
Abstract
The prevalence of poor sleep quality tends to increase progressively as renal function deteriorates. Patients with declining kidney function frequently encounter both physical and psychological discomfort. However, research investigating the factors influencing sleep quality in individuals with early-stage chronic kidney disease (CKD) has been limited. This study aims to identify specific factors associated with early-stage CKD that may contribute to poor sleep quality and to elucidate the relationship between these factors and sleep quality. A hundred and six patients completed the assessment, including the renal function test, Pittsburgh Sleep Quality Index, Beck Depression Inventory-Second Edition, and fatigue severity scale. Logistic regression analyses and partial least squares structural equation modeling were used to analyze the data. Poor sleep quality was reported in 59.43% of patients with early-stage CKD. Significant associations were found between poor sleep quality and age (p < .01; 95% confidence interval: [1.03, 1.17]), severity of depression (p = .01, [1.05, 1.48]), and severity of fatigue (p = .02, [1.09, 2.71]). By contrast, estimated glomerular filtration rate (eGFR) (p = 0.53, [0.96, 1.02]) did not demonstrate a significant association with poor sleep quality. Further analysis revealed that fatigue and depression are key contributors to poor sleep quality and may be influenced by declining renal function, even though the eGFR is not directly related to sleep outcomes. Addressing psychological factors, particularly fatigue and depression, is crucial for the improvement of sleep quality in patients with early-stage CKD. Future strategies should be focused on comprehensive care approaches that specifically target fatigue and depression to enhance sleep quality in this patient population.
Introduction
The prevalence of poor sleep quality among patients with chronic kidney disease (CKD) has been reported to be 64%, highlighting a common and significant issue that adversely affects the overall health and quality of life of these patients (Tan et al., 2022). CKD has been classified as having five stages based on estimated glomerular filtration rate (eGFR) and other markers of kidney damage, with stages 1–3 typically representing the early stages of the disease (Inker et al., 2014; Qaseem et al., 2013). The eGFR is used in the clinic to diagnose and treat CKD early (Cusumano et al., 2021). The early stages of CKD are generally asymptomatic (Chen et al., 2019). Studies have shown that CKD awareness among the general population is low, with only 19.2% of individuals being aware of their condition. Consequently, many individuals with early-stage CKD fail to recognize their disease, particularly in its initial phases (Chu et al., 2021). Poor sleep quality is a common complaint among patients with CKD and tends to worsen as renal function declines (Gela et al., 2024; Ogna et al., 2016). Several factors contribute to poor sleep quality in these patients, such as sensory-reflex dysfunction, sympathetic nervous system imbalance, vagus nerve effects on the hyperactive sympathetic nervous system, decreased vagus nerve tone, sleep-mediated metabolism changes, systemic inflammation, and uremia (Hildreth, 2011; Lindner et al., 2015; Neumann et al., 2004). Additionally, age and obesity can affect sleep quality (Pinto et al., 2021; Tan et al., 2022).
As CKD progresses, patients experience more physiological and psychological discomfort, with fatigue and depression being the most common symptoms (Fletcher et al., 2022). Sleep, fatigue, and depression mutually influence one another (Gregg et al., 2021; Kahn et al., 2013), and their relationship is often accompanied by insomnia and poor sleep quality (Tan et al., 2022). Fatigue in CKD results from various pathophysiological factors (Gregg et al., 2021); it is a multifaced and subjective feeling (Phillips, 2015) characterized by tiredness, weakness, exhaustion, and discomfort (Wessely, 2001) and is present in patients with stages 2–3 CKD (Gregg et al., 2021). The prevalence of fatigue increases with disease progression, reaching 42–89% in patients with terminal kidney disease (Artom et al., 2014 Depressive symptoms are frequently observed in nondialysis patients with CKD, and their prevalence increases as renal function declines.). (Duan et al., 2021; S. Palmer et al., 2013a). These symptoms increase the risk of death and have adverse effects on quality of life (Alshelleh et al., 2022; Palmer et al., 2013b). Despite these insights, a significant research gap remains in understanding the complex interplay between these factors and how they collectively contribute to poor sleep quality in patients with early-stage CKD.
