
Abstract
African American patient populations are disproportionately diagnosed with severe obstructive sleep apnea (OSA) compared to non-Hispanic white adults. Research suggests a link between OSA and anxiety. However, OSA and anxiety symptoms may present differently across minority groups. Research examining the reliability and validity of measures used to assess anxiety symptom severity in African American patient populations living with OSA is needed. This pilot study evaluated the reliability and validity of the Patient Reported Outcomes Measurement Information System (PROMIS) Anxiety short form and the longer State-Trait Anxiety Inventory-State (STAI-S) in a sample of African American adults recently diagnosed with OSA. In this cross-sectional pilot study, 32 African American patients newly diagnosed with OSA were recruited from an academic sleep medicine clinic in the Southeastern United States to complete survey measures. Participants completed the 6-item PROMIS Anxiety short form and 20-item STAI-S. Cronbach’s alphas assessed the internal reliability of measures, and concurrent validity between measures was assessed using correlation coefficients (rs). Both PROMIS Anxiety and STAI-S showed excellent internal consistency with Cronbach’s α ≥.90. The PROMIS Anxiety T-scores and STAI-S scores were positively moderately correlated with each other (rs = .68; p < .0001), indicating concurrent validity. These results illustrate that both the PROMIS Anxiety and STAI-S scales have strong internal reliability in this sample of African American adults with co-occurring OSA and prediabetes. The brief PROMIS Anxiety short-form measure is validated to the longer STAI measure in this sample. An advantage of the PROMIS Anxiety scale is that it has a lower participant burden when completing questionnaires, contributing to a more refined approach to diagnosis and management when both OSA and anxiety coexist. These findings also underscore the importance of validating psychometric measures in marginalized populations, such as African Americans, who have historically been underrepresented in psychometric research.
Background
Globally, approximately 1 billion adults experience obstructive sleep apnea (OSA), a sleep disorder caused by a partial or complete collapse of the airway, which deprives the body of its normal oxygen saturation (Slowik et al., 2023). People living with OSA may experience interrupted sleep multiple times throughout the night. These disturbances in the sleep cycle lead to a host of difficulties, including unrefreshing sleep, excessive sleepiness, fatigue, diminished energy levels (Gottlieb & Punjabi, 2020; Senaratna et al., 2017), reduced work performance, sleepless-related accidents, compromised cardiovascular health, and an overall lower quality of life (Diaz & Brown, 2016; Gottlieb & Punjabi, 2020; Slowik et al., 2023). OSA is associated with the development of prediabetes or type 2 diabetes. These conditions share many common risk factors. (Cass et al., 2013; Ceïde et al., 2015; Gottlieb & Punjabi, 2020). Moreover, beyond impacting sleep quality, OSA is intricately connected to an increase in mental health issues, which can lead to challenges in treatment adherence.
One such mental health issue that often affects people living with OSA is anxiety. Saunamaki and Jehkonen (2007) conducted a review finding that individuals newly diagnosed with OSA frequently reported symptoms of depression and anxiety (Saunamaki & Jehkonen, 2007). Other research indicates that anxiety is more prevalent in patients with OSA when compared to the general population (Diaz & Brown, 2016; Kim et al., 2019; Shapiro et al., 2014). Yet, there is limited research targeted at addressing the relationship between presence and burden of psychological symptoms, including anxiety, in patients who are newly diagnosed with OSA.
There is also a lack of targeted attention on the prevalence of undiagnosed and untreated OSA within minority populations (Johnson et al., 2022). The lack of research on OSA among minority patient populations can be attributed to several factors, including insufficient referrals for evaluation, delays in both evaluation and diagnosis, structural barriers such as transportation or work issues, limited awareness among primary care providers, and patients lost to follow up (Cass et al., 2013; Greenberg et al., 2004; Thornton et al., 2022). Studies have consistently revealed higher OSA prevalence rates among Asian adults, African American adults, and Hispanic individuals (Gottlieb & Punjabi, 2020; Johnson et al., 2022; Slowik et al., 2023), yet these populations and their relationships to OSA have remained underexamined. Teresi et al. (2016) found little difference between minority groups in the evaluation of the Patient Reported Outcomes Measurement Information System (PROMIS) Anxiety scale. However, recent studies suggest that OSA and anxiety might present differently in various minority groups due to psychosocial factors (Johnson et al., 2022). Manseau and Case (2014) found that there were large differences between non-Hispanic Black patients and White patients’ racial-ethnic visit prevalence ratios for anxiety, indicating that non-Hispanic Black patients were significantly less likely to seek treatment for anxiety compared to their White counterparts. This disparity could be attributed to various factors including cultural stigma or differences in health care access. For example, in a study of only non-Hispanic Black adults, a three-fold increase in the odds of being at risk for OSA was associated with anxiety (Ceïde et al., 2015). Unlike Teresi et al. (2016), this work assessed anxiety among African American patients with multiple chronic conditions that may face undue burden or challenges managing their symptoms.
