
Abstract
Objective:
To compare arch widths of patients with isolated Robin sequence (IRS) operated using modified von Langenbeck technique and modified Furlow double-opposing z-plasty.
Design:
Retrospective, transversal study.
Setting:
Hospital of Rehabilitation of Craniofacial Anomalies, University of São Paulo, Bauru, Brazil.
Patients:
Three groups of patients were analyzed. Group VL comprised 30 patients with IRS operated by von Langenbeck technique (mean age of 8.1 years); group FL included 30 patients with IRS operated by Furlow technique (7.6 years); and the control group included 30 noncleft patients with class I occlusion (7.4 years). The palate repair was performed between 1.0 and 1.7 years of age in both study groups. Transversal measurements of maxillary and mandibular arches were performed digitally on 3D digital models.
Statistic:
The intergroup comparison was performed using analysis of variance and Tukey test. An independent t test was used to compare the complete and incomplete types of cleft in both study groups. The level of significance was 5%.
Results:
No statistically significant difference was found between the VL and FL groups for maxillary and mandibular arches. However, both groups showed decreased transversal dimensions compared with the control group (P < .01) for both dental arches. No differences for arch widths were observed for complete or incomplete palatal clefts.
Conclusions:
No influence of palate repair techniques was observed in the transversal arch widths in patients with IRS. Children with IRS operated for palate repair showed constriction of the maxillary and mandibular dental arches compared with noncleft children regardless the palatal cleft extension.
Introduction
Isolated Pierre Robin sequence (IRS ) is characterized by a small and retrognathic mandible, glossoptosis, and upper airway obstruction. The association of micrognathia and glossoptosis leads to obstruction of the upper airway resulting in feeding and breathing difficulties, especially in the first years of life. Cleft palate is present in 90% of the cases (Marques et al., 2005). IRS patients have a significantly decreased mandibular length compared with patients with isolated cleft palate and does not significantly change with growth (Daskalogiannakis et al., 2001).
Previous longitudinal cephalometric studies showed that patients with IRS had smaller cranial base length, smaller maxilla length, and smaller mandibular body length and height as well as smaller ramal length and width (Laitinen et al., 1998; Suri et al., 2010). Another important occlusal feature of patients with IRS is a transversal constriction of the dental arches (Laitinen e al., 1988). Young adult patients with PRS show significantly smaller arch widths compared to patients with isolated cleft palate.
Surgical correction of the palate is performed from 1 to 2 years of age in patients with IRS (Nyströem and Ranta, 1990). Distinct surgical techniques may be used for palatoplasty including von Langenbeck procedures, Veau-Wardill-Kilner (pushback), Bardach (2-flap), and Furlow double zetaplasty (Posnick and Ruiz, 2002; Williams et al., 2009, 2011). A previous study advocated that Furlow technique achieved better results than the Von Langenbeck technique regarding hypernasality and nasal air escape (Spauwen et al., 1992). Facial and dental arch growth may also be considered for guiding the surgical technique choice.
The Von Langenback technique involves 2 relaxing incisions in the lateral region of the palate associated with a medial movement of the flaps. On the other hand, the Furlow technique involves a double zetaplasty, performed in the posterior palate, one in the oral mucosa and the other in the nasal mucosa. Considering the differences between Von Langenback and Furlow techniques, a question arises: Do these surgical procedures have a different influence on dental arch growth in patients with IRS? The aim of this study was to compare dental arch transverse dimensions in patients with isolated Robin sequence operated with Von Langenback and Furlow techniques. The null hypothesis is that patients operated with one or other of the techniques have similar dental arch widths.
