
Abstract
Treatment adherence is a fundamental aspect of heart failure (HF) management. This study aimed to explore the experiences of facilitators and inhibitors of treatment adherence in patients with HF. This descriptive qualitative study was conducted from May 2020 to June 2021. Participants including people with HF, their family caregivers and physicians, and nurses were selected purposefully, with the aim of obtaining sufficient information power. Semi-structured interviews were used to collect data. Data were analyzed using thematic analysis. Two main themes “the driving forces behind treatment adherence” and “the deterrent forces behind treatment adherence” emerged from the analysis. The first theme contained the following subthemes: “supportive family,” “positive personality characteristics,” and “having health literacy.” The second theme consisted of “negligence,” “psychological problems,” “cultural, social, and economic problems,” “physical limitations,” and “lack of self-care management knowledge.” Nurses can consider facilitators and inhibitors of treatment adherence in designing educational and care programs for patients with HF.
Heart failure (HF) is a complex and debilitating clinical syndrome that is associated with significant morbidity and mortality (Nordfonn et al., 2019). Currently, the global prevalence of HF is 64.34 million people (Lippi & Sanchis-Gomar, 2020). The prevalence of HF in Iran is worrying and is an important challenge for the Iranian health system (Esnaasharieh et al., 2022). In Iran, the 1-year mortality rate from HF is reported to be about 32% (Sarrafzadegan & Mohammadifard, 2019). HF is one of the costliest chronic diseases to treat and part of the costs is associated with the readmission of half of the people with HF within 1 year (Ware & Dorai, 2019). In order to reduce the incidence of HF and delay progression of the disease, it is necessary for people with HF to adhere to a strict treatment regimen (Nordfonn et al., 2019).
The World Health Organization defines treatment adherence as “the extent to which individual behaviors (such as medication, diet, lifestyle changes) are following recommendations accepted by a health care provider” (World Health Organization, 2003). Adherence to a treatment regimen refers to the activities that individuals perform in order to maintain life, healthy functioning, personal growth, and well-being (van der Wal et al., 2010). Managing HF requires changes in health-seeking behaviors, including paying careful attention to diet, physical activity, and prescribed medications (Ruppar et al., 2015). Increased complexity in treatment regimen leads to poor adherence among people with HF. Hence, treatment regimen adherence is raised as a complex and challenging phenomenon for both the individual and treatment team in managing HF (Kvarnström et al., 2021). Due to the special importance of HF management, health care providers should pay special attention to the issue of treatment adherence (Amaral et al., 2015).
Unfortunately, treatment adherence in patients with HF is poor (Negarandeh et al., 2021; Pallangyo et al., 2020). The rate of non-adherence to the dimensions of the treatment regimen (pharmacological and non-pharmacological) in people with HF has been reported from 10 to 93% (Dehghanzadeh et al., 2015; Pallangyo et al., 2020; Ruppar et al., 2016; Sánchez et al., 2014; Silva et al., 2015), which is very thought-provoking and a major challenge for the healthcare system of countries (Mikaili et al., 2019). Non-adherence to the treatment regimen is one of the prime reasons for the failure of the treatment plan and lack of favorable response to the prescribed treatment plan (Kamrani et al., 2015). In people with HF, this will lead to worsening of symptoms, disease recurrence, progression of disability, need for urgent immediate treatment, and hospitalization. In addition, not adhering to the treatment regimen is significantly associated with longer length of hospital stay and higher costs (ShariatPanahi et al., 2020; van der Wal et al., 2010). In contrast, positive consequences of following a treatment regimen in people with HF include maintaining physiological stability, delaying disease progression, improving quality of life, and reducing readmission rates and mortality (Wu & Moser, 2018).
Several studies have been conducted on treatment adherence and its dimensions in different contexts. However, in some of them, only the experiences of the patients have been mentioned (Nordfonn et al., 2019). Treatment adherence has a multidimensional nature; however, some studies have focused only on the dimension of medication adherence (Forsyth et al., 2019) or adherence to self-care behaviors (Negarandeh et al., 2021). In another study, only the experiences of patients with respect to dietary sodium adherence have been discussed (Heo et al., 2021).
Despite the advances made in effective therapeutic interventions for treatment adherence among people with HF over the past few decades, the adherence rates have remained unchanged (Shah et al., 2015). Because the experience of each person in treatment adherence is unique; also, considering the increasing growth of the population and the variety of patients with HF, fluidity of the context of each person and the complex and diverse needs of people, it is necessary to provide qualitative insight to identify this experience and its facilitators and inhibitors. A qualitative study will help to explore the various dimensions of this phenomenon and obtain a clearer picture of it. Therefore, the present study was conducted to explore the experiences of patients with HF about adherence to treatment and its challenges.
Method
In this study, a descriptive qualitative methodology (Sandelowski, 2010) was used to explore the experiences of treatment adherence in people with HF. The present study was conducted from May 2020 to June 2021.
