
Abstract
Objective:
To compare the Veau-Wardill-Kilner technique with the Minimal-Incision technique repair of isolated clefts of the hard and soft palate regarding facial growth at 5 and 10 years of age.
Design:
Retrospective study of lateral cephalograms.
Setting:
Hospital and university based.
Patients:
A consecutive series of 145 Caucasian nonsyndromic children born with isolated cleft palate between 1980 and 1996 were studied. Children with Pierre Robin sequence (PRS) were included in the study. The patients were divided into 4 groups: 2 groups regarding surgical technique and 2 groups regarding cleft length.
Intervention:
Veau-Wardill-Kilner or Minimal-Incision palatoplasty.
Main Outcome Measures:
Eleven skeletal and 1 soft tissue measurement were evaluated from lateral cephalograms taken at 5 and 10 years of age.
Results:
Only minor differences in cephalometric morphology were found between the Veau-Wardill-Kilner technique group and the Minimal-Incision technique group. Similar results were found independent of cleft length or the inclusion of PRS in the sample.
Conclusion:
The craniofacial cephalometric morphology at 5 and 10 years of age in patients with isolated cleft palate is similar between the Veau-Wardill-Kilner and the Minimal-Incision technique group.
Keywords
Introduction
It is known since more than 40 years that palatoplasty is a procedure that disturbs maxillary growth (Ross, 1970). Therefore, different surgical procedures have been developed aiming at avoiding growth inhibition and, at the same time, creating good speech development. What technique should be used and at what age it should be performed have been debated. According to Ross (1987), surgery of the hard palate inhibits forward translation of the maxilla and forward development of the alveolar process, and surgery of the soft palate might inhibit posterior vertical maxillary development. He also reported that the common techniques for hard and soft palate repair used at that time period almost had the same effect on facial growth. Other studies (Bishara et al., 1976; Becker et al., 2001) indicated that the effect on anteroposterior and vertical growth of the craniofacial complex did not differ comparing older 1-stage procedures. In 2005, Fujita et al. found that the maxillary length was shorter and that the nasomaxillary complex was positioned more posteriorly in relation to the anterior cranial base of adults with isolated cleft palate (ICP) compared to patients without a cleft. Studying a 2-stage closure of isolated cleft palate, Jakobsson (1990) indicated that the most important independent variables were cleft extent and sex, as both had statistically significant influence on several of the studied cephalometric measurements.
Several new techniques have been developed to reduce the amount of scar tissue, which has been regarded as the cause of the disturbed maxillary and dentoalveolar growth in one-stage, minimal-incision (MI) technique (Mendoza et al., 1994) or two-stage procedures (Friede et al., 1980; Furlow, 1986; Johanson et al., 1986; Friede et al., 1987). In an earlier study of casts comparing the Veau-Wardill-Kilner (VWK) technique (Nylén, 1961) with the MI technique in patients with isolated cleft palate (Karsten et al., 2003), it was found that the MI technique resulted in better transversal development of the upper jaw and a less affected palatal mucosa with significantly less scar tissue. The quality of speech showed no apparent differences between the two surgical techniques concerning the amount of fistulae or the need for pharyngeal flaps (Nyberg et al., 1997).
The aim of this study was to compare the VWK technique with the MI technique regarding facial growth in patients born with isolated cleft palate. The null hypothesis was that there is no difference in facial growth in patients born with isolated cleft palate treated with the two surgical techniques.
Material and Methods
This study has been approved by the ethical committee in Stockholm, no. 2009/1680-31/2.
Patients
In the region of Stockholm, 257 children with isolated cleft palate were born between 1980 and 1996. To be included in the study, the children had to be Caucasian, nonsyndromic, with complete records, and treated by the Stockholm Craniofacial Team. Eighty-nine children were non-Caucasian or had craniofacial malformations and were excluded before the investigation. Children with Pierre Robin sequence (PRS) (micrognathia and glossoptosis with airway obstruction; 19 individuals) were included in the study. Lateral cephalograms were not available for 23 children. The material to be investigated finally consisted of data from 145 children.
The material was divided into two groups according to the surgical procedure performed in Stockholm for palate repair (V [VWK] or M [MI] technique). The VWK technique was applied for children born from 1980 till 1986 and shifted to the MI technique for children born from 1987 till 1996 because of an effort to reduce the amount of scar tissue. Each group was divided into two subgroups depending on the sagittal extension of the cleft (1: small or 2: big) (Table 1).
Group V1. Clefts within the soft palate only and a notch less than 3 mm in the posterior border of the hard palate, repaired using the VWK technique, n = 34 (13 boys, 21 girls); 2 PRS.
Group V2. Clefts within the soft and hard palate, repaired using the VWK technique, n = 25 (8 boys, 17 girls); 5 PRS.
Group M1. Clefts within the soft palate only and a notch less than 3 mm in the posterior border of the hard palate, repaired using the MI technique, n = 30 (16 boys, 14 girls); 1 PRS.
Group M2. Clefts within the soft and hard palate, repaired using the MI technique, n = 56 (24 boys, 32 girls); 11 PRS.
