
Abstract
This descriptive and correlational study investigated the relationship between exposure to obstetric violence and mother–infant attachment and postpartum depression (PPD) among women who had vaginal births. The sample comprised 292 mothers with infants aged 3 to 12 months who attended the outpatient clinics of a hospital in Konya between March and August 2024. Data were collected using a personal information form, an obstetric violence assessment form, the Maternal Attachment Scale, and the Edinburgh Postpartum Depression Scale. Independent samples t-tests and multiple linear regression analyses were conducted. The mean age of the participants was 29.50 ± 6.02 years. Emotional obstetric violence was reported by 32.9% of mothers, followed by verbal violence (19.5%), physical violence (7.9%), and sexual violence (6.2%). Mothers who reported exposure to any form of obstetric violence had significantly lower maternal attachment scores and significantly higher PPD scores (p < .001). Regression analyses indicated that verbal and sexual obstetric violence were significant predictors of both maternal attachment and PPD. Greater exposure to verbal and sexual violence was associated with weaker maternal attachment and higher levels of postpartum depressive symptoms. These findings highlight the detrimental impact of obstetric violence on maternal psychological well-being and early mother–infant attachment. Policies and clinical practices aimed at preventing obstetric violence and promoting respectful maternity care are essential to safeguard the health and well-being of both mothers and their infants.
Introduction
Obstetric violence (OV), although lacking a universally accepted definition, generally refers to gender-based, disrespectful, and inhumane treatment of women by healthcare professionals during childbirth (Avcı & Kaydırak, 2023; Paiz et al., 2021). It encompasses a range of practices, including physical abuse (e.g. fundal pressure and repeated vaginal examinations), verbal humiliation, non-consensual medical procedures, breaches of confidentiality, routine and unnecessary obstetric interventions, lack of informed consent, and delayed mother–infant contact after birth (Khalil et al., 2022; Martinez-Galiano et al., 2021).
Women frequently describe exclusion from decision-making processes, inadequate pain management, dehumanizing attitudes, and coercive behaviors by healthcare professionals as central components of traumatic birth experiences (Ferrão et al., 2022). These experiences directly contradict the fundamental right of all women to receive safe, effective, equitable, timely, and patient-centered maternal healthcare services (Afulani et al., 2019; World Health Organization [WHO], 2014).
Global evidence suggests that the prevalence of obstetric violence during childbirth ranges from 67% to 99% (Azhar et al., 2018; Baranowska et al., 2019). Studies conducted in Türkiye indicate that nearly three-quarters of women report experiencing some form of obstetric violence during childbirth (Aşci & Bal, 2023; Avcı & Kaydırak, 2023). For example, a study in India found that 92% of women were not offered a choice of birthing position and reported frequent exposure to physical violence (Sharma et al., 2019). In Spain, a large-scale study involving 17,541 women identified midwives, obstetricians, and other maternity care providers as the professionals most frequently reported in relation to obstetric violence (Mena-Tudela et al., 2021). Exposure to OV has been associated with reduced healthcare utilization, diminished quality of life, and long-term psychological consequences (Ishola et al., 2017; Silveira et al., 2019).
Traumatic birth experiences linked to obstetric violence may have profound implications for maternal psychological well-being and early mother–infant attachment (Ferrão et al., 2022; Taghizadeh et al., 2021). Maternal attachment refers to the enduring emotional bond that begins during pregnancy and develops through affectionate and responsive interactions between mother and infant (Ponti et al., 2020; Voges et al., 2019). This bond plays a critical role in preparing women for motherhood and supports the infant’s emotional and social development. According to Bowlby’s (1982) attachment theory, early interactions between the infant and the primary caregiver establish the foundation for future relational patterns. Disruptions in early attachment may increase the risk of insecure attachment styles and subsequent developmental challenges (Bowlby, 1982; Kavlak & Şirin, 2009). Despite these theoretical considerations, the potential impact of obstetric violence on maternal attachment remains insufficiently explored.
Exposure to traumatic birth experiences has also been identified as a significant risk factor for postpartum depression (PPD) (Silveira et al., 2019; Souza et al., 2017). The prevalence of PPD varies widely, ranging from 5% to 51%, with symptoms most commonly emerging within the first months after childbirth (Paiz et al., 2021; Slomian et al., 2019; Wubetu et al., 2020). PPD not only affects maternal mental health but also impairs mother–infant attachment and negatively influences family functioning (Paiz et al., 2021; Ponti et al., 2020; Wubetu et al., 2020).
Although several studies have examined the association between obstetric violence and PPD (Martinez-Vázquez et al., 2022; Paiz et al., 2021), research investigating its relationship with maternal attachment remains limited (Taghizadeh et al., 2021). To date, no study has simultaneously evaluated exposure to obstetric violence, PPD, and maternal attachment within the same analytical framework. Moreover, although OV has gained increasing attention internationally, it remains a relatively recent and under-researched topic in Türkiye (Aşci & Bal, 2023; Avcı & Kaydırak, 2023). Further empirical evidence is therefore needed to better understand its prevalence and its psychological and relational consequences for women.
The present study aims to generate scientific evidence that supports women’s access to rights-based, respectful, and empowering maternity care. By examining the relationship between exposure to obstetric violence, PPD, and maternal attachment, this study seeks to contribute to the early identification of at-risk mothers, inform the development of supportive and rehabilitative care interventions, and strengthen patient advocacy within midwifery and maternity care practice. Ultimately, the findings aim to promote positive motherhood experiences and improve maternal well-being.
Research Questions
What is the prevalence of obstetric violence among mothers who have had vaginal births?
Is exposure to obstetric violence associated with maternal attachment levels among mothers who have had vaginal births?
Is exposure to obstetric violence associated with PPD levels among mothers who have had vaginal births?
