
Abstract
Neutropenic sepsis (NS) is one of the leading causes of death among patients with hematologic malignancies. Identifying its predictive factors is fundamental for early detection. Few studies have evaluated the predictive factors in relation to microbial infection confirmation, which is clinically important for initiating sepsis treatment. This study aimed to determine whether selected biomarkers (i.e., body temperature, C-reactive protein, albumin, procalcitonin), treatment-related characteristics (i.e., diagnosis, duration of neutropenia, treatment modality), and infection-related characteristics (i.e., infection source, causative organisms) can predict NS in patients with hematologic malignancies. We also aimed to identify the optimal predictive cutoff points for these parameters. This retrospective case–control study used the data from a total of 163 patients (58 in the sepsis group and 105 in the non-sepsis group). We collected data with reference to the day of specimen collection, with which microbial infection was confirmed. Multiple logistic regression was used to determine predictive risk factors and the area under the curve (AUC) of the receiver operating characteristic for the optimal predictive cutoff points. The independent predictors of NS were average body temperature during a fever episode and procalcitonin level. The odds for NS rose by 9.97 times with every 1°C rise in average body temperature (95% confidence interval, CI [1.33, 75.05]) and by 2.09 times with every 1 ng/mL rise in the procalcitonin level (95% CI [1.08, 4.04]). Average body temperature (AUC = 0.77, 95% CI [0.68, 0.87]) and procalcitonin levels (AUC = 0.71, 95% CI [0.59, 0.84]) have fair accuracy for predicting NS, with the optimal cutoff points of 37.9°C and 0.55 ng/mL, respectively. This study found that average body temperature during a fever episode and procalcitonin are useful in predicting NS. Thus, nurses should carefully monitor body temperature and procalcitonin levels in patients with hematologic malignancies to detect the onset of NS.
Keywords
Introduction
Neutropenic sepsis (NS), also known as febrile neutropenia, is a critical emergency that occurs during the treatment of hematologic malignancies (Kochanek et al., 2019). NS is particularly prevalent in hematologic malignancies (Alali et al., 2021; Ko et al., 2015; Tau et al., 2019). NS is associated with elevated mortality rates and increased healthcare costs (Awad et al., 2021; Kochanek et al., 2019).
NS is the development of sepsis in a neutropenic state (Zac, 2011). Sepsis is the pathological outcome of infection, defined as “life-threatening organ dysfunction caused by a dysregulated host response to infection” (Singer et al., 2016). Diverse immunological mediators (e.g., cytokines, platelet-activating factor) are involved in sepsis pathogeneses, resulting in endothelial dysfunction, altered coagulation and cell function, and cardiovascular dysfunction (Evans, 2018). Due to the lack of a unique molecular signature to diagnose sepsis, clinicians largely rely on clinical features using qSOFA criteria (respiratory rate ≥ 22/min, Glasgow Coma scale < 15, systolic blood pressure < 100 mmHg; Evans, 2018).
Patients in a neutropenic state can be easily infected and are likely to progress to NS; yet not all infected neutropenic patients develop NS. Thus, it is essential to detect the patients at risk for progressing to NS among those with infection at a clinically relevant time point. The time point of infection confirmation is clinically relevant to initiate sepsis intervention. However, limited studies have investigated the predictors at this time point; most studies have collected data in association with an NS diagnosis (Frazer et al., 2019; Islam et al., 2019).
Also, NS may differ from general sepsis in clinical characteristics (Reilly et al., 2016), and hematologic malignancies differ from solid tumors in their pathological processes and treatment modalities. Yet, studies that accurately reflect NS characteristics in hematologic malignancies are limited as studies often do not distinguish between solid and hematologic malignancies or between general sepsis and NS.
Findings from previous studies highlight possible predictors (biomarkers, treatment-related, infection-related characteristics) and assessment time points/methods that should be considered in examining NS in hematological cancer. Many studies have reported body temperature as a predictor of sepsis, including NS. However, the reported predictive cutoff for body temperature and its relative predictive power varied across studies (e.g., 37.5, 37.9 38.5, and 39°C; Alali et al., 2022; Hakim et al., 2010; Rondinelli et al., 2006; Warnock et al., 2018). Such variations may be due to the differences across studies in the timing and type of temperature assessment: the highest temperature measured at home before hospital arrival (Warnock et al., 2018); the highest temperature during fever (Alali et al., 2022; Hakim et al., 2010); and average temperature over 3 days prior to sepsis diagnosis (Frazer et al., 2019). Thus, the predictive cutoff and clinical implications of body temperature should be re-evaluated in considering the best suitable timing (e.g., at fever onset vs. infection confirmation) and type (e.g., highest vs. average temperature) of temperature assessment for patients with hematological malignancy.
