
Abstract
Chronic kidney disease (CKD) has considerable effects on the quality of life of female patients. Receiving the diagnosis and beginning renal replacement therapy (RRT) has a great personal impact on patients. The purpose of this study was to describe the experience of female patients with CKD at an ambulatory dialysis unit regarding diagnosis, life changes, and initiation of RRT. A qualitative exploratory study was conducted based on a social contructivism framework. Participants were recruited using purposeful sampling. In total, 18 women who received treatment for CKD with RRT were included. The women were attending the Ambulatory Dialysis Unit at a hospital belonging to the public health system of Madrid (Spain). Unstructured and semi-structured in-depth interviews, researchers’ field notes, and women’s personal letters were used. A systematic text condensation analysis was performed. The criteria used to control trustworthiness were credibility, transferability, dependability, and confirmability. Two themes emerged from the data: (a) A turning point in their lives, and (b) The emotional journey of beginning RRT. The diagnosis of CKD and the beginning of treatment implies changing routines and adapting to a new life with CKD. The first dialysis and puncture of the arteriovenous fistula is a major experience. Support from other CKD patients with more experience is perceived as a necessity and a tool to share their experiences and resolve doubts among peers. The diagnosis and initiation of RRT leads to numerous changes in the lives of women with CKD, which may influence the acceptance of treatment.
Introduction
Background
Chronic kidney disease (CKD) is a public health problem (Glassock et al., 2017) related to highly prevalent diseases, such as arterial hypertension, diabetes, or cardiovascular disease (Llisterri et al., 2021). It is associated with a high morbimortality that increases healthcare costs (Cockwell & Fisher, 2020; Song et al., 2018). CKD affects kidney function, causing alterations in the elimination of waste substances, control of homeostasis, regulation of blood pressure, and hormone production (erythropoietin, active metabolites of vitamin D, prostaglandins) (Kalantar-Zadeh et al., 2021).
Once established, CKD progresses to more advanced stages, with renal replacement therapy (RRT) being the only effective life-sustaining treatment (Dąbek et al., 2023). Within RRT there are two variants: dialysis through hemodialysis (HD) or peritoneal dialysis (PD); and kidney transplantation (Tx) (Kramer et al., 2018). The objective of RRT is the removal of low and high molecular weight molecules and excess fluid from the blood that would normally be eliminated via the kidneys, and the regulation of the intra- and extracellular milieu (Álvarez-Villarreal et al., 2019). For HD and PD, the blood is filtered through a membrane to purify the blood of metabolites and toxic products and excess fluid (Woo & Lok, 2016).
Impact of RRT
CKD has a great emotional impact on patients and their families (Frandsen et al., 2023), together with the emergence of physical and psychological disorders (Hiramatsu et al., 2020). CKD can make people fragile, disrupt their lives, and interrupt their future projects (Subramanian et al., 2017). Moreover, it is a disease that has a prolonged symptomatology requiring a great effort of adaptation on behalf of the patient (Chen et al., 2022). Both treatments (HD and PD) require surgical vascular access and a dialysis machine (Woo & Lok, 2016). HD requires an arteriovenous fistula (AVF) or central venous catheter (CVC), and PD requires a peritoneal catheter (Woo & Lok, 2016). In the case of HD, the patient is connected for 3 to 4 hr a day, several days a week, according to medical prescription at home or at a health center; whereas PD is performed several times a day by the patients themselves, a family member, or a nurse (See et al., 2018).
Experiences When Initiating Treatment
Patients with advanced CKD acknowledge that the news of needing RRT and beginning treatment comes as a great shock (Kerr et al., 2018). Previous studies have identified how during preparation for the start of RRT they experienced fear, remorse, anger, uncertainty, and emotional distress, being aware of the irreversibility of the disease and facing the different types of treatment and/or dialysis modality (HD or PD) (Liu et al., 2023; Thorsteinsdottir et al., 2022). Unmet needs for care arise during the process of initiating RRT (McKie et al., 2023) such as a lack of sufficient informational support from health professionals or not feeling involved in the decision-making process regarding their treatment (Årestedt et al., 2019), nor on the choice of vascular access (Elliott et al., 2023).
Once on dialysis, patients may feel a loss of identity and control over their lives, increasing their sense of vulnerability (Damery et al., 2019), together with loss of autonomy (Wongboonsin et al., 2021). Coping with treatment and illness involves incorporating new strategies such as seeking support from loved ones (Montalescot et al., 2023), taking refuge in faith, letting go of negative or pessimistic thoughts, and finding one’s own strength (Stoye et al., 2022). RRT involves a change in patients’ lives, forcing them to abandon habits and incorporate new ones depending on the treatment (Filgueiras de Assis Mello & Angelo, 2018; Sedin et al., 2023).