Material and Methods
This study was approved by the Institutional Board of Research, Hospital of Rehabilitation of Craniofacial Anomalies, University of São Paulo, Bauru, Brazil under the number 270/2010-SVAPEPE-CEP. Dental models of patients with IRS in the mixed dentition and registered at a single center. The selection criteria was patients operated for palate repair between 1 and 1.7 years of age from 1996 to 2002 by a single plastic surgeon with 28 years’ experience to operate patients with CLP. The total number of surgeries that the surgeon performed until now is around 3218 primary palatoplasty, among them 300 patients with Furlow technique. The total number of patients with IRS operated in this time were 150 patients. The children were operated in routine, without randomization. During the first 5 years, we used Von Langenbeck technique modified by Kriens for all patients independent of size and mouth opening and in the later 5 years with Furlow technique; at the same time, the surgeon was participating in an international prospective randomized clinical trial involving unilateral cleft lip and palate comparing von Langenbeck and Furlow technique. The exclusion criteria of the study groups were the history of previous orthodontic treatment, early deciduous teeth loss, presence of dental anomalies, and associated syndromes. The study comprised 3 groups. Group FL was composed by 30 patients (15 with complete cleft palate and 15 with incomplete cleft palate) with a mean age of 7.6 years (17 males and 13 females) operated by Furlow technique for palatoplasty. Group VL was composed by 30 patients (17 with complete cleft palate and 13 with incomplete cleft palate) with a mean age of 8.1 years (16 males and 14 females) operated by von Langenbeck technique. The children were operated in the hospital routine, without randomization.
The control group was composed by 30 orthodontics patients without craniofacial anomalies and with class I occlusion and class I skeletal pattern (15 boys and 15 girls). The average age of the control group was 7.4 years.
The dental casts were digitized using the 3Shape R700 3D scanner (3Shape A/S, Copenhagen, Denmark). Intercanine and intermolar distances were measured on the maxillary and mandibular arches (Figure 1) using the Ortho Analyzer 3D software. The measurements were performed by a single calibrated examiner.
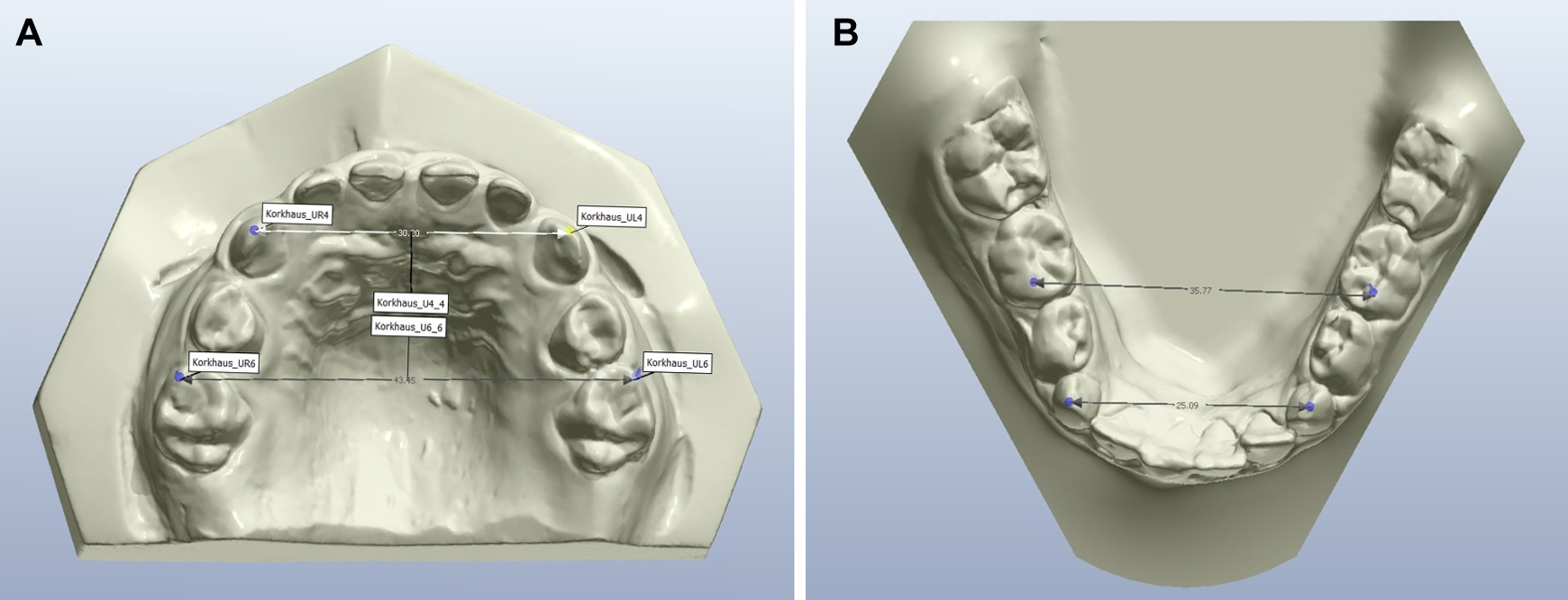
Measurement of the intercanine and intermolar distances on the maxillary and mandibular arches. Intercanine distance was measured at the cusp tips. Intermolar distance was measured at the mesiobuccal cusp tip of the second deciduous molars.
