrast, most patients have had experience with pain scales in prior clinical encounters; the experience and concept of pain is more universally understood, and the language of pain is familiar.
The outcome of this study rests on the selection of a scale with sufficient resolution and reliability. Simple 0–10 scales are in common use for many purposes; our laboratory experience has suggested that a 0–10 scale provides adequate resolution to measure respiratory discomfort. In practical use, for measurement of dyspnea, 0–10 scales are as reliable and sensitive as visual analog scales (which allow theoretically infinite resolution) (Morris et al., 2007). Zero-to-10 scales have much greater sensitivity to change than 4-point scales, an infinitely variable visual analog scale produces only a slight gain in sensitivity compared to a 0–10 scale (Breivik et al., 2000). Numerical 0–10 scales for dyspnea have been well validated (Bausewein et al., 2008; Parshall et al., 2012).
Related Prior Studies
We have been unable to find any published study examining the discrepancies between 0–10 or analog scales and a 2-point yes–no question about the presence of dyspnea (or pain); there are, however, some related studies. A study of dyspnea assessment done by Wysham et al. (2015) compared patient responses using a 11-point numeric scale (like ours) to a 4-point verbal descriptor scale (none, mild, moderate, and severe). In Wysham’s study, 36% of patients who chose the verbal descriptor “none” rated their shortness of breath above zero on the-11 point scale. We know of no other such studies regarding dyspnea.
Rothaug et al. (2013) studied post-surgical pain, and examined the difference between “yes” or “no” questions and rating scales for reporting the interference of pain with four functions (mobility, sleep, breathing, and mood); they did not ask directly about the presence or intensity of pain. They found a significant number of discordant answers, ranging from 12% to 23% of the patients queried, depending on the particular function and the time of day.
Thus, two published studies show a non-trivial discord of symptom report between the response “no” or “none” and the “zero” response on a 0–10 scale. The way in which patients are queried affects the information we receive from them; the present study seeks to help researchers and clinicians decide whether binary questions or rating scales are appropriate for their circumstances.
Methods
Institutional review boards at the concerned institutions approved this study. We interviewed a convenience sample of 60 English-speaking, male and female inpatients aged 18 or older on medical surgical floors during April and May 2017. Data collection was intended to simulate clinical care, so the patient was not initially informed that the data were intended for research. Because it was important to simulate routine patient care conditions and the questioning was brief, institutional review board permission was given for post-hoc informed verbal consent. To comply with the terms of post-hoc consent, no protected health information was recorded (e.g., demographics, medical record information). After the interview, we asked patients for verbal consent to use their responses for a research study. All patients interviewed granted consent to be included in the study.
Our target was to interview at least 50 patients who denied having breathing discomfort in response to the initial yes–no query. This was an exploratory study; given the absence of data on the question we posed, sample size calculations were not possible. Two practicing nurses served as interviewers (authors AMP and JBR). They both used the same protocol to approach hospitalized patients who were currently not busy with tests or routine care. Patients were at rest—seated or recumbent. The interviewer introduced herself to the patient as a nurse, then asked the patient yes–no questions about whether they were experiencing current pain and whether they were experiencing current breathing discomfort (alternating order). After obtaining a “yes” or “no” response for each symptom, the interviewer asked the patient to rate current breathing discomfort and to rate current pain using a 0–10 scale. Zero was defined as “no pain”/“no breathing discomfort” and 10 was defined as “unbearable pain”/“unbearable breathing discomfort.” This is the same 0–10 scale used in routine clinical assessment of dyspnea in our hospital (Baker et al., 2013; Baker et al., 2017, 2020).
If the patient responded “no” when asked if they had breathing discomfort and subsequently gave a rating above zero (i.e., if there was discordance), the patient was asked to explain the apparent discordance using this script: “You stated you had no breathing discomfort, yet you rated your shortness of breath greater than zero. Sometimes patients do this, and we are trying to understand how patients express how they feel. Can you help me understand why you said no at first, then gave a number higher than zero?”