Participants in the study were purposefully selected with different levels of experience from among people with HF, their family caregivers, physicians, and nurses in HF clinics affiliated to Tehran University of Medical Sciences. The first author (SFGH) after obtaining the necessary permits and the consent of the relevant authorities, referred to the study settings and introduced herself, and explained the objectives of the study. Characteristics of participants with HF included the diagnosis of HF class I to III (according to the New York Heart Association (NYHA)) approved by HF fellowship (Nordfonn et al., 2019), age over 18 years, and history of HF for at least 6 months. Participants with HF were excluded from the study if their clinical condition became unstable and they were not willing to continue cooperating in the study. Nurses with at least a bachelor’s degree and a minimum 2 years of experience working with people with HF, as well as physicians with an HF fellowship degree were selected to take part in the study. Characteristics of family caregivers included people with experience in caring for a patient with HF during the past 6 months. A total of 415 patients with HF referred to the HF Clinic were eligible to participate in the study. Thirty participants were included in the study. Four participants refused to participate in the study. The reason for not participating was their unwillingness to be interviewed.
Semi-structured interviews were used to collect data. All interviews were conducted individually and face to face by the first author (female, PhD candidate in nursing) using the interview guide. The questions in the interview guide were designed based on the purpose of the study and according to the type of experience of the participants (patients, family caregivers, nurses, and fellowship). The interview guide was pilot tested with two participants and then modified. This guide is flexible and some questions were modified during the implementation of the study. This study is the first author’s second experience of qualitative research. The first author (SFGH) was present at the HF Clinic for a few months as completion of her non-core course in clinical setting before starting the study to become more familiar with people in the study setting. This outpatient clinic makes it possible to prevent long hospitalizations of patients. Patients are visited by the HF fellowship. Drug infusions (such as furosemide, dopamine, and iron) and EECP (Enhanced External Counter Pulsation) are performed by the nurse in several sessions. The researcher coordinated the time and place of the interview with the participants. The interviews were conducted in a separate and quiet room of the HF Clinic that did not have any disruptive factors such as noise, referrals, and telephone calls, and the observance of ethical principles was considered. After selecting the participants, the objectives of the study were explained to them. Written and oral consents were obtained from each participant to enter the study, conduct an interview, and also record interviews. The first interview was conducted with a woman with HF who was willing to participate in the study and talk about her experiences. A demographic information form was completed for each participant. After communicating and gaining the trust of the participants and based on the interview guide, first simple and more general questions were asked. Then, according to the participants’ answers and experiences, the interview continued interactionally with more specific and detailed probing questions. The interview started with a general question “Can you explain how you adhere to your treatment regimen?” (Patient with HF), “How do you take care of a person with HF?” (Family caregivers), “Can you tell me about your experience of adhering to treatment in people with HF?” (Nurse and Fellowship) and then, the next questions were asked, based on the participants’ answers and the interview guide. During the interview, questions such as “What do you mean” or “If you can explain more” were used as needed. At the end of the interview, the participants were thanked and asked to comment if there was anything left unsaid, and they were also asked about the possibility of holding the interview sessions again in the future. The interviews continued until sufficient information power was reached (Braun & Clarke, 2019). All interviews were recorded using a digital audio recorder. Then, the audio files were transferred to the computer and stored. The duration of each interview lasted from 20 to 60 minutes, depending on the conditions of the participant and the extent of his/her cooperation. The researcher emphasized the participants’ experiences during the interview. In order to confirm the statements of the participants or to conduct subsequent interviews, appropriate coordination was done, including the registration of mobile phone numbers and the permission of the participant to link with him/her on social networks. Also, the researcher’s phone number was provided to the participants.
MAXQDA 2020 software was used to manage textual data. Simultaneously with data collection, textual data was analyzed using Braun and Clarke’s 6-step inductive thematic analysis approach. Inductive analysis (bottom up) is a process of data coding without a preexisting coding framework or the researcher’s analytic preconceptions. Thematic analysis is a method for identifying, analyzing, and interpreting semantic patterns (themes) in qualitative data to answer research questions (Braun & Clarke, 2006; Clarke & Braun, 2014; Maguire & Delahunt, 2017). Each interview was considered a unit of analysis. In the first step for familiarity with data, the audio file of the interviews was transcripted by the first author (SFGH) immediately after each interview. Then, to gain a general and correct understanding, the transcripts were carefully read and re-read several times. Each paragraph, sentence or phrase, and word that was written in terms of concept and content related to the purpose of the study was considered as a semantic unit. Then, sections of the transcripts were summarized and coded separately by the authors (SFGH) and (EN) in line with the research question as well as the interesting points on the subject. The coding performed by two researchers was compared and discussed, and the necessary corrections were made. In the third step, the researcher identified patterns in codes across the entire dataset and grouped related codes into potential themes. In the fourth step, with the authors’ consensus, (SFGH), (EN), and (MACH) themes were investigated to ensure whether the extracted codes and the data set were adequately supported by the data, or whether or not the themes overlap. In the fifth step, the definition and naming of themes were done in line with the research question. In the final step, the findings were reported to examine the themes and the relationship between them. A thematic map was drawn (Figure 1).