Other biomarkers, such as C-reactive protein (CRP), albumin, and procalcitonin, are reportedly important indicators for sepsis development, diagnosis, and prognosis (Gradel et al., 2020; Tan et al., 2019). However, there were concerns about applying these markers in patients with cancer and with neutropenia. For instance, CRP levels may rise owing to the inflammatory response to cancer cells and treatments. Procalcitonin levels may also rise owing to complications from hematopoietic stem-cell transplantation (e.g., graft-vs.-host disease, veno-occlusive disease) and specific drug therapies (e.g., T-cell antibody anti-thymocyte globulin) (Massaro et al., 2014). Serum albumin levels reflect both nutritional and inflammatory status; thus, using this marker alone remains controversial (Gradel et al., 2020; Wu et al., 2018). Recently, CRP–albumin ratio, rather than albumin level per se, was proposed as a potentially useful predictor of general sepsis (Wang et al., 2022). Therefore, additional research is needed to ascertain the usefulness of CRP, CRP–albumin ratio, and procalcitonin to predict NS in patients with hematologic malignancies and to determine which is most clinically significant.
Studies suggest that treatment-related characteristics (diagnosis, recurrence, treatment modality, length of stay [LOS], duration of neutropenia, number of invasive devices) may contribute to NS development. For instance, higher NS prevalence rates are observed in patients with leukemia and non-Hodgkin’s lymphoma (Bou Chebl et al., 2021). Patients with relapsed hematologic malignancies often exhibit severe bone marrow suppression owing to repeated high-dose chemotherapy, increasing the risk of NS (Avilés-Robles et al., 2022; Sano et al., 2017). Although studies including patients with solid tumors have reported treatment modality (stem cell/bone marrow transplantation, chemotherapy, radical radiotherapy) as the factor associated with general sepsis (Te Marvelde et al., 2020), the relative contributions of various treatment methods for hematologic malignancies remain unclear. LOS (Ahiawodzi et al., 2020; Prescott et al., 2015), neutropenia duration (Alali et al., 2021), and the number of invasive devices (Ahiawodzi et al., 2020; Bennett et al., 2018) were reported as associated with the risk of infection or sepsis. Their effect on NS in hematologic malignancies should be further investigated.
Regarding infection-related characteristics, respiratory infection is the most common infection source leading to NS in cancer patients (Na et al., 2022). However, the incidence of catheter-related infection is higher in patients with hematologic malignancies (Bou Chebl et al., 2021; Garrido et al., 2019). Infections caused by multiple bacterial strains are associated with a higher incidence of sepsis and sepsis-related mortality (Facchin et al., 2022). Hence, further clarification is needed regarding the criticality of different infection sources and multiple bacterial strains (vs. single bacterial strain) in NS in hematologic malignancies.
This study, therefore, aimed to examine (a) whether the selected biomarkers (body temperature, neutrophil count, CRP, albumin, CRP–albumin ratio, procalcitonin), treatment-related characteristics (diagnosis, history of recurrence, neutropenia duration, treatment modality, LOS, number of invasive devices), and infection-related characteristics (infection source, number of causative organisms) can predict NS in patients with hematologic malignancies and (b) the optimal cutoff values for these biomarkers.
We assessed the potential predictive factors on the day of specimen collection, with which microbiologically defined infection (MDI) was confirmed. The comparison group was patients with neutropenia who developed microbial infections but did not progress to sepsis (referred to non-NS group). This helped us identify the predictors of those patients who are more likely to progress to sepsis after infection. These considerations make our study design unique.
Methods
Study Design, Sample, and Setting
For this retrospective case–control study (NS group vs. non-NS group), data were collected from the electronic medical records of patients treated at a university hospital in Seoul between March 1, 2017 and February 28, 2018. This hospital is Korea’s largest institution for treating hematologic malignancies, performing 25% of hematopoietic stem-cell transplantations.
For the NS group, the inclusion criteria were (a) currently undergoing inpatient treatment in the selected departments (hematology, hematology infectious diseases), (b) adult patients diagnosed with hematologic malignancies (age ≥ 19), (c) MDI with at least one clear pathogen in any specimens (positive in ≥2 sets, considered positive in case blood culture), (d) neutropenia (defined as absolute neutrophil count less than 1.0 × 109/L), and (e) diagnosis of sepsis after the culture test. The sepsis diagnosis was determined by the disease codes in the medical records: the International Classification of Diseases Codes (A41.5, A41.9, R57.2, R57.9). Physicians used qSOFA/SOFA criteria for diagnosis in the selected setting as in most other settings. The exclusion criterion was patients transferred from other departments. A total of 1,606 patients were admitted and treated in the selected departments during the study period; 343 met inclusion criteria (a)–(d). Fifty-nine among them were diagnosed with sepsis. After excluding one patient (transferred from another department), a total of 58 patients became the final sample for the NS group (Figure 1).