Researchers studying anxiety rely on psychometric data to form and test theories, diagnose symptoms, and develop treatments. Neither the State-Trait Anxiety Inventory nor the PROMIS Anxiety short form have been validated for assessing anxiety among patients living with OSA, despite the heightened co-occurrence of anxiety and OSA among patients. Further, much of the development of patient reported outcome measures, including the STAI and PROMIS measures, did not explicitly center their psychometric research and recruitment on African American patient populations across various chronic physical and mental health conditions. As such, psychometric research focused on historically marginalized patients with complex chronic conditions affected by anxiety symptoms is warranted. As OSA diagnoses rise among African American patients, it is imperative to evaluate the psychometric performance of anxiety assessment tools to enhance OSA treatment adherence.
The purpose of this study was to compare the psychometric performance, specifically reliability and validity, of the Patient Reported Outcomes Measurement Information System (PROMIS) Anxiety short form to the longer State-Trait Anxiety Inventory-State (STAI-S) in a sample of African American adult prediabetic patients who were recently diagnosed with OSA.
Methods
Design and sample
This is a secondary analysis of data collected from a pilot study. The pilot was funded by the National Institute of Nursing Research (NINR) to examine symptom severity and inflammatory presentations (e.g., cytokines) in African American adult patients with prediabetes and recent diagnosis of OSA (Giordano et al., 2023). Thirty-two participants were recruited from a sleep medicine clinic located within a large urban academic medical center in the parent study within 30 days of being diagnosed with OSA (Giordano et al., 2023). All participants gave written consent before enrolling in the study. Participants completed a collection of surveys capturing demographic data and symptom severity of anxiety at baseline. The Institutional Review Board of the university reviewed and approved the parent study (STUDY00002910), including human subject approval.
Measures
PROMIS Anxiety (PROMIS® Item Bank v1.0—Emotional Distress-Anxiety—Short Form 6a) assesses the level of emotional distress and anxiety of an individual. The six-item questionnaire includes questions concerning the nature of the participant’s anxiety symptoms over the past 7 days, inquiring about fear, anxious misery, hyperarousal, and somatic symptoms of arousal. The PROMIS Anxiety instrument is based on a five-point Likert scale (never, rarely, sometimes, often, always) that is summed across all questions into a raw score and then converted to a T-score; raw summed scores range from 6 to 30. The transformed scores are normed to a general population with a mean of 50 and a standard deviation of 10 (Beleckas et al., 2018; Giordano et al., 2023; Pilkonis et al., 2011). Total scores range from 0 to 100; the higher the score, the more anxiety-related symptoms being experienced by a respondent.
Study participants also completed the STAI-S inventory scale (20-item) (Gupta et al., 2016). STAI-S has 10 reverse-scored items (Zsido et al., 2020). Following the reversal of scores for positively-worded items, total scores are computed, ranging from 20 to a maximum of 80 on the STAI-S subscale (Kayikcioglu et al., 2017). STAI scores are often categorized as “no or low anxiety” (20–37), “moderate anxiety” (38–44), and “high anxiety” (45–80) (Kayikcioglu et al., 2017). The STAI-S is capable of measuring anxiety both in healthy individuals and individuals with known depression or anxiety (Knowles & Olatunji, 2020). Historically, the STAI-S has been shown to be both reliable and valid, though its reliability and validity have been largely examined utilizing predominantly white patient samples (Gupta et al., 2016).
Additionally, patient demographics and clinical characteristics were obtained from self-reported surveys and gathered from the medical records. Participants’ age, sex, Hgb A1c values (to detect prediabetes), and race were collected from the electronic medical records. Education levels were collected directly by participants via self-reported surveys.