Gender and RRT
Among women, there are numerous differences regarding clinical presentation, disease tolerance and response to treatment, compared to men (Cobo et al., 2016). These differences include: (a) an increase in the number of hospitalizations and erythropoietin prescriptions in women compared to men (Chesnaye et al., 2024), (b) increased risk of mortality due to the fact that women with RRT have a higher body mass index and greater obesity (Barrera et al., 2023), (c) AVF, associated with improved survival, is used more frequently in men, whereas CVC use is more common in women (Artan et al., 2016), (d) women initiate RRT later (Kovesdy, 2022), (e) women are less likely than men to receive a kidney transplant (Adoli et al., 2024), and (f) women have a poorer health-related quality of life, a higher percentage of depressive symptoms and a higher symptom burden (Beckwith et al., 2022; Da Silva et al., 2023). However, women with RRT have a more favorable prognosis because more effective dialysis is achieved by reaching higher Kt/V values (Chen et al., 2023), also, they have better dietary compliance and/or adherence to phosphorus chelating drugs (Carrero et al., 2018). In addition, for young women, living with CKD is especially challenging as the treatment has effects on fertility (Mc Laughlin et al., 2022; Shah et al., 2023), weight gain, acne, stretch marks, and hair loss that alter their appearance and can lead to decreased self-esteem (Beanlands et al., 2020).
Therefore, it is essential to know the perspective and needs related to disease diagnosis and treatment in women, to understand health-related behaviors, and to incorporate the results into clinical practice (Brar & Markell, 2019). Through the integration of gender into CKD research and management, new therapeutic targets may be identified, current treatment options may be improved, and better support could be provided during disease and decision making (Brar & Markell, 2019). The purpose of this study was to describe the experience of female patients with CKD at an ambulatory dialysis unit regarding diagnosis, life changes, and the initiation of RRT.
Methods
Design
A qualitative study based on an interpretive framework was conducted (Creswell & Poth, 2018). Within interpretive frameworks there are different types, such as postpositivism, social constructivism, transformative frameworks, postmodernism, and pragmatism. In this study, we used social constructivism, which describes how individuals seek to understand the world in which they live and work, constructing and giving meaning to their experiences. Therefore, the aim of this theoretical framework was to study and understand the participants’ perspectives on events and phenomena they experience first-hand (Creswell, 2007). This study was conducted according to the Standards for Reporting Qualitative Research (O’Brien et al., 2014) and the Consolidated criteria for reporting qualitative research (Tong et al., 2007).
Research Team
Prior to the study, the researchers’ positioning was established via two briefing sessions addressing the theoretical framework for the study, their beliefs, and their motivation for the research (Carpenter & Suto, 2008). The results of these sessions were: (a) Theoretical framework: researchers based their approach on an interpretivist paradigm, specifically the social-constructivist theoretical framework. This paradigm was based on the assumption that human beings construct their own social reality, and that knowledge is built through increasingly nuanced reconstructions of individual experiences; (b) beliefs: the diagnosis and treatment of CKD has a major impact on women’s health; however, currently their care is equal to that received by men and gender differences are not considered; and (c) Motivation for the research: to gain insight into CKD through the first-hand experience of female patients; to describe and understand female patients’ point of view regarding aspects which they consider relevant in the diagnosis and initiation of therapy and, as a result, improve healthcare services
Six researchers (three women) participated in this study, including one clinical nurse, a physiotherapist, an occupational therapist, and a two research nurses. Three of them had experience in qualitative study designs, and in health science research. None were involved in clinical activity, nor did they have any prior relationship with the patients included. One researcher had clinical experience with CKD.
Setting and Participants
The study included CKD female patients attending the Ambulatory Dialysis Unit at a hospital belonging to the public health system of Madrid (Spain). In this unit, RRTs are applied, such as HD, kidney transplant, or PD. The inclusion criteria were: (a) female patients; (b) over the age of 18; (c) diagnosed with CKD, following the criteria of Kidney Disease Improving Global Outcomes (Stevens et al., 2013); and (d) women who were receiving or had received RRT. The exclusion criteria were: (a) acute kidney disease requiring HD, (b) serious psychiatric or cognitive disorders, and (c) inability to communicate in Spanish or provide informed consent.