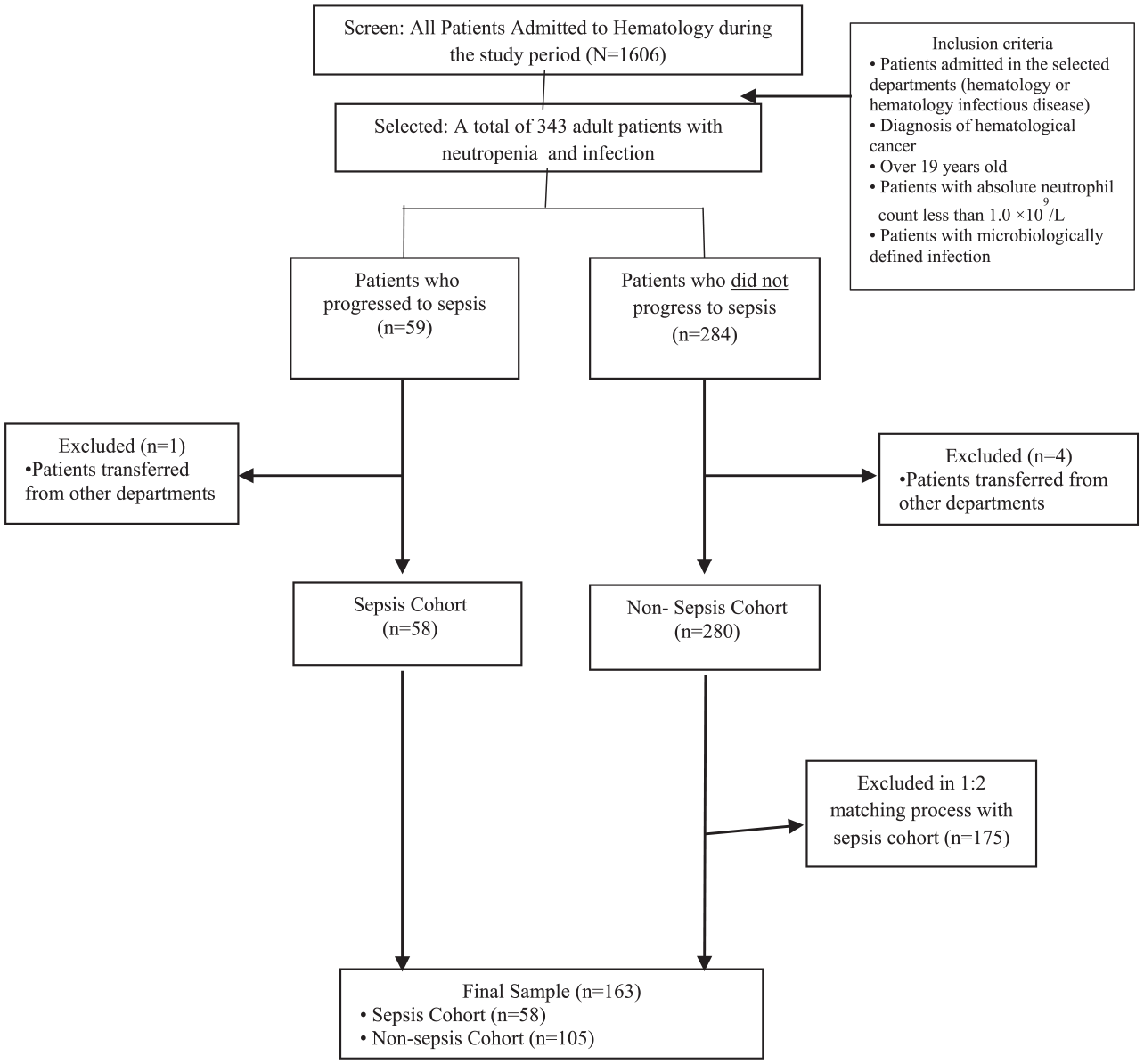
Flow chart for the sample selection procedure.
For the non-NS group, the inclusion criteria were individuals who met the above-mentioned criteria (a)–(d) and (e) did not receive a sepsis diagnosis until discharge. The exclusion criteria were the same as those for the sepsis group. A total of 280 met all inclusion and exclusion criteria for the non-NS group. Following the previous study with a similar design (Akalu et al., 2020), we performed 1:2 individual matching (NS group vs. non-NS group). Thus, 105 individuals were selected as the final sample for the non-NS group. The non-NS group was matched with the NS group based on the date and admitted floor of MDI confirmation. By matching those factors, we tried to control the confounding effects of the healthcare systems: workers (e.g., nurses, interns, and residents), the policy and procedures, and the physical environment.
The final sample size was 163 (58 in the NS group, 105 in the non-NS group), which met the logistic regression sample estimate of 129 calculated using G*Power, with a CRP odds ratio of 1.94 (Juutilainen et al., 2011), significance level of .05, and power of 90%.
Measurements
Data were collected from medical records based on the day of specimen collection, with which MDI was confirmed.
Biomarkers
Biomarkers included body temperature (presence of fever, duration of fever, highest and average temperature during febrile episode), neutrophil count, CRP, albumin, CRP–albumin ratio, and procalcitonin. Body temperature was determined based on axillary measurements recorded within 3 days prior to the day of specimen collection (Frazer et al., 2019). We identified the presence of fever (threshold: 37.5°C) within this 3-day window and the highest body temperature during the febrile episode. Fever duration was calculated as the consecutive number of days with at least one recorded temperature of 37.5°C or higher; average temperature was computed by taking the mean of all temperature values observed during the period. For participants without fever, the highest and average temperatures were processed as missing data.
We collected data on neutrophil count (109/L), CRP levels (mg/dL), albumin concentration (g/dL), and procalcitonin levels (ng/mL) on the day of specimen collection. CRP and albumin levels were obtained on the same date to calculate CRP–albumin ratios. When laboratory values on the day of specimen collection were not available, the most recent measurements within 2 days of the targeted day were used as substitutes. Otherwise, the data were processed as missing.