We did not ask patients about reasons for discordant responses with pain.
There were no missing data; all patients approached gave a binary response to current pain and dyspnea, then rated both on the scale. The interviewers were attentive to indications of impatience or loss of rapport with the nurse that might be provoked by asking a patient to give a rating of dyspnea after the patient had already given a “no” response; none was observed.
Results
The observed prevalence of pain and dyspnea were consistent with previously reported prevalence in the non-intensive care hospital population (Stevens et al., 2018). In the present sample, 92% (55/60) of the patients responded “no” to the binary question regarding dyspnea, and 67% (40/60) responded “no” to the pain question. All “yes” answers were followed by a rating that was concordant (i.e., greater than zero). However, 27% of the “no breathing discomfort” answers were followed by a discordant rating (defined as any rating greater than zero). We used chi-square analysis to compare the observation of 45 concordant responses and 15 discordant responses to the hypothetical expected outcome of 60 concordant responses and zero discordant responses—the resultant p value approaches zero. Discordant answers were more common in response to the pain questions (53%), as shown in Figure 1.
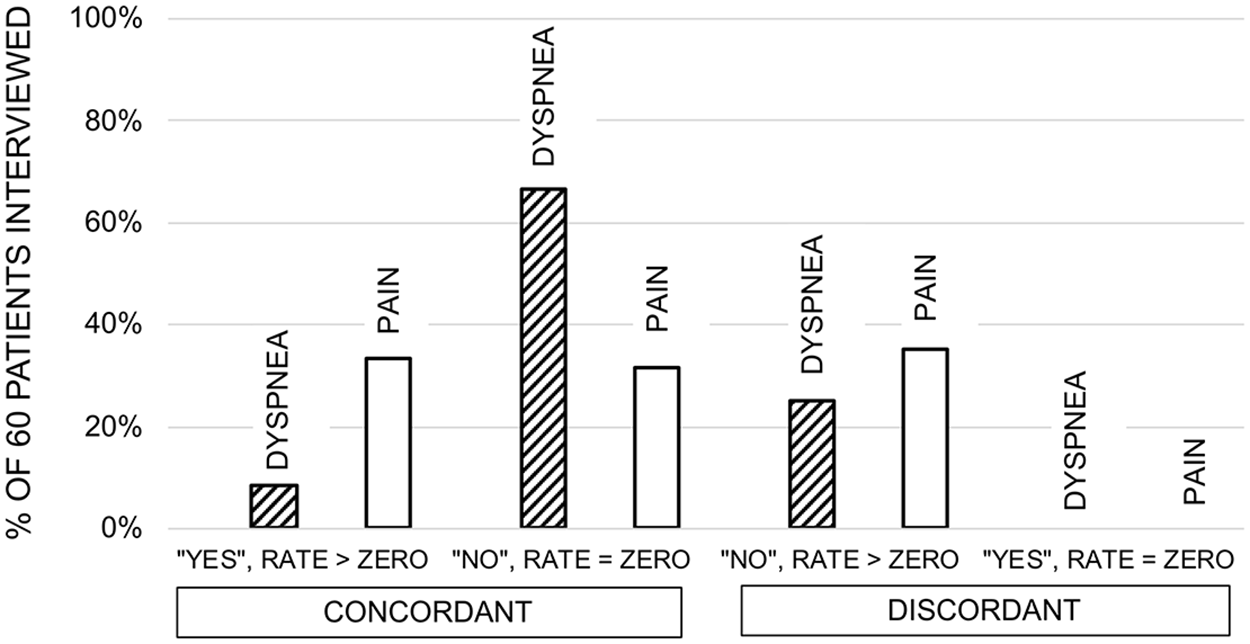
Patients responding “Yes” or “No” to queries about dyspnea and pain categorized by concordance or discordance with subsequent 0–10 ratings of the same symptom. One would logically expect all patients who respond “yes” to rate greater than zero and those who rate “no” to rate “Zero” (“concordant” responses). However, a substantial fraction of patients gave “discordant responses”; they responded “no” and went on to rate the symptom greater than zero (range: 1–6.5, median: 2.5). No patient who responded “yes” gave a discordant rating of zero.