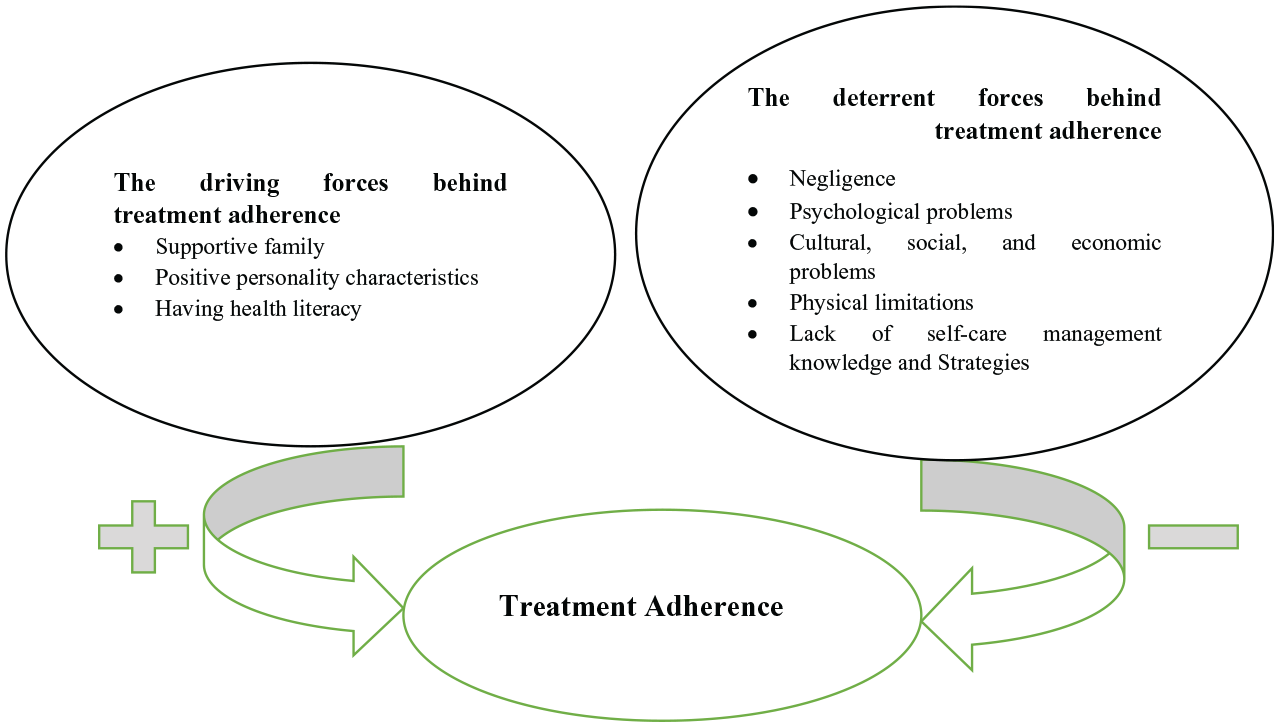
Diagram 1: Thematic map.
According to (Nowell et al., 2017), the trustworthiness of qualitative data was investigated. An in-depth and true understanding of the data was achieved, by engaging with the data for a long time and spending enough time collecting and analyzing them. Researcher triangulation was used in all steps of data analysis. For this purpose, coding and comparing codes, grouping codes, and identifying themes were done by the authors (SFGH & EN). Also, all authors reviewed the final definition and naming of themes. In case of disagreement between the researchers, the extracted codes and themes were reviewed again and the necessary corrections were made. Member check was used to confirm the identified themes. Thus, the themes were investigated by four participants (HF Fellowship & HF Nurse). After reading the themes, if necessary, their feedback was used to change and modify the identified themes. This method helped the researchers fit extracted themes based on the viewpoints of the participants. The transcripts were returned to the participants and they were asked to confirm their experiences. The results of coding and themes extracted by all research colleagues were reviewed and in cases where there was no agreement, the necessary revisions and corrections were made. To check the confirmability of the data in order for the audience and readers to follow the research path, the