Presentation of the Total Number of Patients Divided into 4 Groups After the Surgical Technique: Veau-Wardill-Kilner (V) or Minimal Incision (M), and the Length of the Isolated Cleft in the Palate: Small Cleft (1) or Big Cleft (2).a
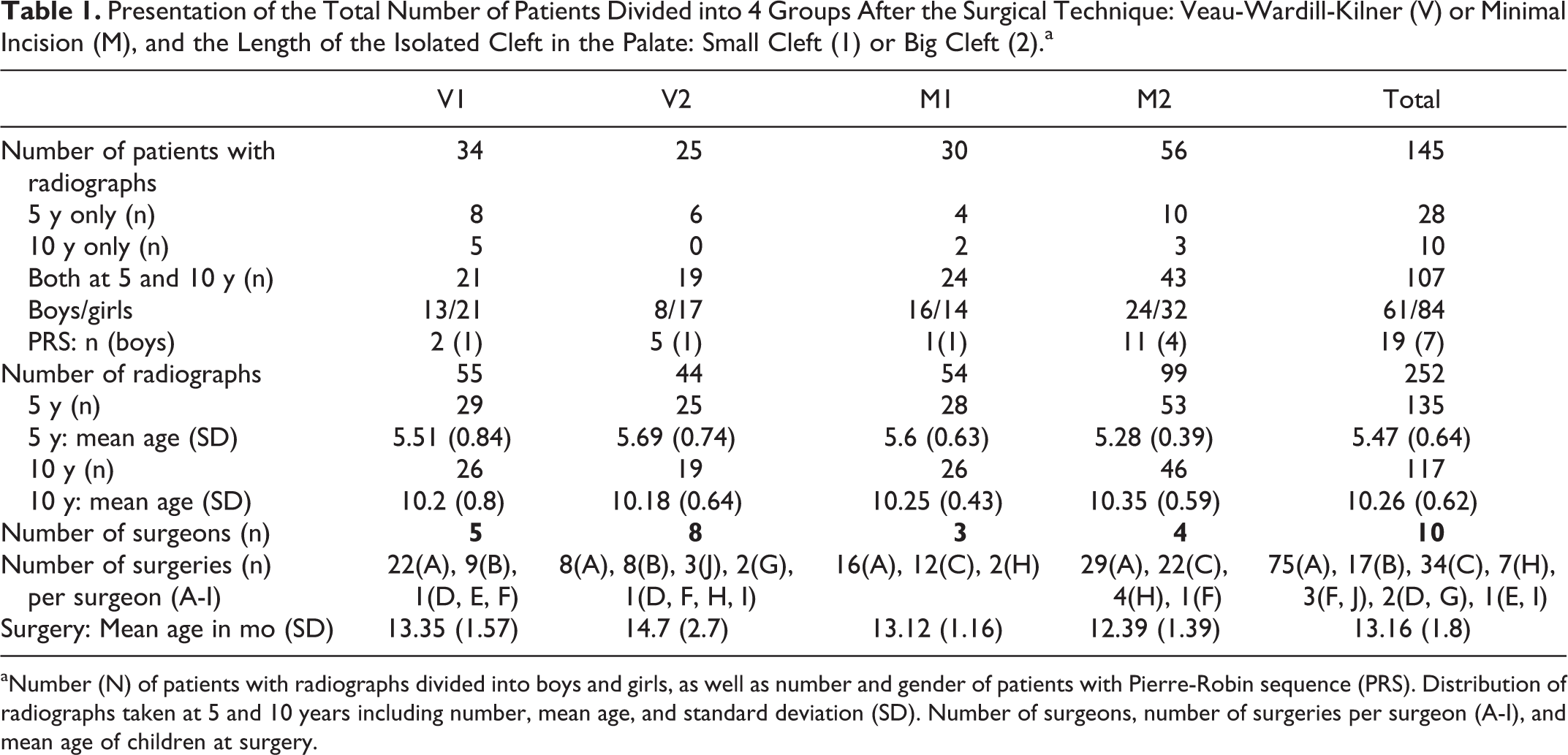
aNumber (N) of patients with radiographs divided into boys and girls, as well as number and gender of patients with Pierre-Robin sequence (PRS). Distribution of radiographs taken at 5 and 10 years including number, mean age, and standard deviation (SD). Number of surgeons, number of surgeries per surgeon (A-I), and mean age of children at surgery.
Comparing the 4 groups (Table 1) concerning age (5, 10 years), gender (male, female), existence of PRS, and age at operation (V, M; 1, 2), chi-square tests and 1-way analyses of variance (ANOVAs) with special contrasts were applied, providing statistically significant results only for age at operation when V and M groups were compared (P = .32, .42, .064, .0001, and .25, respectively).
Treatment Methods
Groups V1 and V2 were operated on by 5 and 8 of the surgeons respectively at the department using the VWK technique (Figure 1A) at an average age of 13 months for group V1, and 14 months for group V2 (Table 1). Children in group M1 were operated on by 3 and in group M2 by 4 of the surgeons at the department using the MI technique (Figure 1) at an average age of 13 months (Table 1).
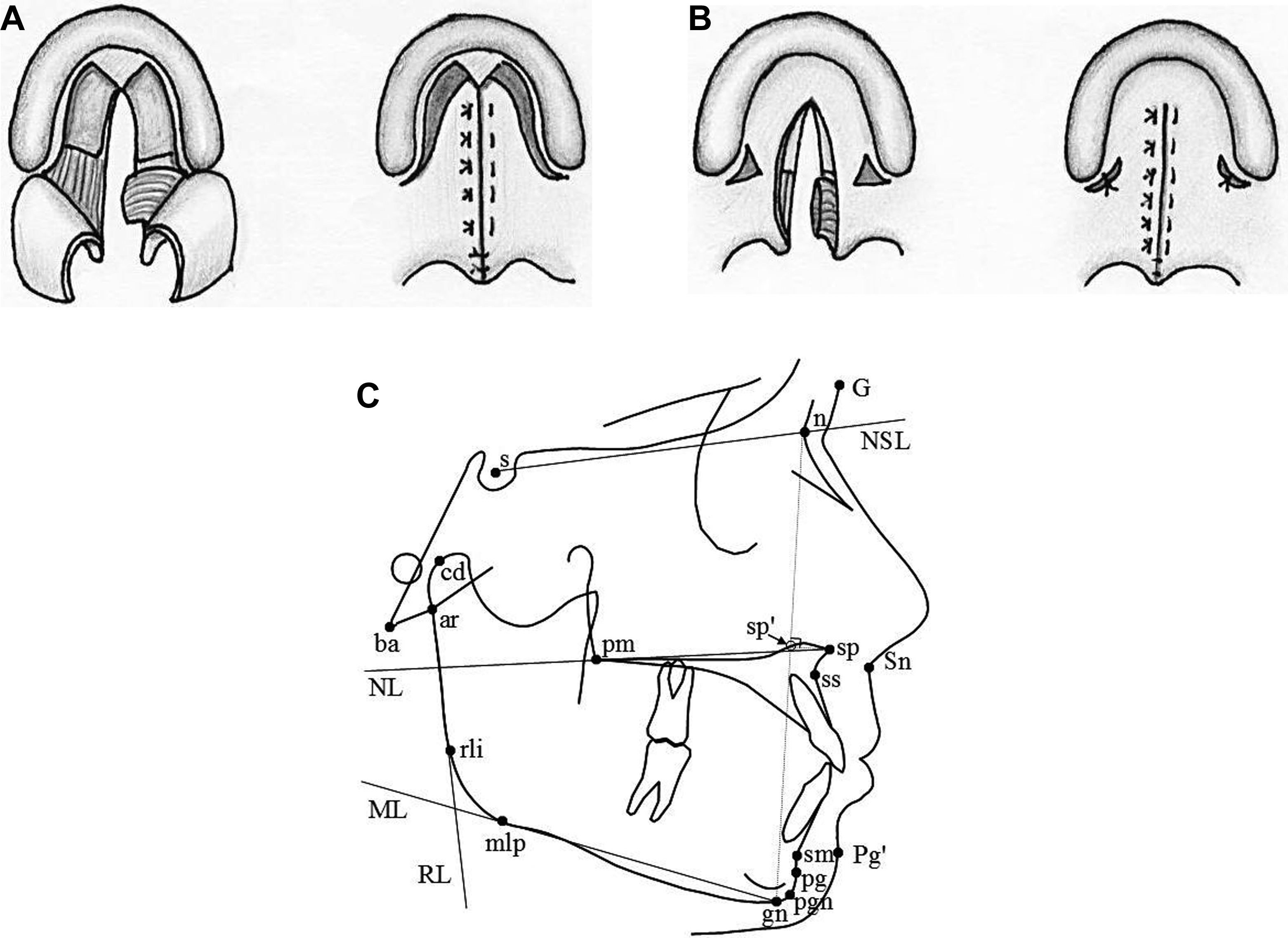
(A) The Veau-Wardill-Kilner technique. Left: Mucoperiosteal flaps are raised, the hamulus is identified, and the tendon of the tensor velopalatini muscle is slipped over the hamulus (not illustrated in the figure); the posterior border of the hard palate is freed from muscle insertions. Right: The nasal mucosa is sutured separately (not shown), the oral mucosa is closed with mattress sutures that within the soft palate also unite the muscle bundles on each side. Raw wound surfaces are left for secondary healing laterally and anteriorly. (B) The minimal incision technique. Left: Within the hard palate, the mucoperiosteum is elevated from the nasal and oral sides of the palatal shelves. In wide clefts, the greater palatine vessels are, when necessary, carefully dissected free to get better mobility of the oral mucoperiosteum. Through the lateral incisions the hamulus is identified and the tendon of the tensor veli palatini muscle is slipped over the hamulus. In medial direction, the muscles are released from the posterior border of the hard palate. The levator muscle is elevated. Right: The nasal, the muscle, and the oral layers are sutured separately. The wound surfaces behind the maxillary tuberosities are only sutured if this is possible without stretching the tissue. (C) Reference points (sp’ is the perpendicular projection of sp on the n-gn line) and linear measurements used in the study. Hard tissue: (n-s-ba)º, (s-n-ss)º, (ss-n-sm)º, (NSL/NL)º, (NSL/ML)º, (ML/RL)º, (n-ss-pg)º; palatal plane length: (sp-pm) mm; mandibular length (cd-pgn) mm, n-sp’/n-gn (%), sp’-gn/n-gn (%); soft tissue: (GSnPg’)º.
Examination Methods
