
Abstract
Family carer involvement in inpatient mental health care is considered beneficial to patient outcomes. Carers and families of patients in inpatient behavioral units often seek basic information about the unit in terms of visiting protocols, communication with staff, questions about the discharge process, and information on local social supports. Recent national and state laws strongly concur that all caregivers, 26% of whom care for those with mental health illness (American Association of Retired Persons [AARP] and National Alliance for Caregiving [NAC]). Recognize, assist, include, support, and engage (RAISE) Family Caregiver Act 2017 directs the Department of Health and Human Services (HHS) to create and make public a road map to support caregivers that includes sharing information. The purpose of this integrative review is to explore the needs and information gaps of carers of individuals hospitalized with mental illness. An integrative review where a detailed search strategy of databases through MeSH and associated terms was conducted between 2017 and 2025. Literature was included if it discussed carer-family, patient, and staff communication in the setting of inpatient behavior health hospitalization. Nine papers met the inclusion criteria and found that current carer information needs are not being met. The following themes were explored: information gap, need for basic information, and empowering caregivers with information. This literature review shows that there is a lack of information and support provided to carers of hospitalized patients with severe mental illness. The literature found that the carer should be treated with respect through the pre-arrangement of carer staff time, listening to carers, and focusing on the provision of recovery-oriented language. Future research should focus on determining if changes to involve families in care, staff training, information packets, required staff meetings or calls to carers, or creating or rewording unit literature to reflect recovery-oriented language would help to meet carer information needs. By addressing information gaps and empowering carers, mental health services can enhance care quality, improve patient outcomes, and strengthen the pivotal role of families in the healing process.
Introduction
Studies have shown that family involvement in the care of in-patients with severe mental illness is important because it better ensures follow-up care (Haselden et al., 2019), reduces stigma (Hsiao et al., 2019), improves outcomes of health for both patients and families and, in sum, should become a significant part of standardized care (Doody et al., 2017; Mackie et al., 2019; Schuster et al., 2020). Care that promotes family involvement involves a close and crucial partnership between the standard triad of patient, carer, and provider, which includes a specified understanding of what family involvement consists of and how it is helpful regarding treatment outcomes (Giacco et al., 2017; Haselden et al., 2019; Hsiao et al., 2019, 2024; Kaselionyte et al., 2019; Schuster et al., 2020).
Globally, less than one-third of those suffering from severe mental illnesses of psychosis receive care, and less than half of those with depression receive the same (World Health Organization [WHO], 2021). Statistics show that psychiatric hospitals take up the bulk (66%) (WHO, 2022) of the very scarce government resources that are allocated to mental health care, while in the United States, only 50% of people in need of care—surely something of a scandal—are receiving it (McGinty & Eisenberg, 2022). In addition, only 7.6% of the 50% legitimately worthy of receiving care actually receive inpatient care (The United States Department of Health and Human Resources [HHS], 2017). These figures point to the fact that many people with mental health issues may only have their families to rely upon for care.
The requirements for carers of those with severe mental illness can be burdensome, heavy, and severe (Hsiao et al., 2019; National Alliance for Caregiving [NAC], 2016; Schuster et al., 2020; Svendsen et al., 2021; Vatne et al., 2021; WHO, 2022). Carers have often expressed their desire to be involved, but just as often do not know how due to a lack of information or guidance from healthcare providers and organizations (Schuster et al., 2020). Research has shown that carers do not feel included in inpatient mental health care for patients simply because of a lack of staff time, inconsistent communication, and confusion over patient privacy laws (Bucknall et al., 2020; Carbonell et al., 2020; Doody et al., 2017; Mackie et al., 2019). Even the current family centered care models emphasize a linear provider-to-patient dynamic (Dirik et al., 2017), one that echoes the old paternalistic medical model, which leaves out family carers.
Studies have shown that carer and family involvement have improved patient outcomes (satisfaction, follow-up visits) whenever patients are hospitalized with needs for acute care (Haselden et al., 2019; Svendsen et al., 2021). Some studies have significantly explored barriers—providers and staff attitudes, for example, as well as stigmatizing attitudes, organizational culture, time limitations, and patient confidentiality—to carer involvement during the inpatient care of mental health patients (Doody et al., 2017; Eassom et al., 2014; Giacco et al., 2017; Hsiao et al., 2019; Kaselionyte et al., 2019; Mackie et al., 2019; Schuster et al., 2019). Therefore, this literature review attempts to determine the carer’s needs, what information gaps may exist, what information is needed, and how carers may be empowered.