Methods
Study Design
This study employed a descriptive and correlational design and was conducted in the pediatric outpatient department of a university hospital. The study population consisted of mothers with infants aged 3 to 12 months who attended the pediatric outpatient clinic of the hospital within the past year for routine examination, follow-up, or treatment services. Data collection was carried out between March and August 2024. The data were obtained through self-report questionnaires administered in a private room allocated specifically for the study. Privacy and confidentiality were strictly maintained throughout the data collection process, and no unauthorized entry or interruption was permitted during the interviews.
Participants
The sample size was calculated using G*Power version 3.1.9.4 (Heinrich Heine University, Düsseldorf, Germany). Based on a previous study conducted in Türkiye that reported an obstetric violence prevalence of 58.23% (Avcı & Kaydırak, 2023), the minimum required sample size was calculated to be 263 mothers to detect a comparable proportion with 90% statistical power and a 5% margin of error. During the data collection period, 302 mothers who met the inclusion criteria were approached. Of these, 292 agreed to participate and completed the data collection forms in full, yielding a response rate of 96.7%.
Inclusion and Exclusion Criteria
Inclusion criteria were as follows: being 18 years of age or older; ability to read, understand, and write in Turkish; having had a vaginal birth; being 3 to 12 months postpartum; having conceived spontaneously; absence of a high-risk pregnancy diagnosis; no visual or hearing impairment; no known psychiatric or chronic illness; and having an infant without congenital anomalies or postpartum health complications.
The postpartum period was defined as 3 to 12 months to ensure the assessment of more established maternal attachment patterns, as the Maternal Attachment Scale (MAS) is recommended for use after the first postpartum month. In addition, PPD may emerge within 4 to 6 weeks after childbirth and can persist for up to 1 year or longer, making this timeframe appropriate for evaluating both maternal attachment and postpartum depressive symptoms (Engindeniz et al., 1996; Kavlak & Şirin, 2009). A simple random sampling method was employed among eligible mothers attending the pediatric outpatient clinic during the study period.
Measures
Data were collected using self-report questionnaires, including the Personal Information Form, the Obstetric Violence Information Form, the Edinburgh Postpartum Depression Scale (EPDS), and the MAS.
Personal Information Form
The Personal Information Form was developed by the researchers based on a review of the relevant literature (Avcı & Kaydırak, 2023; Çankaya & Dikmen, 2023). The form consists of 19 items: 8 questions assessing participants’ sociodemographic characteristics (e.g. age, educational level, spouse’s educational level, marital status, employment status, and family type) and 11 questions related to obstetric characteristics (e.g. number of births, type of delivery, and pregnancy-related variables).
Obstetric Violence Information Form
The Obstetric Violence Information Form was developed by the researchers based on a review of the relevant literature (Aşci & Bal, 2023; Avcı & Kaydırak, 2023; Çankaya & Dikmen, 2023). The form includes 24 items organized into 5 domains: physical obstetric violence (10 items), emotional obstetric violence (3 items), verbal obstetric violence (5 items), sexual obstetric violence (2 items), and violation of privacy (4 items). Each domain contains items that assess specific behaviors corresponding to that type of violence. Mothers were asked to indicate “Yes” if they experienced the described situation during childbirth.
A respondent was considered exposed to obstetric violence if she answered “Yes” to at least one item in any domain. In addition, negative responses to certain rights-based care questions, such as experiencing physical contact without informed consent, being subjected to an angry or aggressive tone, or hearing threatening or negative verbal expressions during labor, were also classified as indicative of obstetric violence.
Edinburgh Postpartum Depression Scale
The EPDS was developed by Cox et al. (1987) and adapted into Turkish by Engindeniz et al. (1996). The original scale demonstrated good internal consistency, with a Cronbach’s alpha coefficient of .87. The EPDS is a 10-item self-report instrument rated on a four-point Likert scale, with each item scored from 0 to 3. Items 1, 2, and 4 are scored directly (0–3), whereas items 3, 5, 6, 7, 8, 9, and 10 are reverse-scored (3–0). Total scores range from 0 to 30, with higher scores indicating more severe depressive symptoms. The recommended cut-off score for the Turkish version is 12 (Engindeniz et al., 1996). In the present study, the Cronbach’s alpha coefficient for the EPDS was .85, indicating good internal consistency.
Maternal Attachment Scale
The MAS was developed by Müller (1994) to assess maternal attachment. The validity and reliability of the Turkish version were established by Kavlak and Şirin (2009). The MAS is a 26-item self-report scale rated on a four-point Likert scale ranging from “always” (4) to “never” (1). Total scores range from 26 to 104, with higher scores reflecting stronger maternal attachment. The scale does not include reverse-scored items or a specified cut-off value. Cronbach’s alpha coefficients for the Turkish version were reported as .77 for mothers of 1-month-old infants and .82 for mothers of 4-month-old infants (Kavlak & Şirin, 2009). In the present study, the Cronbach’s alpha coefficient was .97, indicating excellent internal consistency.
Data Analysis
Statistical analyses were performed using SPSS version 20.0 (IBM Corp., Armonk, NY, USA). The normality of the data distribution was assessed using skewness and kurtosis values. As these values ranged between −1.5 and +1.5, the data were considered normally distributed, and parametric tests were applied (Tabachnick & Fidell, 2013). Descriptive statistics, including frequencies, percentages, means, standard deviations, and minimum and maximum values, were used to summarize the data. Independent samples t-tests were conducted to examine differences between groups.
Variables found to be significant in univariate analyses were subsequently entered into multiple linear regression models using the enter method. MAS and EPDS scores were treated as continuous dependent variables. All assumptions for multiple linear regression were satisfied. No multicollinearity was detected among the independent variables (variance inflation factor < 4). No autocorrelation was observed (Durbin–Watson = 1.754 for MAS; 1.718 for EPDS). Furthermore, no influential outliers were identified (standardized residuals within ±3.29; Cook’s distance < 1) (Hair et al., 2010). Independent variables included exposure to physical, verbal, emotional, and sexual obstetric violence, each coded as a binary variable (1 = yes, 0 = no). Statistical significance was set at p < .05.