Analyses
Descriptive statistical analyses were applied to summarize participant characteristics. A one-sample t-test was calculated to compare the means of the PROMIS Anxiety in the sample to the known general population’s T-score of the PROMIS Anxiety scale. Spearman’s correlation coefficients (rs) evaluated the convergent validity between PROMIS Anxiety and STAI-S. Given the widespread use of the STAI in anxiety assessments, it was natural to investigate the convergent validity between the well-established STAI and the shorter, newer PROMIS measure. Correlation coefficients were interpreted based on standard criteria where a value of .10 to .39 would be considered a weak correlation (association) and .40 to .69 would be considered a moderate correlation, and 0.70 or above a strong correlation between the scales (Schober et al., 2018). Reliability of PROMIS Anxiety and STAI was examined by calculating the Cronbach’s alpha for each measure; values greater than .70 are generally considered satisfactory for internal reliability (Clover et al., 2022; Mulhern, 2011; Taber, 2018). The parent study was a hypothesis-generating pilot study that was not powered to detect differences across demographic groups. However, a sample size of N = 32 provides sufficient power (80%) to detect even a small correlation between measures (r = .21). All analyses were conducted in R (R_Core_Team, 2023).
Results
This pilot study included 32 African American adult patients newly diagnosed with OSA of whom 53.1% were female. The mean age was 47.8 (±8.8) years. A large portion of patients (40.6%) were college graduates (Table 1). Moderate-to-severe OSA was present in 55.2% of patients. The sample’s A1c scores, averaging 5.97 (±0.2), indicated the presence of prediabetes. Average PROMIS Anxiety scores were 46.0 (±9.3) with 25.0% of participants scoring above 55, indicating higher than average anxiety symptoms (Table 1). The average STAI-S scores was 27.7 (±10.3) and 18.8% scored greater than 37 on the scale indicating higher anxiety symptoms (Table 1).
Patient Characteristics (N = 32).
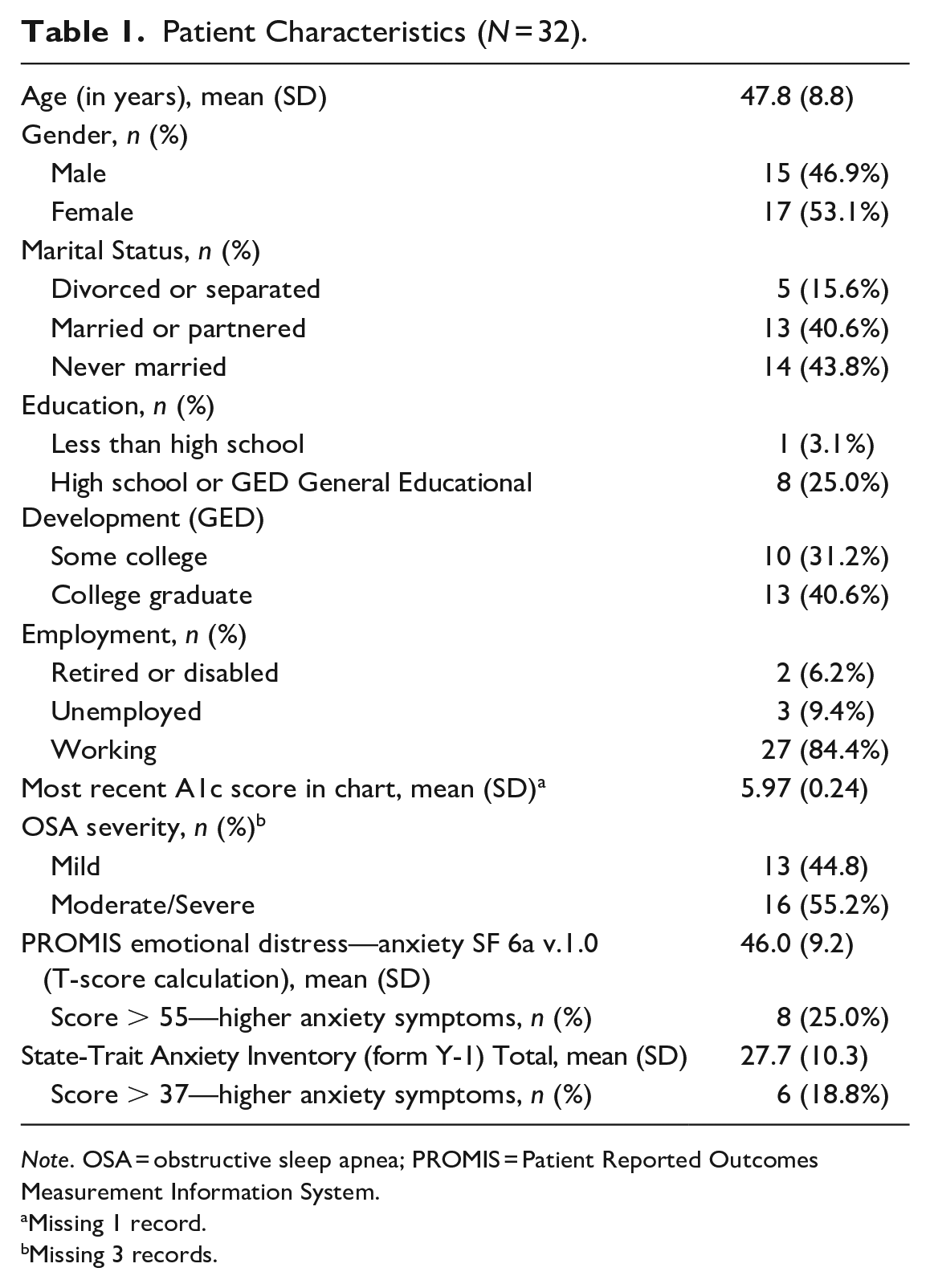
Note. OSA = obstructive sleep apnea; PROMIS = Patient Reported Outcomes Measurement Information System.
