
Abstract
Cleft lip and palate (CLP) is the most common congenital craniofacial abnormality. Obstructive sleep apnea syndrome (OSAS) is a highly prevalent but underdiagnosed disease and is frequently associated with craniofacial anomalies. There are few studies describing the sleep breathing pattern of children with CLP. This study sought to characterize the respiratory profile of 23 children with unilateral cleft lip and palate, aged 7-12 years, who had undergone cleft lip and nasal repair at age 3-4 months and palatoplasty at 12-15 months, with a particular focus on evaluating the presence of OSAS in children with CLP. Polysomnography was performed and findings were analyzed descriptively. We found a mean and median for apnea/hypopnea index (AHI) of 1.11/h (SD = 0.78) and 0.9/h, respectively. The mean obstructive apnea index (OAI) was 0.27/h (SD = 0.38) and the median, 0.1/h. Nearly 30% of patients had an AHI above 1.4 events/h. There was no significant oxyhemoglobin desaturation in the study group. In this group, the prevalence of OSAS was higher than in noncleft populations when compared to the normality values adopted. This sample of patients with unilateral cleft lip and palate exhibited an increased prevalence of OSAS during the mixed dentition stage. Although the results showed that OSAS was mild, we advise closer observation of these patients. Polysomnography is recommended for the assessment of children with airway abnormalities, to individualize the extent of treatment.
Introduction
Cleft lip and palate (CLP) is the most common craniofacial congenital anomaly, affecting 1 in 500 to 1 in 1000 newborns (Altemus, 1966; Altemus and Ferguson, 1966; Bianchi et al., 2000; Collares, 1990; Fogh-Andersen 1963). The obstructive sleep apnea syndrome (OSAS) is a highly prevalent, yet underdiagnosed, disease (Gislason et al., 1995; Lumeng and Chervin, 2008; Tufik et al., 2010) and is often associated with craniofacial malformations (Lumeng and Chervin, 2008; MacLean et al., 2008; Mossey et al., 2009).
Anatomic modifications in patients with CLP, with consequent alterations of airflow and upper airway size, can lead to an oral or mixed respiratory pattern (Hairfield et al., 1988; Warren et al., 1988a, 1988b).
The American Academy of Pediatrics recommends early diagnosis and treatment of OSAS in children because a delay in identification can lead to permanent cognitive sequelae (Amin et al., 2002; Amin et al., 2005; Blunden et al., 2001; Gozal 1998; Greene and Carroll 1997). The spectrum of sleep-disordered breathing (SDB) ranges from primary snoring, through the upper airway resistance syndrome (UARS), with sleep fragmentation and excessive daytime sleepiness, to the most intense manifestation of these disturbances, which is OSAS (Guilleminault et al., 1976; Marcus, 2001).
OSAS can affect children of any age and lead to serious consequences, including problems at school, behavioral disturbances, and cardiovascular complications (Amin et al. 2002; Amin et al. 2005; Blunden et al., 2001; Lewin et al., 2002; O’Brien et al., 2003; O’Brien et al., 2004; O’Brien et al., 2004). It is difficult to diagnose in children because its signs and symptoms need constant observation, and it is usually underscrutinized by health care professionals (2002; Beck and Marcus, 2009; Brietzke et al., 2004; Kushida et al., 2005). The diagnosis of OSAS is less reliable when it is based on clinical findings alone; polysomnography is required to confirm it (Brietzke et al., 2004). In children and adolescents, the epidemiologic profile, clinical characteristics, and treatment of OSAS are distinct from those in adults with the disorder (Accardo et al., 2010; Anders and Guilleminault, 1976; Fagondes and Moreira, 2010; Grigg-Damberger et al., 2007; Guilleminault and Anders, 1976). Within this context, the present study sought to elucidate the respiratory profile during sleep of a group of children who had undergone primary surgical repair of unilateral cleft lip and palate.