Radiographic records were retrieved for 145 children. A cephalometric evaluation at 5 (mean age 5.5 ± 0.6 years) and at 10 years (mean age 10.3 ± 0.6 years) of age was performed in a total of 252 lateral cephalograms (Table 1). One hundred seven of the 145 children were examined at both 5 and 10 years. The analog radiographs were scanned at 300 dpi and an 8-bit gray-scale with a scanner (Epson Perfection V700 Photo; Seiko Epson Corp, Japan) providing digitized cephalograms. All radiographs were adjusted to zero magnification and analyzed using a cephalometric software (Viewbox 3.1.1.12; dHAL Software, Kifissia, Greece). The lateral cephalograms were unidentified and were traced and analysed at 5 and 10 years by one author (K.P.). Reference points were defined by Solow and Tallgren (1976) and Legan and Burstone (1980) and marked directly on the radiographs on the computer screen. For the calculation of facial heights, a constructed point (sp’; the perpendicular projection of sp on the n-gn line) was used. Eleven skeletal and 1 soft tissue measurement were evaluated (Figure 1C).
To test for intraobserver errors of measurements, 15 randomly selected cephalograms from each group were traced twice within a 2-week interval. After this evaluation, all 252 radiographs were unidentified and randomly traced twice by the same author (K.P.) and the mean values of the 2 digitizations were used. Because of difficulty in providing full registrations for all patients and the variety of quality of the radiographs, all available lateral cephalograms were included but measurements based on landmarks difficult to identify were excluded for every individual film. The main areas of uncertainty in some x-rays were the area of anterior nasal spine (especially ss point) and the soft tissue profile.
Statistical methods
Separate analyses for the data at 5 and 10 years were performed to compare the methods V and M. In comparisons between method V and M for subgroup 1 (soft palate only) and for subgroup 2 (soft and hard palate), a 2-way ANOVA with the factors surgery types (V, M) and cleft types (1, 2) was performed.
The growth for each patient from 5 to 10 years was analyzed using a 3-way ANOVA with repeated measurements on 1 factor. As there also were additional incomplete data, a mixed model analysis was performed, which does not require complete data from all patients (Brown and Prescott 2006; Littell et al., 2006). The between-group factors in the models were type of surgery (V, M) and cleft types (1, 2), and the within-group factor was time (5 years and 10 years). Mean values and 95% confidence intervals were estimated from the ANOVA model for different subgroups. The 0.05 level of significance was used. When applying the Bonferroni correction for multiple testing, as our variables are not independent, the α value was lowered to 0.01.
All the statistics were calculated using the software SPSS 22.0 (IBM Corp, Armonk, NY). According to the calculation of the sample size (α = 0.05; effect size ω2 = 0.06; power = 0.80), a total sample of 128 individuals was needed.