Treatment-Related Characteristics
Treatment-related characteristics included diagnosis, history of recurrence, neutropenia duration, treatment modalities, LOS, and the number of invasive devices. Diagnoses were categorized into leukemia, myelodysplastic syndrome, lymphoma, multiple myeloma, and aplastic anemia. Neutropenia duration was assessed as the period during which absolute neutrophil count remained below 1.0 × 109/L until the day of specimen collection. Treatment modalities included chemotherapy, radiation therapy, and hematopoietic stem-cell transplantation conducted within 6 months prior to MDI confirmation. LOS was calculated from the admission date to the day of specimen collection. The number of invasive devices on the day of MDI confirmation was assessed for central venous catheters, urinary catheters, nasogastric tubes, endotracheal tubes, tracheostomy tubes, and other drainage tubes.
Infection-Related Characteristics
Infection-related characteristics included infection source and number of causative organism strains. Infection sources were classified as respiratory system, gastrointestinal system, bloodstream, renal and urological system, skin and soft tissue, and others. The number of causative organisms was categorized as one versus two or more strains.
Ethical Considerations and Procedures
This study was approved by the Institutional Review Board (no. KC18RESI0714). Two nurses in the hematology department independently retrieved the medical records to collect data and cross-checked the data to ensure accuracy.
Data Analysis
Data were analyzed using SAS v. 9.4 (SAS Institute, Cary, NC, USA). We conducted a logistic regression analysis to examine the predictive factors of NS. Characteristics that were significantly different between groups in the bivariate analysis were selected as independent variables for logistic regression. To compare and evaluate the predictive power of the biomarkers, we conducted a receiver operating characteristic curve (ROC), followed by the calculation of area under the curve (AUC), sensitivity, and specificity. An AUC closer to 1 indicates good predictive power (Yin et al., 2022). The most appropriate cutoff point for prediction on the ROC curve was determined using the Youden index. Missing data were excluded from the analysis.
Results
Main Characteristics of Patients in Each Group
Table 1 presents each group’s characteristics. In the NS group, the mean age of patients (n = 58) was 54 years (range: 22–83). There were more females (55.2%) than males. Nearly all patients (91.4%) developed a fever (≥37.5°C) within 3 days of specimen collection day, with the mean fever duration being 1.52 days (range: 1–8).
Differences Between Neutropenic Sepsis Group and Non-Neutropenic Sepsis Group.
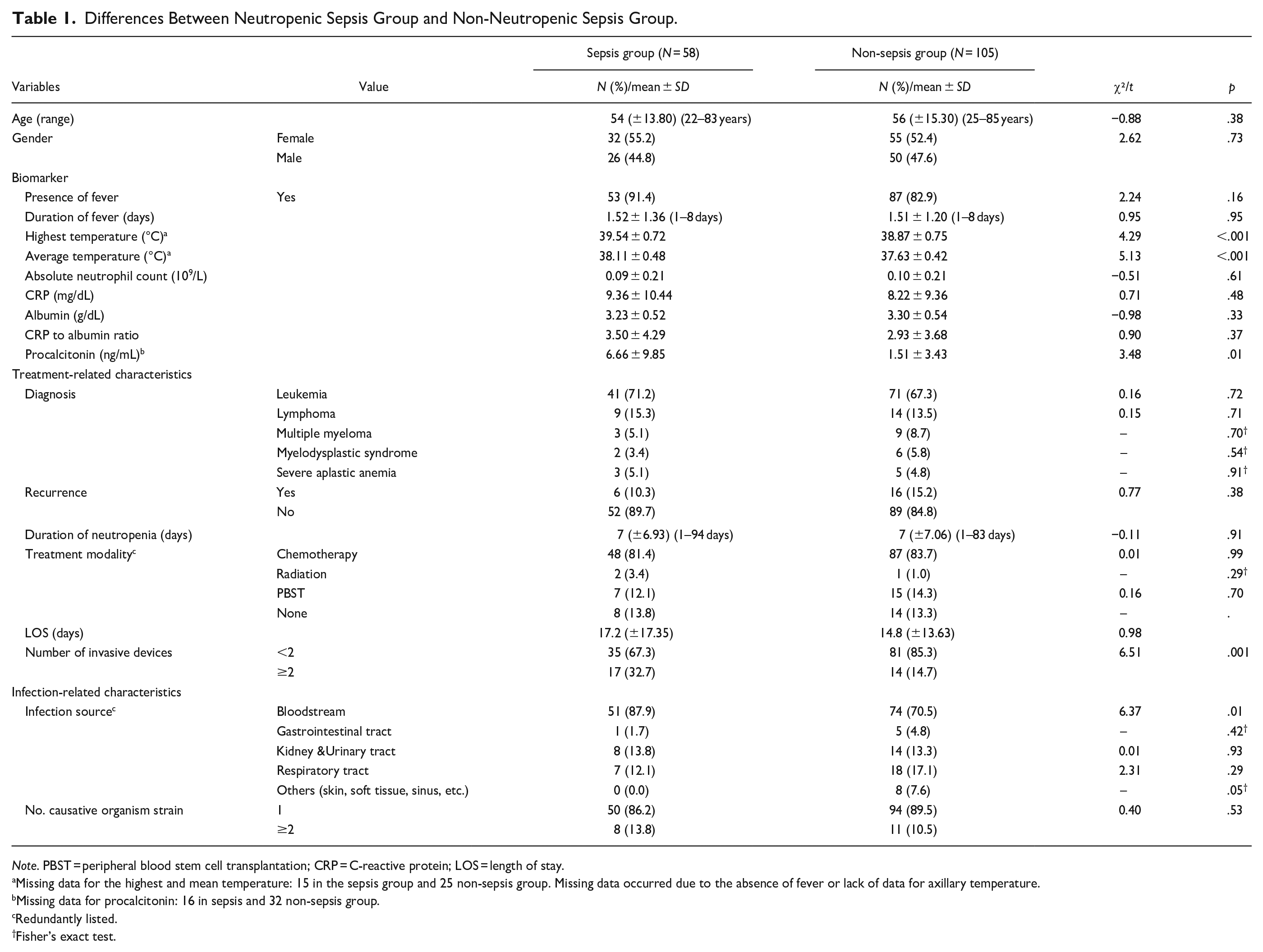
Note. PBST = peripheral blood stem cell transplantation; CRP = C-reactive protein; LOS = length of stay.
