
Abstract
Family caregivers (FCGs) of cancer patients play a critical role in providing emotional and physical support. Mindfulness-based interventions (MBIs) have been increasingly explored as a potential approach to improving the psychological well-being of FCGs. However, the caregiving burden often results in significant psychological distress, including stress, anxiety, and depression. This systematic review and meta-analysis aims to evaluate the effects of MBIs on the stress, anxiety, and depression of FCGs of cancer patients. This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis 2020 guidelines and was registered in PROSPERO. A comprehensive search was conducted in PubMed, Cumulative Index to Nursing and Allied Health Literature, PsycINFO, Cochrane Library, ERIC, and Google Scholar to identify relevant studies published between 2010 and 2024. Randomized controlled trials (RCTs) and quasi-experimental (QE) studies assessing MBIs’ impact on psychological outcomes in FCGs were included. Risk of bias was evaluated using the Joanna Briggs Institute Critical Appraisal Checklists. A total of 10 studies (5 RCTs and 5 QE studies) met the inclusion criteria. Meta-analysis results demonstrated that MBIs significantly reduced anxiety and depression in FCGs of cancer patients compared to usual care or no intervention. Effect sizes varied across studies, with moderate to strong effects observed for anxiety, while depression showed smaller but significant improvements. However, the meta-analysis on stress yielded non-significant results with moderate-to-high heterogeneity. The heterogeneity across studies was moderate, suggesting variability in populations, measurements, intervention formats, duration, and delivery methods. MBIs are effectively improving the psychological well-being of FCGs by reducing anxiety and depression. Given the significant caregiving burden, integrating MBIs into caregiver support programs could enhance their resilience and overall mental health. Future research should explore culturally adapted mindfulness interventions to optimize their applicability in diverse caregiving populations.
Keywords
Introduction
Informal caregivers, often referred to as family caregivers (FCGs), play a crucial role in cancer care by providing patients with a range of support services, including assistance with daily living activities, medical care tasks, emotional and social support, and advocacy with healthcare providers and insurance companies (Berry & Mate, 2016). An estimated 4.6 million Americans act as informal caregivers for loved ones battling cancer, offering vital support within the home environment (Berry et al., 2017). The International Agency for Research on Cancer has reported in Pakistan that the proportion of newly diagnosed cancers is 0.18 million, the number of cancer fatalities is 0.11 million, and the number of prevalent cases (5 years) is 0.32 million, who are being taken care of by their FCGs (Ali et al., 2022). However, the demands of this vital role often exceed the caregivers’ level of preparedness, particularly among family members and close friends who assume this position. A mismatch between expectations and resources can lead to considerable physical and emotional strain for the caregiver, potentially translating into suboptimal care and outcomes for the patient (Berry et al., 2017).
The term FCG encompasses anyone who provides informal emotional and physical support for a sick family member, be it at home or within the hospital setting. This role often encompasses parents, adult children, spouses, and other close relations. As such, the FCG of a cancer patient can be considered an essential member of the healthcare team (Ferrell et al., 2019; Zavagli et al., 2019). Especially in Pakistan, the extent of care provided by FCGs within hospitals due to nurse shortages is significant (Ghaffar et al., 2021). This uncharted territory can elicit a complex range of emotions, including worry, anger, and despair, particularly for women in the family, such as wives or daughters, who often take on caregiving roles (Zavagli et al., 2019).
FCGs need proper support to effectively manage their caregiving responsibilities while maintaining their own well-being (Cai et al., 2021). To meet the needs of FCGs, healthcare professionals should offer targeted interventions (Türkoğlu & Kavuran, 2024). Among the various interventions, the mindfulness-based interventions (MBIs) are effective in alleviating symptoms such as anxiety, stress, fatigue, chronic pain, and depression (Li et al., 2023). MBIs treat different psychological disorders, such as depression (Bower et al., 2021), anxiety disorders (Türkoğlu & Kavuran, 2024), and post-traumatic stress disorder (Schure et al., 2018) among the patients.
Mindfulness is generally defined as a state of awareness that emerges through intentionally focusing on the present moment without judgment (Schuman-Olivier et al., 2020). The term “mindfulness” was first translated in 1881 by English scholar Rhys Davids from the Pali term sati used in Buddhist texts, which originally conveyed meanings such as “memory,” “recollection,” “awareness of specific facts,” and has also been interpreted as “lucid awareness” or “bare attention” (Schuman-Olivier et al., 2020). Mindfulness, which involves cultivating focused attention on the present moment with a receptive and nonjudgmental attitude, has proven to be a valuable approach for easing symptoms of anxiety and depression in patients (Kubo et al., 2019).
MBIs are structured programs that use mindfulness practices, such as meditation, body awareness, and mindful breathing, aimed at increasing awareness of the present moment and reducing negative psychological patterns (Zhang et al., 2021). These interventions were designed to help FCGs of cancer patients manage their psychological well-being, which includes reducing stress, anxiety, depression, and psychological distress (Fish et al., 2014). Recent research suggests that mindfulness training can alleviate both psychological and physical symptoms (Johns et al., 2020). This intervention has been modified and utilized to address various challenges, including stress (Song & Lindquist, 2015), suicidal thoughts (Serpa et al., 2014), and cancer-related concerns (Kubo et al., 2019). Research indicates that it is an effective approach for alleviating stress and enhancing both the physical and emotional well-being of caregivers tending to cancer patients (Al Daken & Ahmad, 2018; Ranjbar Noei et al., 2023; Vinci et al., 2021).
FCGs of cancer patients in Pakistan endure significant psychological burdens, including high levels of stress, anxiety, and depression, which can impair their well-being and caregiving capabilities (Ali et al., 2022). While MBIs have been studied internationally for their potential to alleviate such psychological challenges, there is limited synthesized evidence on their effectiveness specifically for Pakistani caregivers. Existing studies have yet to conclusively determine the impact of MBIs on the psychological well-being of cancer caregivers in culturally diverse and resource-limited settings like Pakistan.
Pico
Operational Definitions
Mindfulness
Traditionally, mindfulness has been described as “a state of presence of mind which concerns a clear awareness of inner and outer experiences, including thoughts, sensations, emotions, actions or surroundings as they exist at any given moment” (Schuman-Olivier et al., 2020).
Mindfulness-Based Stress Reduction
Originally designed as a structured treatment program for managing chronic pain, mindfulness-based stress reduction (MBSR) has since been widely adopted to alleviate psychological distress linked to chronic illnesses. It is also used to address emotional and behavioral disorders. Research findings have been promising, with recent controlled trials demonstrating significant reductions in psychological distress associated with various medical conditions (Niazi & Niazi, 2011).
Psychological Well-Being
MBIs are designed to help FCGs of cancer patients manage their psychological well-being, which includes reducing stress, anxiety, and depression. To assess the impact of MBIs on FCGs’ psychological well-being, the following outcome variables will be assessed:
Objectives
The aim of this systematic review is as follows:
To systematically review and synthesize existing research on the effects of MBIs on the psychological well-being, including anxiety, depression, and stress, of FCGs of cancer patients.
Methods
Study Design
This systematic review was planned, conducted, and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 guidelines (Page et al., 2021). The review is registered in PROSPERO.
Eligibility Criteria
Inclusion Criteria
Studies including FCGs of adults diagnosed with cancer.
Studies on the human species were selected.
Studies evaluating MBIs delivered in individual or group formats were included.
Studies that report having measured specifically stress, anxiety, and depression.
Randomized controlled trials (RCTs) and quasi-experimental (QE) studies, published in peer-reviewed journals from 2010 to 2024 with no geographical limitations.
Exclusion Criteria
Studies that focus on professional caregivers or domestic helpers.
Studies in languages other than English or Urdu, unless translations are available.
The PRISMA flowchart in Figure 1 provides a detailed overview of the study selection process and reasons for exclusion.