Statistical Analysis
Data distribution was analyzed using Shapiro-Wilk test. Intergroup comparisons were performed using analysis of variance (ANOVA) and the Tukey test. Independent t test was used to compare the complete and incomplete types of cleft. The significance level considered was 5% (P < .05).
Results
Reliability using intraclass correlation coefficient was considered excellent (0.98). Data showed a normal distribution (P > .05). Table 1 shows the results for intergroup comparisons. No differences were observed between arch widths in patients operated by Furlow and von Langenbeck techniques either in maxillary arch widths comparing complete and incomplete palatal clefts (Table 2). However, the study groups showed decreased maxillary and mandibular arch widths when compared to the control group.
Intergroup Comparisons for Arch Widths (Analysis of Variance and Tukey Test).a
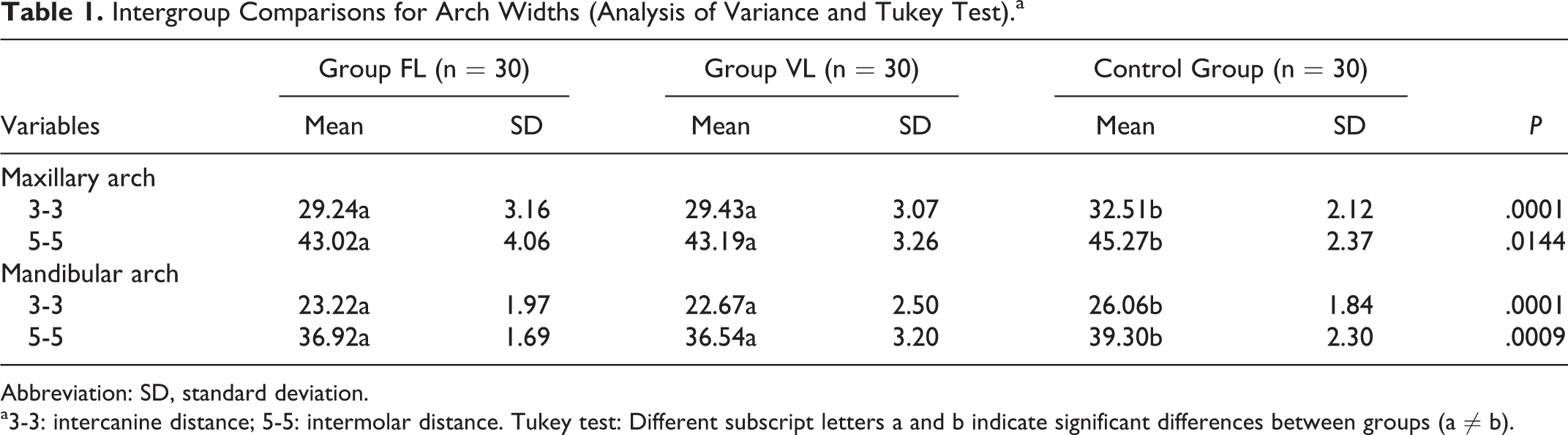
Abbreviation: SD, standard deviation.
a3-3: intercanine distance; 5-5: intermolar distance. Tukey test: Different subscript letters a and b indicate significant differences between groups (a ≠ b).