The intraobserver method errors Si
were calculated using the formula
Results
Age of 5 Years (Table 2)
Difference in the mandibular length among groups was the only statistically significant finding at the age of 5 years when applying the Bonferroni correction for multiple testing, including or excluding patients with PRS. Comparing the groups V2 and M2 at 5 years of age, a statistically significant difference was found for the mandibular length (P < .01), which was shorter in group M2. Studying the cleft groups M1 and M2 at 5 years of age, a significantly shorter mandibular length (P < .01) was found in cleft group M2 (Figure 2A).
Mean Values and Standard Deviations (SDs) for the Cephalometric Variables Based on Complete Data on the Patients at 5 Y of Age.
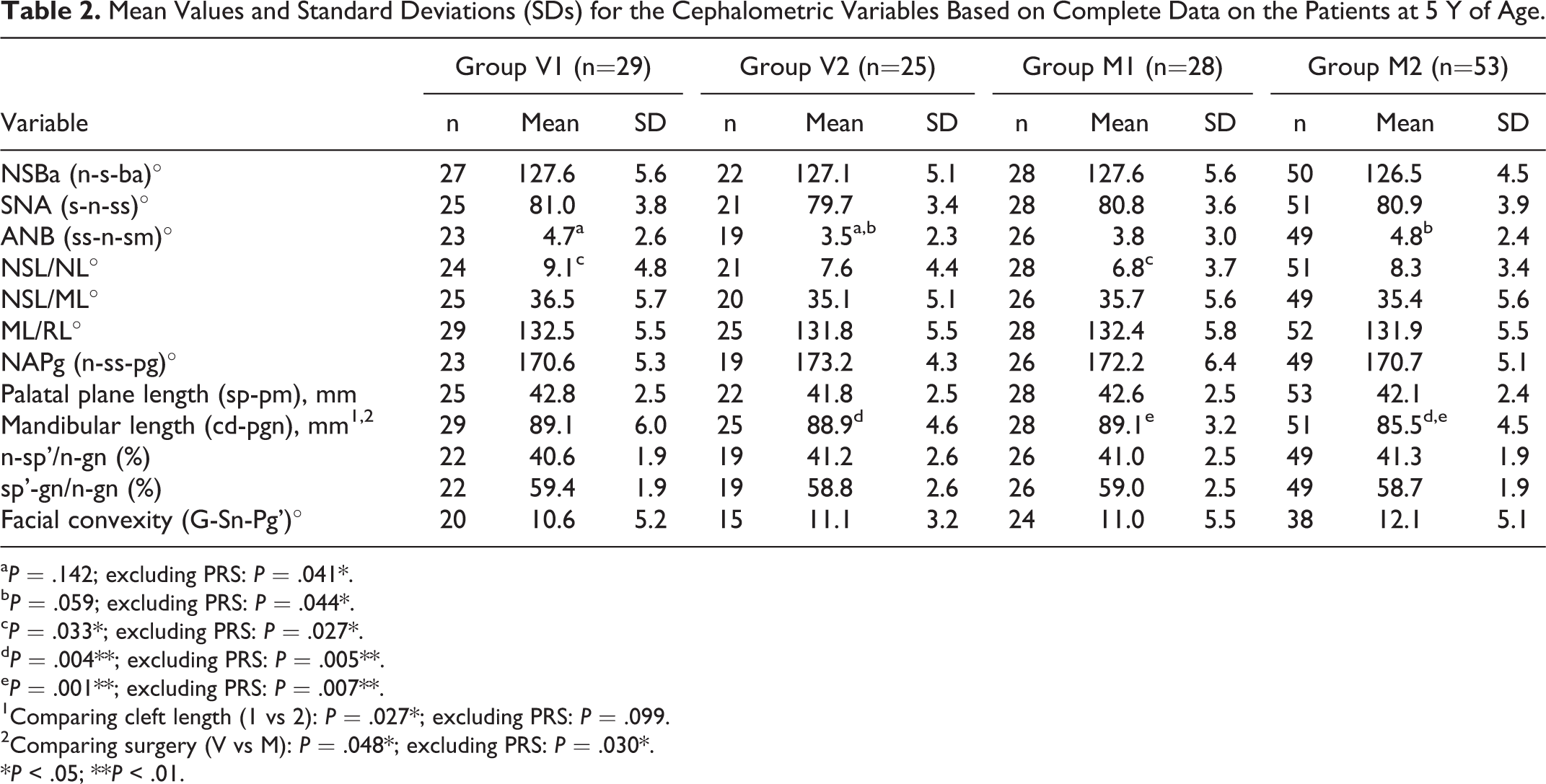
a P = .142; excluding PRS: P = .041*.
b P = .059; excluding PRS: P = .044*.
c P = .033*; excluding PRS: P = .027*.
d P = .004**; excluding PRS: P = .005**.
e P = .001**; excluding PRS: P = .007**.
1Comparing cleft length (1 vs 2): P = .027*; excluding PRS: P = .099.
2Comparing surgery (V vs M): P = .048*; excluding PRS: P = .030*.
*P < .05; **P < .01.