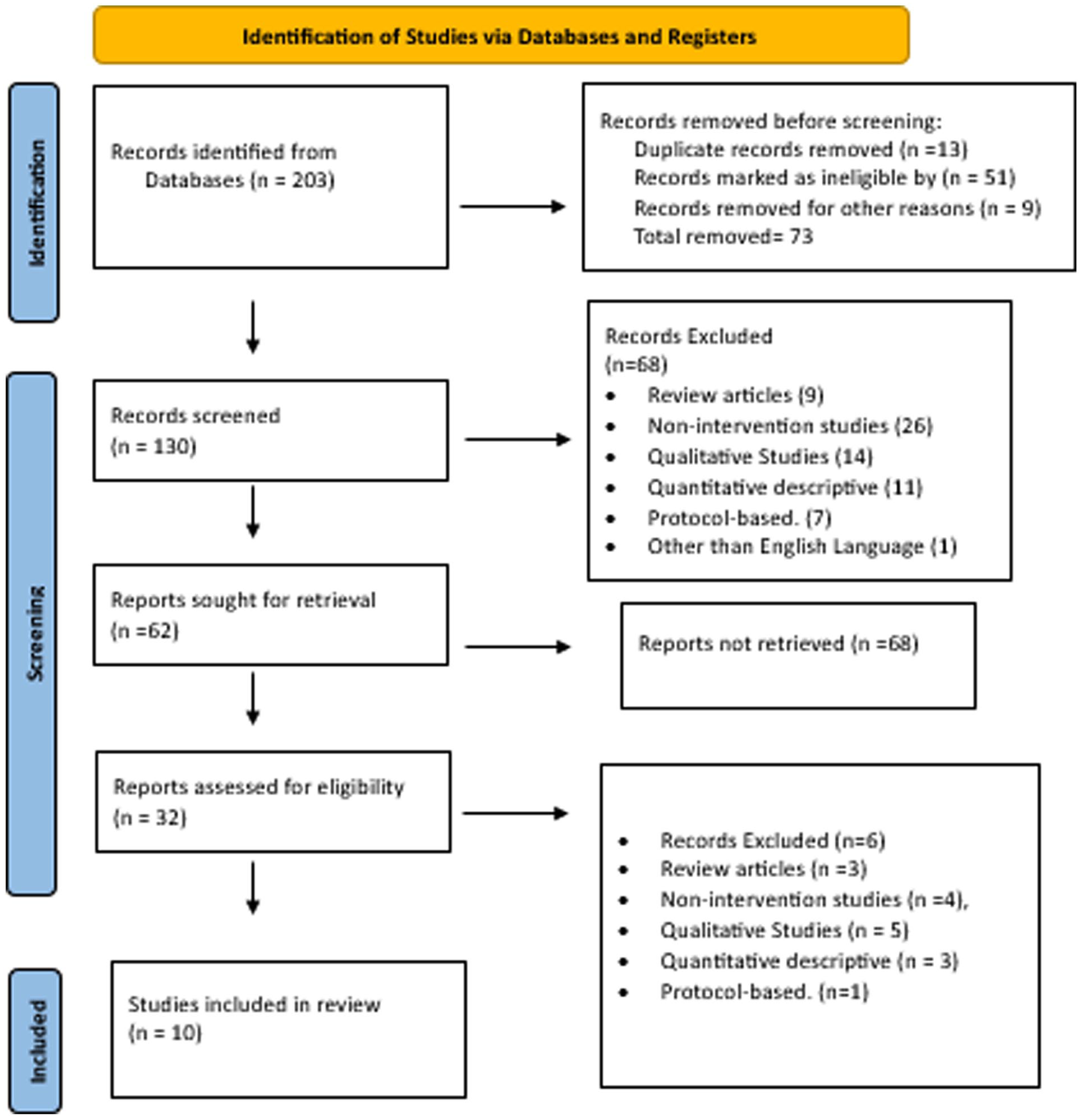
PRISMA flow diagram of the search strategy.
Search Strategy
A comprehensive search was conducted using electronic databases to identify relevant studies published between 2010 and 2024. The search strategy utilized multiple databases, including PubMed, Cumulative Index to Nursing and Allied Health Literature, PsycINFO, Cochrane Library, ERIC, and Google Scholar. The librarian at Shifa Tameer-e-Millat University was consulted, and he (A.U.) provided valuable assistance in conducting searches for relevant studies across various academic databases. Search terms were systematically developed to encompass the main focus of this review: MBIs, FCGs, and psychological outcomes such as anxiety, depression, and stress. Boolean operators (AND, OR) were employed to refine and expand the search results as needed. The specific keywords and Mesh terms used included: “Mindfulness-based interventions” OR “Mindfulness-based stress reduction” OR “Mindfulness-based cognitive therapy”) AND “family caregivers” OR “cancer caregivers” AND “psychological well-being” OR “stress” OR “anxiety” OR “depression.” Figure 1 illustrates the search results.
Selection Process
The systematic search initially yielded 203 articles. After removing 73 duplicate and ineligible records, 130 abstracts were screened. Of these, 68 studies were excluded based on title and abstract, leaving 62 reports for retrieval. Following a full-text assessment of 32 eligible reports, 22 were excluded for not meeting intervention criteria, resulting in the final inclusion of 10 studies (5 RCTs and 5 quasi-experimental studies) for qualitative and quantitative synthesis. A second reviewer (S.S.) independently conducted a search of the aforementioned databases using the same keywords, confirming the initial search findings. Another reviewer (S.I.) checked accuracy, and discrepancies were resolved with a forth reviewer (E.F.). Studies were screened using an eligibility form, and reference lists were manually reviewed to find additional relevant articles. Duplicates were removed using Mendeley. The timeframe for studies was 2010 to 2024.
Data Extraction
Data extraction was performed using an Excel sheet (Tables 1a, b and 2a, b), which systematically captured study characteristics such as authors, publication year, country, study design, sample size, and caregiver demographics. Intervention details, including the type of MBI, duration, delivery method, and mode of delivery (group-based), were also recorded. Outcomes were reported as differences in scores and standard deviations for stress, anxiety, and depression, between control and intervention groups for RCT’s and between baseline and after the intervention for QE studies.
Effects of Mindfulness-Based Interventions on the Psychological Well-being of FCGs of Cancer Patients: Randomized Controlled Trials.