Methods
A literature search was conducted to explore the needs of carers of those hospitalized with serious mental illness and to understand approaches for better involving them in their care plan. Existing literature was searched in February 2025. The following databases were searched: the PsycINFO & Cumulative Index of Nursing and Allied Health Literature (CINAHL) in EBSCOhost and PubMed. MeSH topic headings were used when possible. Combinations of the terms “Psychiatric Hospitals” OR “Mental Hospital” AND “caregiver” OR “family” AND “Professional-Family Relations” were used and adapted for each database (see Table 1).
Search Summary Table.
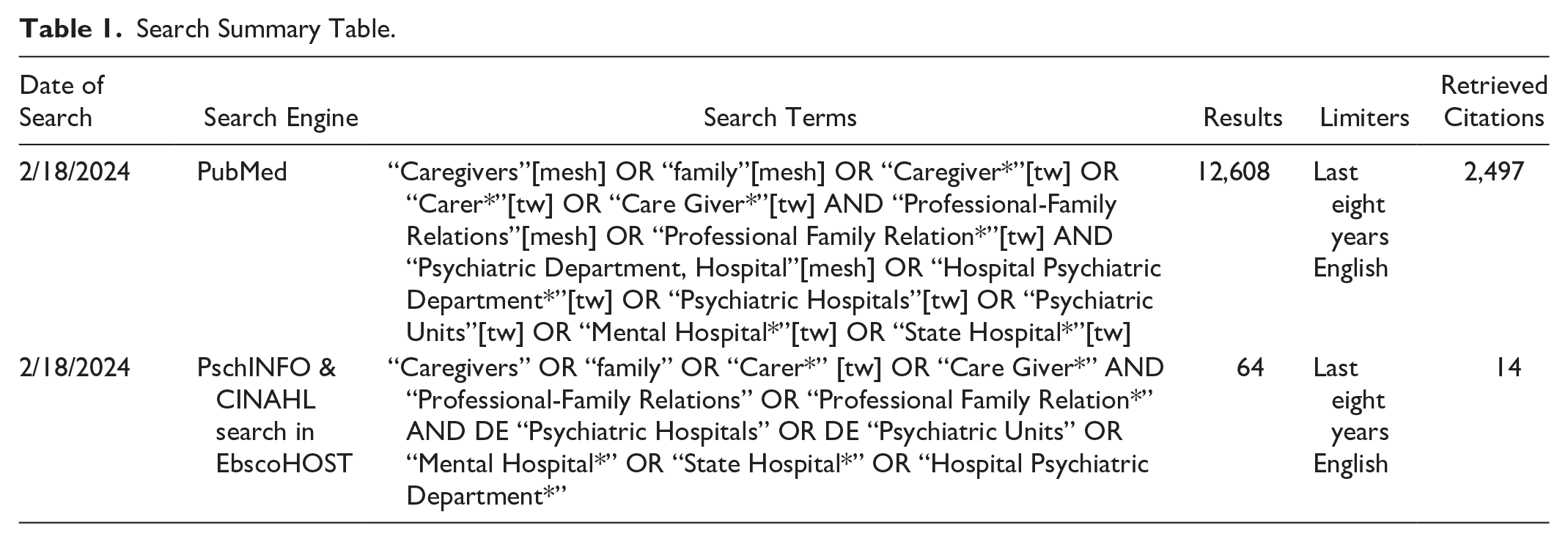
Inclusion criteria included articles written in English and published in the last eight years. The time frame was limited to current research because this literature review supported a full-scale quality improvement project. Scoping, literature, and systematic reviews were excluded for the same reason. Articles that addressed written communication needs, mechanisms of support, perception of support, and satisfaction with support of carers of people with mental illness while in hospital were included. Exclusion criteria included articles that did not directly address the support and information needs of carers of inpatient mental health patients, only focused on pediatric patients, or excluded direct representation of family carers.
Note: See Table 1 for a detailed search strategy with the terms used. The databases yielded 12,672 articles (967 duplicates removed, 803 marked as ineligible). A hand search yielded three articles; one was excluded due to the wrong setting. With set limiters of English for the last eight years, the search elicited 2,461 articles. Titles and abstracts were screened from 743 items, and 710 were excluded. Therefore, 36 articles (including three hand-searched records) received a full-text review. In addition, 27 articles were excluded because they did not meet the inclusion criteria, leaving nine articles included. Figure 1 shows the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) diagram shows the number of articles excluded and included for review (Moher et al., 2009a).