Purposive sampling was used, based on relevance to the research question (Sebele-Mpofu, 2020). Sampling and data collection was pursued until the researchers achieved information redundancy, at which point no new information emerged from the data analysis (Moser & Korstjens, 2018; Sebele-Mpofu, 2020). In our study, this situation occurred after including 18 women.
Data Collection
The first stage of data collection (participants 1–5) consisted of unstructured interviews using open questions. During the interviews, the researchers listened carefully, noted the key words and topics identified in the participants’ responses, and used their answers to ask for and clarify the content. In this manner, relevant information was collected from the perspective of the women. After the unstructured interviews, a first analysis was conducted. After this, it was necessary to deepen and understand relevant topics that appeared and required further study. This justified the need for a second stage of data collection. The second stage (participants 6–18) consisted of semi-structured interviews based on a question guide to obtain information regarding specific topics of interest (Table 1) (Moser & Korstjens, 2018). The semi-structured question guide was constructed based on the analysis of the first five interviews, thus reflecting relevant aspects to be investigated from their perspective. The time elapsed between each stage of data collection was 2 months. The second stage began once the first stage was completed.
Unstructured and Semi-Structured Interview Guide.
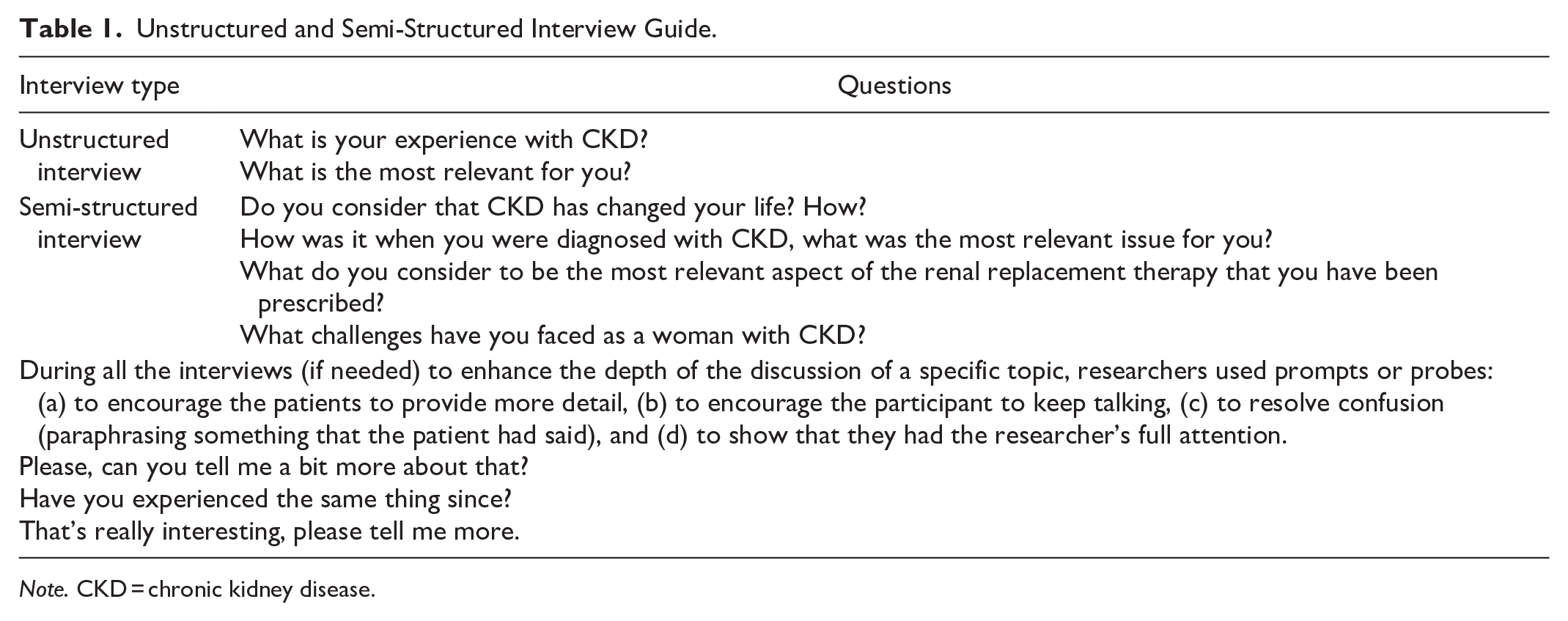
Note. CKD = chronic kidney disease.