Missing data for the highest and mean temperature: 15 in the sepsis group and 25 non-sepsis group. Missing data occurred due to the absence of fever or lack of data for axillary temperature.
Missing data for procalcitonin: 16 in sepsis and 32 non-sepsis group.
Redundantly listed.
Fisher’s exact test.
The sample mean of the highest body temperature during the fever episode was 39.54°C and that of the average body temperature was 38.11°C. For the sample mean of other biomarkers, the CRP level was 9.36 mg/dL, the CRP–albumin ratio was 3.50, and the procalcitonin level was 6.66 ng/mL. The most common diagnosis was leukemia (71.2%), and most cases were not recurrent (89.7%). The mean duration of neutropenia was 7 days, and the most common treatment modality within the past 6 months was chemotherapy (81.4%). The mean LOS was 17.2 days (range: 1–94). Most patients had fewer than two invasive devices (67.3%) and were infected through the bloodstream (87.9%).
In the non-NS group (n = 105), the mean age was 56 years (range: 25–85). This group included slightly more females (52.4%). Most patients (82.9%) developed a fever (≥37.5°C) within 3 days of specimen collection, with a mean fever duration of 1.51 days. Regarding the sample mean of biomarkers, the highest body temperature during the fever episode was 38.87°C, and the average body temperature was 37.63°C. The CRP level was 8.22 mg/dL, the CRP–albumin ratio was 2.93, and the procalcitonin level was 1.51 ng/mL. The most common diagnosis was leukemia (67.3%), and most cases were not recurrent (84.8%). The mean neutropenia duration was 7 days, and the most common treatment modality was chemotherapy (83.7%). The mean LOS was 14.8 days (range: 1–83). Most patients had fewer than two invasive devices (85.3%) and were infected through the bloodstream (70.5%), followed by the respiratory tract (17.1%).
Differences Between Groups in Treatment-Related Characteristics, Infection-Related Characteristics, and Biomarkers
The NS and non-NS groups significantly differed in highest body temperature, average body temperature, procalcitonin levels, number of invasive devices, and bloodstream infections (Table 1). The highest body temperature (39.54°C vs. 38.87°C), average body temperature (38.11°C vs. 37.63°C; p < .001), and procalcitonin levels (6.66 ng/mL vs. 1.51 ng/mL; p = .008) were all higher in the NS group. More patients in the NS group had two or more invasive devices (32.7% vs. 14.7%, p < .001) and bloodstream infections (87.9% vs. 70.5%, p = .012) than in the non-NS group. There were no significant differences between groups in other characteristics (Table 1).
Independent Predictors of Neutropenic Sepsis Development
We conducted logistic regression using the variables that significantly differed between the groups in the bivariate analyses (highest body temperature, average body temperature, procalcitonin, number of invasive devices, bloodstream infections). Variance inflation factor (VIF) was computed to test for multicollinearity among the independent variables; the VIF values for the highest body temperature and average body temperature were above 5. We chose average body temperature as an independent variable to predict NS occurrence since it is based on the repeated assessment of body temperature during the fever episode and is more reliable than a single measurement of the highest body temperature. After removing the highest body temperature, the VIF values of all independent variables were below 5 (Table 2).
Predictors of Neutropenic Sepsis Development (N = 163).