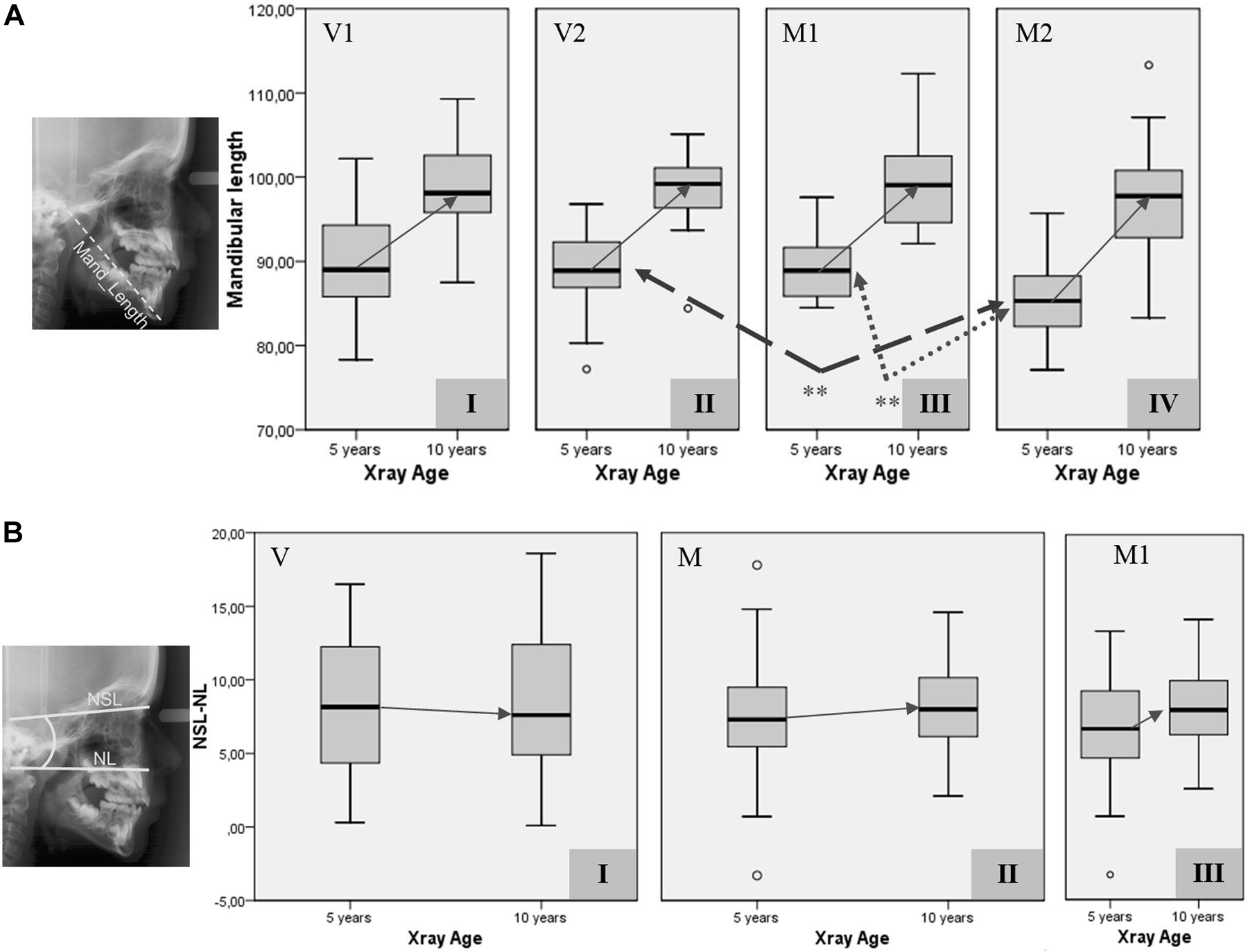
(A) Mandibular length from 5 to 10 years for the investigated groups according to surgery type (V: Veau-Wardill-Kilner palatoplasty; M: Minimal Incision palatoplasty) and cleft length (1: cleft of the soft palate—small; 2: cleft of the soft and hard palate–big). I: group V1, II: group V2, III: group M1, IV: group M2. Statistically significant results at 5 years are illustrated with stars. (B) NSL/NL angle from 5 to 10 years for the investigated groups according to surgery type. I: group V, II: group M, III: subgroup M1.
More differences were significant before the application of the Bonferroni correction for multiple testing. Comparing the cleft length group 1 (V1+M1) to 2 (V2+M2) or the surgical technique group V (V1+V2) to M (M1+M2), the differences in the mandibular length were statistically significant (P < .05).
Studying the groups V1 and M1 at 5 years of age, a statistically significant difference was found for the NSL/NL angle (P < .05), which was smaller in group M1.
Comparing the surgical technique groups V2 and M2 at 5 years of age, a statistically significant difference was found for the ANB angle (P < .05), which was smaller in group V2 when excluding patients with PRS. Studying the cleft groups V1 and V2 at 5 years of age, a significantly smaller ANB angle (P < .05) was found in cleft group V2 when excluding patients with PRS.
Age of 10 Years (Table 3)
No statistically significant differences were found between the groups at the age of 10 years when applying correction for multiple testing, including or excluding patients with PRS.
Mean Values and Standard Deviations (SDs) for the Cephalometric Variables Based on Complete Data on the Patients at 10 Y of Age.