The interviews were video-recorded and transcribed verbatim. The transcripts were returned to participants for comments and corrections. A total of 18 interviews with 18 researcher field notes were undertaken. One interview was collected per participant.
There was no repeat interview per participant and no participant dropout during the study. After the interviews, the participants were asked if they had any document in which they had written down their experiences since the onset of the disease, and if so, if they wished to share it to further enhance the study. No specific instructions were given for the elaboration of these written notes. Only participant 2 reported having a diary and agreed to share part of it, transcribing and copying those parts that she chose to share.
During the interviews, only the researcher and the participant were present. Overall, 1,210 min of interviews were recorded. Of these, 450 min corresponded to the first stage and 760 min corresponded to the second stage. All interviews were conducted at the participants’ homes or in a private hospital room, according to the women’s preference. Researcher field notes and personal letters provided by the women were also collected.
Analysis
Complete verbatim transcripts were produced for each of the interviews, researcher field notes, and letters. The texts were collated to enable qualitative analysis (Moser & Korstjens, 2018). A systematic text condensation (STC) analysis was performed (Malterud, 2012). This descriptive approach presents the experience of the participants as expressed by themselves; thus, STC represents an explorative proposal to present vital examples from peoples’ life worlds (Malterud, 2012). STC includes four steps of analysis: (a) total impression; reading all the material and an overview of the data. (b) identifying and sorting meaning units and codes; systematically reviewing the transcript line by line to identify meaning units. A meaning unit is a text fragment containing some information about the research question. Subsequently, decontextualization begins, which includes identifying, classifying, and sorting meaning units and marking these with a code—a label that connects related meaning units into a code group. (c) Condensation—from code to meaning; involving the systematic abstraction of meaning units within each of the code groups established in the second step of analysis. Empirical data are reduced to a decontextualized selection of meaning units sorted as thematic code groups across individual participants. (d) Synthesizing—from condensation to descriptions and concepts; data are reconceptualized, putting the pieces together again. By synthesizing the contents of the condensates, descriptions and concepts are developed, providing stories that reflect the participants’ experiences (Malterud, 2012). Each of the interviews were analyzed separately, without performing any comparison between one and the other. After analyzing each interview, each researcher listed their themes. Finally, in the case of different opinions, theme identification was decided by consensus. No qualitative software was used on the data.
Rigor Criteria
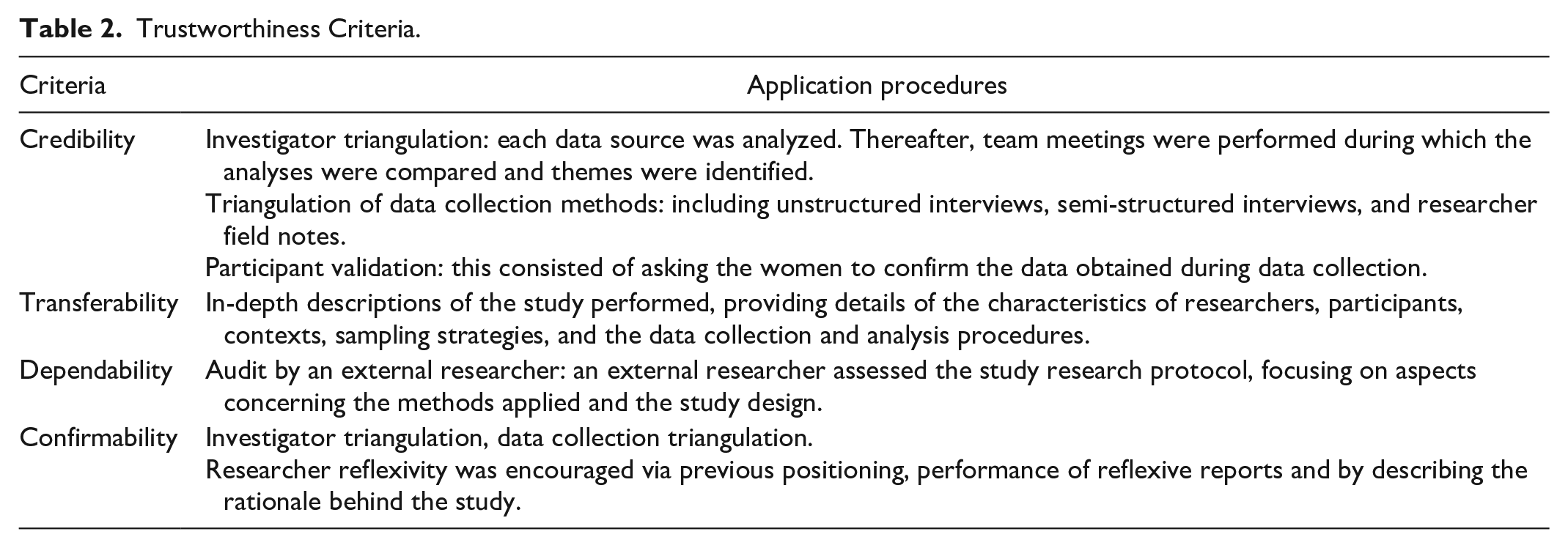
The Guba and Lincoln criteria for guaranteeing trustworthiness were followed (Korstjens & Moser, 2018). The techniques performed are described in Table 2 (Korstjens & Moser, 2018; O’Brien et al., 2014).