Previous studies have demonstrated that age, sex, and body mass index (BMI) are associated with depressive symptoms (Hawes et al., 2019). Additionally, fatigue, poor sleep, and depression are prevalent symptoms among nondialysis patients with CKD, and these burdens tend to worsen with declining renal function (Fletcher et al., 2022; Huang et al., 2023). Early detection plays a crucial role in preventing CKD, slowing its progression and mitigating its complications (Anna Francis et al., 2024). However, studies have consistently shown that public awareness of CKD remains low, which may contribute to delayed diagnosis and suboptimal disease management (Chu et al., 2021; A. Francis et al., 2024). While sleep disturbances are increasingly recognized as a common issue among CKD patients, research exploring the specific factors influencing sleep quality in individuals with early-stage CKD remains limited. Existing studies have primarily focused on patients with advanced CKD or those undergoing dialysis, leaving a gap in understanding how sleep disturbances manifest in the early stages of the disease. Identifying key determinants of sleep disturbances in patients with early-stage CKD is crucial for informing targeted interventions aimed at improving patient symptom management and quality of life. Given the low level of public awareness of CKD, such insights may also promote earlier recognition of the disease and more comprehensive care planning. Therefore, this study aims to examine the specific factors associated with early-stage CKD that contribute to poor sleep quality and to elucidate their relationships with sleep quality. By doing so, we seek to provide insights for tailored interventions aimed at improving sleep quality and overall health outcomes in this population. To achieve these objectives, we conducted a cross-sectional study and hypothesized that lower eGFR contributes to poorer sleep quality through increased fatigue and depressive symptoms in patients with early-stage CKD. Understanding these factors could provide valuable insights for public health policymakers, enabling them to implement targeted strategies that guide and educate early-stage CKD patients on improving their sleep quality.
Methods
Participants
In this descriptive cross-sectional study, enrollment commenced after the study received approval from the Institutional Review Board on December 31, 2021, with the IRB number of IRB110-291-B. Convenience sampling was used from July 2022 to December 2022, and a structured questionnaire was used for data collection. Patients diagnosed with stage 1–3a CKD by a physician, based on standard diagnostic criteria, were recruited as participants at the nephrology outpatient clinic of a regional hospital in Taiwan. CKD is classified into stages based on glomerular filtration rate and other indicators of kidney damage. Stage 1 is glomerular filtration rate more significant than 90 mL/min/1.73 m², which is normal, but there are some signs of kidney damage on other tests (e.g., Blood or protein leak in urine). Stage 2 involves a slightly reduced glomerular filtration rate (60–89 mL/min/1.73 m²) with additional signs of kidney damage. Stage 3a is defined by a moderately reduced glomerular filtration rate (45–59 mL/min/1.73 m²). The inclusion criteria were as follows: patients who (1) were aged 20–80 years, (2) were literate and able to read and write Chinese, (3) did not work shifts in the last month, and (4) were not pregnant. G-Power 3.1 was used in this study, and linear multiple regression analysis was employed to estimate the sample size with an effect size (f2) = .15, α = .05, and power = .80. The estimated minimum sample size was 85.
Measures
Basic Demographic Questionnaire
The primary demographic questionnaire included data on the patient's gender, age, BMI, eGFR, CKD stage, and classification of diseases.
Pittsburgh Sleep Quality Index
The Pittsburgh Sleep Quality Index (PSQI) is a self-rated questionnaire to evaluate a patient's sleep quality within the previous month. The index comprises seven dimensions: subjective sleep quality, sleep latency, total sleep time, habitual sleep efficiency, sleep disorders, use of sleep medications, and daytime dysfunction. The questionnaire consists of 19 questions, each scored from 0 to 3. The total score ranges from 0 to 21, with higher scores indicating poorer sleep quality (Buysse et al., 1989). The Chinese version of the PSQI demonstrates good internal consistency (Cronbach’s α = .82–.83) and a test-retest reliability of 0.85 over a 14- to 21-day interval, with primary insomnia having a test-retest reliability of 0.77. Cronbach’s α for the PSQI in this study was 0.76, indicating acceptable internal consistency. A study found that a total score of 5 had a sensitivity of 98% and specificity of 55% in identifying sleep disorders (Tsai et al., 2005).
Beck Depression Inventory-Second Edition
The Beck Depression Inventory-Second Edition (BDI-II) is a self-rated questionnaire with 21 questions, with each item scored as 0 to 3 points on a scale. The total score ranges from 0 to 63, with higher scores indicating greater severity of depression and scores of 0 to 13 points being considered as a standard range (Beck et al., 1996). The Chinese versions of the BDI-II have demonstrated good reliability and validity (Che et al., 2006). Cronbach’s α for the BDI-II in this study was 0.88, indicating good internal consistency.