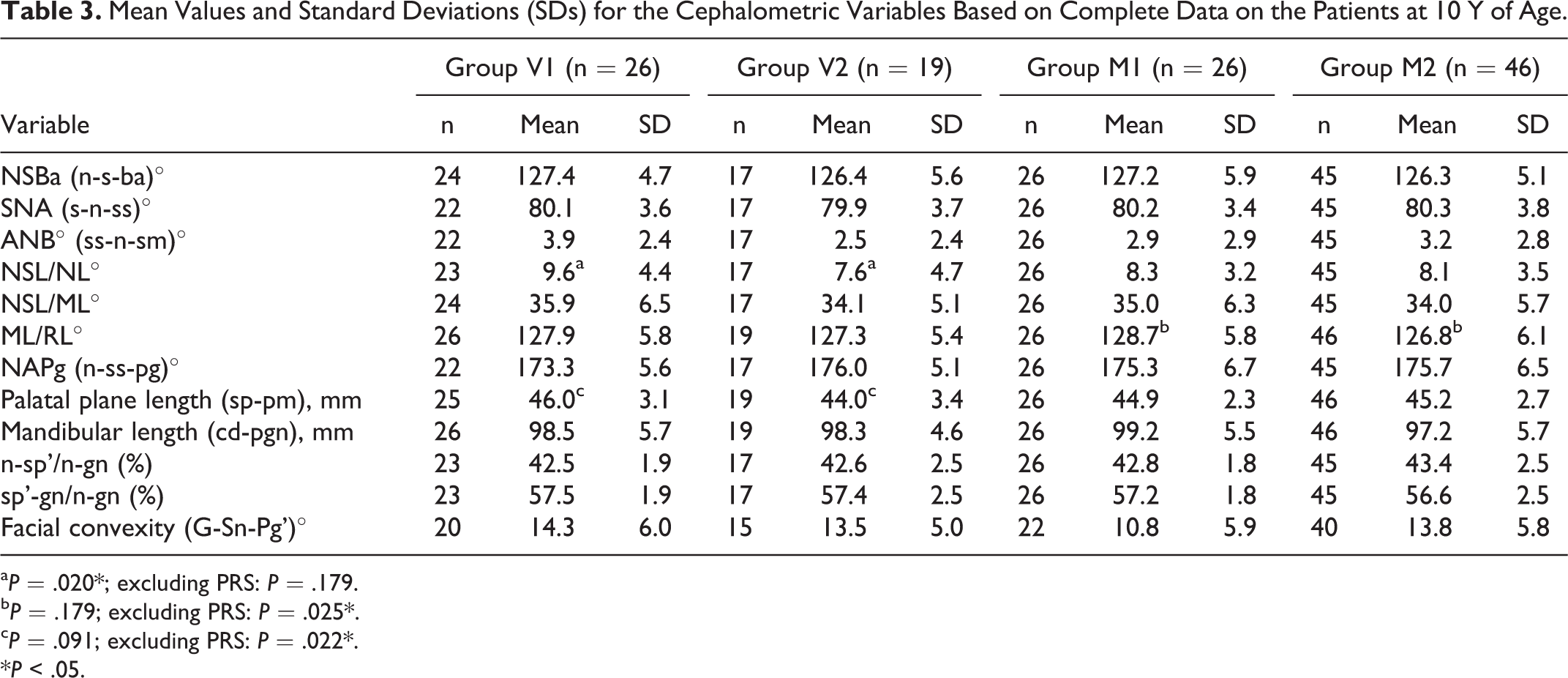
a P = .020*; excluding PRS: P = .179.
b P = .179; excluding PRS: P = .025*.
c P = .091; excluding PRS: P = .022*.
*P < .05.
Differences were significant before the application of the Bonferroni correction. Studying the groups V1 and V2 at 10 years of age, a significantly shorter palatal plane length (P < .05) was found in cleft group V2 when including the 19 patients with PRS. Comparing the cleft groups V1 and V2 at 10 years of age, a significantly smaller NSL/NL angle (P < .05) was found in cleft group V2 when excluding the patients with PRS. Studying the groups M1 and M2 at 10 years of age, a significantly smaller ML/RL angle (P < .05) was found in cleft group M2 when excluding the 19 patients with PRS.
Changes from 5 to 10 Years (Table 4)
The application of the 3-way factorial ANOVA as well as the mixed model analysis provided the same results (Table 4). The variables NAPg, palatal plane length, mandibular length, n-sp’/n-gn, and facial convexity were increased and ANB, NSL/ML, sp’-gn/n-gn, and gonial angle were decreased significantly (P < .001) from 5 to 10 years (Table 4).
Three-Way ANOVA and Mixed Model Analysis Performed Both for the Complete Material (PRS) and Excluding the PRS Children (no PRS): Significant P Values Between 5 and 10 Y Evaluating Factors Cleft Length (1, 2), Surgery Type (V, M), and Time (5, 10 y).
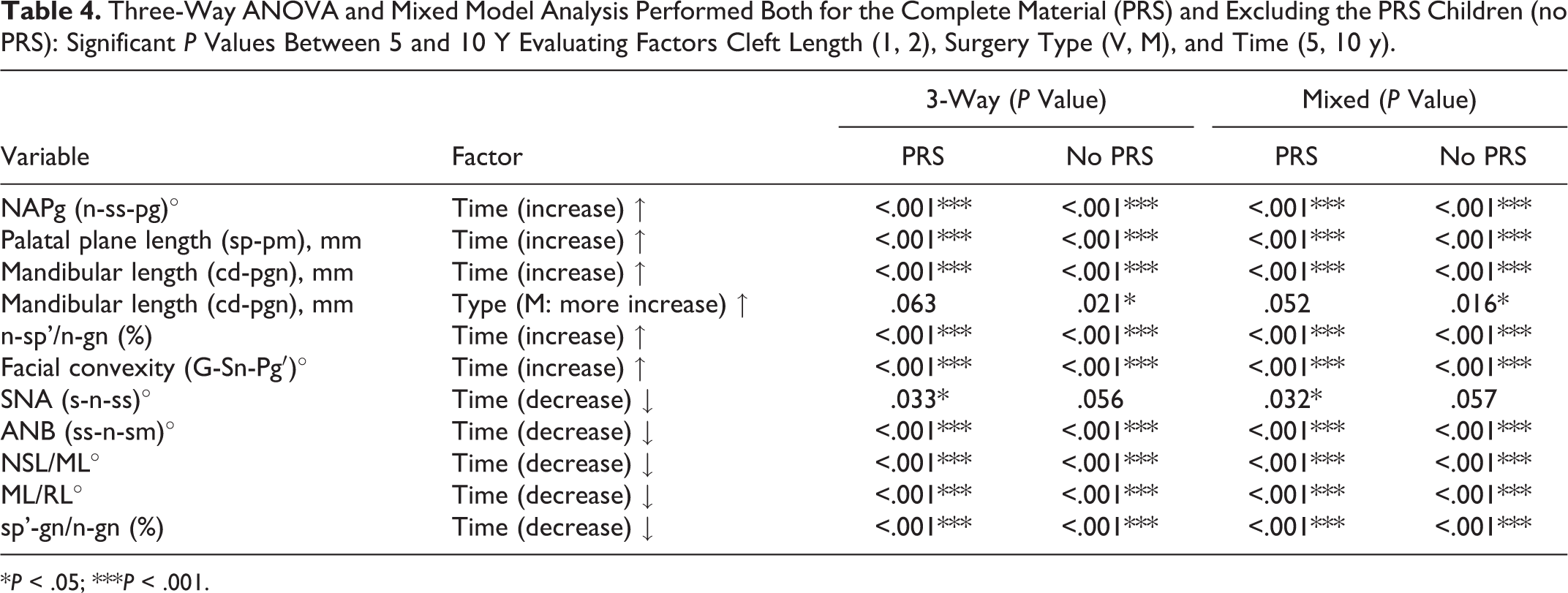
* P < .05; *** P < .001.