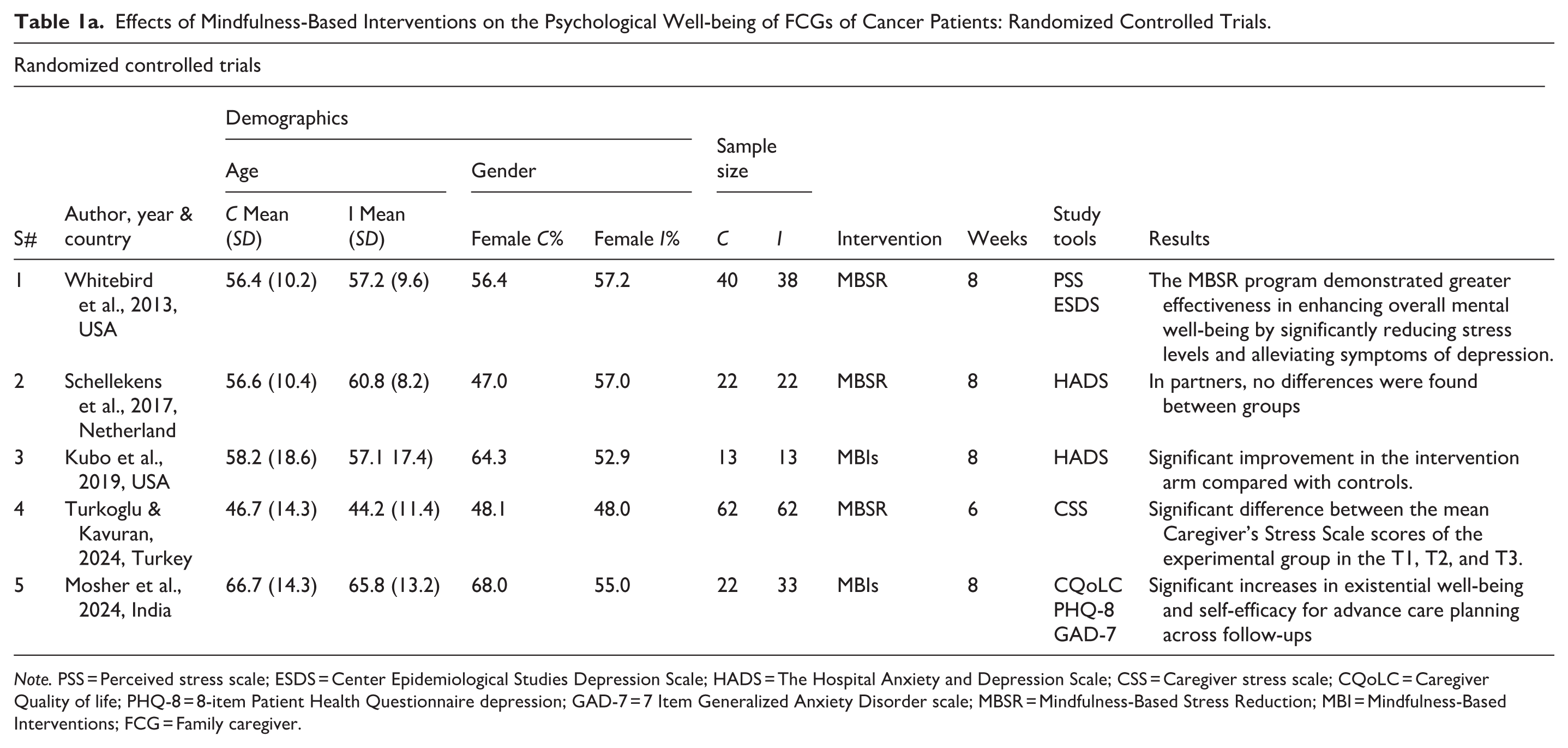
Note. PSS = Perceived stress scale; ESDS = Center Epidemiological Studies Depression Scale; HADS = The Hospital Anxiety and Depression Scale; CSS = Caregiver stress scale; CQoLC = Caregiver Quality of life; PHQ-8 = 8-item Patient Health Questionnaire depression; GAD-7 = 7 Item Generalized Anxiety Disorder scale; MBSR = Mindfulness-Based Stress Reduction; MBI = Mindfulness-Based Interventions; FCG = Family caregiver.
Outcome Measures: RCTs.
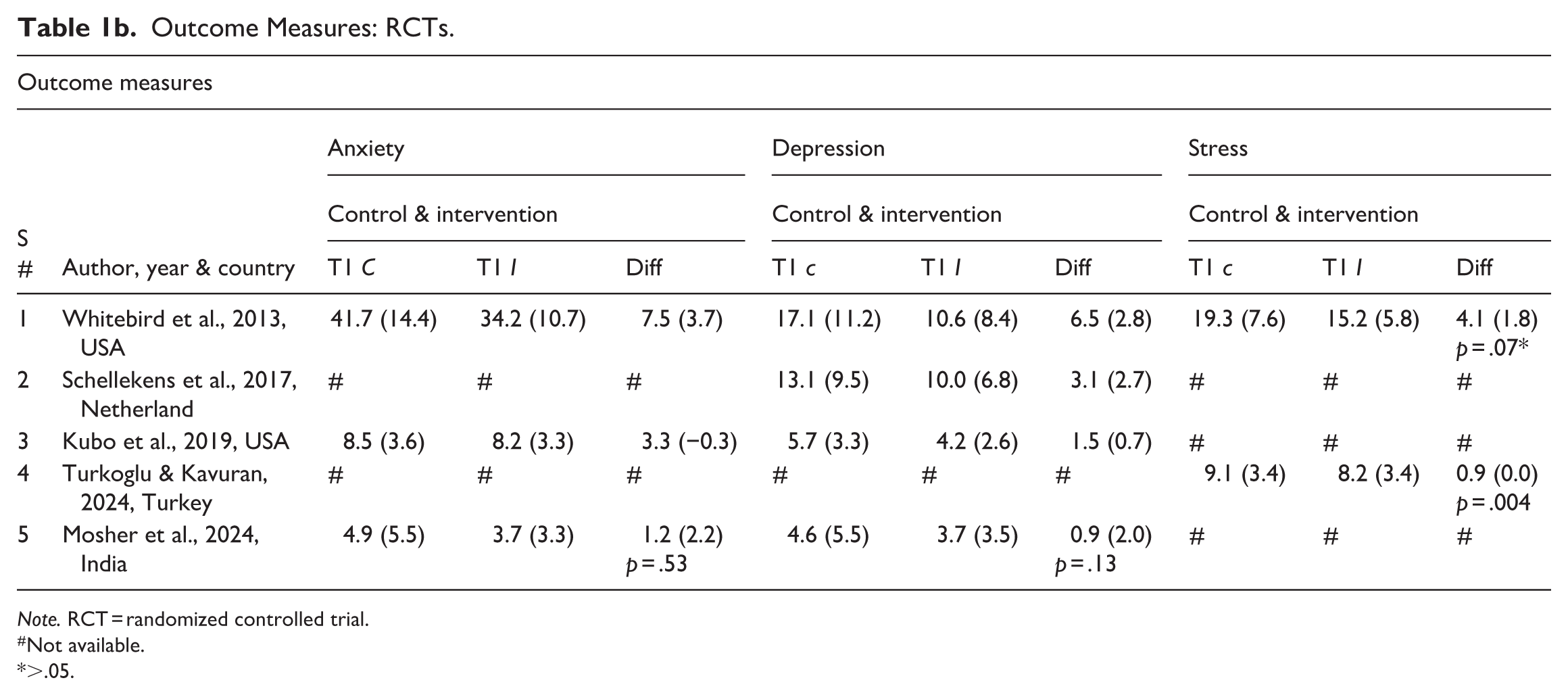
Note. RCT = randomized controlled trial.
Not available.
>.05.
Effects of Mindfulness-Based Interventions on the Psychological Well-being of FCGs of Cancer Patients: Quasi-Experimental Studies.