When patients were asked why, after responding “no,” they rated dyspnea higher than zero on the 0–10 scale, their responses varied and sometimes did not directly address the question. Of these 15 patients, four indicated it was similar to the shortness of breath they always lived with; five described their current fatigue or deconditioning, that is, “just had surgery” or not being in their best condition; one stated, “I don’t know how the scale works”; and five did not provide a direct answer to the question. All individual responses are found in the Supplemental Table.
Discussion
The results of this pilot study show that when a binary (yes–no) query is used to assess symptoms, information is lost. In our study, a substantial fraction of patients who respond “no” to a question about symptoms went on to give a rating greater than zero for that symptom; limiting the assessment to a yes–no response may lead to underestimation of symptom burden and a delay in the diagnosis of new or worsening problems. In our study, 27% of patients who chose “no” breathing discomfort rated above zero, comparable to the results obtained by Wysham et al. (2015), although they compared the 11-point scale to a 4-point scale. As in our results, Wysham et al. observed that most patients with discrepant responses gave ratings less than 4/10. We found even more discrepant answers in response to queries about pain: 53% of patients who said they had “no” pain rated pain greater than zero. To our knowledge, there are no other published data on this topic. These data provide a solid reason to proceed with further studies and guidance for study design.
Does Response Threshold Explain the Discord Between “no” and “zero”?
A decision to say “yes” when a patient is asked if she or he is experiencing discomfort arises from the evaluation of sensory evidence. But the response threshold to say “yes” is determined by more than just sensory input. The individual establishes his or her own response criterion based on personal factors (e.g., the threshold will be higher in a stoic patient) and situational factors (e.g., the threshold may be lowered if the patient perceives some gain for a positive response). In the psychophysics laboratory, where graded intensity stimuli can be accurately measured, it can be shown that the response threshold for reporting sensation is above the actual sensory threshold measured using other means—this response threshold has been termed “decision criterion” (Swets, 1959). In our study, more than half of the patients who gave discordant answers to dyspnea queries subsequently gave low ratings (1/10 to 3/10); likewise, three-quarters of the patients who gave discordant answers to pain queries subsequently gave low ratings. Because it is not possible to quantitatively measure the intensity of stimulus generated by pathophysiology, we cannot measure a true decision criterion for clinical symptoms. However, this phenomenon is a likely explanation when patients respond “no” or “none” and give low, but non-zero ratings.
Other Factors may Contribute to Discord Between Patient Report and Symptom Intensity
Personal factors such as stoicism/somatization, expectation of treatment, inability to use scales, and the patient’s usual level of discomfort can affect yes/no responses, patient ratings, or both. Factors shown to influence how patients rate pain include the impact on daily life, level of distress, gender roles, cultural preferences, and how patients view their current pain compared to their “worst” pain (de Williams et al., 2000). Past experiences of pain have been shown to shape perception of current pain which can then lead patients to under-report or over-report current pain (Apkarian, 2011).
Usual level of discomfort
Indeed, several patients said they reported “no” but gave above-zero ratings because they ordinarily live with some baseline level of breathing discomfort; the rating scale elicited a response that had been hidden in the binary response.
Ability to use scales
In psychophysical experiments where the stimulus level is known and can be related quantitatively to subjective rating, some people (estimated 10–15%) are unable to use a scale reliably (i.e., the correlation between stimulus and rating is poor) (Revelette et al., 1984). Poor rating could provide an alternative explanation for the 27% discordant dyspnea responses and 53% discordant pain responses, but we think this is unlikely.