Fatigue Severity Scale
The fatigue severity scale (FSS) is a self-rated questionnaire used to evaluate the severity of fatigue and its impact on daily life over the past week. It comprises nine questions, with 1–7 points scored per question. A higher score indicates greater fatigue severity, and a score >4 indicates the presence of fatigue (Krupp et al., 1989). The Chinese version of the FSS has good validity and reliability (Feng et al., 2019). Cronbach’s α for the FSS in this study was 0.89, indicating good internal consistency.
Statistical Analysis
After the questionnaires were collected, the data were coded and entered into a computer. Statistical analyses were performed using SPSS version 27.0. Descriptive statistics were used to summarize participants’ demographic and clinical characteristics. Continuous variables were expressed as mean ± standard deviation. Categorical variables were presented as frequencies. Independent t-tests were conducted to compare continuous variables, including age, BMI, the eGFR, the BDI-II score, and the FSS score, between good sleepers (PSQI ≤ 5) and poor sleepers (PSQI > 5). Chi-squared tests were used to examine group differences in categorical variables such as gender, the CKD stage, and the classification of kidney disease between the two sleep quality groups. A p-value <.05 was considered statistically significant. Logistic regression analyses were conducted to identify risk factors associated with sleep quality. The model included age, the eGFR, the BDI-II score, and the FSS score. These variables were selected based on their statistical significance in univariate analyses and their established clinical relevance. Among the variables related to kidney function (the eGFR, CKD stage, and disease classification), only the eGFR was included in the multivariable model. It was selected because it is a continuous variable and a widely accepted clinical indicator, offering greater sensitivity in the detection of subtle changes in renal function than categorical classifications. The results are presented as adjusted odds ratios with 95% confidence intervals (CI), providing insight into the strength and direction of the associations between these variables and sleep quality. Structural equation modeling (SEM) with partial least squares (PLS) and bootstrapping was used to examine the direct effects of the eGFR, fatigue, and depression on sleep quality. The research model was constructed using SmartPLS 4, and bootstrapping was applied to assess the significance of the relationships between constructs. The research model was constructed using SmartPLS 4 (SmartPLS GmbH, Boenningstedt, Germany). Bootstrapping offers the advantage of conducting inferential analysis without strict data distribution limitations.
Results
Participant Characteristics
Table 1 presents the patient characteristics, including group comparisons between good sleepers (PSQI ≤ 5) and poor sleepers (PSQI > 5). In total, 106 patients met the inclusion criteria. The mean age of the sample was 64.24 ± 9.77 years. In terms of disease characteristics, the majority of participants were diagnosed with stage 1 CKD (63.20%), with a mean eGFR of 93.88 ± 18.29 mL/min/1.73 m2. Significant differences emerged between good and poor sleepers across several key variables. Poor sleepers were older on average (67.27 ± 8.47 years) than good sleepers (59.79 ± 9.95 years). The eGFR was significantly lower in poor sleepers (89.74 ± 19.28 mL/min/1.73 m2) than that in good sleepers (99.95 ± 14.98 mL/min/1.73 m2), suggesting that reduced kidney function is associated with poorer sleep quality. Furthermore, both fatigue and depression symptoms were significantly more severe in poor sleepers (FSS: 4.40 ± 1.05; BDI-II: 7.52 ± 4.75) than those in good sleepers (FSS: 3.20 ± 1.22; BDI-II: 3.07 ± 2.81; all p-values <.001). These results indicate strong negative associations among fatigue, depression severity, and sleep quality. A significant difference in CKD stage distribution was also observed between the two groups (p = .027). A larger proportion of poor sleepers was classified as having stage 2 CKD (50.79%) than good sleepers (16.28%). These findings underscore the influence of clinical and psychological factors—particularly fatigue, depression symptoms, and declining kidney function—on sleep quality among patients with CKD.
Participant Characteristics and Sleep Quality Comparisons.