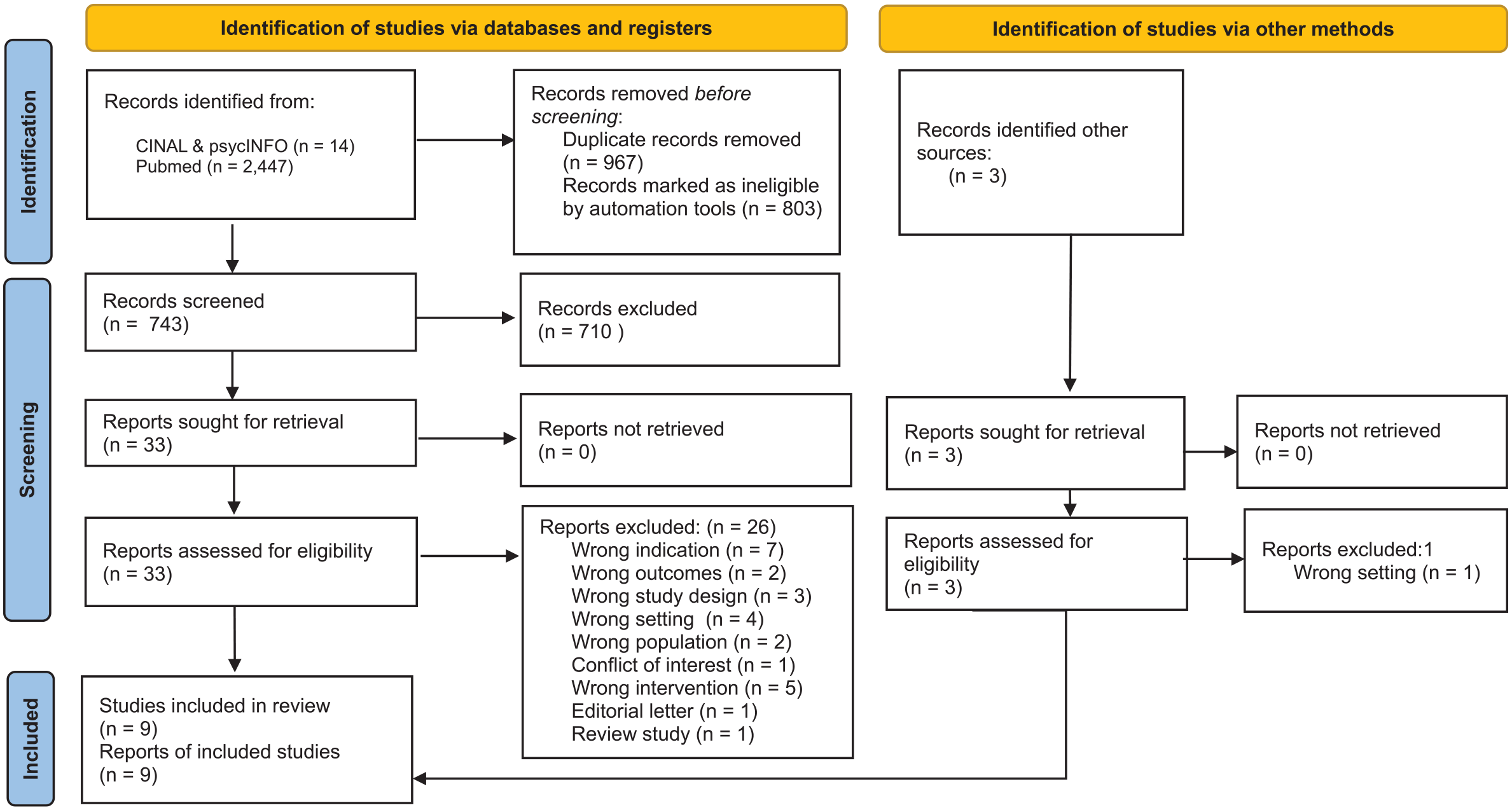
PRISMA flow diagram.
Findings
Nine articles published between 2017 and 2025 met the inclusion criteria and were included for final analysis. The Johns Hopkins Nursing Evidence-Based Practice (JHNEBP) model ranks each article’s level and evidence quality in Table 2 (Dang & Dearholt, 2018). All nine papers were ranked level III, quality B (Anttila et al., 2023; Giacco et al., 2017; Haselden et al., 2019; Hsiao et al., 2019, 2024; Kaselionyte et al., 2019; Schuster et al., 2020; Sercu, 2022; Svendsen et al., 2021).