Ethical Considerations
Ethical approval for this study was obtained from the Ethics Committee of Selçuk University, Noninvasive Clinical Research Ethics Committee (Approval No: 2023/1369) prior to data collection. The study was conducted in accordance with the principles of the Declaration of Helsinki (1964) and its subsequent amendments. Institutional permission (Date and Number: 02.02.2024-E.691638) was obtained from the relevant hospital administration. Written informed consent was obtained from all participants prior to enrollment in the study.
Results
The mean mother’s age (years) was 29.50 ± 6.02, and the mean number of births was 1.90 ± 1.17 (Table 1). Regarding the mode of delivery and birth attendant, 54.1% of the mothers had a vaginal delivery attended by a midwife, and 89.4% reported receiving midwife support during birth. In terms of obstetric violence types, emotional obstetric violence was the most frequently reported type (32.9%) (Table 2). The mean MAS score was 101 ± 13.45 (range: 26–104), and the mean EPDS score was 9 ± 5.49 (range: 0–30). Based on the EPDS cut-off score (≥13), 21.9% of the mothers were identified as having PPD (EPDS ≥ 13) (Table 2).
Sociodemographic and Obstetric Characteristics of Mothers (N = 292).
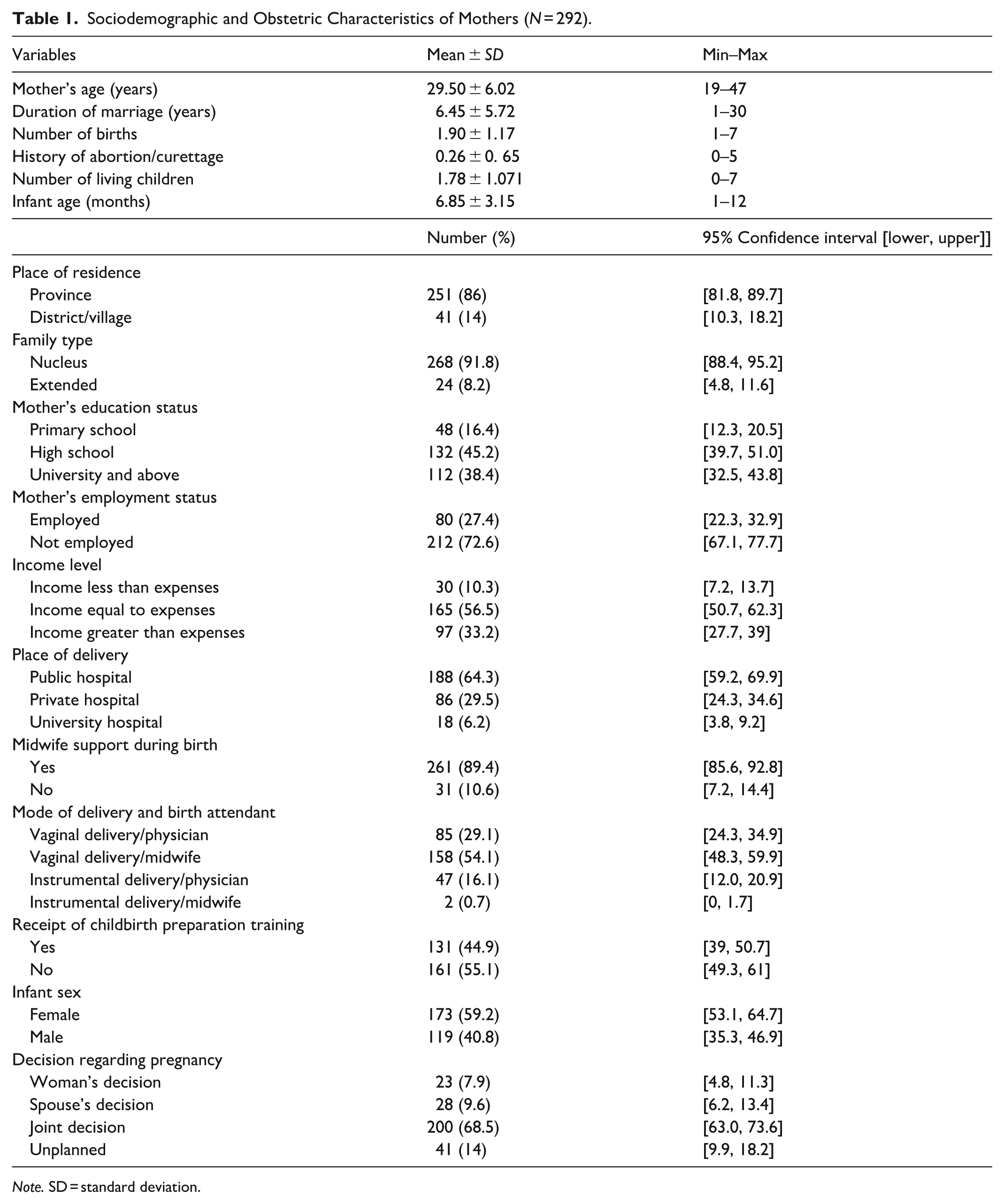
Note. SD = standard deviation.
Distribution of Obstetric Violence Types and Mean MAS and EPDS Scores among Mothers (N = 292).