Trustworthiness Criteria.
Ethics/IRB Statement
The study was approved by the Local Ethical Committee at Rey Juan Carlos University (code: 2806201711017), and the Clinical Research Ethics Committee of Hospital Universitario Puerta de Hierro Majadahonda (code: 11.17). The participants were informed of the objective of the study and the reasons for doing the research. All participants gave their informed consent before inclusion.
Results
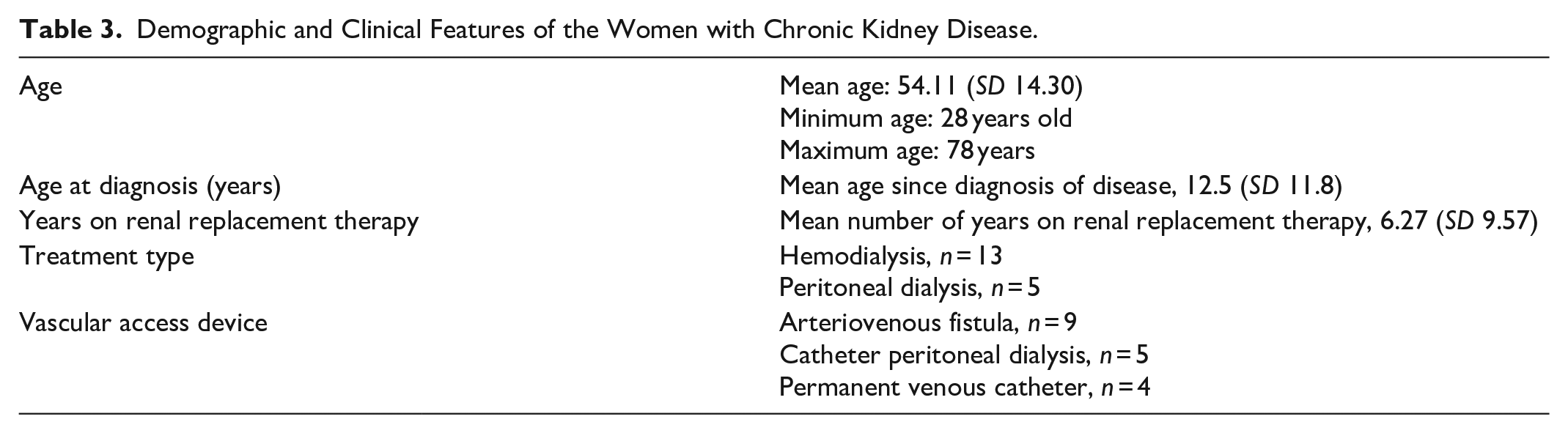
The sample consisted of 18 women. The mean age was 54.11 (SD 14.30). The mean number of years since disease diagnosis was 12.5 (SD 11.8), and the mean number of years on RRT was 6.27 (SD 9.57) (Table 3). Two themes emerged from the data: (a) a turning point in their lives, and (b) the emotional journey of beginning RRT. We included some of the women’s narratives taken directly from the interviews in relation to the emerging themes (Table 4).
Demographic and Clinical Features of the Women with Chronic Kidney Disease.