Table of Evidence.
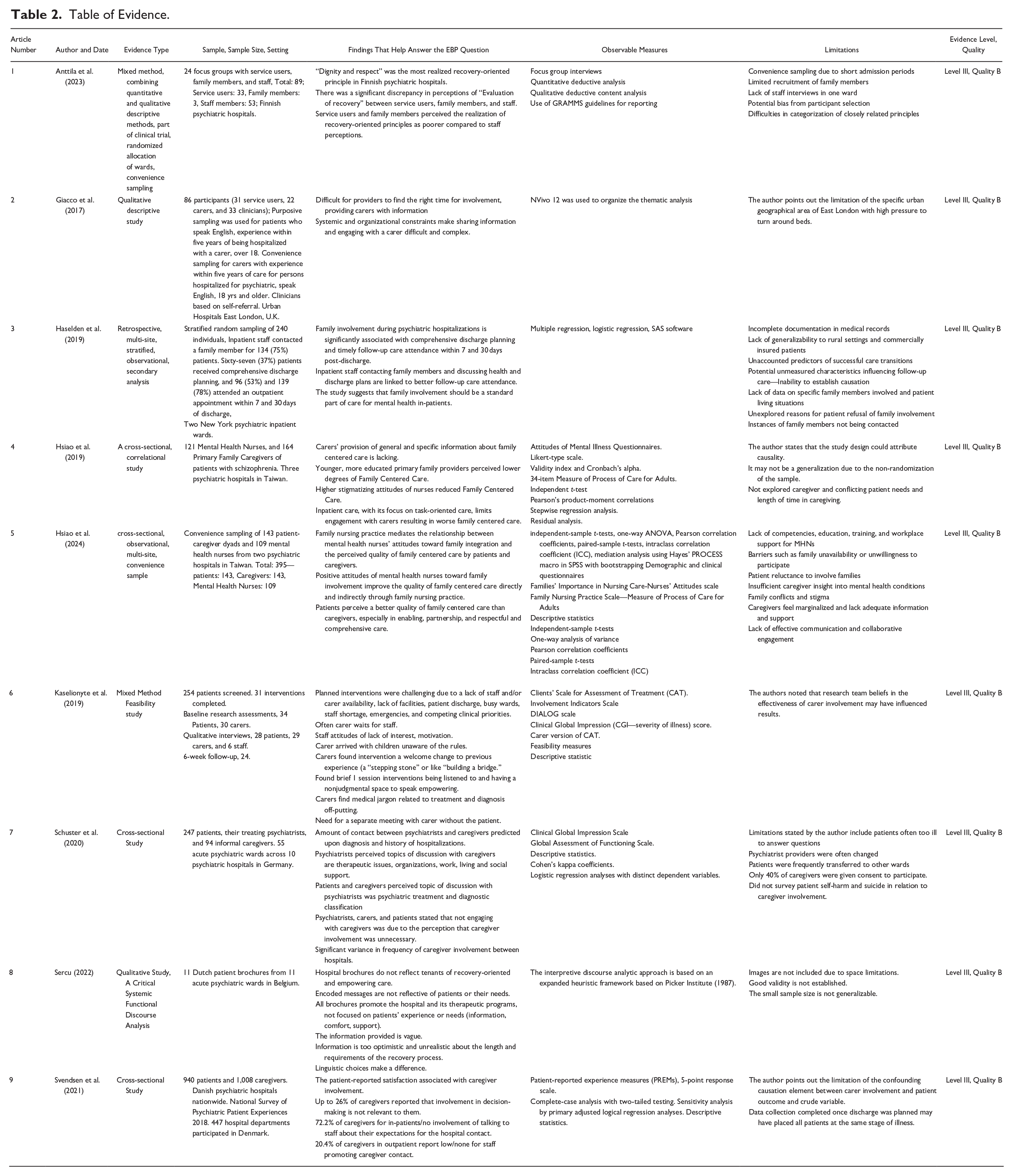
Articles were included from seven countries across the globe: United States (Haselden et al., 2019); Tawain (Hsiao et al., 2019, 2024); United Kingdom (Giacco et al., 2017; Kaselionyte et al., 2019 ); Germany (Schuster et al., 2020); Belgium (Sercu, 2022); Denmark (Svendsen et al., 2021); and Finland (Anttila et al., 2023).