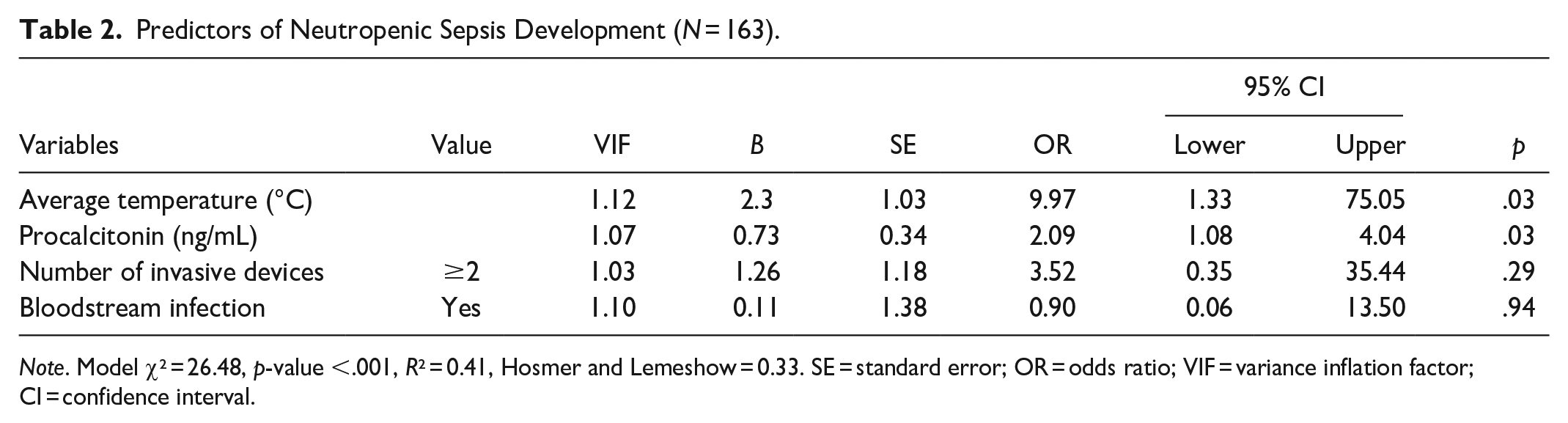
Note. Model χ² = 26.48, p-value <.001, R² = 0.41, Hosmer and Lemeshow = 0.33. SE = standard error; OR = odds ratio; VIF = variance inflation factor; CI = confidence interval.
The χ² test and Hosmer and Lemeshow’s goodness-of-fit test confirmed good model fit, and the model explained 41% of the variance. The significant independent predictors were average body temperature during a fever episode and procalcitonin level. The odds of NS increased 9.97 times (95% CI [1.33, 75.05]) for every 1°C increase in average body temperature during the fever episode and 2.09 times (95% CI [1.08, 4.03]) for every 1 ng/mL increase in procalcitonin levels. The number of invasive devices and bacteremia were not independent predictors.
Optimal Cutoffs for Average Body Temperature and Procalcitonin in Predicting NS
In the ROC analysis, the AUC of average body temperature for predicting NS was 0.77 (95% CI [0.68, 0.87], p < .001) and that of procalcitonin was 0.71 (95% CI [0.59, 0.84], p < 0.001; Figure 2). Based on the Youden index, the optimal cutoff for average body temperature was 37.9°C, with 71% sensitivity and 70% specificity. The optimal cutoff for procalcitonin was 0.55 ng/mL, with 68% sensitivity and 70% specificity (Table 3).
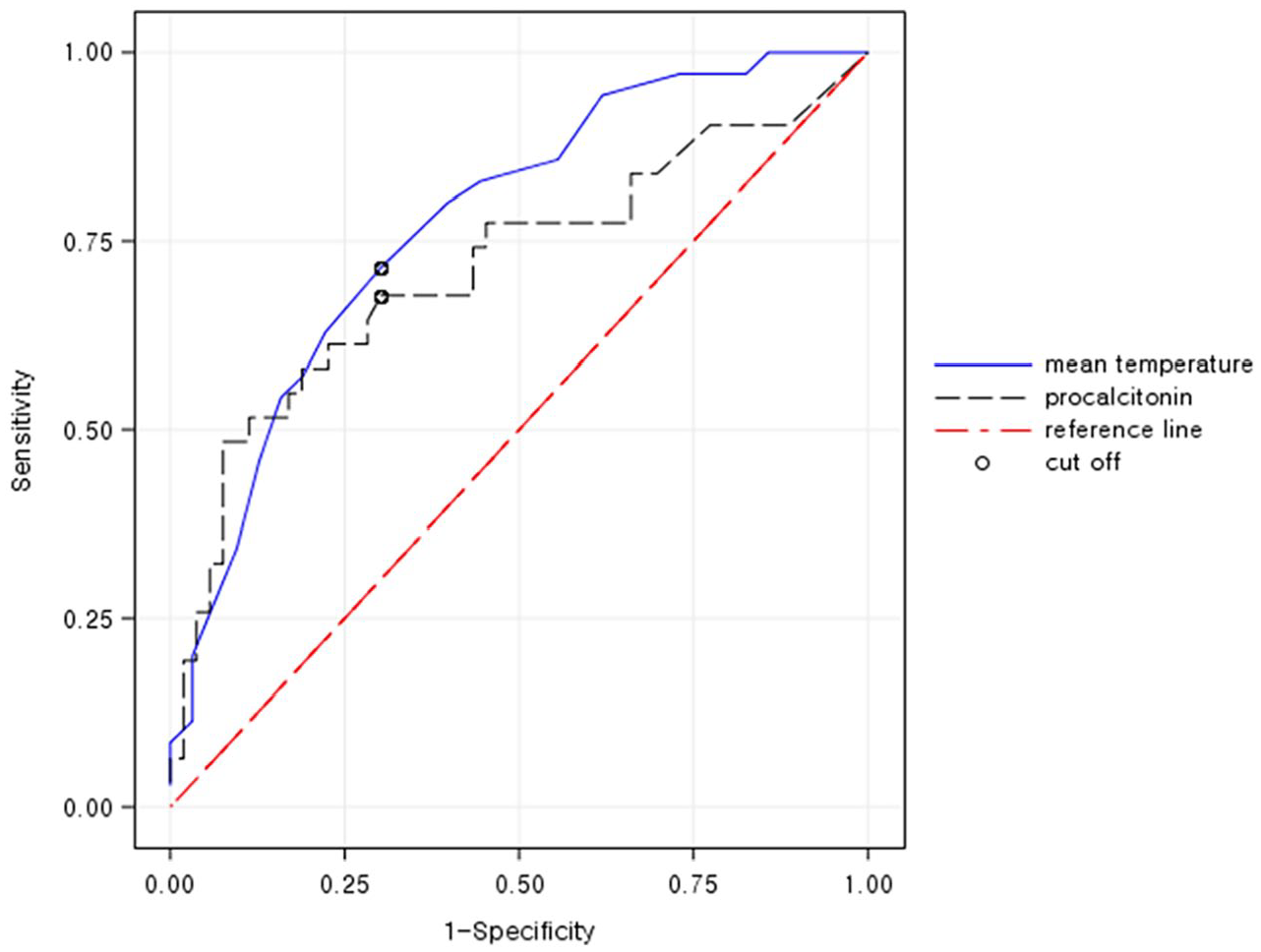
ROC curve for predicting NS.