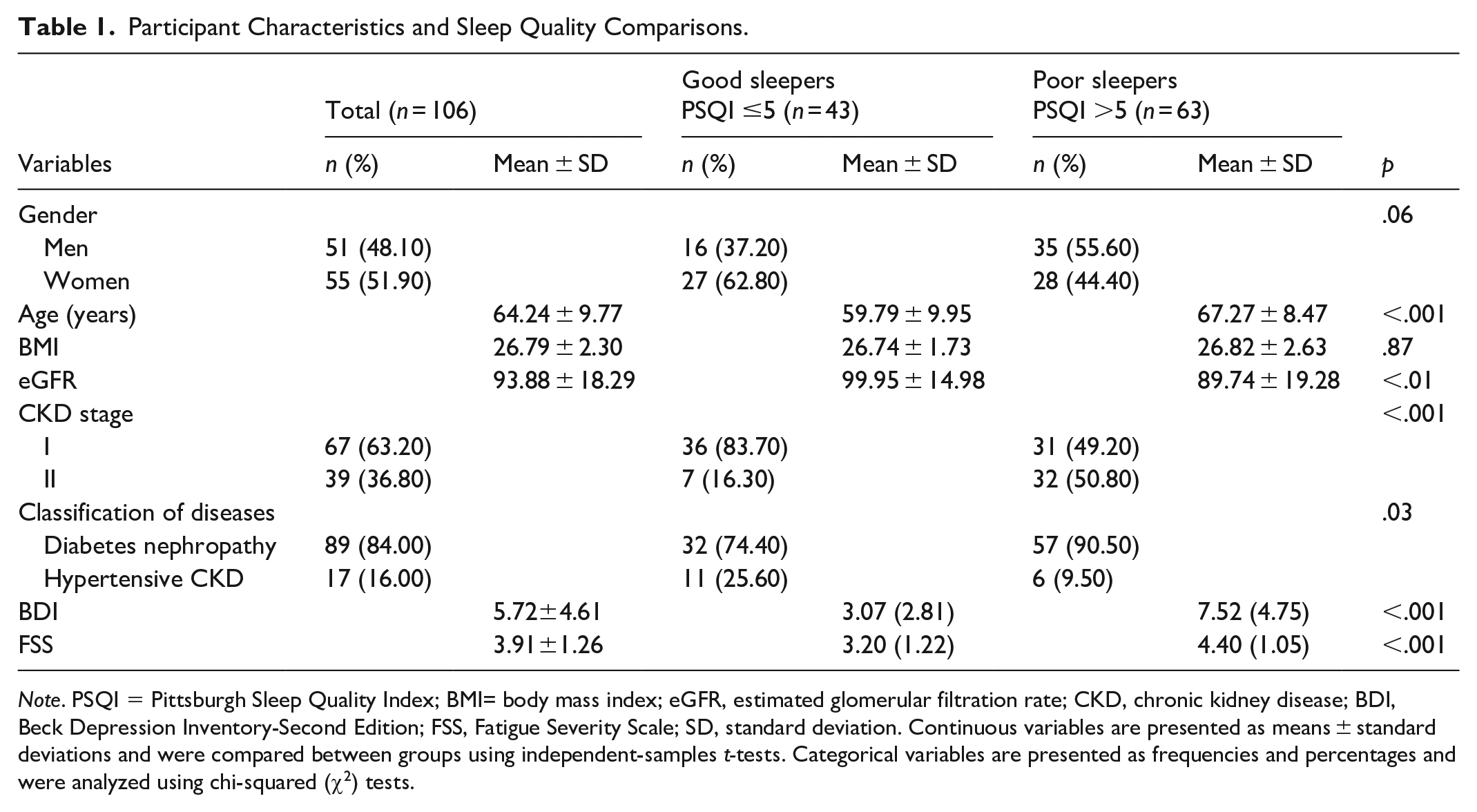
Note. PSQI = Pittsburgh Sleep Quality Index; BMI= body mass index; eGFR, estimated glomerular filtration rate; CKD, chronic kidney disease; BDI, Beck Depression Inventory-Second Edition; FSS, Fatigue Severity Scale; SD, standard deviation. Continuous variables are presented as means ± standard deviations and were compared between groups using independent-samples t-tests. Categorical variables are presented as frequencies and percentages and were analyzed using chi-squared (χ2) tests.
Predictive Factors Associated With Poor Sleep Quality
Logistic regression analysis was used to identify predictive risk factors for poor sleep quality, including age, eGFR, severity of depression, and severity of fatigue. The multivariable results indicated that age (p < .01; 95% CI [1.03, 1.17]), the severity of depression (p = .01, [1.05, 1.48]), and the severity of fatigue (p = .02, [1.09, 2.71]) were significantly associated with poor sleep quality, while the eGFR (p = .53, [0.96, 1.02]) was not. For further details, refer to Table 2.
Results of Logistic Regression Analyses of Factors Associated With Poor Sleep Quality, as Denoted by a OR (95% CI).