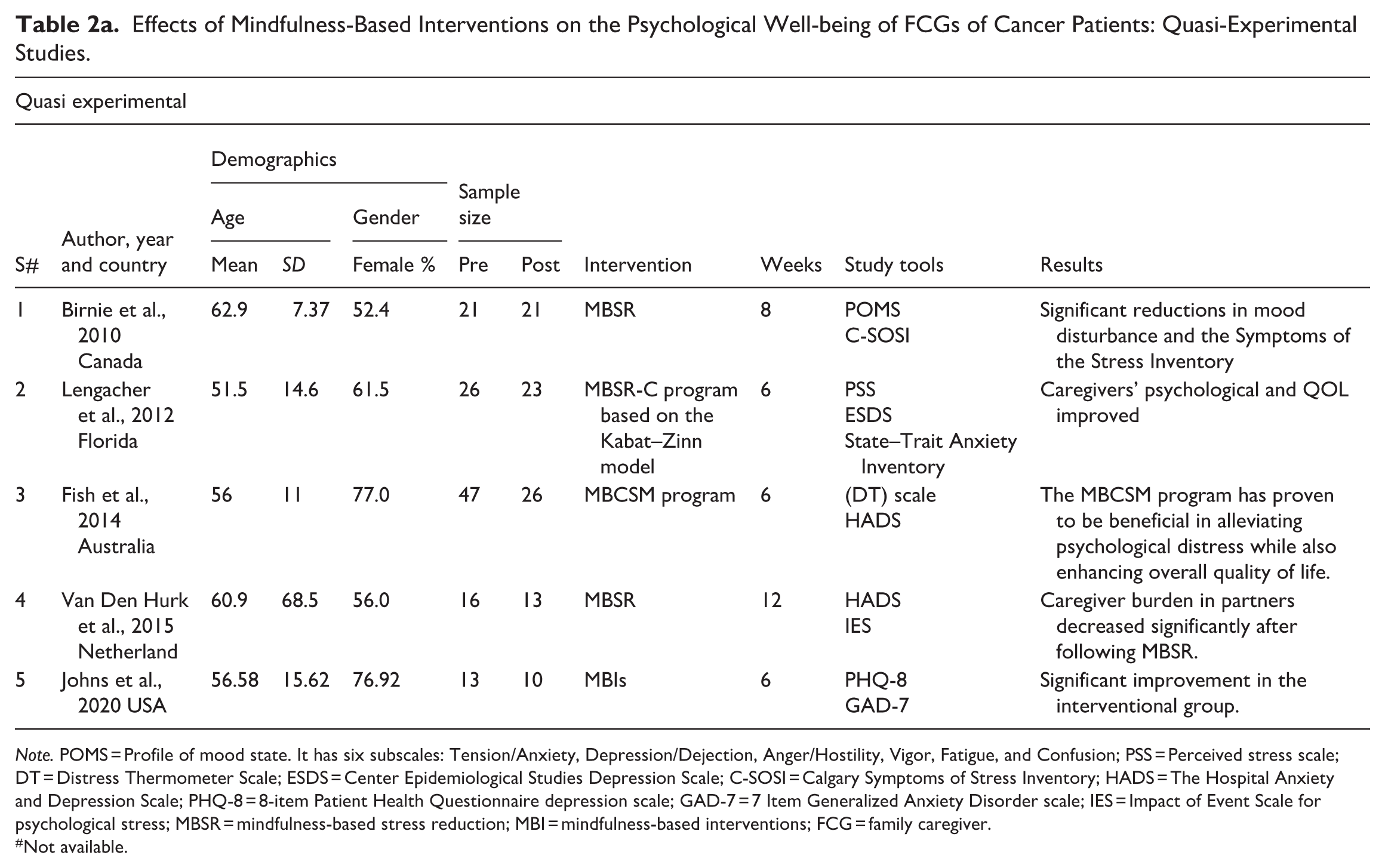
Note. POMS = Profile of mood state. It has six subscales: Tension/Anxiety, Depression/Dejection, Anger/Hostility, Vigor, Fatigue, and Confusion; PSS = Perceived stress scale; DT = Distress Thermometer Scale; ESDS = Center Epidemiological Studies Depression Scale; C-SOSI = Calgary Symptoms of Stress Inventory; HADS = The Hospital Anxiety and Depression Scale; PHQ-8 = 8-item Patient Health Questionnaire depression scale; GAD-7 = 7 Item Generalized Anxiety Disorder scale; IES = Impact of Event Scale for psychological stress; MBSR = mindfulness-based stress reduction; MBI = mindfulness-based interventions; FCG = family caregiver.
Not available.
Outcome Measures: Quasi-Experimental.
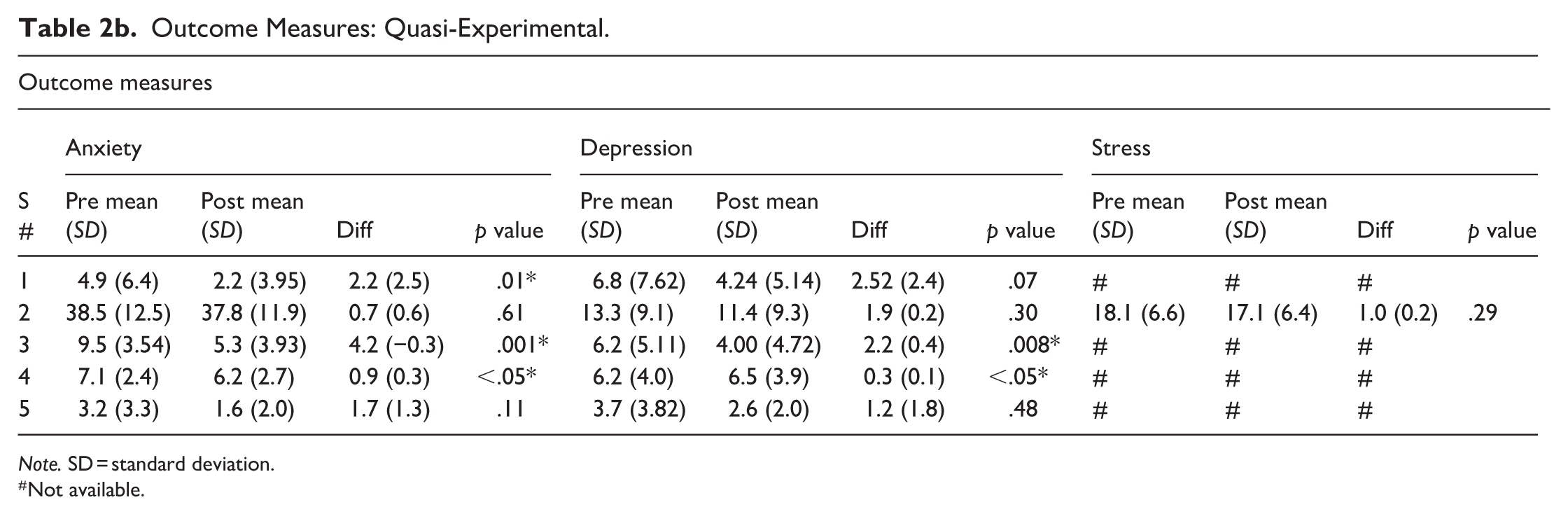
Note. SD = standard deviation.
Not available.
Risk of Bias Assessment
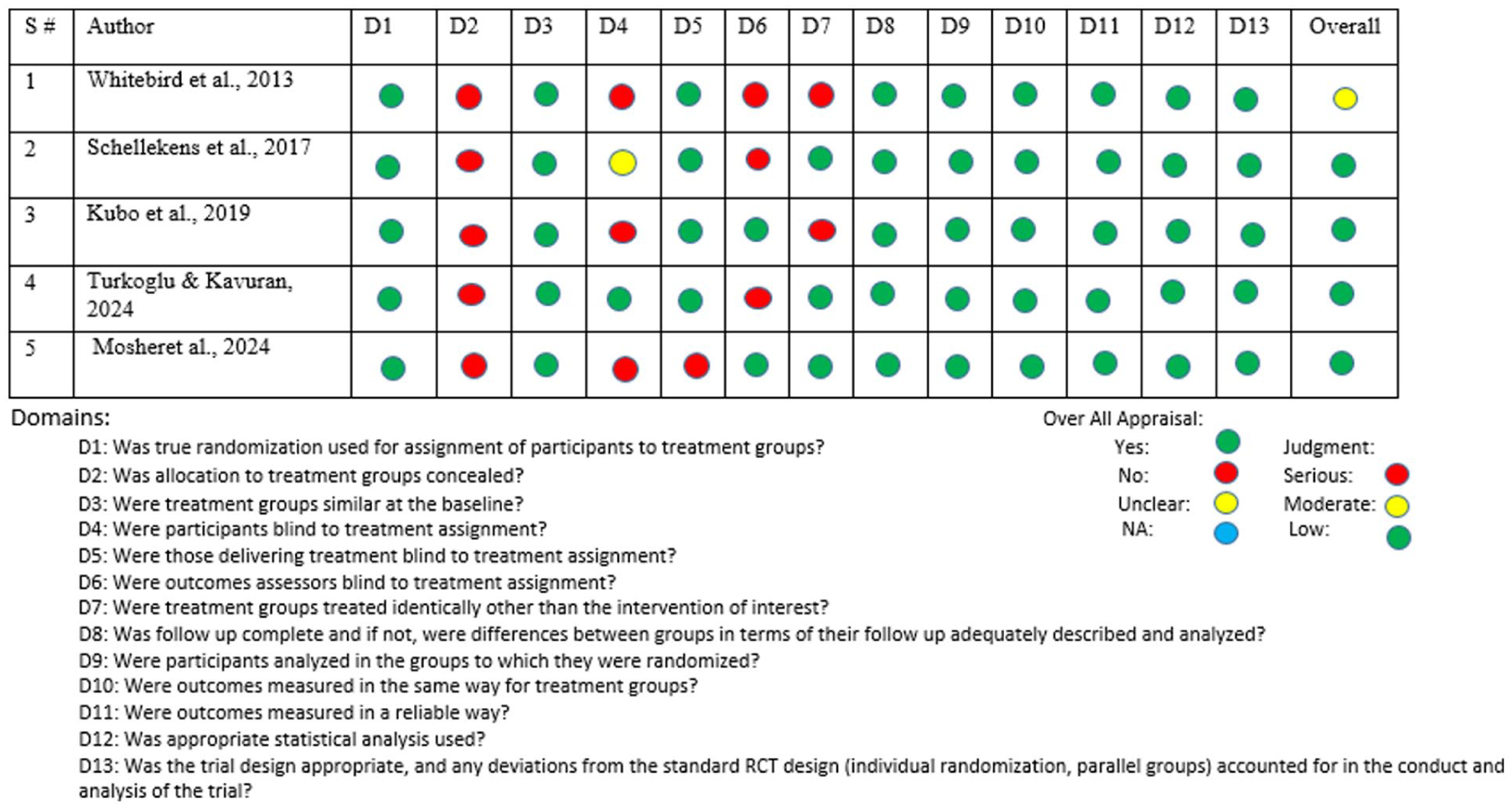
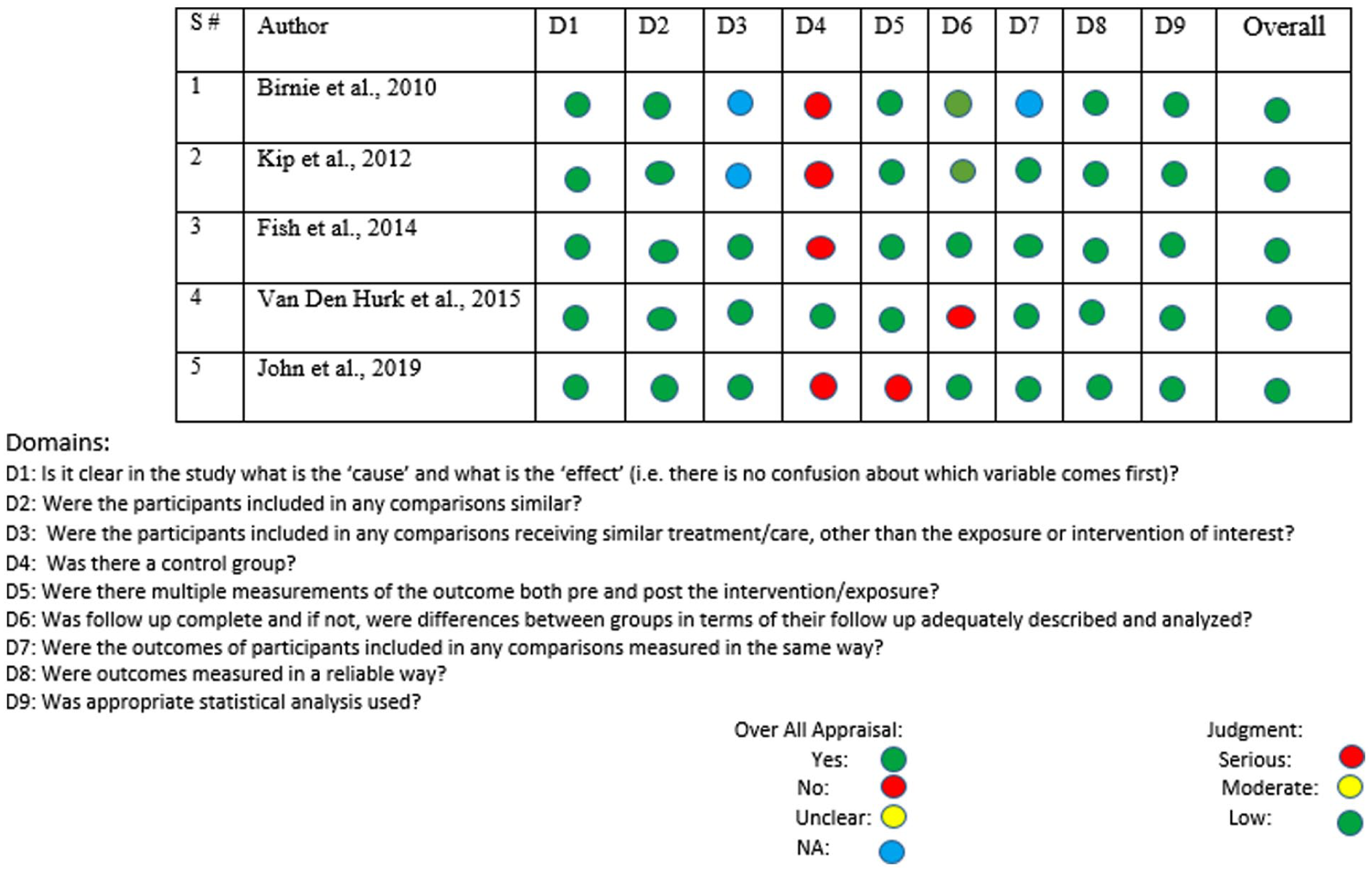
The Joanna Briggs Institute (JBI) Critical Appraisal Checklists (Barker et al., 2024) were used to assess the quality of the study. JBI Checklists for RCTs and QE studies (Barker et al., 2024) were applied to evaluate methodological quality, including validity, bias, and rigor. High-quality studies met most checklist items. Results are shown in Figures 2 and 3.
JBI risk of bias assessment (RCT).
JBI risk of bias assessment (quasi-experimental).
Results
The effectiveness of MBIs on the psychological well-being of cancer patients’ FCGs was evaluated in this systematic review. Ten studies in all were included, five were RCTs, and five were QE. The studies represent a variety of geographic regions, including North America (Birnie et al., 2010; Johns et al., 2020; Lengacher et al., 2012; Kubo et al., 2019; Whitebird et al., 2013), Europe (Schellenkens et al., 2017; Türkoğlu & Kavuran, 2024; Van Den Hurk et al., 2015), Asia (Mosher et al., 2024), and Australia (Fish et al., 2014).
Participant Demographics