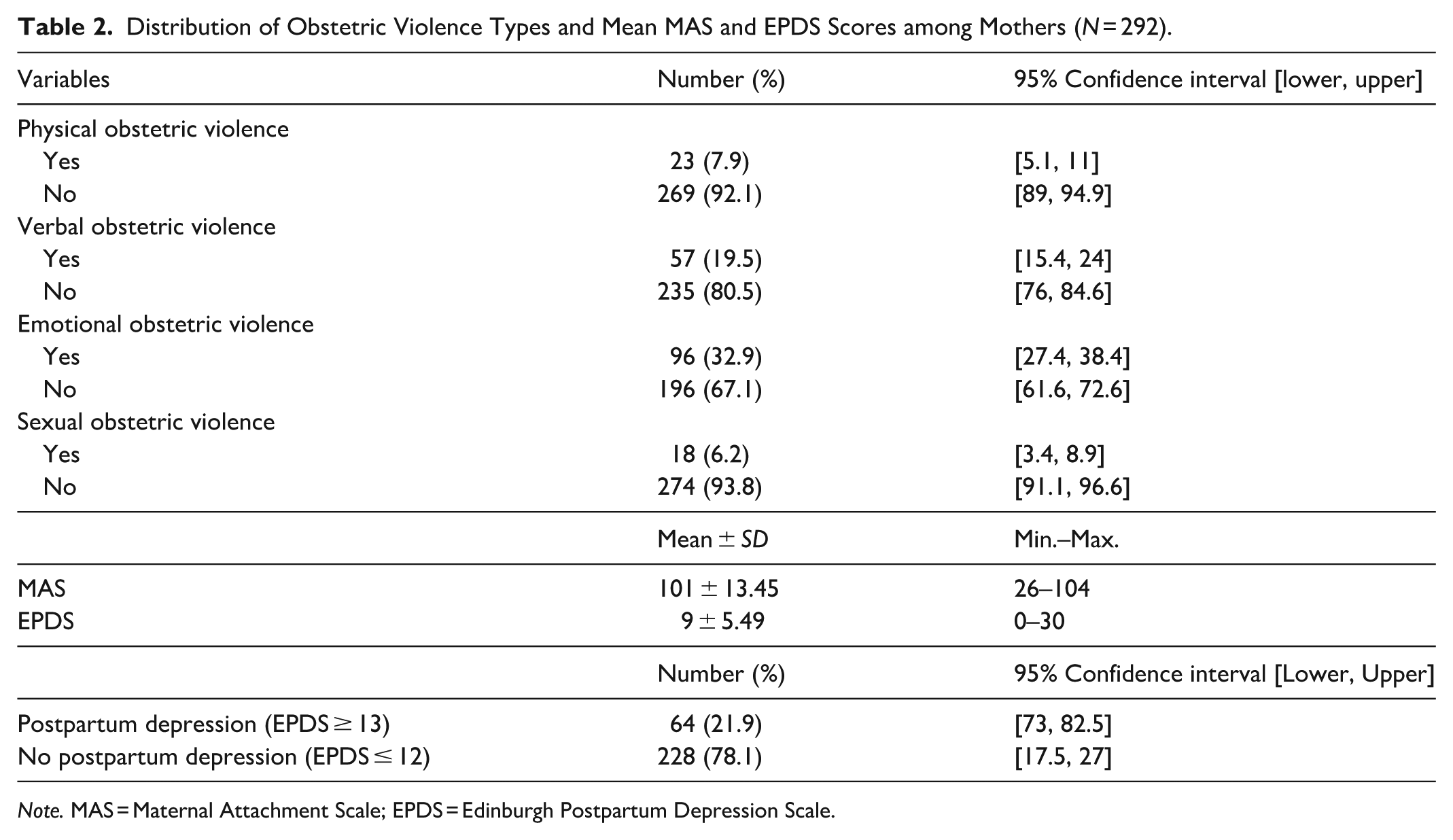
Note. MAS = Maternal Attachment Scale; EPDS = Edinburgh Postpartum Depression Scale.
Regarding childbirth care experiences, 39.4% of mothers reported exposure to vaginal examinations by multiple healthcare professionals during labor. The use of threatening or negative verbal expressions during labor was reported by 13% of mothers. The absence of a companion of choice during labor was reported by 83.2%, and 25.3% indicated that their privacy was not respected during labor. Physical obstetric violence during labor was most frequently attributed to nurses/midwives (3.8%), whereas verbal and sexual obstetric violence during labor were more commonly attributed to physicians (7.2% and 4.1%, respectively) (Table 3).
Distribution of Respectful Maternity Care during Childbirth (N = 292).