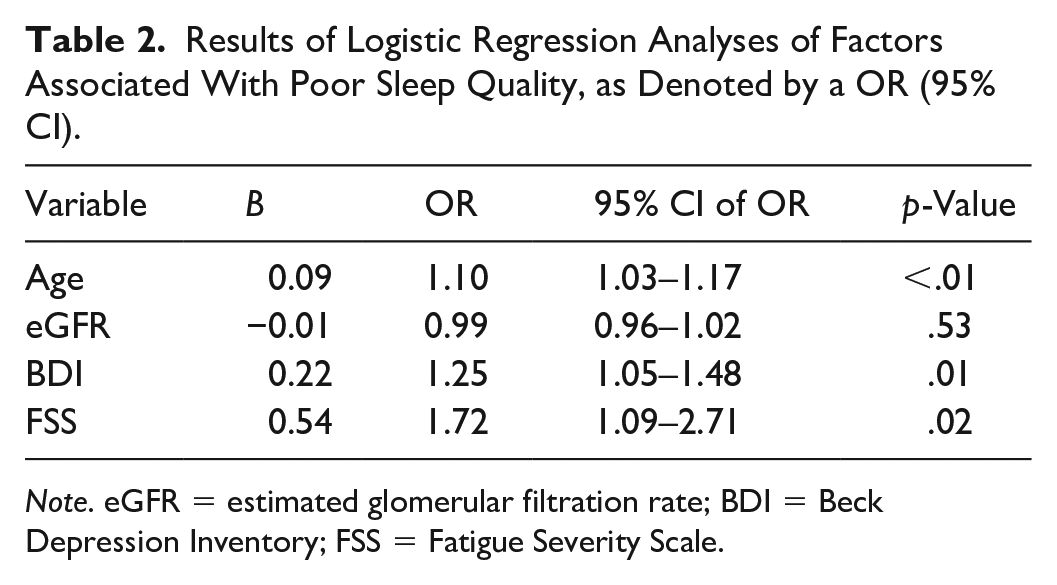
Note. eGFR = estimated glomerular filtration rate; BDI = Beck Depression Inventory; FSS = Fatigue Severity Scale.
After controlling for confounders, the eGFR was shown not to have a significant direct effect on sleep quality (β = −.03, [−0.19, 0.14]). However, fatigue and depression exhibited significant direct effects, both emerging as strong predictors of sleep quality. These findings indicate that although the eGFR is not directly related to sleep quality, fatigue and depression are critical contributors to sleep outcomes, and these contributors may themselves be influenced by a decline in kidney function (Figure 1).
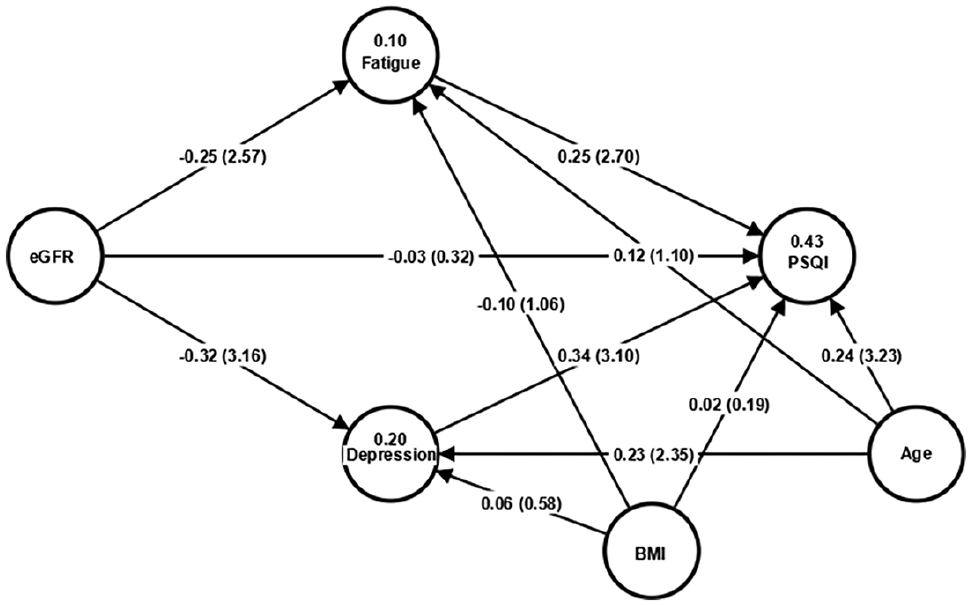
Structural equation modeling with partial least squares analysis of eGFR, fatigue, and depression on sleep quality.