Before the application of the Bonferroni correction for multiple testing, an additional difference with time, a decrease of the SNA angle was statistically significant when including the PRS subjects (P < .05). Additionally comparing the surgical technique groups V and M from 5 to 10 years, excluding the PRS children, a statistically significant greater increase in mandibular length (P < .05) was found for the surgical technique group M, which included both cleft group 1 and 2 (Table 4, Figure 2A).
Discussion
The purpose of this retrospective study was to compare the Veau-Wardill-Kilner technique with the Minimal-Incision one regarding facial growth in patients with isolated cleft palate within the soft palate only and within the hard and soft palate at 5 and 10 years of age.
The total material consisted of 61 boys and 84 girls. It was decided to combine both genders as the investigated ages were before adolescence. The subgrouping of the material into surgical technique and cleft length was based on the same definition as in Karsten et al. (2003) using surgical records and casts. The diagnosis of PRS was based on clinical judgment. Compared to patients with ICP, children with PRS seem to have a wider and U- or V-shaped cleft (Godbout et al., 2014). At the age of 4 to 7 years, they have similar mandibular lengths, but at the age of 10 to 13 years they have a shorter mandible and a slightly shorter maxilla (Shen et al., 2012). As the inclusion of PRS children might influence the result of maxillary growth and mainly of mandibular sufficiency in growth, the material was investigated with and without the PRS children.
The material was first studied at 5 years including patients with PRS. Comparing the 2 surgical methods and the 2 cleft lengths, the mandibular length was significantly shorter in children having a big cleft and operated with the minimal incision technique (group M2) (Figure 2A). This is in agreement with Viteporn et al. (1991) who showed that patients with total clefts had the shortest mandibular lengths. The M2 group was the biggest and whether the smaller mandible in this group at 5 years was due to the surgical intervention (or length of cleft) or to the material of isolated cleft palate is unclear. A significantly smaller NSL/NL angle was also found at the small cleft group for the MI technique (group M1).
The only exception found at 5 years when excluding the children with PRS was that the big cleft group operated with the Veau-Wardill-Kilner (V) technique (group V2) had a smaller ANB angle. Furthermore, the addition of PRS could lead to an increase of the ANB angle, making the difference not statistically significant.
At the age of 10 years including patients with PRS, the big cleft group of the V technique showed a shorter palatal length than the small cleft group, which could be due to a restriction in maxillary growth as the surgical intervention is more severe. However, the difference was not statistically significant when evaluating children without PRS.
At the age of 10 years excluding patients with PRS, 2 new results were found when comparing the 2 cleft lengths. The big cleft group showed a smaller gonial angle at the M surgical group, showing a more horizontal pattern of growth. Further, a smaller inclination of the NL to NSL was revealed for the big cleft group at the V surgical technique (group V2) when comparing the 2 cleft lengths. However, the results on the inclination of NL to NSL should be interpreted with caution as the method error of NSL/NL was high.
From 5 to 10 years including patients with PRS, 2 examined variables remained the same and 9 changed significantly toward the direction of normal development (Table 4). Facial convexity, apart from the M1 group, increased, which was unexpected according to the growth of unaffected children (Thilander et al., 2005) and a previous study by Heliövaara et al. (2003). However, the V2 group was the smallest group (25 children) and both cephalograms at 5 and 10 years could be analyzed only from 19 individuals. Furthermore, only 15 cephalograms were used for measurement of facial convexity (the smallest number of all variables), as the soft tissue on the cephalograms was not always of good quality and some had to be excluded. The hard tissue convexity (NAPg) changed in the opposite direction, which may imply that a skeletal retrusion can be masked by soft tissue, as found by Smahel (1984) and Heliövaara and Ranta (1993) at adulthood. The SNA angle from 5 to 10 years reduced significantly in all groups. This finding indicates that horizontal maxillary growth in children born with an isolated cleft in the palate seems to be restrained no matter surgical technique or cleft length. This is in disagreement with the literature, where SNA has been reported to be smaller at complete compared to partial clefts (Jonsson and Thilander, 1979; Smahel, 1984; Heliövaara and Ranta, 1993; Iwasaki et al. 2014).
Examining the changes from 5 to 10 years excluding the children with PRS, 2 additional differences were found. The mandibular length was significantly more increased in patients operated with the MI technique for both small and big clefts. The increase of the mandible in the M group could be explained by the fact that the inclusion of children with PRS can mask the “catch-up” growth of the mandible of individuals with ICP. Xu et al. (2014) comparing unoperated ICP to normal found a shorter mandible at the age of 5 to 7 years, but a similar mandible at the age of 12 to 14 years. Additionally, as we know that the V technique constricts the maxilla transversally already at the age of 5 (Karsten et al., 2003), probably a restricted maxilla could lock the mandible and impede its growth. According to a previous study comparing craniofacial morphology at adulthood after 2 different palatoplasties (Heliövaara and Ranta, 1993), mandibular length was found to be increased in the VWK group compared to a group operated with a modified Cronin technique. The second difference from 5 to 10 years when excluding the PRS children is that the difference in SNA angle is not significant anymore. One could assume that the restriction in anteroposterior growth of the maxilla is due to the PRS children. However the high method error of the A point could be one reason for interpreting the result on SNA with caution. Further, an almost statistically significant increase (P = .05) was found regarding NSL/NL for the surgical technique group M, especially M1, compared to a small change for group V (Figure 2B). It is interesting, even if this is on the border of significance, that the direction of change of NSL/NL from 5 to 10 years is different at group V, where it decreases, and at group M, where it increases. The main change among the 4 subgroups is at M1 group where the angle NSL/NL increases more, showing a different mode of growth depending on subgrouping.
When applying the Bonferroni correction for multiple tests, the level of significance is lowered to 0.01. Then at the age of 5 years, differences at ANB and NSL/NL angles are not statistically significant anymore. At the age of 10 years, no differences are found, and from 5 to 10 years the difference at mandibular length according to the applied surgical method, as well as the difference at SNA with time, is not statistically significant.