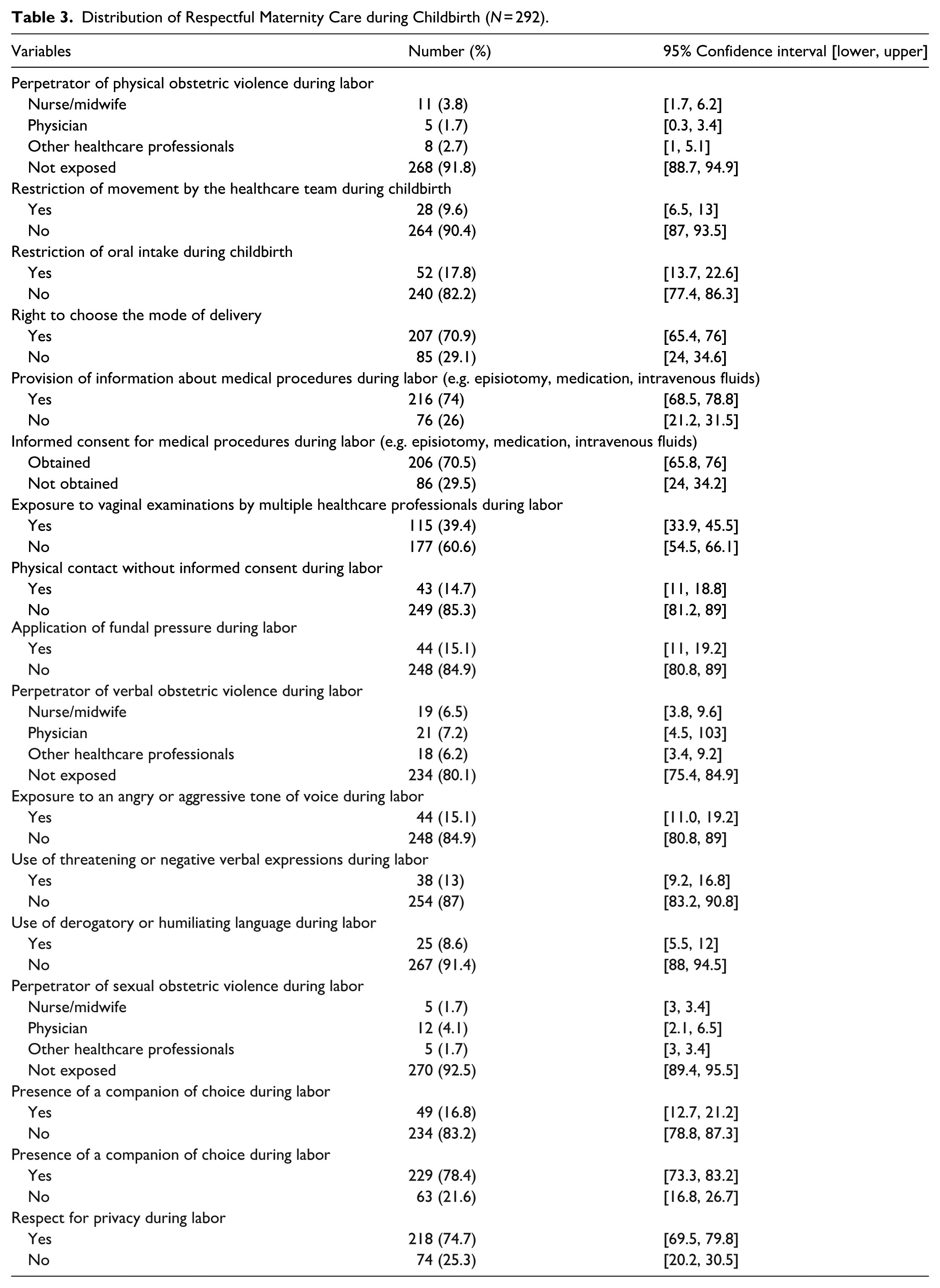
Table 4 presents the comparison of MAS and EPDS scores according to exposure to different types of obstetric violence. Mothers who were exposed to physical violence had significantly lower mean MAS scores (88.52 ± 19.58) compared to those who were not exposed (96.71 ± 12.63) (p = .005). Similarly, exposure to verbal, emotional, and sexual violence was associated with significantly lower maternal attachment scores (p < .05 for all comparisons). The lowest MAS scores were observed among mothers exposed to sexual violence (75.33 ± 24.82). By contrast, EPDS scores were significantly higher among mothers exposed to all types of obstetric violence. For example, mothers exposed to sexual violence had a mean EPDS score of 16.61 ± 5.87, compared to 8.10 ± 5.06 among those not exposed (p < .001). Overall, exposure to obstetric violence was consistently associated with weaker maternal attachment and higher levels of postpartum depressive symptoms.
Association between Exposure to Obstetric Violence, Maternal Attachment, and Postpartum Depression.
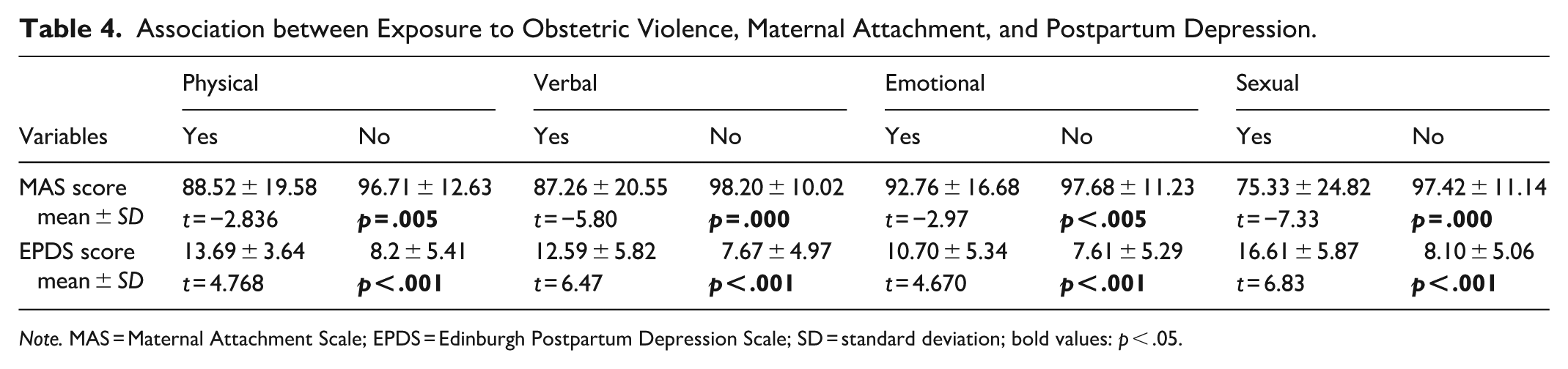
Note. MAS = Maternal Attachment Scale; EPDS = Edinburgh Postpartum Depression Scale; SD = standard deviation; bold values: p < .05.