All studies involved some form of provider communication with carers of patients receiving hospitalization for psychiatric illness (Anttila et al., 2023; Giacco et al., 2017; Haselden et al., 2019; Hsiao et al., 2019, 2024; Kaselionyte et al., 2019; Schuster et al., 2020; Sercu, 2022; Svendsen et al., 2021). Eight articles included carers of patients in mental health facilities (Anttila et al., 2023; Giacco et al., 2017; Haselden et al., 2019; Hsiao et al., 2019, 2024; Kaselionyte et al., 2019; Schuster et al., 2020; Svendsen et al., 2021). One of the previously mentioned articles considered carers and patients (Svendsen et al., 2021); another, carers and providers (Hsiao et al., 2019); while five other articles looked at carer, patients, and their providers (Anttila et al., 2023; Giacco et al., 2017; Hsiao et al., 2024; Kaselionyte et al., 2019; Schuster et al., 2020). One retrospective study examined staff contact with carers and patient outcomes (Haselden et al., 2019). Finally, another article examined information brochures for mental health facilities (Sercu, 2022).
The smallest sample sizes were in the 11 to 24 range (Anttila et al., 2023; Sercu, 2022). The largest population included 940 patients and 1,008 caregivers among 447 hospitals (Svendsen et al., 2021). Most studies included 86 to roughly about 300 participants (Giacco et al., 2017; Haselden et al., 2019; Hsiao et al., 2019, 2024; Kaselionyte et al., 2019; Schuster et al., 2020).
This literature review was conducted to explore what kinds of information carers both needed and wanted (Anttila et al., 2023; Giacco et al., 2017; Haselden et al., 2019; Hsiao et al., 2019, 2024; Kaselionyte et al., 2019; Schuster et al., 2020; Sercu, 2022; Svendsen et al., 2021). Themes were found by assessing how information for carers was shared or failed to be shared effectively via providers across the studies. As a result, three main themes have emerged: (a) the information gap, (b) the need for basic information, and (c) empowering caregivers with information.
Among the nine studies, there was a wide variety in study design, including five cross-sectional studies (Hsiao et al., 2019, 2024; Schuster et al., 2020), including an extensive nationwide cross-sectional survey (Svendsen et al., 2021); one multimethod research design (Anttila et al., 2023); two feasibility studies with mixed method components (Haselden et al., 2019; Kaselionyte et al., 2019), and one qualitative approach using a critical discourse analytic framework to examine brochures from 11 acute psychiatric wards (Sercu, 2022). Giacco et al. (2017) used a focus group study with patients, carers, and clinicians. Carer information gaps as a theme came from qualitative data in focus groups and interviews (Giacco et al., 2017) and quantitative data (Hsiao et al., 2019). Carers’ need for basic information was also identified through both qualitative and quantitative methods (Giacco et al., 2017; Schuster et al., 2020). The last theme, the need for carer empowerment, emerged through primarily qualitative data and the interpretation of quantitative results (Anttila et al., 2023; Svendsen et al., 2021). Sercu’s (2022) examination of inpatient psychiatry brochures showed how they failed to provide useful recovery-oriented information to family carers. Despite the various study designs, these themes were consistently seen across multiple studies. This consistency of themes reinforces the importance of these themes around family carers’ need for information in the field of mental health care for carers of patients during inpatient psychiatric care.
Information Gap
There are consistent gaps in education desired by carers for both general and specific information about the patient plan of care, hospital processes, and caregiver rights (Giacco et al., 2017; Hsiao et al., 2019, 2024; Kaselionyte et al., 2019; Schuster et al., 2020; Sercu, 2022; Svendsen et al., 2021). One paper cited that care involvement varied depending on a patient’s diagnosis and the number of hospitalizations (Schuster et al., 2019). Moreover, other studies spoke about the inconsistency in staff communication and about staff not being available (Giacco et al., 2017; Haselden et al., 2019; Hsiao et al., 2019; Kaselionyte et al., 2019; Schuster et al., 2020; Svendsen et al., 2021).
Haselden et al. (2019) also mention the difficulty of a patient withdrawing consent and discharge before carers can be involved. Three studies stress early intervention as important because of these variables (Giacco et al., 2017; Haselden et al., 2019; Kaselionyte et al., 2019). Inconsistencies were based on individual hospital and unit culture (even within the same hospital), time constraints, and competing clinical tasks associated with inpatient care (Anttila et al., 2023; Giacco et al., 2017; Hsiao et al., 2019; Kaselionyte et al., 2019; Schuster et al., 2020; Svendsen et al., 2021).