following was done: A complete description of the research process, including a detailed description of participants, selection of participants, time, and place of data collection, analysis, and formation of codes and themes. Having a history of conducting qualitative studies and publishing qualitative articles by seven members of the research team was considered to the credit of the researchers.
This study received ethics approval from the Organizational Ethics Committee of the School of Nursing and Midwifery and the School of Rehabilitation—Tehran University of Medical Sciences (Ethics Code: IR.TUMS.FNM.REC.1398.174).
Results
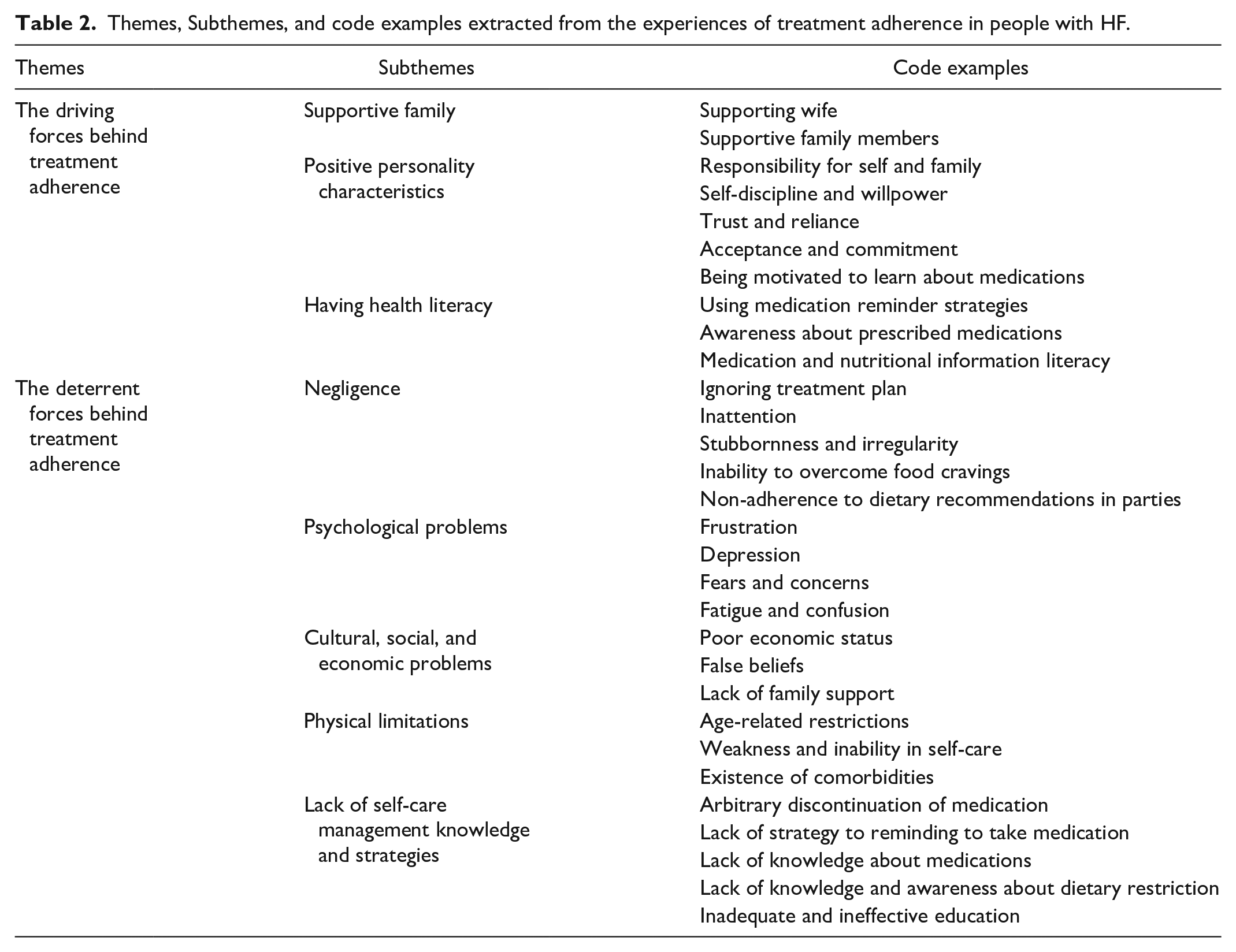
A total of 35 interviews were conducted with 30 participants including 15 people with HF, two HF fellowships, eight nurses who had experience working with people with HF, and five family caregivers. The demographic information of the people with HF participating in the study is presented in Table 1. Most physicians and nurses participating in the study (70%) had a mean age of 39.40 ± 8.40 years and a mean work experience of 13.50 ± 8.22 years. The majority of family caregivers participating in the study were female (80%) and had a mean age of 44.80 ±9.67 years. Participants’ experiences were classified into eight subthemes and two main themes (Table 2).
Demographic Information of Participants of the Study.
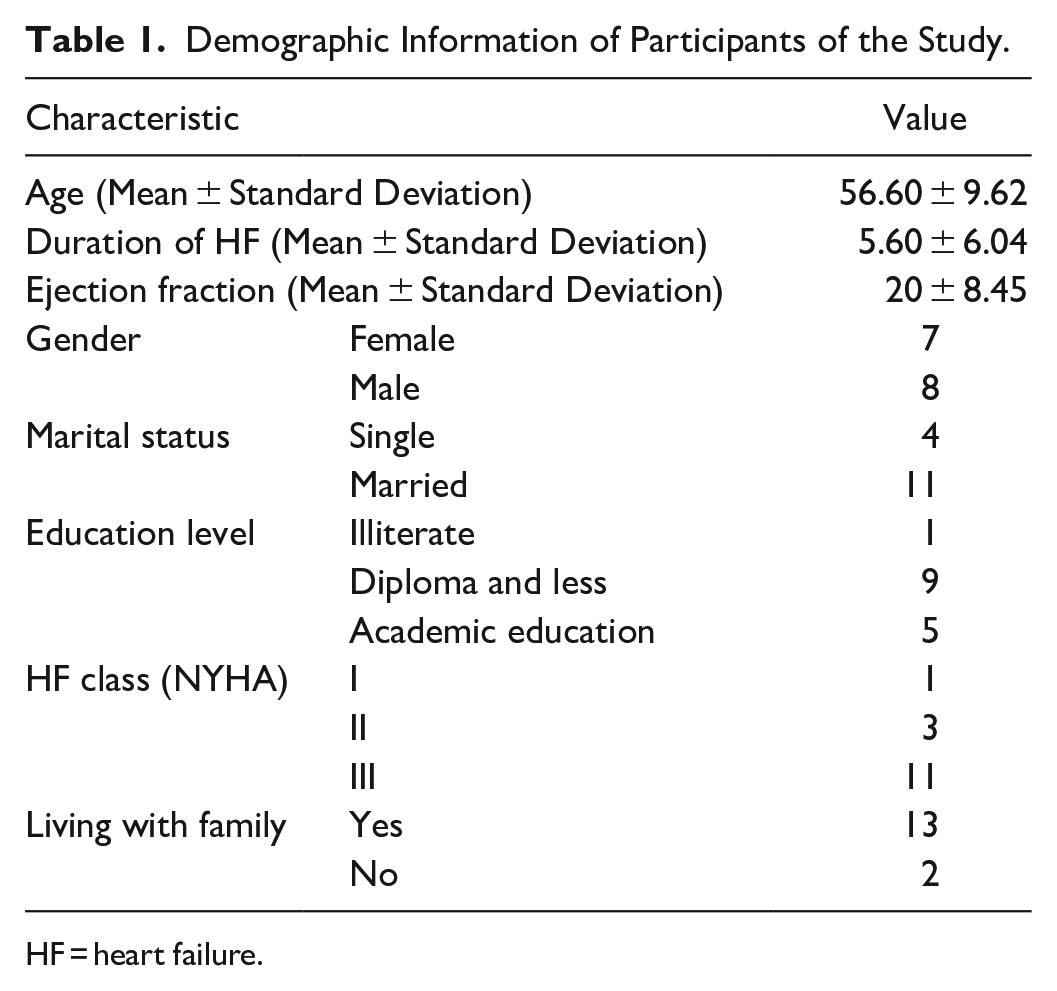
HF = heart failure.