Most of the caregivers were women; percentages range from 16% (Van Den Hurk et al., 2015) to as high as 77% (Fish et al., 2014). Participants’ average age ranged from 44.23 years (Turkowicz & Kavuran, 2024) to 66.7 years (Mosher et al., 2024). The sample size consisted of small pilot studies with as few as 10 participants (Johns et al., 2020) to trials including up to 124 participants. There were 449 participants in total across all RCTs, with 228 assigned to intervention groups and 221 to control groups. In most of the studies, the gender of the caregivers and patients has been represented in percentages (Fish et al., 2014; Lengacher et al., 2012; Schellekens et al., 2017).
Interventions
MBSR was the most frequent intervention as it was tested in six of the studies (Birnie et al., 2010; Lengacher et al., 2012; Schellekens et al., 2017; Türkoğlu & Kavuran, 2024; Van Den Hurk et al., 2015; Whitebird et al., 2013) that utilized various types of MBIs. Other interventions comprised other MBIs, which did not have a fixed format (Johns et al., 2020; Kubo et al., 2019; Mosher et al., 2024).
The duration of the interventions in 9 out of the 10 studies ranged between 6 weeks (Fish et al., 2014; Johns et al., 2020; Lengacher et al., 2012; Mosher et al., 2024) and 8 weeks (Birnie et al., 2010; Kubo et al., 2019; Schellekens et al., 2017; Türkoğlu & Kavuran, 2024; Whitebird et al., 2013). The exceptions were 12-week programs (Van Den Hurk et al., 2015). Follow-up periods were reported as well, and only a few focused on long-term outcomes, which were defined as follow-ups greater than 6 months (Mosher et al., 2024).
Measurement Tools
Different validated tools were utilized to assess psychological outcomes. Depression was measured using the “The Hospital Anxiety and Depression Scale-HADS” (Fish et al., 2014; Schellekens et al., 2017), the Patient Health Questionnaire depression scale (PHQ-9; Johns et al., 2020; Mosher et al., 2024), and the Center Epidemiological Studies Depression Scale (Lengacher et al., 2012; Whitebird et al., 2013). The Generalized Anxiety Disorder scale (GAD-7; Johns et al., 2020; Mosher et al., 2024) and the State-Trait Anxiety Inventory (Lengacher et al., 2012; Whitebird et al., 2013) were commonly used measures of anxiety. Stress was assessed using the Perceived Stress Scale (PSS) (Lengacher et al., 2012; Whitebird et al., 2013), Caregiver Stress Scale (Türkoğlu & Kavuran, 2024), and Calgary Symptoms of Stress Inventory (C-SOSI; Birnie et al., 2010).