Hasleden et al. (2019) identified certain groups, such as youth and those with extended hospital stays, as having more family involvement. Schuster et al. (2020) saw diagnosis as a variable of family involvement; those with schizophrenia had more, among other factors. Svendson et al. (2021) found that 72.2% of caregivers reported low or no staff inquiry into their expectations for hospital contact.
In addition, staff attitudes, perceptions, lack of motivation, and lack of acceptance toward those with mental health illness and their carers all contributed to a failure to engage carers (Giacco et al., 2017; Hsiao et al., 2019; Kaselionyte et al., 2019; Schuster et al., 2020). A feasibility study (Kaselionyte et al., 2019) to engage carers exposed the following barriers to involving families: staff availability and motivation, patient mental states, and difficulty contacting carers. In addition, Giacco et al. (2017) found barriers to obtaining patient consent, difficulty identifying carers, and cultural/language barriers. Schuster et al. (2019) found different perceptions between carers and psychiatrists after a meeting; the carers felt that the focus was on treatment and diagnosis, while the psychiatrists felt that they covered therapeutic issues, organization, work, living, and social support. Many psychiatrists, patients, and carers believed carer involvement was unnecessary (Schuster et al., 2020; Svendsen et al, 2021).
Lastly, Sercu (2022) noted that family carer brochures to provide information to families of inpatient psychiatric patients do not provide much specific information to meet family caregivers’ needs so much as to promote the hospital and its services. Hospital brochures failed to promote recovery-oriented principles and offered hollow reassurances (Sercu, 2022). Sercu (2022) pointed out that reassurances that the facility would help the patient can be misleading to family carers by not acknowledging family carers’ long-term role in supporting the patient with a serious mental health diagnosis toward stability (Sercu, 2022). Anttila et al. (2023) compared the perception of recovery-oriented principles by staff versus family and patients. They found that staff consistently rated implementation higher, with “Dignity and respect” as the best implemented and “Evaluation of recovery” as the least (Anttila et al., 2023).
Need for Basic Information
Carers require basic information, not so much about diagnosis and treatment, as meeting the basic needs of navigating the mental health facility and how it works and what is available to them, and practical patient care (Giacco et al., 2017; Hsiao et al., 2019; Schuster et al., 2020; Svendsen et al., 2021). Essential information explains how to communicate with staff or about visitation rules (Giacco et al., 2017; Kaselionyte et al., 2019). The information each carer seeks is realistic, not too vague, overly optimistic about recovery, or too filled with medical jargon (Kaselionyte et al., 2019; Sercu, 2022). Giacco et al. highlight the fact that carers reported feeling frustrated without the provision of information, “left in the dark” and “alone,” and wanting regular updates about patient movement off of the ward, legal rights, and medication (Giacco et al., 2017, p. 13). Two studies indicate that carers felt left out of discharge planning (Giacco et al., 2017; Hsiao et al., 2019). It was noted that carers also need emotional support, crisis planning, and support with decision-making (Giacco et al., 2017; Schuster et al., 2019; Svendsen et al., 2021). Svendsen et al. (2019) found that increased carer involvement, which included receiving information, resulted in patient-reported benefit and satisfaction.
Empowering Caregivers with Information
Evidence supports that caregivers lacked empowerment and felt sidelined or ignored by staff (Kaselionyte et al., 2019; Svendsen et al., 2021). For example, carers are often ignored (Kaselionyte et al., 2019). Alternatively, they arrive at meetings only sadly to discover that children are not allowed because no one has bothered to let them know (Kaselionyte et al., 2019). With this perceived lack of empowerment, 26% of caregivers felt that involvement in decisions was irrelevant to them (Schuster et al., 2019; Svendsen, 2021). In addition, Svendsen et al. (2021) found that 72% of caregivers noted that staff did not engage them about their expectations.
In contrast, when a given intervention, such as taking time to listen to carers openly and non-judgmentally occurs, carers show a dramatically positive response when their feelings and thoughts are heeded (Kaselionyte et al., 2019). Kaselionyte et al. (2019) discovered that even a brief and/or early intervention of a staff meeting with a carer was virtually akin to “building a bridge” or a “stepping-stone,” something quite in contrast to what they had previously experienced with psychiatric hospital staff. Sercu (2022) notes that hospital brochure language fails to empower caregivers or promote person-centered recovery but works to minimize the significance of carer and patient.