Table 5 summarizes the results of the multiple linear regression analysis examining the independent effects of different types of obstetric violence on maternal attachment. The overall model was statistically significant (F = 18.540, p < .001), explaining 20.5% of the variance in maternal attachment scores (R² = 0.205; Adjusted R² = 0.194). Verbal violence (B = −7.925, p < .001) and sexual violence (B = −20.708, p < .001) emerged as significant negative predictors of maternal attachment, indicating that exposure to these forms of violence was associated with lower attachment scores. By contrast, physical (p = .079) and emotional violence (p = .866) were not significant predictors in the adjusted model. Collinearity statistics suggested no multicollinearity problems, and the Durbin–Watson value (1.754) indicated acceptable independence of residuals. These findings suggest that verbal and, particularly, sexual obstetric violence have a substantial and independent adverse impact on maternal attachment.
Association of Obstetric Violence with Maternal Attachment and Postpartum Depression: A Multiple Linear Regression Analysis.
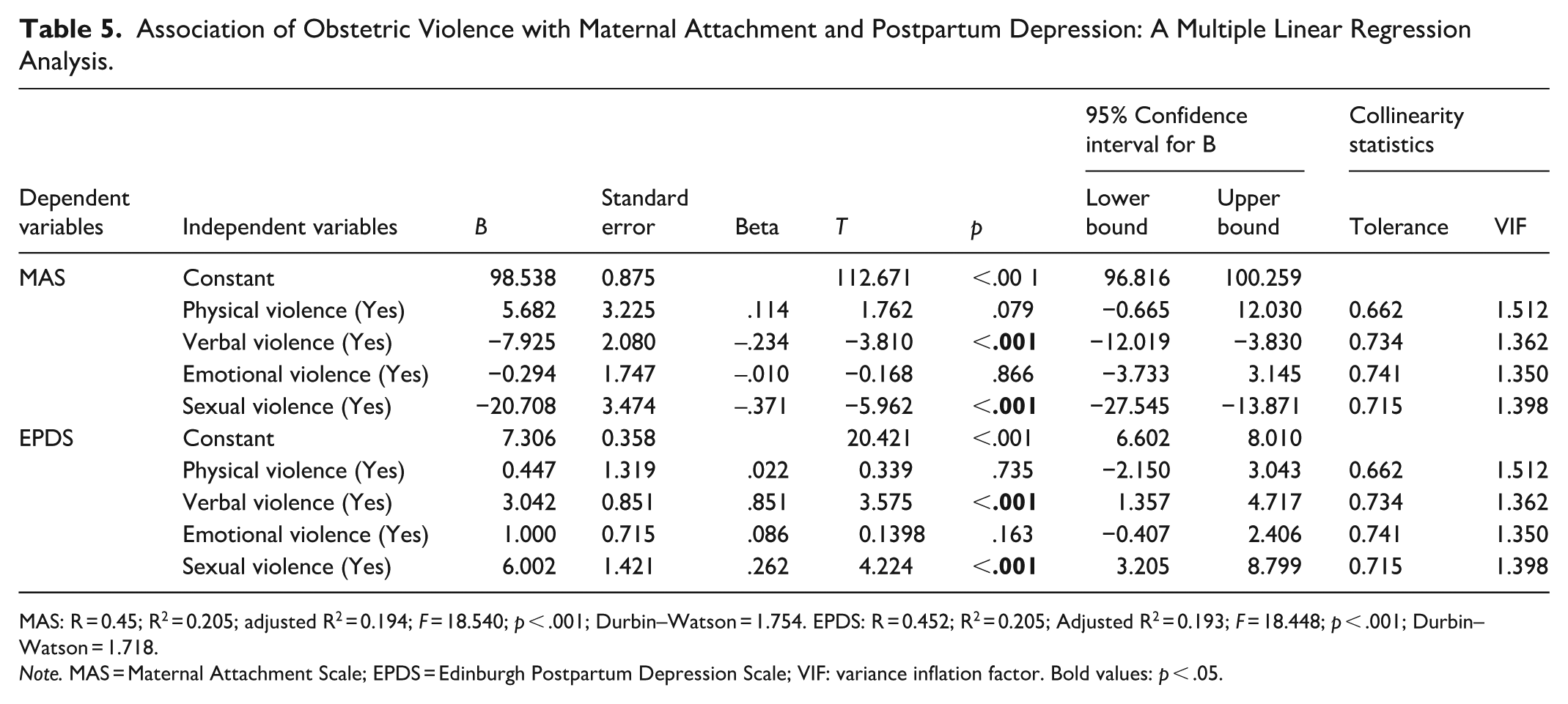
MAS: R = 0.45; R2 = 0.205; adjusted R2 = 0.194; F = 18.540; p < .001; Durbin–Watson = 1.754. EPDS: R = 0.452; R2 = 0.205; Adjusted R2 = 0.193; F = 18.448; p < .001; Durbin–Watson = 1.718.
Note. MAS = Maternal Attachment Scale; EPDS = Edinburgh Postpartum Depression Scale; VIF: variance inflation factor. Bold values: p < .05.
Discussion
The high prevalence of obstetric violence (OV) represents a serious violation of respectful maternity care principles and fundamental human rights related to dignity, autonomy, and bodily integrity (Azhar et al., 2018; WHO, 2014). Although OV is frequently reported in low-income and under-resourced settings (up to 99.7%) (Azhar et al., 2018), evidence indicates that it also remains highly prevalent in high-income countries (81%) (Baranowska et al., 2019). These findings underscore that obstetric violence is not confined to specific healthcare systems but reflects broader structural and cultural challenges in maternity care.