Themes, Subthemes, and code examples extracted from the experiences of treatment adherence in people with HF.
Theme 1: The Driving Forces Behind Treatment Adherence
Supportive family
Interviews and experiences of the participants showed that living with the family, having healthy relationships and family integration is effective in treatment adherence as prescribed in the dimension of lifestyle modification. Based on the participants’ experiences, individuals who had family support were more successful in managing stress and following regularly scheduled visits.
“My wife and children are very careful not to make me feel nervous or stressed. Whenever I feel stressed, my wife talks to me and comforts me. Sometimes when I feel stressed, we go for a walk together and I become calmer. Everyone in the house considers my condition.” (45 year male, NYHA III)
Positive personality characteristics
The participants’ experiences showed that self-responsibility and responsibility toward family, self-discipline, willpower, and trust in God lead to diligence in adhering to treatment regimen.
“It depends on how much everyone cares about his/her own life. As the saying goes, let's see how responsible a person feels for himself/herself and his/her family. How much can a person control himself/herself and do what is prescribed for him/her?” (45 year male, NYHA III)
Acceptance and commitment to treatment are important in the effectiveness and success of the prescribed treatment program.
“Because I’m sick and have HF, I'll get worse if I do not take my medicine. The doctor told me that I should take medicine for the rest of my life. I always take my medicine on time. It may be delayed a bit, but it never happens that I don’t take my medicine at all.” (50 year male, NYHA III)
Being motivated to be aware of medications as a strong point can lead to better adherence to the medication regimen.
“I would like to know about the benefits of these drugs that I take, what their effects are and what happens in my body? What if I do not eat or if I do eat? These are very important. I am taking medicine, but I do not know what it is, and you should know this.” (63 year male, NYHA III)
Having health literacy
Health literacy refers to the use of medication reminder strategies, awareness about prescribed medications, and medication and nutritional information literacy.
Based on the findings, people with HF use medication reminder strategies to improve their treatment plan adherence.
“I take my medications as the doctor prescribed. I have a small box in the house that is divided from Saturday to Friday, my wife puts my medications in it and I take them. So, I know what medications I should take every day.” (50 year male, NYHA III)
Awareness about prescribed medications as part of self-care knowledge is also a strong point of other people with HF in adhering to the medication regimen.
“Well, I take one aspirin daily to thin out my blood. I take it after lunch and food. There is a Furosemide pill that is a diuretic that prevents my body from swelling. I have to take it every 6 hours.” (65 year female, NYHA III)
Another driving force of treatment adherence for people with HF was the medication and nutritional information literacy, which was gained from participants' experiences.
“I always check the food I use, if it has sodium on the label, I do not eat it, for example, on the bottle of mineral water, if it says sodium, I do not drink it.” (48 year female, NYHA III)
Theme 2: The Deterrent Forces Behind Treatment Adherence
Negligence
Negligence in treatment adherence obtained from the interviews included five concepts, ignoring the treatment plan, inattention, stubbornness and irregularity, inability to overcome dietary cravings, and non-adherence to dietary recommendations in parties, which are important in adhering to the treatment among people with HF.
“When you know salt is not good for you and you eat it again, it is a sign of being indifferent to your health. Indifference causes you not to follow the treatment plan anymore. . ..” (73 year male, NYHA III) “My husband is very stubborn and nervous. I cook food with a very small amount of salt. Even though we eat less salt, he adds salt and does not listen to me at all. When I insist, he gets angry and we end up in a tough spot. . ..” (family caregiver, 55 year female)
Psychological problems
Frustration, depression, fears and concerns, fatigue, and confusion are some of the psychological factors involved in adhering to treatment plan, which was obtained from interviews with participants.
“They do not exercise at home for fear of symptoms. But we recommend them to do light exercises for at least 20 minutes daily, and many of them do so, but concern about the shortness of breath and heart problems prevents them from exercising.” (Nurse, 23 year of experience) “HF Patients have low morale, they are often depressed, and their families get tired and complain about them. All of this affects patients and they no longer have any hope of adhering to their treatment plan and follow-up visits.” (Nurse, 26 year of experience)
Cultural, social, and economic problems
According to the experiences of the participants, one of the perceived barriers to treatment adherence in terms of lifestyle modification is economic problems. Some patients with HF may not adhere to their diet due to poor financial status and high costs associated with buying unusual foods recommended by health care providers.
“Their economic status may limit them from improving their lifestyle. Now, maybe in this economic situation, someone cannot prepare what we recommend in his/her diet and so they cannot follow the prescribed diet.” (Nurse, 23 year of experience)
Negative and false beliefs can be a barrier to successful treatment adherence. One of the false beliefs of patients with HF in this study was that HF improves with time and they thought that HF could be cured.