ROC Curve Analysis for Prediction of Neutropenic Sepsis.
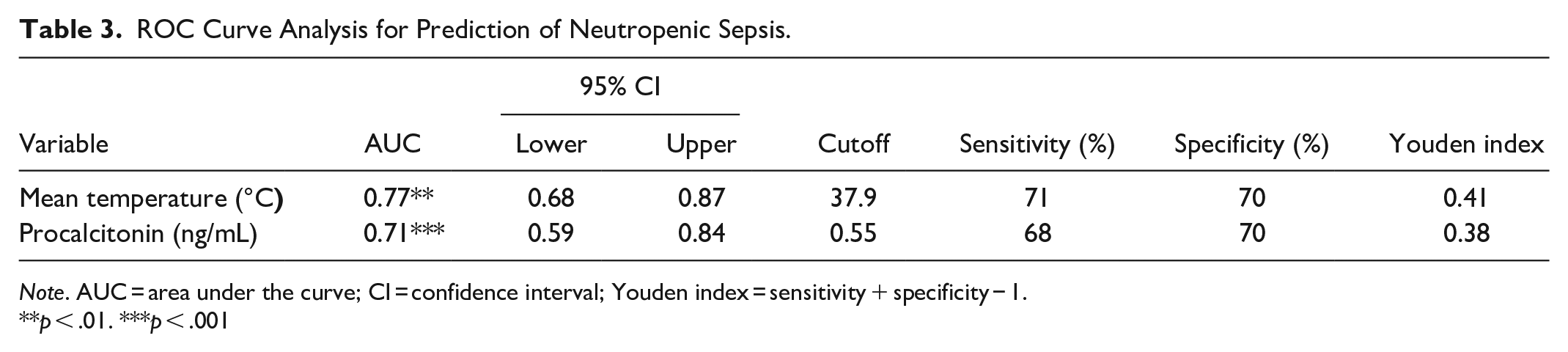
Note. AUC = area under the curve; CI = confidence interval; Youden index = sensitivity + specificity − 1.
p < .01. ***p < .001
Discussion
This study examined NS predictors in patients with hematologic malignancies based on data collected with reference to the day of specimen collection, with which MDI was confirmed. We identified average body temperature and procalcitonin level as independent predictors of NS. Individuals with higher average body temperature and procalcitonin levels were at higher risk of NS. The AUC for average body temperature (cutoff = 37.9°C) and procalcitonin (cutoff = 0.55 ng/mL) were 0.77 and 0.71, respectively, demonstrating an appropriate level of prediction accuracy (Islam et al., 2019). Since both the odds ratio (OR) and AUC for average body temperature (OR = 9.97, AUC = 0.77) surpassed those for procalcitonin (OR = 2.09, AUC = 0.71), average body temperature is the most crucial predictor.
Diverse criteria (e.g., 37.5°C, 38°C, 38.5°C, 39°C) are used to determine clinically significant fever when caring for NS patients (National Collaborating Centre for Cancer (UK), 2012). We have provided a temperature cutoff (37.9°C) for the early detection and treatment of patients progressing to NS. Unlike other studies (Hakim et al., 2010; Rondinelli et al., 2006), we determined this cutoff based on average body temperature over the 3 days preceding specimen collection. Average temperature is more reliable since it is based on multiple assessments, not a single episode. Also, cutoffs based on average temperature tend to be lower than those for the highest body temperature (e.g., 38.5°C in Rondinelli et al., 2006; 39°C in Hakim et al., 2010). Therefore, it is more conservative and can help clinicians make timely decisions. Nevertheless, further research is needed to confirm the clinical significance of average body temperature since few studies have provided cutoff points based on average body temperature, and the patient populations varied (e.g., post-cardiac surgery patients with an average body temperature of 36.7°C, sensitivity = 59.1%, specificity = 56.0%; Porizka et al., 2019).