There is no single assessment method appropriate for all settings; a number of factors must be considered, for example, the kind of symptom (dyspnea vs. pain), the setting (laboratory research vs. clinical research vs. clinical practice), the training of personnel, language barriers, etc. In addition, one must consider how the information is intended to be used (symptom management, risk assessment, care planning, treatment evaluation). It is clear that laboratory and clinical research can benefit from the additional resolution (sensitivity) of 0–10 or continuous visual analog scales compared to binary questions. We will discuss here whether the added information is important for patient care. Rothaug et al. (2013) argue, based on simplicity, fewer missing responses, and patient preference that binary queries are preferable. One must bear in mind that their approach included four binary questions, thus eight response possibilities; this additional information may compensate for the reduction from 11-scale to 2-scale options, and may have impacted patient preference. We would argue that when a single dimension of pain or dyspnea is assessed, as is usual in clinical settings, that a 0–10 scale is to be preferred.
Is the Lost Information Important?
Might the missing information be useful for symptom management?
As shown in Figure 2, data on patient acceptance of dyspnea in hospital inpatients, pain in hospital inpatients, and pain in post-surgical patients suggest that low levels of dyspnea are unacceptable to an appreciable fraction of patients, while low levels of pain, especially post-surgical pain, may be more “acceptable” to patients (Stevens et al., 2019; van Boekel et al., 2017). An argument can be made that the more sensitive rating assessment should be used to detect the presence of pain or dyspnea, after which further questioning can determine the need for symptom management. Obtaining and documenting a dyspnea or pain rating takes less than a minute, and does not impede nursing work flow (Baker et al., 2017, 2020).
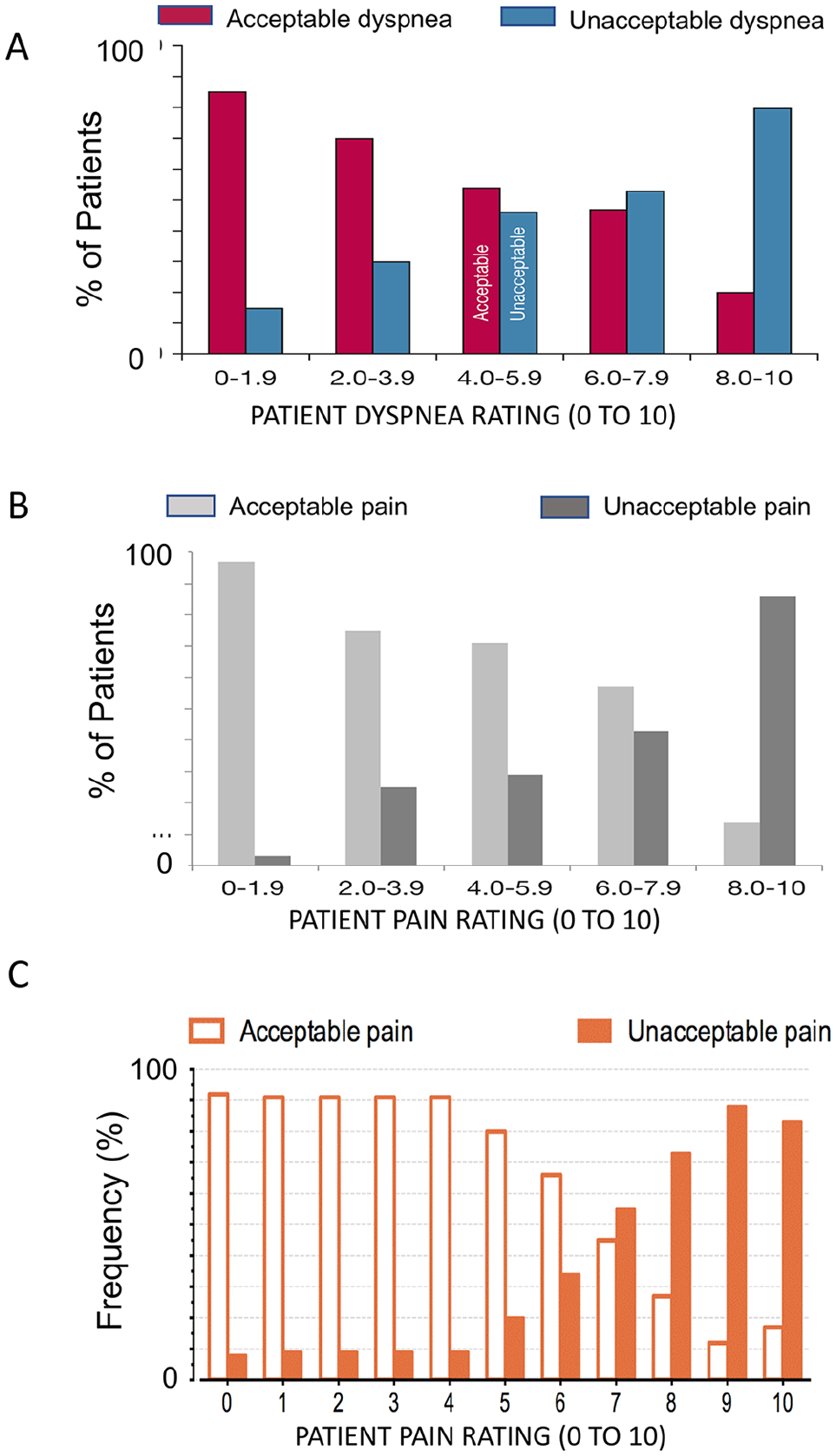