Discussion
This review reveals what is known about the information needs of family carers of patients in psychiatric units related to staff and organizations. The emerging themes of information gaps, the need for basic information, as well as carer empowerment, can help providers learn how to meet the needs of carers of patients in acute mental health facilities and identify gaps in the literature. For example, the present findings (Giacco et al., 2017; Haselden et al., 2019; Svendsen et al., 2021) consistently acknowledge and identify with previous research (Carbonell et al., 2020; Doody et al., 2017; Eassom et al., 2014; Mackie et al., 2019) that carer involvement enhances patient outcomes and should be encouraged. Newer research expands on this by showing quantitative evidence of benefits (Haselden et al., 2019) or taking a more nuanced look at things such as optimal timing of intervention (Giacco et al., 2017; Kaselionyte et al., 2019). The themes of carer information gaps are recognized in previous research (Carbonell et al., 2020; Eassom et al., 2014), while newer research through feasibility studies identified real-life barriers to and strategies to improve carer involvement such as staff training, leadership support, and organizational change (Kaselionyte et al., 2019). Current research also offers a more nuanced exploration of stakeholders’ attitudes toward family centered care (Anttila et al., 2023; Hsiao et al., 2019, 2024). In addition, in other examples of how current research expands on previous research, Schuster et al. (2019) explore more deeply into contexts predicting the frequency of family involvement. Sercu (2022) explores how the choice of language communicates to carers in hospital brochures. In summary, these studies provide more detailed quantitative evidence (involvement, barriers) and implementation-focused evidence, offering concrete strategies to expand improvement and a deeper look at communication practices compared to broader findings in earlier research.
However, the literature also highlighted several gaps in carer information needs, including how inpatient psychiatric units fail to communicate in a recovery-oriented language, not only in their patient and carer literature (Sercu, 2022) but in staff interactions with carers (Giacco et al., 2017; Haselden et al., 2019; Hsiao et al., 2019; Kaselionyte et al., 2019; Schuster et al., 2020; Svendsen et al., 2021). Also, it is important to convey to staff that they should listen to and respectfully acknowledge carers as equal collaborators in care (Giacco et al., 2017; Kaselionyte et al., 2019). Another gap is inpatient consent for a carer to speak with staff, which was touched on by most articles but not explored deeply. Another gap was cultural language communication barriers, as Giacco et al. (2017) mentioned.
According to the National Alliance on Mental Illness, 8.4 million people in the United States care for an adult suffering from a mental health illness and spend 32 hours of unpaid work a week providing care (National Alliance on Mental Illness [NAMI] 2023). Given the time carers invest in caring for these individuals, often over a lifetime, it is a gross oversight that such individuals are not actively and systemically engaged in the inpatient process. When carers are not provided basic information about navigating a hospital or visitation rules, their valuable time is wasted with a lack of concern (Kaselionyte et al., 2019; Svendsen et al., 2021). The gaps in care seem to be both systemic (Giacco et al., 2017; Haselden et al., 2019; Hsiao et al., 2019; Kaselionyte et al., 2019) and also due to perceptions and stigmatized attitudes of staff toward the value of involving carers during inpatient care of psychiatric patients (Hsiao et al., 2019; Schuster et al., 2020). Carers also fell into the terrible trap of not valuing themselves and their importance in care outcomes (Schuster et al., 2020; Svendsen et al., 2021).
In contrast, when listened to and engaged by staff, carers feel empowered, emphasizing that recognition and being heard may be more important than the information itself (Giacco et al., 2017; Kaselionyte et al., 2019). Lastly, the literature highlights that the information hospitals provide carers can help to empower and increase engagement with carers through the choice of language. For example, Sercu found that many hospital brochures miss this opportunity by simply promoting the hospital and its treatments and not using recovery-oriented language (2022).
Future research should focus on determining if changes such as the structured and consistent approach to involve families in care, early intervention to involve families, staff training, information packets, required staff meetings or calls to carers, or creating or rewording unit literature to reflect recovery-oriented language would help to meet carer information needs.
Evidence-Based Practice Recommendations
This integrative review suggests that providers can encourage carer involvement in patients with severe mental illness in the hospital simply by effortfully acknowledging them and so empowering them. All providers should, therefore, understand the importance of carers and, as a consequence, prove and exhibit this understanding in their actions and words. Hospital leaders should instill this into the program of care, as studies show how the inclusion of carers in mental health is so crucially dependent on the individual hospital’s culture (Giacco et al., 2017; Kaselionyte et al., 2019; Schuster et al., 2020). This lack of understanding about the importance of carers translates into poor communication. All staff needs to be trained and educated to understand the importance of the carer’s role in patient-improved outcomes. As Hsiao et al. (2024) show, nurses’ attitudes toward family involvement directly impact the quality of family centered care perceived by patients and families (Hsiao et al., 2024).