Narratives from Female Participants with Chronic Kidney Disease
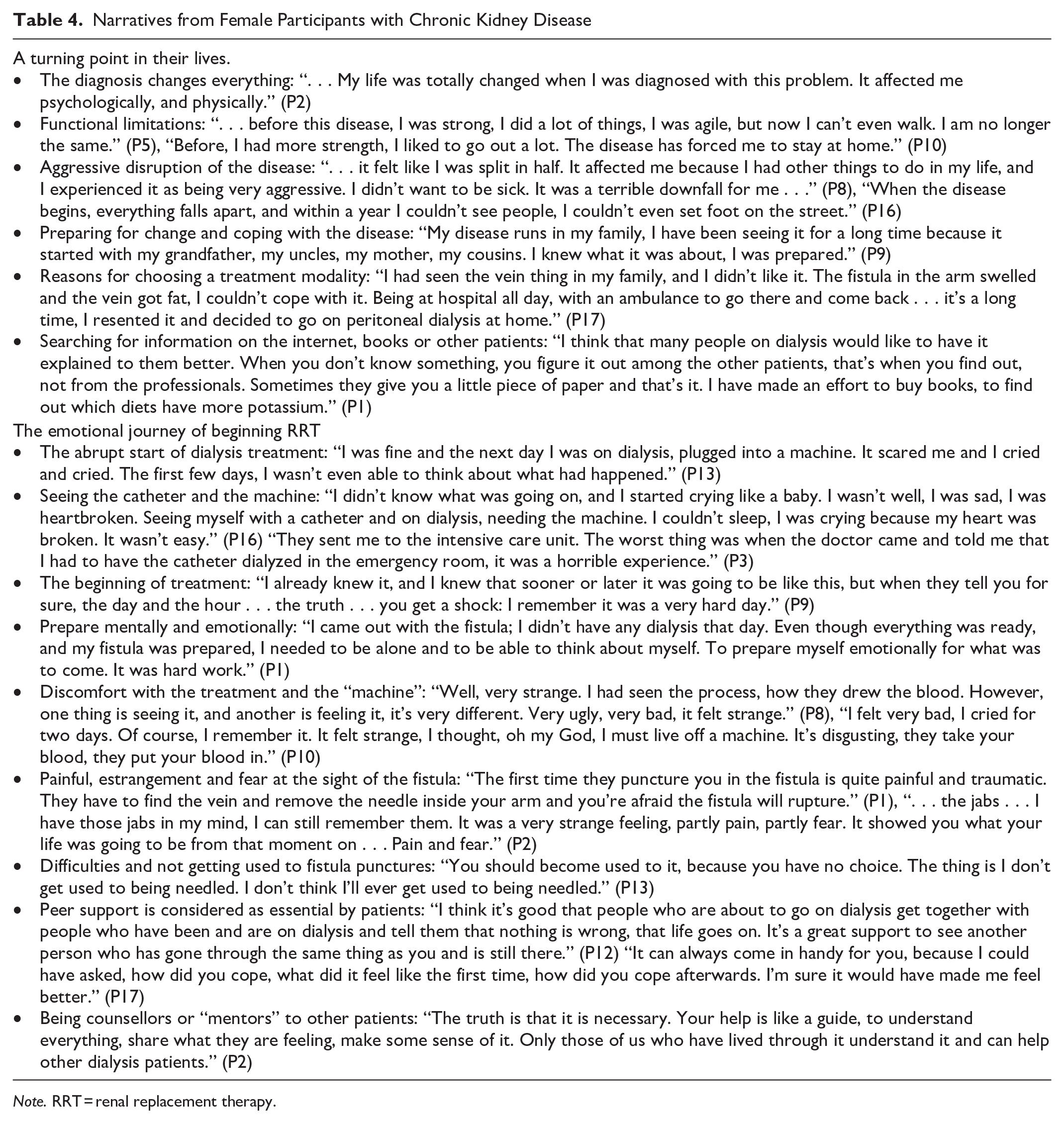
Note. RRT = renal replacement therapy.
A Turning Point in Their Lives
The CKD diagnosis marked a turning point, provoking an abrupt change in the lives of the women interviewed. All participants related that the diagnosis resulted in a break from their former lifestyle, resulting in numerous physical and psychological changes, forcing them to adapt to a situation that imposed new rules on them. The women’s narratives highlighted the progression of the disease, which caused a direct impact in the physical and functional dimension. They described loss of strength, muscle decline, fatigue, loss of energy, and vitality, leading to significant limitations. After the diagnosis, the women felt that their life was torn apart. In the narratives, the emotional impact of receiving the CKD diagnosis was described. The chronic nature of the disease was experienced with a sense of “permanence,” “for life,” which caused a drastic change in their world. This forced them to modify their life projects and to adapt to losses derived from the disease. The women who had previous contact with the disease and/or with people or loved ones with CKD responded more quickly. Upon the diagnosis, after the shock of the news, they began to organize their lives to cope with the disease. In addition, having had previous contact with the disease at the time of diagnosis can influence the choice of treatment modality. Thus, participant 17 described how living with a relative with AVF and daily in-center dialysis made her decide on another treatment modality.