In the present study, emotional violence was the most frequently reported form of OV (32.9%), followed by verbal (19.5%), physical (7.9%), and sexual violence (6.2%) (Figure 1). These findings are consistent with reports from Spain (Martinez-Vázquez et al., 2022), Mexico (Cecilia et al., 2019), Poland (Baranowska et al., 2019), and Türkiye (Avcı & Kaydırak, 2023). Variations in prevalence rates across countries may reflect differences in sociocultural norms, healthcare policies, and awareness levels. Because OV is largely based on women’s subjective experiences, behaviors that healthcare professionals may perceive as routine clinical practice can be experienced by women as disrespectful or violent (Lansky et al., 2019; van der Pijl et al., 2022). This discrepancy highlights insufficient awareness and normalization of certain harmful practices within maternity care settings. The persistence of such practices, combined with underreporting and institutional tolerance, contributes to the continuation of the cycle of obstetric violence, posing significant risks to both maternal and infant well-being.
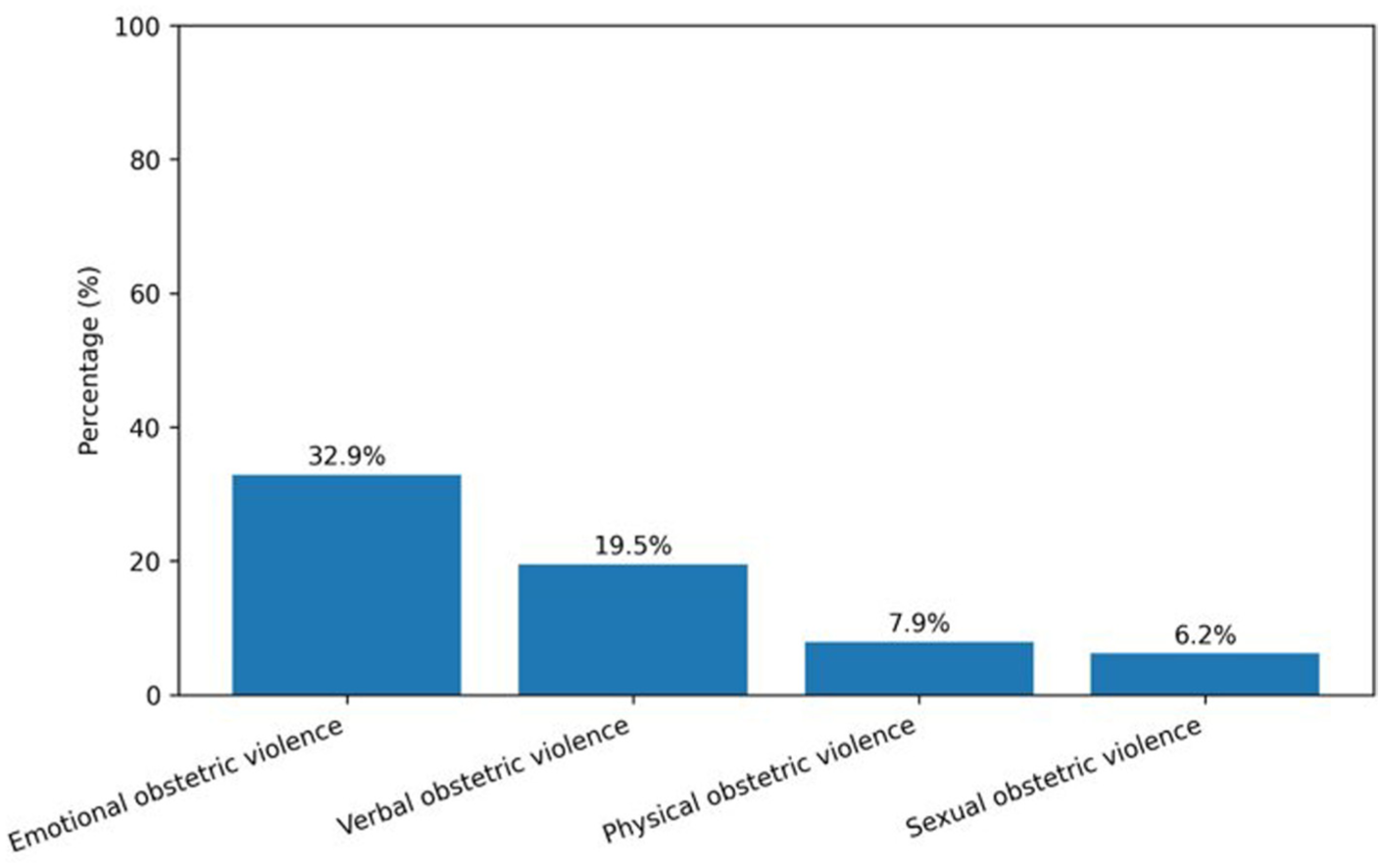
Types of Obstetric Violence.
The study findings indicate that exposure to verbal and sexual obstetric violence was associated with lower maternal attachment levels. This aligns with the findings of Taghizadeh et al. (2021), who reported that OV negatively affected maternal attachment and was linked to breastfeeding difficulties and challenges in infant care. Traumatic and dehumanizing birth experiences may disrupt a mother’s emotional connection with her infant, potentially undermining confidence in the maternal role. Over time, unresolved traumatic memories of childbirth may also diminish trust in healthcare providers and reduce willingness to seek future maternity care (Ferrão et al., 2022). Attachment theory suggests that early relational experiences between mother and infant are foundational for long-term socioemotional development (Bowlby, 1982). Disruptions in maternal attachment may manifest as reduced sensitivity to infant cues, emotional withdrawal, irritability, or inconsistent caregiving behaviors, which, in turn, may increase the risk of adverse developmental outcomes (Esposito et al., 2017; Ponti et al., 2020; WHO, 2022). By examining the relationship between OV and maternal attachment, this study contributes to a relatively underexplored area of the literature and highlights the relational consequences of disrespectful maternity care. Strengthening respectful, woman-centered birth practices and promoting early attachment interventions such as skin-to-skin contact and early initiation of breastfeeding may mitigate some of these negative effects. Nevertheless, further research is needed to clarify the mechanisms linking obstetric violence and maternal attachment.