Study Outcomes
Most studies noted statistically significant reductions in stress, anxiety, and depression scores after the intervention. Anxiety ratings, for example, dropped dramatically from a mean of 4.90 (6.49) to 2.19 (3.95) in Birnie et al. (2010). In Türkoğlu and Kavuran (2024), caregivers likewise showed a notable drop in stress; mean scores dropped from 8.29 to 4.24 over several time points. The studies collectively reported improvements in anxiety, depression, and stress levels among FCGs following participation in MBIs, though the magnitude and statistical significance of these effects varied.
Impact of MBIs on Anxiety
Eight of the 10 studies evaluated anxiety as their main result. For example, Birnie et al. (2020) found a notable drop in anxiety levels among the QE studies with a mean difference = 2.71. Similarly, Johns et al. (2020) found that following a 6-week mindfulness program, anxiety scores were reduced with a mean difference of 1.67. With mean differences of −7.5 (p < .05), Whitebird et al. (2013) showed in the RCTs a notable drop in anxiety in the intervention group relative to the control group. Kubo et al. (2019) discovered, however, only slight variations in anxiety scores (mean difference = 0.4), so suggesting variation in intervention efficacy.
Impact of MBIs on Depression
Nine studies claimed improvements in depression symptoms. Van Den Hurk et al. (2015) noted a mean decrease of 2.7 points on the HADS depression scale among QE designs; Lengacher et al. (2012) reported a smaller decline of 1.9 points. Mosher et al. (2024) reported among the RCTs a significant decrease in depression scores in the intervention group relative to controls (mean difference = −2.32, p < .05). By contrast, Schellekens et al. (2017) found no appreciable variations in depression scores between the intervention and control groups. Overall, MBIs that incorporated structured mindfulness training, such as MBSR, appeared more effective at reducing depression symptoms, particularly in RCTs, suggesting that the delivery method and study design may influence outcomes.
Impact of MBIs on Stress
Six studies evaluated stress. Lengacher et al. (2012) reported a modest decrease in stress levels (mean difference = 1.0) in the QE studies; Fish et al. (2014) and Van Den Hurk et al. (2015) did not specifically document stress outcomes. Among RCTs, Türkoğlu and Kavuran (2024) showed statistically significant declines in caregiver stress over time in the experimental group relative to controls (p = .001). With a mean difference of −11.1, p < .05, Whitebird et al. (2013) also noted a notably lower perceived stress in the MBSR group relative to normal treatment.
Meta-Analysis
A meta-analysis was conducted using RevMan software Version 5.4. A random-effects model was used to account for potential heterogeneity. We calculated standardized mean differences (SMD) for continuous outcomes (stress, anxiety, depression) with 95% confidence intervals (CI). Heterogeneity was assessed using Cochran’s Q test and I² statistics. Out of the five RCTs included in the review, only three were included in the meta-analysis. The remaining two RCTs were excluded because they did not report anxiety as an outcome measure, which was essential for inclusion in the quantitative synthesis. This criterion ensured consistency in outcome measurement across studies included in the meta-analysis.
Anxiety
The meta-analysis included three studies (Kubo et al., 2019; Mosher et al., 2024; Whitebird et al., 2013) that evaluated the effects of MBIs on anxiety among FCGs of cancer patients. The pooled SMD using a random-effects model was −0.39 (95% CI [−0.71, −0.07]), p = .02; the wide CIs indicate limited precision. The funnel plot did not show significant asymmetry, indicating a low likelihood of publication bias. However, given the small number of studies, the potential for bias cannot be ruled out completely. These findings suggest that MBIs can effectively reduce anxiety in FCGs of cancer patients. Moreover, the reliability of this conclusion is constrained by the limited number of studies included in the analysis. When the sample size is small, statistical tests for detecting publication bias become less reliable, making it difficult to draw definitive conclusions. Therefore, while the findings indicate that MBIs effectively reduce anxiety in FCGs of cancer patients, the possibility of unpublished studies with negative or non-significant results cannot be entirely ruled out. Figure 4(a) and (b) shows the results for anxiety.
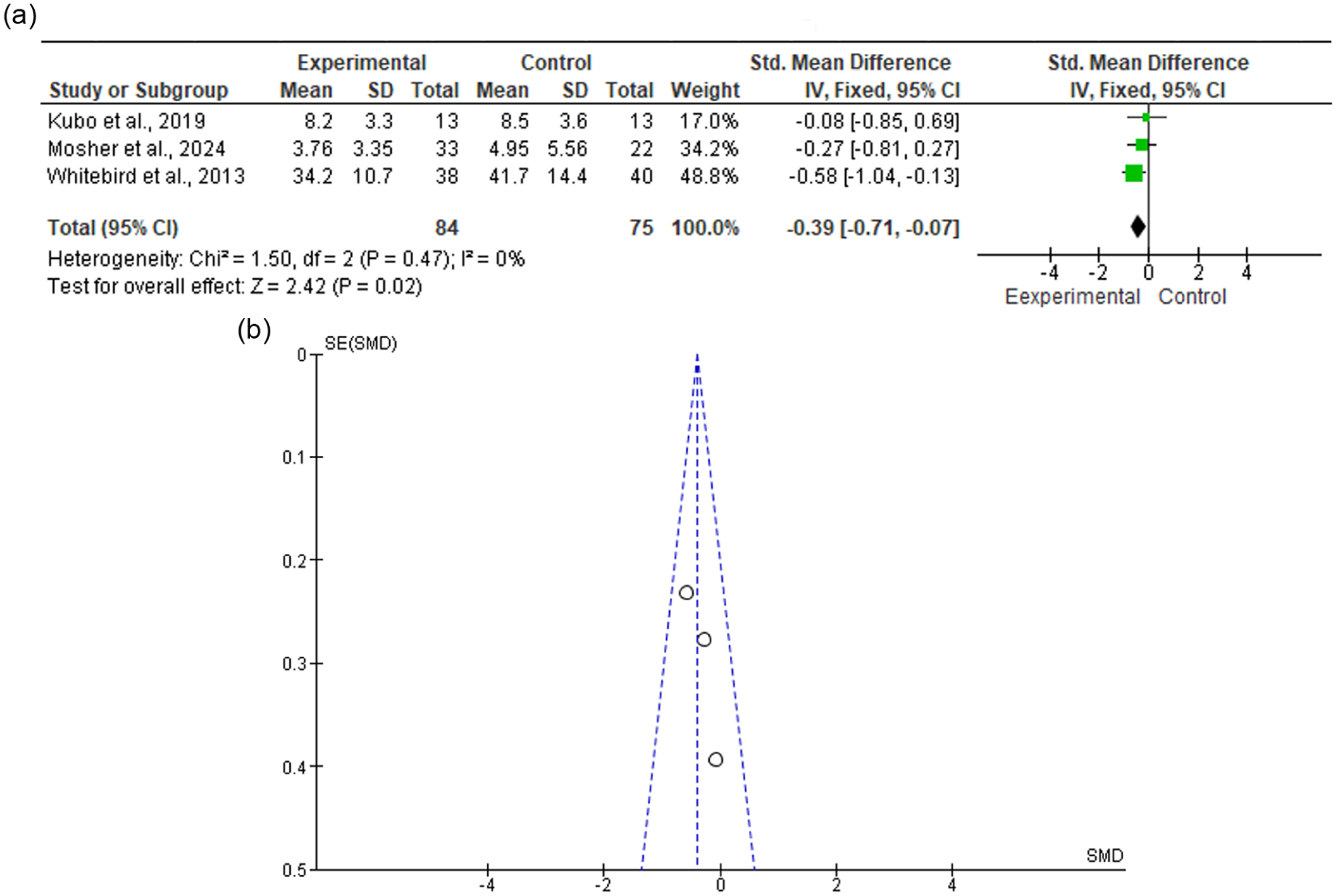
(a) Forest plot anxiety (b) Funnel plot anxiety.