Methods
We studied a group of 23 patients aged 7-12 years who had undergone primary treatment of cleft lip and palate according to our institutional protocol. This group of patients belong to a cohort (n=30) that has been studied (Froés Filho, 2008; Paniagua et al., 2010) since 2001. All cohort patients were invited to participate in the new study. The inclusion criteria were parental consent and agreement to undergo overnight polysomnography (PSG). The exclusion criteria were syndromic CLP, open palate due to complications and failures inherent to palate surgery, inability to undergo PSG, and clear respiratory disturbances manifested while awake during the preoperative period. Seven patients were excluded. All included participants underwent type I overnight polysomnography according to 2007 American Academy of Sleep Medicine (AASM) criteria for this age range: 10-20 system of surface electrodes for electroencephalography (montage: F3/A2, F4/A1, C3/A2, C4/A1, O1/A2, O2/A1) right and left electrooculography (EOG), submental electromyography, airflow sensors (nasal pressure transducer and thermistor), peripheral pulse oximetry (Spo2), thoracic and abdominal respiratory effort measurement (piezo-crystal sensors), snoring sensor, and position sensor (Grigg-Damberger et al., 2007). Sleep and ventilation were spontaneous. All records were obtained using a digital polygraph. Criteria for sleep staging and marking of cardiorespiratory events were based on AASM 2007 Manual rules. An apnea/hypopnea index (AHI) less than 1.4/h was considered normal (Beck and Marcus, 2009). The results obtained were analyzed by descriptive statistics and confronted to the normality values using software SPSS for Windows, version 14.0 (SPSS Inc, Chicago, IL).
All patients underwent noninvasive tests, with prior parental consent obtained through signed informed consent forms that contained detailed information about the procedures. This project was approved by the local research ethics committee with protocol number 09-618.