Comparison Between Complete and Incomplete Palatal Cleft (Independent t Test).a
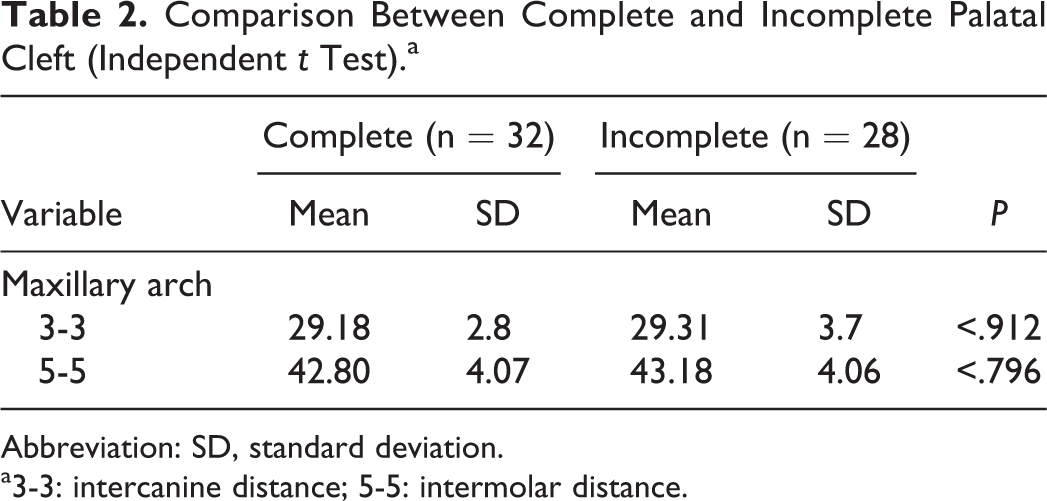
Abbreviation: SD, standard deviation.
a3-3: intercanine distance; 5-5: intermolar distance.
Discussion
The goal of the palatal repair is to obtain a morphologic and functional reconstruction of the velopharyngeal mechanism leading to normal speech without impairing facial growth (Brown et al., 1983; Millard and Latham, 1990; Oliveira, 2009). The present study showed no difference between von Langenbeck and Furlow techniques for the transverse dimensions of the dental arches in children with IRS (Table 1).
Previous studies showed that Furlow technique yields better results for speech and a decreased need for secondary pharyngoplasty when compared with the veloplasty intravelar in cleft palate patients (Gunther et al., 1998; Oliveira, 2009).
Both groups with IRS showed smaller maxillary and mandibular arch widths compared to the control group (Table 1). These findings are in agreement with Laitinen and Ranta (1998) and may be explained by the absence of midpalatal suture and tension produced by the palatal repair. The dimensions of the dental arches in subjects with isolated cleft palate are significantly smaller than those of individuals without cleft, before and after palatoplasty (Nyströem and Ranta, 1989; Heliövaara et al., 2007). Children with IRS at the age of 6 years showed a decreased maxillary and mandibular premolar widths compared to patients with isolated cleft palate (Laitinen, 1993). Patients with isolated Robin sequence usually shows class II molar relationship with mandibular anterior crowding, increased overjet, and convex profile due to mandibular deficiency (Ozawa et al., 2012). The class II interarch relationship may contribute to decreased transversal dimensions of the maxillary arch. In subjects with a retrognathic mandible, the upper arch occludes with the more anterior region of the mandibular arch, leading to a maxillary transversal compensation (Silva Filho et al., 2009). The interesting finding was that the mandibular dental arch also showed decreased transversal dimensions in patients with PRS compared with the control group (Table 1). The possible explanation for the constriction of the mandibular arch is the hypothesis of an inherent mandibular micrognathia in IRS, that does not change with growth (Daskalogiannaki et al., 2001).
No differences for the dental arch transversal dimensions were observed between patients with complete and incomplete palatal cleft (Table 2). These results are not in accordance with Hellquist et al. (1978) and Heliövaara and Rautio (2005), who observed significant differences between complete and incomplete clefts. However, the sample of these previous studies included patients with submucosal palatal clefts, and the sample included only patients with isolated cleft palate.
Conclusions
The null hypothesis was accepted. Patients with IRS operated with Furlow and von Langenbeck techniques had similar transversal arch widths. Children with IRS operated for palate repair in the first year of life show constriction of maxillary and mandibular dental arches compared to noncleft children, regardless of cleft extension.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.