A patient came to me and said, “I felt that I was cured and so I haven’t followed my treatment plan.” (Nurse, 23 year of experience)
On the other hand, some patients with HF think that they should not have any activity due to their disease and for this reason they do not adhere to their treatment plan in the field of exercise and activity as a behavior related to lifestyle modification.
“A lot of patients think that because of their heart problem they should not move and must completely rest. Based on this idea, they have no activity. The next time they come, if they have a problem, they say that I did not move from the house at all, so why did I become like this?!.” (Nurse, 8 year of experience)
Family is a source of social support. The stress and fatigue caused by long-term care and the dependence of patient with HF on their family caregivers have a negative effect on family support for the patient.
“Some patients do not receive support from their families. They do not come to visit on time or regularly and do not follow up their regular visits.” (Nurse, 26 year of experience)
Physical limitations
Our findings showed that patients with HF have physical limitations due to reasons such as age-related limitations, weakness and inability caused by the disease, and the existence of co-morbidities. These limitations have an effect on treatment adherence in terms of lifestyle modification.
“Some HF patients are young and have a lot of social activities and cannot be too limited. For example, when we say due to air pollution, you must stay home, they do not pay attention. Because they think that HF is more dangerous in the elderly, but most of them suffer from shortness of breath and become hospitalized.” (Nurse, 26 year of experience)
Findings from the participants’ experiences indicated that the majority of people with HF are old and this issue has an effect on lifestyle modification.
“HF patients are mostly old and physically disabled. They cannot be very active or take care of themselves and need the help of those around them; they are not able to do activities such as taking their medication or cooking and other tasks.” (Nurse, 8 year of experience)
Lack of self-care management knowledge and strategies
Exploring the participants’ experiences indicated that a lack of knowledge in people with HF is one of the deterrents of treatment adherence. One of the inhibitors identified in this field was the arbitrary discontinuation of the medication.
“Sometimes the doctor changes a patient’s medication based on the patient’s condition and prescribes a new medication for him/her. The patient decides not to take it anymore because they believe the new medicine bothers him/her or, for example, or he/she may not find it.” (Nurse, 23 year of experience)
Lack of an approach to be reminded of medication was another problem in the case of insufficient self-management knowledge. Lack of a reminder approach can lead to irregular use of medications and even forgetting the daily dose of medication.
“For example, in the morning if you take your medicine, you are OK, but when you postpone it, you see that you forgot and did not take any medicine. Of course, sometimes you may take your medicine and forget. It means you took your medicine, but you do not remember taking it.” (73 year male, NYHA III)
Participants’ experiences showed that lack of medication knowledge is another inhibitor of treatment adherence among people with HF.
“For example, some patients who take digoxin refer to us with digoxin poisoning. Because they did not know how to check their pulse rate at all. Or they should not take digoxin every day of the week or two days a week. They are not aware of the symptoms of digoxin poisoning, they used digoxin continuously, and now they come back with vomiting, severe diplopia, and seeing yellow spots; although there are signs of digoxin poisoning, they still think that they have a digestive problem and don't know anything about side effects of digoxin at all.” (Nurse, 8 year of experience)
Lack of knowledge, and inadequate and ineffective education are other deterrents to treatment adherence among HF patients.
“I do not know what foods are good foods to eat or what I should not eat. Nobody has provided me with any education in this regard. Now you are telling me what I should eat or not eat, I did not know this at all. For example, my wife just cooked vegetable rice yesterday, even though it was without salt, I ate it with a half can of fish.” (43 year male, NYHA III)
Discussion
This study aimed to explore the experiences of facilitators and inhibitors of treatment adherence in patients with HF. Based on our findings, the participants’ experiences were divided into two main themes, namely “the driving forces behind treatment adherence” and “the deterrent forces behind treatment adherence.” These results represented the facilitators and inhibitors with regards to treatment adherence in patients with HF.
In our study, a supportive family was identified as a driving force in treatment adherence in people with HF. Family can influence the success of the treatment program and the stability of changes in lifestyle-related behaviors among people with HF (Shahriari et al., 2013). Results of an integrative review study indicated that family-centered care improved knowledge, self-care management, medication adherence, and individual satisfaction (Marques et al., 2021). HF as a disease is chronic and disabling in nature and requires long-term care; therefore, the participation of family members and their support plays an important role in the management of people with HF because most people with HF live at home with other family members (Kitko et al., 2020; Shahriari et al., 2013). The results of another study indicated that support from family caregivers improved treatment adherence in people with HF (Wu et al., 2019). The results of a study by Silva et al. also showed that the rate of treatment adherence was higher in people with HF living with family than in people living alone (Silva et al., 2015), which is in line with the finding of the present study.
The present study revealed that positive personality characteristics such as self-responsibility and responsibility toward family, self-discipline, trust and reliance, acceptance and commitment, and motivation to learn about medications drive treatment adherence in people with HF. Siabani and colleagues propounded that placing trust in health care providers and having spiritual beliefs act as facilitators in adhering to the treatment of people with HF in a meta-synthesis qualitative study. After reviewing 23 articles, she reported that the impact of cultural issues, personal values, and acceptance of adherence to self-care behaviors as one of the main dimensions of HF treatment programs was controversial; thus, these factors can play both positive and negative roles in following self-care behaviors of HF (Siabani et al., 2013). In our study, participants pointed to the positive effects of these factors on treatment adherence. Based on findings in Herborg’s study, promotion in treatment adherence was associated with strong patient acceptance and participation in treatment, as well as the relationship between patients and health care providers (Herborg et al., 2008). Based on a study by Kamath et al., trust in health care providers was identified as a positive factor in adhering to a long-term treatment plan. Health care providers can build trust with patients and their caregivers by appropriate communication and involving them in self-care behaviors (Kamath et al., 2021). The results of these studies are in accordance with our findings.