Results
As shown in Tables 1 and 2, measures of central tendency revealed that respiratory parameters were very close to the average. One patient had an obstructive apnea index (OAI) >1/h (1.6/h). The AHI was average (<1.4/h) in approximately 70% of patients; 7 patients had an AHI >1.4/h, and the highest value found was 2.7/h. Oxyhemoglobin saturation levels during sleep did not exhibit any significant alterations that could be considered pathologic. Only 1 patient had a brief period of oxyhemoglobin saturation in the region of 90%, whereas all other patients had levels higher than 91%. Only 4 patients did not snore. The time lapse to snore onset varied greatly among the 19 patients who did snore (mean, 52.4 minutes; median, 20.2 minutes). The mean total sleep time (TST) was 381.54 minutes, and the shortest recorded TST was 282 minutes. Mean and median sleep efficiency indices were 84.94% and 87.4%, respectively. Sleep structure analysis showed a percentage decrease in REM sleep and a slight decrease in the N3 (slow-wave) stage when group means and medians were considered. More than 60% of patients had normal arousal indexes (mean, 10.64/h; median, 9.2/h).
Descriptive Statistics of Polysomnography Parameters in the Study Group.
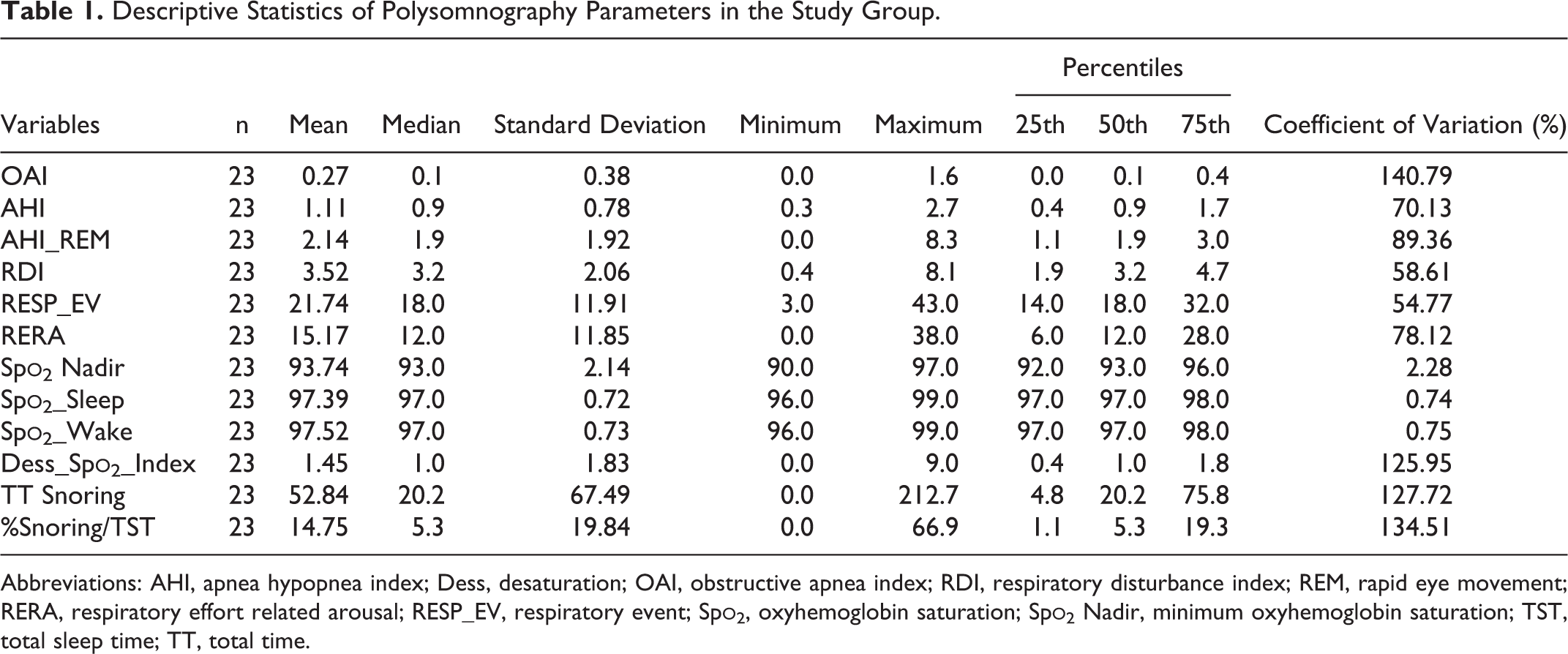
Abbreviations: AHI, apnea hypopnea index; Dess, desaturation; OAI, obstructive apnea index; RDI, respiratory disturbance index; REM, rapid eye movement; RERA, respiratory effort related arousal; RESP_EV, respiratory event; Spo2, oxyhemoglobin saturation; Spo2 Nadir, minimum oxyhemoglobin saturation; TST, total sleep time; TT, total time.
Prevalence Analyses of Patients Above the Cutoff Point for Abnormal Values.
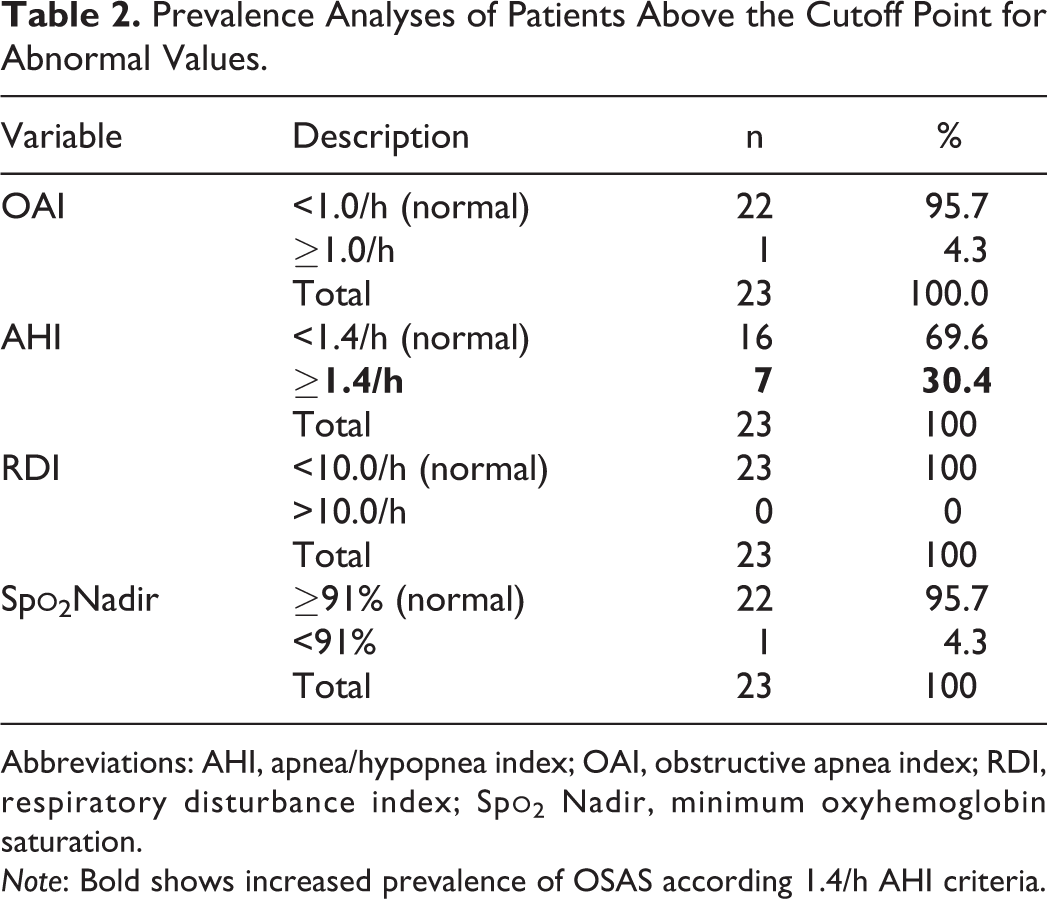
Abbreviations: AHI, apnea/hypopnea index; OAI, obstructive apnea index; RDI, respiratory disturbance index; Spo2 Nadir, minimum oxyhemoglobin saturation.