Discussion
In our study, 59.43% of patients with early-stage CKD reported poor sleep quality, which was significantly associated with age, depression, and fatigue. These findings provided valuable insights into the complex interplay between kidney function decline and sleep quality, mainly through the mediating roles of fatigue and depressive symptoms. Notably, while eGFR did not directly affect sleep quality, its impact was indirectly mediated by both fatigue and depressive symptoms. Our findings indicated that eGFR was not significantly associated with sleep quality in patients with early-stage CKD. One possible explanation is that our study population consisted of early-stage CKD patients. Stage 1 CKD is characterized by a glomerular filtration rate values >90 mL/min/1.73 m², which falls within the normal range but is accompanied by signs of kidney damage. Since an eGFR in this range is generally considered indicative of normal renal function, it is plausible that their kidney function was not the primary determinant of sleep quality. Instead, sleep disturbances in these patients may have been influenced by other factors commonly seen in CKD, such as inflammation or psychological distress, rather than by reduced renal clearance per se (Han et al., 2020; Lindner et al., 2015). Fatigue and depressive symptoms contributing to poor sleep quality align with the findings of previous research (Al Naamani et al., 2021; Ho et al., 2022).
Studies have shown similar associations among eGFR, fatigue, and sleep quality. Patients with CKD often experience fatigue, which affects their sleep quality (Hsu & Yang, 2022). This supports our finding that fatigue serves as a crucial mediator in the relationship between eGFR and sleep quality. Additionally, previous research by Huang et al. (2023) highlighted the prevalence of depressive symptoms in CKD patients and their strong correlation with sleep quality. Our study further corroborates these findings by demonstrating that depressive symptoms significantly mediate the effect of eGFR on sleep quality. However, some differences exist between our study and previous literature. While certain studies have reported a direct association between kidney function and sleep quality (Gela et al., 2024), our findings did not support this direct link. One possible explanation for this discrepancy could be differences in the disease severity. Our study focused on patients with predominantly early-stage CKD, whereas previous studies often included patients with more advanced CKD stages. This highlights the need for further research to determine whether the impact of kidney function on sleep quality varies across different CKD stages.
Our study adds to the growing body of evidence emphasizing the complex interplay among kidney function, fatigue, depressive symptoms, and sleep quality. Our findings suggest that interventions targeting fatigue and depression in patients with early-stage CKD may help improve sleep quality, even in the presence of only mildly to moderately reduced renal function or renal damage with albuminuria. Future longitudinal studies are warranted to establish causal relationships and explore additional mediators that may further explain the link between early-stage CKD and sleep disturbances. Additionally, clinical caregivers should assess patients with early-stage CKD for symptoms of fatigue and depression and implement appropriate interventions to prevent symptom deterioration and its subsequent effect on sleep quality.
This study has several strengths. First, it focuses on early-stage CKD patients, a population that has been relatively underexplored. Second, by identifying fatigue and depressive symptoms as mediators, it enhances the understanding of potential mechanisms contributing to poor sleep quality in early-stage CKD. However, this study also has limitations. First, given the cross-sectional study design, we could not determine causality. The participants in future studies should include patients from different regions, and a cohort study should be conducted to examine causality. Second, there was a lack of objective data on sleep quality evaluation; therefore, the actual situation could not be presented. Objective sleep quality data should be collected using validated physiological measures to gain a better understanding of actual sleep conditions. Third, the initial sample size estimation was performed for linear multiple regression; however, the primary analyses in this study were conducted using logistic regression and SEM, which differ methodologically from linear regression. As a result, the originally assigned power level may no longer be an accurate reflection of the statistical power associated with the methods employed in the main analyses. Moreover, the relatively small sample may have limited both the statistical power and the generalizability of the findings. Future researchers should aim to recruit sufficiently large samples according to the statistical techniques they will use to validate our results and verify their applicability to broader populations.
Conclusions
This study highlighted that fatigue and depression are key contributors to poor sleep quality and may be influenced by declining renal function, even though the eGFR is not directly related to sleep outcomes. These findings underscore the need for a comprehensive approach to early-stage CKD management that includes assessments and interventions for fatigue and depressive symptoms to improve sleep outcomes. Furthermore, the observed discrepancies with previous studies suggest that the impact of eGFR on sleep quality may vary across different CKD stages. Future research should further explore these variations and investigate additional biological mechanisms that may contribute to poor sleep quality in early-stage CKD patients.
Footnotes
Ethical Considerations
This descriptive cross-sectional study was conducted at a regional hospital and was approved by the Research Ethics Committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available to the corresponding author, upon reasonable request.