Health literacy was another driving force to adherence to treatment in people with HF that was identified in the present study. Health literacy is defined as the degree to which individuals can obtain, process, and understand basic health information to be able to make health-related decisions through the ability to understand and interpret numbers, texts, and documents. Health literacy is a strong social component that is related to the ability of the individual to make fundamental decisions in taking responsibility for their health and ultimately how they use the necessary health care. People with low health literacy have difficulties with understanding the disease, reading brochures and medication labels, remembering to take medications and their dosage, and interpreting vital signs such as blood pressure and heart rate (Cabellos-García et al., 2020; Oscalices et al., 2019). In this regard, the results of a study also showed that low levels of health literacy are directly related to less treatment in people with HF (Oscalices et al., 2019). The results of this study were in line with those obtained from the experiences of the participants in the present study.
Based on the experiences of participants in the present study, negligence in people with HF was identified as, ignoring the treatment plan, inattention, stubbornness, inability to overcome dietary cravings, and non-adherence to dietary recommendations in parties. A grounded theory study in the field of treatment adherence in diabetic patients reports negligence as an unperceived threat in treatment adherence of diabetic patients (Mousavizadeh et al., 2018) which was consistent with the results of our study.
Herborg reported in her study that the majority of patients intentionally or unintentionally do not follow prescribed treatments. She identified experiences and mental feelings (such as negative emotions, lack of confidence in the health care system and staff, distrust of medications, misunderstandings, and negative experiences), which cause patients to intentionally not adhere to common medical advice. Unintentional non-adherence to treatment arises from forgetting or inattention and patients need help to implement their treatment regimen (Herborg et al., 2008). Careless consumption of food without considering the restrictions and non-adherence with medication can be due to a lack of awareness. The results of a study indicated that people with HF did not adhere to their medication and diet due to lack of awareness, eating habits, stubbornness, and fatigue from restrictions (Hekmatpou et al., 2009), which is congruent with the results of the current study. “Diet foods are often unpleasant for people because, symbolically, they are more likely to be eaten by people with illness than with family” (Farahani, qtd. in Thompson). Diet foods cause a person to feel isolated in society. On the other hand, patients think that they are allowed to eat high-fat and salty foods when they take medicines (Ashghaly Farahani M et al., 2008). Experiences of participants in our study also showed that tasteless and unpleasant taste of salt-free food, unawareness about salt restrictions in people with HF, fatigue from adhering to restrictions, lack of family companionship in following a low-salt diet, and feeling sick due to restrictions, are the other factors which inhibit patients from adhering to salt restriction in their diet.
Findings of the current study indicated that the majority of participants did not adhere to their treatment due to reasons such as frustration, depression, fears and concerns, fatigue, and clumsiness as deterrent psychological problems. Depression and frustration are the most common psychological problems in people with HF, which are related to factors such as dietary restrictions, medications’ use, smoking, feeling sick, insomnia, fatigue, loneliness, treatment costs, employment status, low income, the severity of HF, sexual dysfunction, low educational level, and age. Depression and frustration in HF are associated with adverse outcomes such as decreased treatment adherence, poor performance, increased hospitalization, and mortality. Depression and frustration can be a major challenge in treatment adherence of people with HF. For example, a depressed person adheres less to controlled diet, regular exercise, and intake of prescribed medications (Celano et al., 2018; Ferguson et al., 2017). Some studies reported that depression, anxiety, fatigue, comorbidities, and older age were among the deterrents of treatment adherence (Alosco et al., 2012; Dehghanzadeh et al., 2015). In another study, depression has been propounded as one of the barriers to self-care in HF patients (Negarandeh et al., 2021). The results of the above studies were consistent with our findings.
Fear and concern about the disease as well as uncertainty about the future can be deterrents to treatment adherence in people with HF. Fear and concern may have both positive and negative effects on people which can provide a great opportunity to motivate and change people with HF behavior. Some studies on individuals with chronic illnesses showed fear as an incentive to increase self-care recommendations. In this regard, the results of Zahmatkeshan’s study revealed that fear of COVID-19 led to improved self-care behaviors among people with cardiovascular disease (Zahmatkeshan et al., 2021). On the other hand, fear and concern, as one of the factors related to the patient, can be obstacles to treatment adherence in people with HF which led to delay in treatment, worsening its consequences, and also can be barriers to help-seeking behaviors in people with HF. It seems factors such as terminology of HF, diagnosis, treatment plan, child care, worsening of symptoms, death, medication use, exercise, uncertainty about the future, financial adequacy, and social support are associated with fear and concern in people with HF (Abshire et al., 2015; Breathett et al., 2020; Jankowska-Polańska et al., 2020; Kvarnström et al., 2018; Rashidi et al., 2020; Van der Laan et al., 2019). Results of some studies also showed that people with chronic conditions reduced or discontinued their medications due to fear of medication side-effects (Costantino et al., 2021). These results are in line with the results described in the present study. People with HF refused to engage in activity and exercise as a self-care behavior due to fear of experiencing the unpleasant symptoms of HF. Kvarnström et al. reported that economic problems and lack of support from family or others are among the cultural, social, and economic barriers to medical adherence of people with chronic conditions such as cardiovascular disease (Kvarnström et al., 2021), which are consistent with the result of the present study.