Missing 1 record.
Missing 3 records.
Both PROMIS Anxiety and STAI-S showed excellent internal consistency with Cronbach’s α of .93 (95% Confidence Interval [CI]: 0.89, 0.96) and 0.94 (95% CI: 0.90, 0.97) (Table 2), respectively. When compared to less diverse samples, these values are comparable, as both measures typically show high internal consistency across various populations. Our results illustrate that both the PROMIS Anxiety and STAI-S scales have strong internal reliability in this sample of the African American population with co-occurring OSA and prediabetes. The PROMIS Anxiety T-scores and STAI-S scores were also moderately correlated with each other (rs = .68; p ≤ .0001), which indicates concurrent validity between the two measures.
Reliability of Measures.

Note. PROMIS = Patient Reported Outcomes Measurement Information System; STAI-S = State-Trait Anxiety Inventory-State; α = alpha.
Discussion
Our analysis confirmed that both the PROMIS Anxiety short form and the STAI-S reached a threshold of acceptable internal reliability in a sample of prediabetic African American patients living with OSA. Anxiety symptoms are common among individuals with OSA, and the causes may vary between males and females and different ethnicities (Gharsalli et al., 2022; Gupta et al., 2016; Lee et al., 2015; Saunamaki & Jehkonen, 2007). It is crucial to assess and concurrently address psychological symptoms, particularly anxiety, to achieve optimal treatment outcomes for individuals with OSA. In this specific population of African American patients with newly diagnosed OSA, the PROMIS Anxiety scale and STAI-S also demonstrate concurrent validity.
The PROMIS Anxiety scale offers several advantages, including form versatility in administration, availability to use in multiple languages, and it has a lower participant burden when completing questionnaires, contributing to a more refined approach to diagnosis and management when both conditions coexist. This study’s findings show that the short-form six-item version of the PROMIS Anxiety scale can be used in clinical care and research settings to accurately capture anxiety symptom severity among African Americans living with OSA.
Other studies have used the PROMIS or STAI-S to assess for anxiety and evaluate measure performance, some of which included African Americans but did not purposely center them in their research. Researchers studying orthopedic populations and patient populations with other chronic conditions have validated the psychometrics PROMIS Anxiety measure, but did not include large samples Black or African American patients (Beleckas et al., 2018; Cella et al., 2010). For instance, only 11.7% of participants in Beleckas et al. (2018) and 9% in Cella et al. (2010) identified as Black adults. Schalet et al. (2016) further showed the clinical validity of PROMIS Anxiety and other PROMIS measures in various longitudinal clinical groups such as patients with major depressive disorder, cancer, chronic heart failure, back pain, and chronic obstructive pulmonary disease. However, the ethnicity of the participants in these groups was not disclosed. Though these studies contained a subsample of African Americans, to date, no study has used the PROMIS Anxiety short form and the STAI-S scale to gauge the severity of anxiety symptoms solely among prediabetic African American patients with OSA. The findings from this study confirms the reliability and validity of the PROMIS Anxiety and the STAI-S, which is consistent with existing psychometric literature (Beleckas et al., 2018; Pilkonis et al., 2011). Our findings indicate that the PROMIS Anxiety short form and STAI-S provides reliable results when used with prediabetic African American patients with OSA.