Organizational leadership should provide the occasion for staff to engage with carers, as many articles highlighted the lack of time providers have to give to carers due to the demands of clinical tasks and emergencies. Carers should be involved early (Giacco et al., 2017; Kaselionyte et al., 2019). Achieving this will require a “top-down” organizational intervention to give staff the time and means to engage carers to support open communication and collaborative decision-making. Kaselionyte et al. (2019) feasibility study of carer involvement intervention in psychiatric inpatient settings found it feasible in 53% of cases and beneficial to improving collaborative care with carer. However, implementing the intervention was not without its challenges.
Communication with carers needs to be improved and more comprehensive (Giacco et al., 2017; Hsiao et al., 2019) to include basic information on unit policies, legal aspects, consent, and more specific information about the patient’s treatment, movements, and discharge planning. Language choices are a powerful tool to use to engage family carers successfully. All communication brochures should be analyzed, updated, or created with this in mind. Sercu (2022) suggests that providing brochures with recovery-oriented language that explains that process instead of reassuring carers that “hospitals” will take good care of their loved ones would be more helpful. Providing information is important, but acknowledging carers as collaborators in care and listening to them is also very empowering (Kaselionyte et al., 2019).
In addition, younger and more educated carers had higher expectations of being included in family centered care (Hsiao et al., 2019), which means that, as time passes, carers may demand change from a medical culture that has traditionally excluded them.
Limitations
All the articles included in the study are Level III, Quality B category and identify the following study limitations of being less generalizable (Giacco et al., 2017; Haselden et al., 2019; Hsiao et al., 2019, 2024; Sercu, 2022); more prone to confounding elements (Svendsen et al., 202) or gaps in participation (Schuster et al., 2020) two studies admits to possible bias (Anttila et al., 2023; Kaselionyte et al., 2019). One study had limited family recruitment (Anttila et al., 2023). Several studies mention a lack of data on specific family members or reasons family members are not involved in care (Haselden et al., 2019; Hsiao et al., 2019, 2024).
Limitations of this review would be the limited number of databases searched and the timeframe of the last 8 years. This study was initially used to support a quality improvement project and was limited to current research. Furthermore, no studies in this review explored health literacy levels and information. In addition, most of the studies were limited to native speakers. Therefore, no consideration of the information needs of non-native speakers was given, except for that of Giacco et al. (2017). Another limitation is that the articles represent countries worldwide that may have more advanced methods of incorporating family centered care than the United States.
Conclusion
This article shows that there are consistent information gaps for family carers of patients in mental health units, and there is a need for comprehensive and accessible information to support carers. Giacco et al. (2017) show that carers need basic information about treatments and hospital procedures, while Hsiao et al. (2019) noted a deficiency in both general and specific information provided to carers. Schuster et al. (2020) and Svendsen et al. (2021) showed that increasing caregiver involvement and information sharing is associated with better patient outcomes. To empower family carers, Hsiao et al. (2024) emphasized the importance of nurses in embracing family nursing practice. Anttila et al. (2023) stressed carrying out and understating recovery-oriented principles by both staff and carers.
For future practice, mental health services administrations should adopt a structured approach to family involvement, involve families in decision-making, provide regular patient progress updates, and train staff in effective family communication (Haselden et al.,2019; Kaselionyte et al. (2019). Families should be given information packages geared to their needs that contain recovery-oriented language (Sercu, 2022). Department leadership should seek consistent ways to engage families (Giacco et al., 2017; Kaselionyte et al., 2019; Schuster et al., 2020).
Future research should focus on determining if changes to involve families in care, staff training, information packets, required staff meetings or calls to carers, or creating or rewording unit literature to reflect recovery-oriented language would help to meet carer information needs.
By addressing information gaps, supporting family information needs, and empowering carers, mental health services can enhance care quality, improve patient outcomes, and strengthen families’ essential role in the healing process of patients seeking help for mental illness.
Footnotes
Acknowledgements
Ellen Carty, PMHNP, FNP, PNP; Diane Meyer, PhD, RN, MPH; Carla Aquino, DNP, RN; Donna Hesson, MLS; Stella M. Seal, MLS; Mirinda Tyo, PhD, RN, TCRN; Kari Mofford, MLS; Alexander Theroux, PhD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.