The prevalence of PPD (21.9%) observed in this study is consistent with global estimates reported in the literature. Verbal and sexual obstetric violence emerged as significant predictors of higher PPD scores. These findings align with prior studies demonstrating a strong association between obstetric mistreatment, particularly violations involving autonomy and bodily integrity, and postpartum depressive symptoms (Martinez-Vázquez et al., 2022; Paiz et al., 2021; Souza et al., 2017). Exposure to non-consensual or humiliating practices during childbirth may compromise maternal mental health not only through depressive symptoms but also by contributing to anxiety and post-traumatic stress responses (Silva-Fernandez et al., 2023; Slomian et al., 2019). Importantly, these results emphasize that obstetric violence extends beyond physical harm and includes violations of dignity, autonomy, and respectful communication, all of which may have enduring psychological consequences.
In addition to preventive strategies, there is a growing need for supportive interventions that address the psychological aftermath of obstetric violence. Mind–body and compassion-based interventions have demonstrated potential in reducing emotional distress, depressive symptoms, and trauma-related responses among women exposed to adverse experiences (Koroglu & Durat, 2024). Interventions that enhance emotional regulation, self-compassion, and stress management may be particularly beneficial for women who perceive their childbirth experiences as traumatic or dehumanizing. Digital health formats may further improve accessibility for postpartum women who encounter barriers to in-person services.
Several limitations should be considered when interpreting these findings. The postpartum period of participants ranged from 3 to 12 months, and emotional processing of childbirth experiences may evolve over time. Women in later postpartum stages may recall and interpret their birth experiences differently from those in earlier stages. However, previous research indicates that traumatic birth memories may remain vivid and emotionally intense for extended periods (Ponti et al., 2020; Silva-Fernandez et al., 2023). Furthermore, obstetric violence was assessed based on women’s subjective perceptions rather than objective clinical records, which may introduce recall bias. Although subjective perception is central to understanding experiences of violence, the reliance on self-report and the variability in postpartum timing represent important methodological limitations. Longitudinal studies following women from the early postpartum period onward would provide more comprehensive insight into the evolving impact of obstetric violence on maternal mental health and attachment. In addition, future research may benefit from examining postpartum duration as a potential moderating variable.
Limitations and Strengths
This study has several limitations that should be considered when interpreting the findings. First, the results are limited to the study sample and therefore cannot be generalized to the broader population. The cross-sectional design precludes causal inferences regarding the relationship between obstetric violence, maternal attachment, and PPD. Future longitudinal studies are needed to clarify the directionality and long-term effects of these associations.
Second, obstetric violence experiences and psychological outcomes were assessed using self-report measures. Although subjective perception is central to the conceptualization of obstetric violence, reliance on self-reported data may introduce recall bias, social desirability bias, or underreporting. In addition, the postpartum period among participants ranged from 3 to 12 months. Emotional processing and reinterpretation of childbirth experiences may evolve over time, potentially influencing how women recall and report obstetric violence.
Despite these limitations, this study has several notable strengths. To our knowledge, it is among the first studies to simultaneously examine the relationship between obstetric violence during vaginal birth, maternal attachment, and postpartum depressive symptoms within the same analytical framework. By integrating relational (attachment) and psychological (depression) outcomes, the study provides a more comprehensive understanding of the multidimensional impact of obstetric violence. Furthermore, focusing specifically on vaginal birth experiences allows for a more homogeneous clinical context, reducing variability related to delivery type. The findings offer important implications for strengthening respectful maternity care practices, improving early mother–infant attachment, and integrating routine mental health screening into postpartum services. In this regard, the study contributes both theoretically and clinically to the emerging literature on obstetric violence.
Conclusion
This study demonstrates that obstetric violence remains a significant concern within maternity care, with emotional and verbal forms reported more frequently than physical and sexual violence. Although childbirth should represent a moment of safety and support, the persistence of disrespectful and non-consensual practices indicates ongoing gaps in the implementation of respectful maternity care principles.
The findings highlight that obstetric violence is not merely a matter of service quality but a multidimensional issue with psychological and relational consequences. Exposure to verbal and sexual obstetric violence was associated with lower maternal attachment and higher postpartum depressive symptoms, underscoring the broader impact of childbirth experiences on maternal mental health and early mother–infant attachment.
Ensuring dignified, evidence-based, and woman-centered care is a fundamental right of every woman. Strengthening professional communication, informed consent procedures, and awareness among healthcare providers may be critical steps toward preventing obstetric violence. In addition, integrating routine mental health screening and early attachment support into postpartum care may help mitigate its adverse consequences. Future research should further explore protective and supportive interventions aimed at reducing the psychological and relational effects of traumatic birth experiences, including accessible and digitally delivered postpartum services. At the policy level, institutional commitment, staff training, and accountability mechanisms are essential for fostering a culture of respectful maternity care and safeguarding maternal and infant well-being.
Footnotes
Acknowledgements
The authors would like to thank all Turkish women participating in the study.
Ethical Considerations
Ethical approval for this study was obtained from the Ethics Committee of Selçuk University, Noninvasive Clinical Research Ethics Committee (Approval No: 2023/1369) prior to data collection. The study was conducted in accordance with the principles of the Declaration of Helsinki (1964) and its subsequent amendments. Institutional permission (Date and Number: 02.02.2024-E.691638) was obtained from the relevant hospital administration.
Consent to Participate
Written informed consent was obtained from all participants prior to enrollment in the study.
Author Contributions
H.A.D.: Conceptualization, Formal analysis, Methodology, Project administration, Supervision, Writing—original draft; S.A.K.: Investigation, Writing—original draft; H.T.K.: Visualization, Writing—original draft, Writing—review & editing; R.Y.: Supervision, Validation, Writing—original draft.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from the Selçuk University Scientific Research Coordinator (Project No: 24401077).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions. Research data are not shared.