These findings highlight the need to validate psychometric measures in underrepresented populations, such as African Americans (Beard et al., 2011; Shrestha et al., 2020). Because the African American population has historically faced exclusion from such assessments, many cultural nuances in self-reporting have not been taken into account during the creation nor administration of these assessments. For example, significant stigmas are attached to members of the African American community who disclose that they suffer from anxiety or other mental health issues, this leads to hesitancy in seeking assistance due to fear of negative judgment or memories of past discrimination which results in under-reporting of anxiety (Hopkins & Shook, 2017; Shrestha et al., 2020; Williams et al., 2012). Other historical challenges, such as small sample sizes in minority-focused research studies, highlights the need to include understudied populations in research endeavors (Shapiro et al., 2014). This study enriches our understanding of the reliability and validity of the PROMIS Anxiety and STAI-S scales within a population that has faced exclusion from psychometric research for various reasons. This awareness enhances the generalizability of these measures, paving the way for more culturally sensitive mental health assessments in clinical and research settings. Nurses and clinicians working with minority communities can rely on assessments that include culturally appropriate questions, gathering more inclusive and accurate data. This enables clinicians and researchers to develop targeted interventions and strategies, ultimately improving overall health outcomes in minority communities.
When minority patients living with OSA and exhibiting anxiety are promptly and accurately diagnosed and their symptoms are properly managed, they are more likely to experience a beneficial impact on sleep, co-morbidities (e.g., prediabetes or hypertension) associated with OSA, and overall quality of life (Jackson et al., 2019). By assessing for anxiety when screening and managing African American patients for OSA, nurses and other clinicians can optimize referrals for appropriate symptom management, ensuring comprehensive care and improved outcomes for these patients. Additionally, addressing anxiety in conjunction with OSA management may lead to a better effect on treatment regimens, patient engagement, and quality of life (Diaz & Brown, 2016; Shapiro et al., 2014). Further research is needed across these areas.
Limitations
This pilot study has inherent limitations that warrant consideration. For example, the relatively small sample size of African American prediabetic individuals with OSA poses a potential limitation to the generalizability of the findings. Future research, with an expanded sample size, may yield a more robust psychometric dataset to evaluate the reliability and validity of anxiety measures, such as the PROMIS Anxiety and STAI-S, and contribute to a more comprehensive understanding of the co-occurrence of anxiety and OSA. Introducing multiple time points for anxiety assessments, including pre- and post-treatment evaluations, would enable researchers to capture dynamic changes and measure responsiveness to change over time, which was not possible in this cross-sectional study. Pre- and post-treatment evaluations using these psychometrically sound measures would not only offer a more complete picture of anxiety symptom severity but also help elucidate the impact of interventions on anxiety outcomes among individuals with OSA. Future research with other anxiety measurement tools, such as Beck Anxiety Inventory and Generalized Anxiety Disorder 7-item scale, should also be administered to prediabetic African American patients with OSA and compared to the PROMIS Anxiety and STAI-S measures, in order to evaluate their reliability and validity. Exploring subgroup analysis by gender or OSA severity in anxiety assessments could offer additional valuable insights into the accuracy of these measures. Despite these limitations, this analysis is among the first to investigate the psychometric strength of the short-form PROMIS Anxiety measure and the longer STAI-S measure in a sample comprised entirely of prediabetic African American patients newly diagnosed with OSA.
Conclusion
The current study expands upon prior psychometric research of both the PROMIS Anxiety and STAI-S scales by evaluating the reliability and validity of these measures when administered to a sample of prediabetic African American individuals with OSA. Anxiety symptom presentations among African American individuals with OSA remains insufficiently explored, largely due to underdiagnosis and limited research. The measures demonstrated high internal reliability and concurrent validity. While recent studies have enhanced understanding of the shared risk factors and relationships between individuals living with OSA and anxiety, less is known on which brief and psychometrically sound measures nurses can use to guide symptom management and referrals when caring for patients seeking OSA care. An advantage of the PROMIS Anxiety scale is that it has a lower participant burden when completing questionnaires, contributing to a more efficient approach to diagnosis and management when both conditions coexist. Findings from this research may inform researchers and clinicians to incorporate validated measures, such as the PROMIS Anxiety short-form and STAI-S, into routine practice and research studies, enabling quicker and more accurate anxiety assessments in African American patients with OSA.
Footnotes
Acknowledgements
The authors thank the participants for their contributions and time. In addition, the authors thank the Center for the Study of Symptom Science, Metabolomics, and Multiple Chronic Conditions leadership and staff for their assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported in part by the National Institute of Nursing Research under award number P30NR018090, the National Institute of Diabetes and Digestive and Kidney Diseases under award number P30DK111024, and the National Institute of Drug Abuse under award number K23DA057415. The content is solely the responsibility of the authors and does not represent the official views of the National Institutes of Health.