For the women, one of the key aspects influencing their coping with the disease was the relationship with the healthcare professionals at the dialysis unit, the information and preparation provided, together with the support received during the disease. Faced with a lack of information from professionals, participants decided to seek information from the Internet, books, or other patients, instead of asking for clarification.
The Emotional Journey of Beginning RRT
Once the diagnosis was given, RRT began. The beginning of treatment was a crucial moment of great impact. The experience was different when it was a scheduled treatment (there was time to prepare) compared to whether it was implemented suddenly. Thus, participant 13 recounted how she experienced the abrupt start of her dialysis treatment. The women who abruptly began treatment described it as a horrible experience. They recounted how from 1 day to the next, they found themselves connected “to a machine” without knowing what it did, and with a high-flow vascular access, without enough time to assimilate it. In the case of scheduled RRT, although patients have more time to prepare, the moment patients are told that they will begin RRT, they still find it challenging and difficult to accept. Many women, despite knowing that it will come 1 day, hoped that it would not materialize. Conversely, participant 1 described how the time required by the professionals to construct and prepare her AVF in her arm to administer dialysis helped her to prepare mentally and emotionally. Regardless of the type of treatment, the women described a series of sensations, emotions, and feelings that they experienced during the first dialysis sessions, including fear, sadness, anger, pain, surprise, uncertainty, frustration, the feeling of being trapped, the awkwardness of the catheter, of being connected to the machine, the unfamiliarity of the treatment and “blood purification,” reported as “traumatic” experiences. The narratives of two of the women (P8 and P10) highlight their feelings of unease regarding the treatment and the “machine.” Moreover, women with CKD with HD, recalled their experience with the first AVF punctures in detail. They narrated how it was painful, accompanied by a sense of estrangement at the sight of the fistula, along with fear. Over time, despite the continuous need to administer RRT, many women reported that they continued to have difficulties and had not yet gotten used to the fistula punctures. The women described the importance of receiving support throughout the treatment, emphasizing the support received from other patients who had experienced or were still undergoing RRT, enabling them to share their experiences, fears, and insecurities. The women described their desire to become counselors or “mentors” to other patients, highlighting two essential messages for future patients: (a) the disease must be accepted as part of life, (b) encouragement to continue with treatment, and (c) an opportunity to continue living despite the seriousness of the disease.
Discussion
Our results show that the diagnosis of CKD marked a turning point in the lives of our participants. Previous studies on the meaning of RRT have described this change as a “life metamorphosis” (Gullick et al., 2017). This term refers to the transformation that appears in the daily life of people and in their physical and emotional dimensions, when they are diagnosed with CKD (Filgueiras de Assis Mello & Angelo, 2018). After diagnosis, patients are faced with a new reality (Stavropoulou et al., 2020). New habits and routines are incorporated, lifestyles are changed, and they begin to adapt to a new life conditioned by the disease (Stavropoulou et al., 2020). These changes include dietary requirements, frequent contact with the hospital environment and interruption of daily activities that affect work or studies (Stavropoulou et al., 2020). Learning to cope with the disease and the new challenges that arise is a long process that requires patients to be patient and persevere in the face of difficulties (Ghaffari et al., 2019). This is not something that can be achieved overnight (Ghaffari et al., 2019). When these changes occur suddenly, in relation to diagnosis and urgent treatment, patients feel that their whole world is shaken (Ghaffari et al., 2019; Lin & Chu, 2022).
Previous qualitative studies on the impact of CKD in women describe how the disease influences the experience of motherhood, becoming pregnant, and childcare, triggering changes in the self-perception of their body and sexuality (Alvarez-Villarreal et al., 2021). Álvarez-Villarreal et al. (2019) described how the catheter and the fistula caused alterations in the body image and sexuality of women with CKD. Thus, patients perceived their bodies as swollen or deformed. In addition, women changed the way they dressed, in an attempt to hide the catheter and/or fistula and reported how the presence of catheters and/or AVF was uncomfortable during sexual relations.
The initiation of RRT is an important change in the life of the CKD patient; therefore, an adequate adaptation is necessary to achieve a good health-related quality of life (Fuertes et al., 2017; Sousa et al., 2023). Our participants recounted the difficulties faced to adapt to the treatment. They were not used to this new routine in their life. Previous studies (Schrauben et al., 2021; Stavropoulou et al., 2020) highlight contradictions in the self-care of patients with CKD, due to erratic and irregular compliance with professional recommendations because it was difficult for patients to change their previous habits and routines.