Acceptable levels of dyspnea and pain. Panel A shows the acceptability of dyspnea in general hospital inpatients; the data show that resting dyspnea levels below 2/10 are unacceptable to more than 10% of patients in this circumstance; dyspnea levels 2/10 or above are unacceptable to many patients. Panel B shows the acceptability of pain in general hospital inpatients; the data show that pain levels 1/10 are very well tolerated, but in this circumstance pain levels 2/10 or above are intolerable to many patients. Panel C shows the acceptability of pain in post-surgical patients; it appears that pain levels below 5/10 are generally well tolerated in this circumstance. Panels A and B from Stevens et al. (2019) reprinted with permission from the publisher, Panel C from van Boekel et al. (2017) reprinted under CC BY License.
Might the missing information be useful for risk assessment?
The presence of any dyspnea at rest in hospitalized patients, even a rating of 1/10, predicts increased risk of adverse outcome; for example, the risk for mortality, transfer to intensive care, and the need for extended care are approximately doubled with low dyspnea ratings (Stevens et al., 2021). If patient-reported dyspnea data are to be utilized for planning care and resource allotment, then the more sensitive patient 0–10 rating assessment is advisable.
Limitations
This was a single institution study, data were gathered by two individuals, and the data were gathered in only two of the hospital’s inpatient units. It is not possible to generalize the observed prevalence of discordant responses to other settings. Patient sociodemographic characteristics, nurse characteristics, illness history, and institutional factors may modulate the overall prevalence. However, the prevalence we observed is in approximate accord with the most comparable studies (Rothaug et al., 2013; Wysham et al., 2015), and it clearly shows the existence of the no-zero discrepancy.
The experience of patients in our institution may modify the result. Our nurses routinely assess dyspnea; thus, our patients have been asked to rate their dyspnea every shift. One would expect these factors to reduce the discord between binary questions and rating scales, leading to an underestimate, rather than an overestimate, of discordant responses.
Our sample was based on convenience—those patients not otherwise occupied with care activities, sleep, or visitors; it is difficult to know whether this biased the frequency of discordant responses.
Our study design required that we ask patients to report the same symptom twice in succession—the logical order was to proceed as the care nurse normally would: first ask the yes–no question, followed by the rating scale. We do not know the effect on responses of asking twice, or of presentation order.