Consistent with a few other studies involving patients with hematologic malignancies (Intke et al., 2022; Reyes Mondragón et al., 2021; Stoma et al., 2017), we identified procalcitonin level as an independent predictor of NS. Despite concerns regarding the validity of procalcitonin levels in hematologic malignancies, such consistent findings support procalcitonin levels as a valid biomarker for predicting NS risk in patients with hematologic malignancies. Also, we found it is the most useful predictor among serum biomarkers (i.e., CRP, albumin, and CRP–albumin ratio).
In previous studies, the cutoff points of procalcitonin for predicting NS in patients with hematologic malignancies varied from 0.14 to 1.50 ng/mL; sensitivity and specificity were 62–91% and 53–88%, respectively (Intke et al., 2022; Reyes Mondragón et al., 2021; Stoma et al., 2017). Such variations could be attributable to differences in measurement timing. In the study most similar to ours in terms of assessment time point, the cutoff points were 0.138 ng/mL (sensitivity = 88%, specificity = 53%) on the first day of fever onset and 0.887 ng/mL (sensitivity = 63%, specificity = 89%) on the second day (Intke et al., 2022). Our cutoff point (0.55 ng/mL) is slightly lower than that for the second day of fever (Intke et al., 2022). Yet, sensitivity (68%) and specificity (70%) are both appropriate in our study, and our assessment time point is more clinically useful.
Our bivariate and multivariate analyses did not show evidence that CRP, albumin, and CRP–albumin ratio play a role in predicting NS development. Although the assessment time points for several cases departed from the targeted day, there were few such cases (n = 9), and departure from the MDI date was only 1–2 days. Thus, measurement errors did not threaten the internal validity of this finding. Notably, CRP level was high in most participants and ranged widely, whereas albumin level was mostly normal or marginal. Such distributions could have influenced the findings, suggesting their limited usefulness in predicting NS.
Bloodstream infection was associated with NS in bivariate analysis but not in multivariate analysis. Notably, it was the most common source of infection in both groups (87.9% vs. 70.5%). Respiratory infections are the most common source of infection leading to sepsis in general (Jeon et al., 2019). Patients with hematologic malignancies are at a higher risk of bloodstream infection owing to various factors (e.g., mucosal barrier injury, maintenance of invasive devices, immunosuppression) (Garrido et al., 2019; Vesteinsdottir et al., 2022). Therefore, this finding accurately reflects the clinical characteristics of patients with hematologic malignancies and highlights the importance of managing devices that serve as pathways for bloodstream infections. Nurses should be well-versed in infection control methods when managing invasive devices and implement strategies for the early removal of unnecessary devices.
Implications for Clinical Practices and Research
Our finding suggests that upon detecting a microbial infection, healthcare professionals could identify individuals at risk of progressing to NS based on average body temperature and procalcitonin levels and provide early intervention.
It is well known that monitoring body temperature in neutropenic patients is essential for assessing infection status and progression to sepsis (Kochanek et al., 2019). This study’s unique contribution, however, is that we demonstrate the implications of average body temperature over the 3 days preceding the specimen collection date. The minor difference in average body temperature between the NS group and non-NS groups (0.5°C) underscores the importance of accurate temperature assessment. It is necessary to maintain consistency in the measurement site (axillary, oral, tympanic) and be well-versed in the use of measuring instruments. Also, strategies for meticulous temperature monitoring (frequency, method) need to be established during neutropenia. Patients and their caregivers should receive education about temperature assessment.
Recent studies have used machine learning to predict sepsis. While benefiting from processing vast quantities of medical records, such approaches often lack design rigor (Vesteinsdottir et al., 2022). By contrast, we ensured rigor by establishing clear criteria for data collection points for each variable and the control cohort. Machine learning techniques (vitals, peripheral capillary oxygen saturation, Glasgow coma score, age) are reported to enable the early recognition and accurate prediction of sepsis 3–4 hr before its onset (ROC = 0.89, sensitivity = 0.81, specificity = 0.72) (Islam et al., 2019). However, identifying sepsis 3–4 hr before onset has little clinical utility. By focusing on the day of specimen collection for MDI diagnosis, we provide valuable information for the early detection and management of NS.
Limitations
This study has several limitations. The selection of participants from a single center and the small sample size limit generalizability. Given the low incidence rate of NS, the sample size is realistic. The missing data for temperature (n = 40) and procalcitonin (n = 48) were concerns, but they were mostly in the non-NS group (see Table 1). Nonetheless, further studies should be conducted with larger samples from multiple centers. Moreover, our sample included several patients with MDI confirmed on the first day of hospitalization (eight NS and 16 non-NS). The fever duration for those patients was unclear, which could have affected the findings. Lastly, as this was a retrospective study using electronic medical records, there were slight variations in data collection time points for the blood biomarkers. There were cases where the CRP and procalcitonin measurement date did not coincide (n = 2) or where the most recent measurements were used instead of those taken on the targeted date (n = 9, 1–2 days departure from the targeted date). There could be bias due to such inconsistency in assessment time points.
Conclusion
Nurses play a critical role in preventing, identifying, and managing NS. Upon detecting a microbial infection, healthcare professionals should identify individuals at risk of progressing to NS based on average body temperature and procalcitonin levels and provide early intervention. Clinical pathways for identifying and managing patients at high NS risk should include assessing average body temperature and procalcitonin levels on the MDI diagnosis day.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We gratefully acknowledge support from the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (grant no. 2016R1A2B4009800). This study is based on the first author’s master’s thesis.