Children born with an isolated cleft palate were examined longitudinally with lateral cephalograms at 5 and 10 years to study the effect of palatoplasties on growth. Conclusions from this study could therefore apply to the same surgical techniques used to close the cleft in the palate in more complex cases including lip and alveolus. Traditional x-ray films were digitized and combined with digital lateral cephalograms. A computerized tracing technique was used as it is less time consuming and equally reliable to hand-tracing as far as cephalometric measurements are concerned (Tsorovas and Karsten, 2010). As the cephalograms were not available for both 5 and 10 years for every child, a mixed model analysis using all the data was additionally used. This could possibly reveal hidden differences in the material. Studying the results, the mixed model analysis was in total agreement and confirmed the 3-way ANOVA test. Consequently, when studying the difference from 5 to 10 years, only 1 of these tests can be used achieving the same results.
Previous studies comparing different surgical techniques for correction of cleft palate, even having differences in material and method (type and time of surgery, surgeon, cleft morphology, age, sex, syndromes, other treatment) could hardly demonstrate differences in craniofacial morphology (Bishara 1974; Bishara et al., 1976; Jonsson and Thilander, 1979; Jacobsson 1990) which seems to be valid also for the 2 examined surgical techniques in this paper. Ross, in 1987, proposed that the surgeon has a greater effect on growth than the applied technique. In our study, during the investigated period there were 3 high-volume surgeons operating 87% of the patients. One of these surgeons was active during the whole period and a shift on the second main surgeon, because of retirement, was performed at almost the same time as the shift of the surgical technique. The rest of the children were operated on by 8 other surgeons with the VWK technique and 2 surgeons with the MI surgical method (Table 1). This might have an influence on the results.
To eliminate the confounding factor “surgeon,” a separate statistical analysis was performed based on the material from the 75 children operated by 1 main surgeon (surgeon A, Table 1). The findings, after correction for multiple testing, were similar to those from the total material with the exception of a new finding at the age of 10 years. At 5 years of age, studying the cleft groups 1 and 2, a significantly shorter mandibular length (P = .049) was found in cleft group 2. This is in agreement with the results from the total material, but its statistical significance is reduced. At the age of 10 years, comparing the surgical technique groups V2 and M2, a statistically significant difference was found for the ANB angle (P = .004) which was smaller in group V2 and is a new finding. From the age of 5 to 10 years, the variables NAPg, palatal plane length, mandibular length, n-sp’/n-gn, and facial convexity were increased and ANB, NSL/ML, sp’-gn/n-gn, and gonial angle were decreased significantly (P < .001), which is in complete agreement with the results from the total material. The analysis from the 75 cases operated by one surgeon has decreased statistical power and should be interpreted as indicative.
No measurement was calculated concerning the width of the cleft, so no evaluation could be performed investigating this important factor. Other unknown reasons, not related to the surgery itself, could lead to small differences among the techniques. Additionally, according to the sample size calculation, a total sample of 128 individuals was needed to perform this study. As mentioned before, because of the limitation of the existing material, the number of children included in the V2 group was small, including registrations from 25 children at 5 years and only 19 children at 10 years of age, so results should be interpreted with caution.
An important factor when evaluating growth from the age of 5 years to that of 10 years is the shift from deciduous to late mixed dentition. Ideally the investigators should be very careful to get data at almost the same chronological time from all groups, as is the case in our study (Table 1). Four main orthodontists were involved in the care of the children, all being part of the Stockholm Craniofacial Team and following the same protocol of the department. Before the age of 10 years, patients received orthodontic treatment for the correction of posterior crossbite (by transversal expansion using mainly a removable plate or rarely a fixed Quad-Helix appliance). Growth could be also influenced by existence of fistulas or an additional operation with pharyngeal flap. In this investigation, 11 cases presented fistulas, more cases belonging to the big cleft group (V1: 2.9%, V2: 16%, M1: 3.3%, M2: 9.3%). Thirty-two children were operated with pharyngeal flaps to improve speech, with an increased demand at group M2 (V1: 11.1%, V2: 20%, M1: 10%, M2: 37.5%).
One of the limitations on evaluating growth through lateral cephalograms is that changes found cannot provide data on transversal growth. Both surgical methods for correction of cleft palate, Veau-Wardill-Kilner and Minimal Incision, as well as both cleft lengths, extension in only soft or both soft and hard palate, seems to produce equal sagittal and vertical results at 5 years and permit similar further growth from 5 to 10 years. The initial hypothesis was accepted, as the differences in facial growth were small between the investigated groups, especially if we consider their clinical significance. This was smaller in comparison with the differences in the transversal dimension found in the study regarding dental occlusion (Karsten et al., 2003), where the results were in advantage for the MI technique. According to Nyberg et al. (1997), speech quality showed no apparent differences between the 2 surgical techniques.
This might raise the question whether the examination including lateral cephalograms at both 5 and 10 years of age is needed to follow growth in children born with isolated cleft palate. The timing for lateral cephalograms to evaluate growth in patients born with an isolated cleft palate can be further discussed. Investigations at complete growth are needed to be able to confirm conclusion about maxillary restriction due to the surgical method used to correct the cleft in the palate. Further studies separating sexes at completed growth, including also a group of nonaffected individuals, are needed to confirm the findings of this article.
Conclusion
The craniofacial cephalometric morphology at 5 and 10 years of age in patients with isolated cleft palate was similar between the VWK technique and the MI technique or cleft length in this study.
At the age of 5 years, a statistically significant shorter mandibular length (P < .01) was found in cleft group 2 for the surgical technique group M. From 5 to 10 years of age, the variables NAPg, palatal plane length, mandibular length, n-sp’/n-gn, and facial convexity were increased and the variables ANB, NSL/ML, sp’-gn/n-gn, and gonial angle were decreased with time.
Footnotes
Authors’ Note
The authors are members of the Stockholm Craniofacial Team.
This paper was presented at the 10th International Congress on Cleft Palate and Related Craniofacial Anomalies, Fortaleza, Brazil, September 2009, and at the 87th Congress of the European Orthodontic Society, Istanbul, Turkey, June 2011.
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.