Note: Bold shows increased prevalence of OSAS according 1.4/h AHI criteria.
Discussion
Few authors have described the relationship between surgical treatment of cleft lip and palate and presence of respiratory disturbances. Consistent with our results and in an analysis of a similar group, Rose et al. (2002), studying 43 children with CLP aged 12.11 (SD = 3.8) years, found a higher incidence of microsymptoms of nocturnal respiratory obstruction when compared to a group matched by age, gender, and BMI index. Furthermore, the absence of oxyhemoglobin desaturations and little disruption of sleep architecture indicates a mild OSAS profile in CLP populations.
Liao et al. (2002), in a prospective study, found a high incidence of OSAS in CLP patients who had undergone pharyngeal flap correction of velopharyngeal insufficiency. More than 90% of these individuals (10 adults and 28 children) had SDB, as evaluated through polysomnography 6 months after surgery.
Liao et al. (2003) found transient SDB and a 10% OSAS prevalence in a group of 10 patients after palatoplasty with Furlow’s technique. This prevalence is lower than that found in our sample. However, Liao evaluated only 10 patients, and polysomnography was performed using temperature sensors, which can underestimate the respiratory disturbance because of poor detection of partial obstructive events.
In 1996, Josephson et al. published 2 case reports of patients who developed sleep apnea after closure of unilateral lip cleft and later improved after correction of septal deformity.
Muntz et al. (2008) retrospectively analyzed 539 children with syndromic and nonsyndromic clefts. Twenty-two percent exhibited symptoms suggestive of SDB. Syndromic children had a significantly higher rate of SDB symptoms (34% vs 17%, P < .001). The author concludes that the incidence of OSAS is high in the CLP population and that this syndrome is underdiagnosed. Muntz et al. suggest that polysomnography be recommended more frequently for postoperative follow-up.
In 2008, Maclean et al. corroborated the finding of high OSAS prevalence in the CLP population and called for prospective studies to better characterize hazards and major risk factors. The same author conducted a study exploring the prevalence and distribution of OSAS symptoms in patients with cleft palate using questionnaire data alone (no PSG was performed). OSAS was identified in 31.4% of patients with a mean age of 33.4 months. Children with cleft palate had a fivefold higher risk of OSAS. Unlike our group, the Maclean cohort also included syndromic children with craniofacial alterations such as the Pierre Robin sequence, which had a direct impact on worsening of respiratory parameters and increased the odds of OSAS. We also found a 30% prevalence of OSAS when an AHI >1.4/h was considered (Beck and Marcus, 2009), although no patient exhibited an respiratory disturbance index (RDI) >10/h, which is the assumed limit of normal; however, this parameter is only valid for adults, and no equivalent, valid pediatric parameters have been described to date. As only 2 patients presented central events (one event per child) and apnea index (AI) ≈ OAI and AHI ≈ OAHI, here we used OAI and AHI. The mean Spo2 nadir was 93.74 (SD=2.74), and only 1 patient exhibited oxyhemoglobin saturation below 91%, in a single event. This is indicative of a normal oxyhemoglobin saturation profile in this population. Whether the presence of obstructive events alone without desaturation leads to significant morbidity in children remains unclear (Poets et al., 1993).
More studies are needed to further discern the cause and behavior of OSAS in this patient population. The use of matched control groups, bigger series, and long-term follow-up will improve the strength of this information. Adequate monitoring and constant observation of these patients is imperative to OSAS diagnose. Polysomnographic data are very important for immediate diagnosis and long-term follow up. When OSAS is identified, treatment should be instituted immediately to prevent potentially fatal symptoms associated with this condition.
Conclusion
Patients with unilateral cleft lip and palate have an increased prevalence of OSAS during the mixed dentition stage. Although the results of this study showed OSAS prevalence to be low and of mild severity, we recommend close observation of these patients, individualizing the extent of airway obstruction treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.