Depression
The meta-analysis included four studies (Kubo et al., 2019; Mosher et al., 2024; Schellenkens et al., 2017; Whitebird et al., 2013) assessing the impact of MBSR on depression in FCGs of cancer patients. The forest plot results indicate a statistically significant pooled SMD of −0.44 (95% CI [−0.72, −0.16]), favoring the experimental group. The overall effect size (Z = 3.08, p = .00) suggests a significant reduction in depression levels following MBSR interventions. Heterogeneity was low (I² = 0%, p = .64), indicating consistency among the included studies. However, given the small number of studies, the possibility of selective reporting cannot be entirely excluded. Figure 5(a) and (b) shows funnel plot and forest plot for depression.
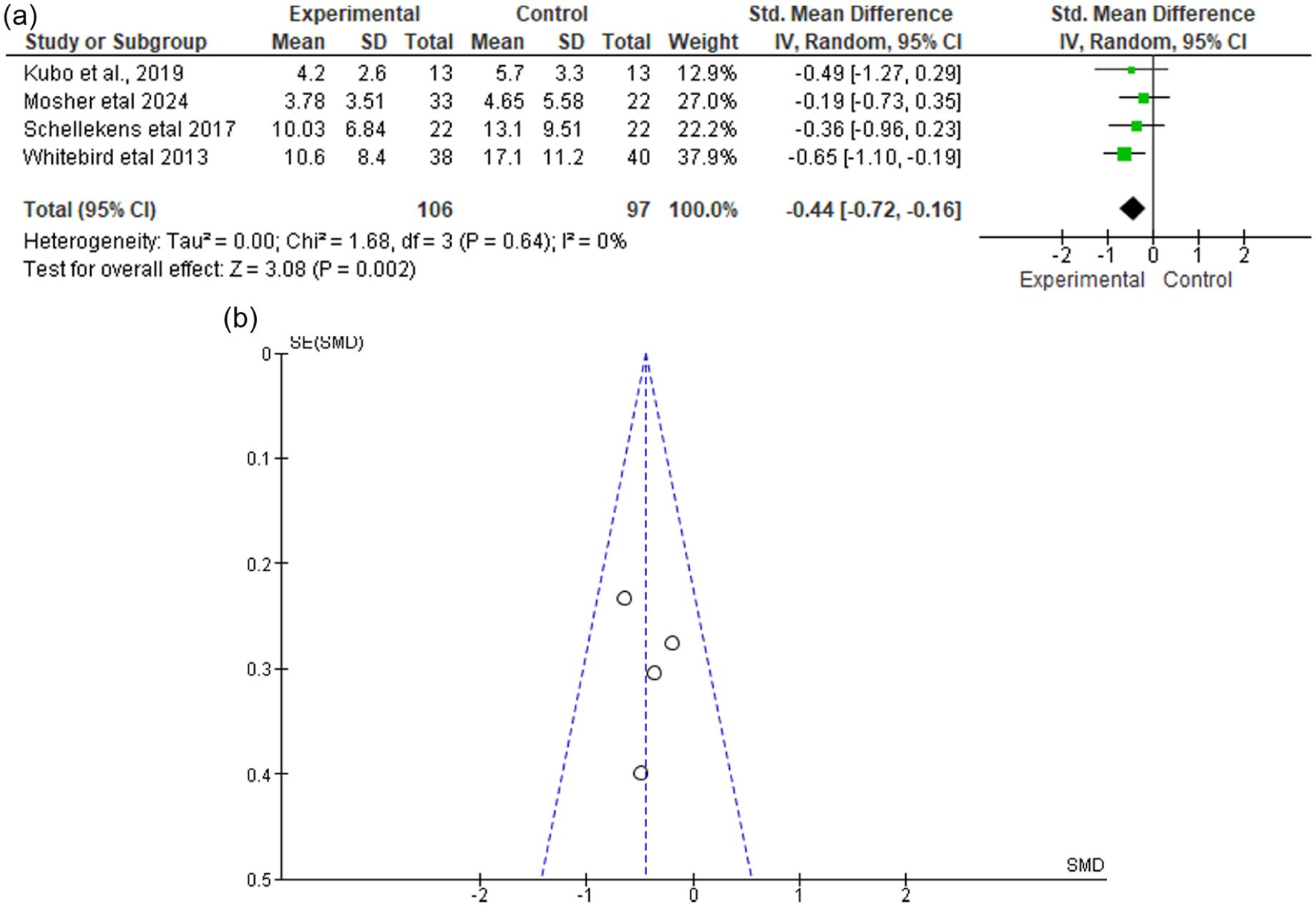
(a) Depression forest plot. (b) Depression funnel plot.
Stress
Two studies (Türkoğlu & Kavuran, 2024; Whitebird et al., 2013) were analyzed for the effect of MBSR on stress. The pooled mean difference was −2.20 (95% CI [−5.30, 0.90]), showing a non-significant effect (Z = 1.39, p = .16). The heterogeneity was moderate to high (I² = 73%, p = .05), indicating variability in the results across studies. The funnel plot for stress exhibits asymmetry, indicating a potential publication bias. This suggests that smaller studies with non-significant results may be underreported or unpublished. In addition, the moderate-to-high heterogeneity (I² = 73%) highlights variability in study designs, sample sizes, and intervention protocols, which may contribute to inconsistencies in the findings. These results are constrained by the small number of studies, which limits the statistical power to draw definitive conclusions regarding the interventions’ impact on stress. Figure 6(a) and (b) illustrates the results for stress.
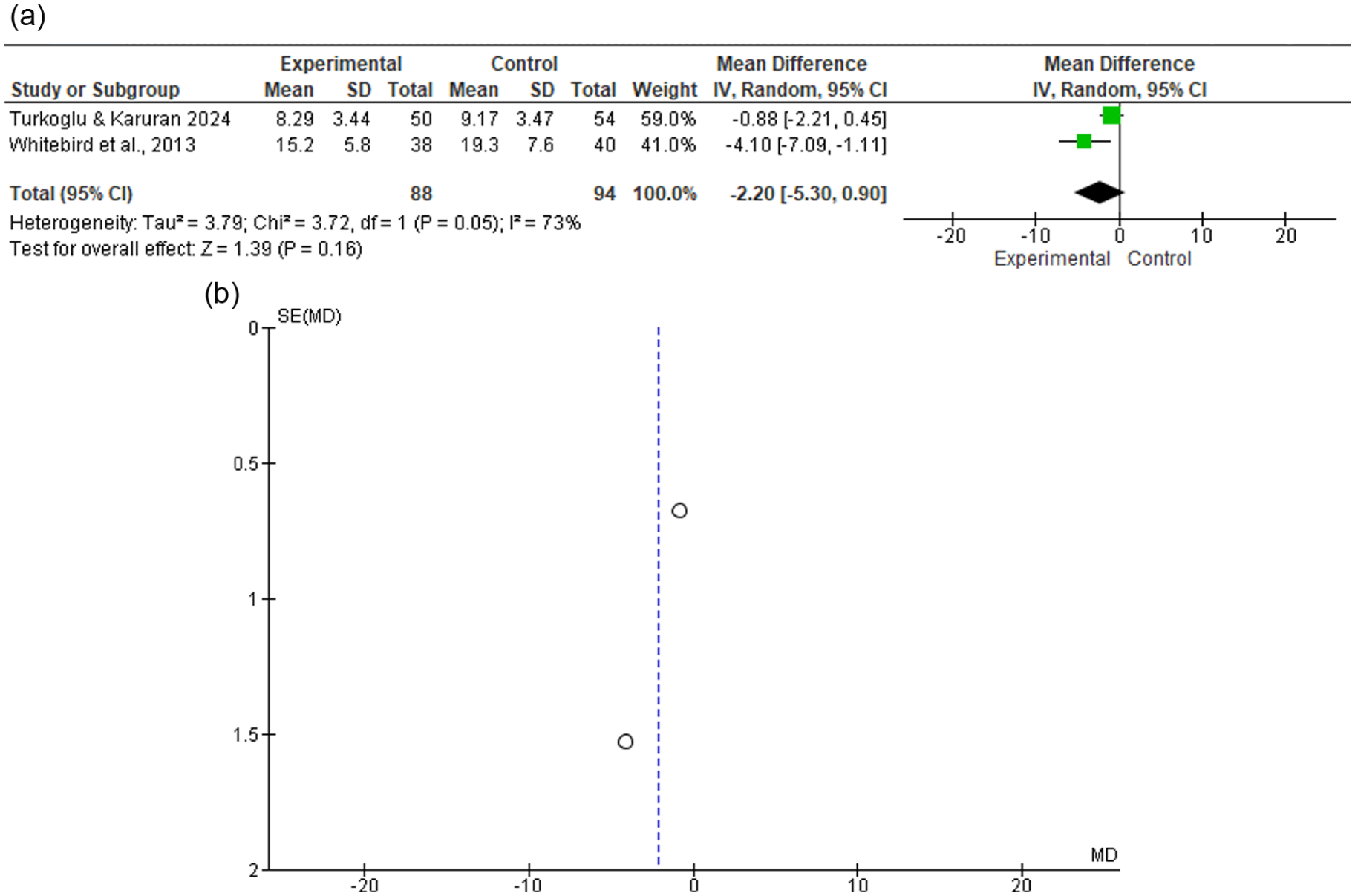
(a) Stress forest plot (b) Stress funnel plot.