According to our knowledge, HF may lead to disability, job loss, and reduced income in patients. In the meantime, follow-up visits, lab tests, echocardiography, medications, diets, re-hospitalizations, and frequent transportation increase costs in HF patients. It seems that on the one hand, the decrease in income and on the other hand, the financial burden of care causes the ability of self-care to decrease in patients with HF; Therefore, due to financial problems, patients may prioritize some therapeutic measures and ignore some aspects of self-care such as diet. In previous studies, financial problems have been identified as one of the barriers to treatment adherence in chronic patients (Mousavizadeh et al., 2018; Negarandeh et al., 2021).
One of the inhibitors to lifestyle modification is false cultural beliefs. In the study by Negarandeh et al., some patients with HF believed that if they took their medications regularly, they would no longer need to adhere to their diet (Negarandeh et al., 2021). In another study, more than 40% of patients with HF had false beliefs about HF. One of the false beliefs of patients with HF in their study was that the disease improves with time and they thought that HF could be cured (Bozorgzad et al., 2021). The results of these studies confirm our findings. Patients with HF need to be supported by family caregivers to perform self-care behaviors. According to the experiences of the participants in the present study, the lack of family support as a source of social support was a deterrent force for treatment adherence. Poor family support is associated with poor patient self-care (Siabani et al., 2013). Our findings on these aspects were consistent with the results of some studies (Negarandeh et al., 2021; Rokhomah et al., 2020).
According to the experiences of our participants, the limitations and physical disabilities of individuals are deterrent forces to treatment adherence in people with HF, which is in line with the findings of a review study on qualitative studies (Kvarnström et al., 2021). In a study, progressive physical degeneration and comorbidity were among the identified barriers in the self-care behaviors of patients with HF (Negarandeh et al., 2021).
Knowledge alone is not enough to accept treatment but to accept a treatment regimen, a minimum knowledge about the disease and the treatment regimen is required (Ezzati, 2021). A review study on sodium restriction and adherence in people with HF indicated that interventions such as education and counseling to increase adherence of people with HF to sodium restriction were not successful (Najafi-Ghezeljeh & Akhondzadeh, 2016). Although patient education had many benefits, it is often overlooked in most medical centers. Patients received little information about the disease and how to take care of themselves at discharge (Kamrani et al., 2015). In some studies, the lack of self-care knowledge was identified as a barrier to self-care in HF which was consistent with our results (Negarandeh et al., 2021; Sezgin & Mert, 2017). According to the findings of the present study, people with HF were very concerned about their unawareness of the disease and it seems that usually, they did not have enough information to make knowledge-based decisions for self-management.
This study was conducted with a qualitative approach. Although, our results may reflect the experiences of patients with HF, their family caregivers, nurses, and HF fellowships, due to the small size of the sample, the generalization of the results is limited. On the other hand, the nature of treatment adherence is such that it should be investigated based on the existing context; therefore, the generalizability of the results is limited.
Limitations
The impossibility of using the experiences of nurses and physicians due to the high and unexpected workload following the Covid-19 pandemic, the inability of people with HF to visit the clinic due to the Covid-19 pandemic, and also the lack of access to diverse patients were among the limitations of our study.
Conclusion
Supportive family, positive personal characteristics, and having health literacy were identified as subthemes of the driving forces behind treatment adherence in people with HF. Factors such as negligence, psychological problems, cultural, social, and economic problems, physical limitations, and lack of self-care management knowledge and strategies were identified as subthemes of the deterrent forces behind treatment adherence in people with HF. Some of these deterrent forces identified behind treatment adherence are preventable. Paying attention to the psychological problems of people with HF, using the family potential in treatment adherence, and increasing awareness about medications and dietary restrictions can improve treatment adherence and clinical outcomes in people with HF. Adequate and correct knowledge about facilitators and inhibitors of treatment adherence can help develop the body of nursing knowledge, and help the nurses and other healthcare professionals improve the quality of care provided for patients with HF. Moreover, considering the nature and diversity of these identified facilitators and inhibitors, designing care programs can be effective in facilitating treatment adherence among patients with HF. Therefore, it is recommended to design programs in future studies based on current findings to improve treatment adherence in patients with HF.
Footnotes
Acknowledgements
The authors thank Tehran University of Medical Sciences for supporting this research project. We would appreciate the participants of this study, officials of Tehran Heart Center and Heart Failure Clinic.
Authors Contributions
Authors SFGH, EN, and MACH designed the study, and HP, AKH, KHS, HN, MKH, MD, and ME approved the study design. SFGH collected the data, and analyzed and interpreted the data first. All authors were involved in the final interpretation of the data. SFGH prepared the manuscript. All authors critically reviewed the manuscript and approved the final version for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Tehran University of Medical Sciences (Grant No: 46079).
Ethical Approval
This study received ethics approval from the Organizational ethics committee of the School of Nursing and Midwifery and the School of Rehabilitation – Tehran University of Medical Sciences (Ethics Code: IR.TUMS.FNM.REC.1398.174).