Perhaps the most important limitation of our study is that we did not employ a structured debriefing to determine individual patients’ level of understanding of questions, their ability to articulate their answers and assess their numeracy. We did not ask direct questions about the likely mechanisms affecting response threshold. Patients’ answers to our open-ended free-form question were not always to the point and were difficult to interpret.
Application
Nurses in our hospital strongly supported dyspnea assessment and documentation using a rating scale. They reported it was easy to do, and objective observations showed that it requires less than a minute (Baker et al., 2017). When clinicians use a scale to assess pain and dyspnea, the patient has an opportunity to report more subtle gradations of discomfort, lessening the effect of decision criterion (Lansing & Banzett, 1996). Pain ratings are now well accepted in the clinical community—our results suggest that patients are at least as consistent when rating shortness of breath as when rating pain. This is consistent with the impression of many nurses in a prior study that patients find “rating of dyspnea was easier than rating pain” (Baker et al., 2017).
In the busy inpatient setting, the simple 0–10 numeric scale provides a good compromise between binary questions and more sophisticated assessments of dyspnea or pain that evaluate sensory quality, emotional response, etc. (e.g., the Multidimensional Profile, Dyspnoea-12, McGill Pain Questionnaire, or Multidimensional Affect and Pain Survey) (Banzett et al., 2015; Clark et al., 2003; Melzack, 1975; Yorke et al., 2010).
Conclusion
We believe this is the first study directly comparing a binary question to scalar ratings for assessment of breathing discomfort. Although representing a small sample of patients in a single institution, our data provide provocative observations that raise awareness of the issues about patient assessment and an impetus for larger, more sophisticated studies. We found that documenting the response “no” as “zero” missed information—a substantial fraction of patients who answered “no” went on to give ratings above zero. This missing information can be useful in planning care and resource use, because patients who rate dyspnea above zero are at significantly greater risk of adverse outcomes (Stevens et al., 2021). In addition, this information may provide opportunity to open up a discussion with patients who may benefit from symptom management. Given the large number of patients with dyspnea, care in how we assess this symptom may improve treatment decisions and impact patient outcome.
Supplemental Material
sj-docx-1-cnr-10.1177_10547738221134564 – Supplemental material for Rating Dyspnea and Pain: “No” is Not Always “Zero”
Supplemental material, sj-docx-1-cnr-10.1177_10547738221134564 for Rating Dyspnea and Pain: “No” is Not Always “Zero” by Kathy M. Baker, Alison M Phelan, Jennifer B Reilly, Robert W. Lansing, Richard M Schwartzstein MD and Robert B. Banzett in Clinical Nursing Research
Research Data
sj-pdf-2-cnr-10.1177_10547738221134564 – Research Data for Rating Dyspnea and Pain: “No” is Not Always “Zero”
Research Data, sj-pdf-2-cnr-10.1177_10547738221134564 for Rating Dyspnea and Pain: “No” is Not Always “Zero” by Kathy M. Baker, Alison M Phelan, Jennifer B Reilly, Robert W. Lansing, Richard M Schwartzstein MD and Robert B. Banzett in Clinical Nursing Research
Footnotes
Acknowledgements
The authors thank the patients at BIDMC for their time and cooperation with this study. This study was supported by a grant from the National institute for Nursing Research (10006).
Authors’ contributions
This study was conceived and designed by RBB, KMB, and RWL. JBR and AMP collected the data. Data analysis was performed by JBR, AMP, KMB, and RBB. RBB, KMB, RMS, and RWL interpreted the findings. All authors participated in writing and editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by NIH grant NR10006 to Robert B. Banzett. The funding body had no part in designing this study or interpreting its results.
Ethics approval and consent to participate
Institutional review boards at Beth Israel Deaconess Medical Center and Simmons College approved this study. Institutional review board permission was given for post-hoc informed verbal consent. To comply with the terms of post-hoc verbal consent, no protected health information was recorded (e.g., demographics, medical record information). All patients interviewed granted consent to be included in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.