Discussion
This systematic review and meta-analysis aimed to evaluate the effects of MBIs on the psychological well-being (anxiety, depression, stress) of FCGs of cancer patients. While these findings suggest a potential for MBIs to reduce anxiety, the limited number of studies and wide confidence intervals necessitate a cautious interpretation regarding their overall clinical precision.
The meta-analysis revealed that MBIs led to a small to moderate but statistically significant reduction in anxiety among FCGs. Heterogeneity analysis showed χ² = 1.50, df = 2 (p = .47), I² = 0%, suggesting low heterogeneity, indicating that the effect sizes across studies were consistent. These results align with prior research, such as Whitebird et al. (2013), who reported a significant decline in anxiety following an 8-week MBSR program. Similar findings were observed by Birnie et al. (2010) and Kenne Saremalm et al. (2017), who support the notion that mindfulness training enhances emotional regulation by reducing rumination and improving present-moment awareness (Bamber & Morpeth, 2019; Strohmaier, 2020; Strohmaier et al., 2021).
For depression, the meta-analysis of four studies found a significant reduction in depressive symptoms following MBIs. The low heterogeneity (I² = 0%) indicates a consistent effect across studies, reinforcing the reliability of these results. Studies by Lengacher et al. (2012) and Van Den Hurk et al. (2015) support these findings, demonstrating that mindfulness fosters a compassionate attitude and emotional resilience in caregivers, thereby reducing depressive symptoms (Juster, 2022; Dutta et al., 2023). Furthermore, Fish et al. (2014) found that mindfulness programs, particularly mindfulness-based cancer stress management, improved quality of life, which is closely linked to reduced depression. The funnel plot for depression suggests minimal publication bias, further validating these results. Future research with a larger sample of studies and rigorous study protocols can help confirm the robustness of these findings and reduce the risk of publication bias.
By contrast, the meta-analysis for stress, based on two studies, yielded non-significant results with moderate-to-high heterogeneity (I² = 73%). This variability is likely driven by differences in intervention protocols, such as variations between the standard 8-week MBSR program and shorter 6-week formats. Furthermore, the use of diverse measurement tools, including the PSS, Caregiver Stress Scale, and the C-SOSI, contributes to the inconsistency in reported effect sizes across the included trials. These methodological differences must be accounted for when evaluating the overall effectiveness of MBIs. Furthermore, integrating the risk-of-bias assessment reveals that the reliance on self-reported scales (e.g., PHQ-9, HADS) may introduce social desirability bias. Small sample sizes in several included studies further limit the overall strength and generalizability of these findings.
While some individual studies, such as those by Kubo et al. (2019) and Türkoğlu and Kavuran (2024), reported significant stress reductions, the overall inconsistency suggests that methodological differences may have influenced the outcomes. The funnel plot for stress exhibited asymmetry, indicating publication bias. Theories suggest that mindfulness practices enhance stress tolerance by promoting relaxation and emotional regulation (Iani et al., 2019; Masih et al., 2020; Stjernswärd & Hansson, 2020), yet further research with larger sample sizes and standardized stress outcome measures is needed to evaluate these effects.
Overall, the findings support MBIs’ role in improving FCGs’ psychological well-being, specifically reducing anxiety and depression. Integrating MBIs into structured interventions can provide mental health benefits. Future research should focus on culturally tailored interventions, standardized protocols, and long-term effects.
Limitations and Strengths
Limitations include variability in intervention protocols, small sample sizes, and a lack of culturally tailored programs, particularly in low-resource settings like Pakistan. In addition, limited data on long-term effects and potential biases due to self-reported outcomes remain a concern. Moreover, there are constraints inherent in the review process. These include potential for language bias, as the review was restricted to English-language publications, and the possibility of missing relevant studies due to the focus on specific databases. A significant limitation of this review is the geographical imbalance; although the study was prompted by the needs of caregivers in Pakistan, the available literature is primarily centered on high-income Western populations, which may not account for the unique cultural and resource-based challenges of the South Asian context. While efforts were made to assess publication bias, it remains a potential concern. Furthermore, the process of extracting data, though conducted by multiple reviewers, involves a degree of subjectivity that may have introduced inconsistencies.
Although there are some limitations, this systematic review also possesses multiple strengths that contribute to its overall validity and significance. It follows a rigorous PRISMA-based methodology, ensuring transparency and reliability in the review process. The inclusion of a comprehensive analysis of diverse MBIs highlights their consistent positive impact on reducing anxiety and depression among FCGs of cancer patients. The robust selection process, which included RCTs and quasi-experimental (QE) studies, was conducted with the assistance of an STMU librarian (A.U.) to enhance accuracy. Furthermore, two independent reviewers (E.F. and S.I.) ensured the validity and consistency of the study selection and data extraction process.
Implications
Future research should include diverse caregiver populations, larger samples, and more RCTs to assess the impact of MBIs and improve generalizability. It should also focus on standardized protocols and long-term impacts to enhance the effectiveness and applicability of MBIs in diverse caregiving settings. For practice, healthcare settings should integrate MBIs into routine caregiver support, train healthcare professionals in MBI delivery, and develop digital/remote mindfulness programs for wider accessibility.
Conclusion
This meta-analysis provides strong evidence that MBIs play a crucial role in enhancing the psychological well-being of FCGs of cancer patients. By significantly reducing symptoms of anxiety and depression, these interventions help caregivers better manage the emotional and psychological challenges associated with their caregiving responsibilities. However, the effect on stress remains inconclusive due to a small number of studies, high heterogeneity, and potential publication bias. Future research should focus on standardized protocols and long-term impacts to enhance the effectiveness and applicability of MBIs in diverse caregiving settings.
Footnotes
Acknowledgements
I am thankful to all those who contributed to this systematic review and meta-analysis. I am especially appreciative to Somia Saghir (S.S.) for assisting in the database search, whose diligent efforts as an independent reviewer ensured the validity and consistency of the study selection and data extraction process. I also extend my appreciation to Aman Ullah (A.U.) for their valuable support in refining the database searches. Additionally, I am thankful to Dr. Kainat Asmat (K.A.) for her guidance and assistance in using RevMan software. Their collective contributions have greatly enhanced the quality and rigor of this review.
Ethical Considerations
This systematic review and meta-analysis synthesized and analyzed data from previously published studies. Ethical approval was not required for this synthesis. This study was registered in PROSPERO (CRD42024599005).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data analyzed in this systematic review and meta-analysis consisted of previously published studies. These source studies are individually cited within the reference list. The extracted data and analyses presented in this review are contained within the manuscript.