The experience of the participants in the present study is marked by the first dialysis sessions and the first AVF punctures. In previous studies (Griva et al., 2019; Kopple et al., 2017), patients described their first dialysis session as a process that was hard, long, and insidious. The beginning of dialysis treatment brings an end to their dreams, and their professional, social, and personal activity.
In the presence of fear, uncertainty and the emotional impact of the treatment and the changes derived from it, previous studies show that it is necessary to establish educational programs for patients and family members, where they can reflect on the perceived difficulties (Díaz-Medina & Guerreiro-Vieira-da-Silva, 2020). It is key to provide comprehensive, concise education on a regular basis, encouraging patient motivation and participation in their self-care (Al Rahbi & Al Salmi, 2020; López-Vargas et al., 2016). This education should lead patients to modify their behaviors and help them to adopt new life habits that will enable them to control their thoughts, feelings, motivations, and actions (Al Rahbi & Al Salmi, 2020).
Furthermore, to incorporate a comprehensive perspective of CKD care, it is necessary to incorporate the patients themselves as agents of change and with a voice within the collective spaces of care and health promotion (López-Vargas et al., 2016). Haldar et al. (2017) showed that the strategy of “learning from the experience of others” with people who share a similar life situation is effective for behavioral changes and educational processes. Our participants demand the help of other patients with whom to share experiences and clarify the uncertainties that arise as CKD patients. Patient-led hospital mentoring programs help to incorporate the community into healthcare strategies and provide emotional support in long-term illnesses (Ghahramani et al., 2021).
The experience of peer support in CKD, as an educational tool in hospital teams, covers patient needs that are not usually addressed, such as the emotional dimension (García-Llana et al., 2019; Ghahramani et al., 2021). In addition, it offers an opportunity for patients to share their difficulties and concerns with others regarding the challenges of CKD (Enriquez & Conn, 2016; Ghahramani et al., 2021). There are other initiatives regarding peer-to-peer support and mentoring that are effective for promoting adherence to pharmacological treatment, through social support networks, the use of Internet discussion groups and peer-led interventions (Enriquez & Conn, 2016).
The involvement of chronic patients in the exchange of information and support for patients with chronic diseases has a positive influence on coping strategies, helping patients to feel more hopeful by sharing their real-life experiences (Enriquez & Conn, 2016). In CKD, the use of peer mentors leads to improved quality of life for patients, resulting in patient-centered care, anxiety relief, reduced feelings of isolation, and improved adherence to self-care (Ghahramani et al., 2021).
The limitation of the present study is that it only includes women; therefore, we cannot determine whether the experiences described in the paper are unique to them or whether men have similar experiences. Future research should incorporate both perspectives or address the experience of male patients. In addition, gender roles should be taken into account when considering concealment of disease, as underlying differences due to gender may influence the disease experience and how it affects daily life (Tong et al., 2015). Indeed, our results cannot be extrapolated to the whole population with CKD; however, they can most likely be applied to other contexts with similar characteristics (Creswell & Poth, 2018).
Conclusions
The diagnosis of CKD and the initiation of treatment marks a profound change in the lives of women with CKD. It involves a change of routines and habits and an adaptation to their new life with CKD. The first dialysis and the use of AVF puncture is an experience that marks the lives of women with CKD. The presence of support from other patients in similar situations, and/or who have more experience is perceived positively as a necessity, and a way to share their experiences and resolve their doubts and treatment uncertainty treatment among peers. Women with CKD should receive more information and education on aspects such as the AVF and the RRT application process.
Relevance for Clinical Practice
The results this study could be applied to establish peer mentoring programs among CKD patients in dialysis units and would enable the establishment of collaborations between healthcare centers and CKD patient associations. Care programs should take gender into account by providing care that is specifically focused on women, given the impact of CKD diagnosis and treatment.
Footnotes
Acknowledgements
The research team would like to thank the women who participated in this study for sharing their experiences.
Author Contributions
M.A.-V.: investigation, methodology, formal analysis, writing—original draft preparation; J.F.V.-G.: conceptualization, formal analysis, writing—review and editing; A.S.M.-G.: conceptualization, formal analysis, writing—review and editing; S.M.G.-S. and A.G.-C.: conceptualization, resources, writing—review and editing; D.P.-C.: conceptualization, investigation, formal analysis, funding acquisition, writing—original draft preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.