
Abstract
Objective:
In wide palatal defects, closure of the nasal layer can prove a considerable challenge. Mobilizing nasal flaps posteriorly usually facilitates soft palate closure. However, the defect is often too wide within the hard palate; hence, bilateral vomerine flaps are frequently required. Despite this, there is often a small defect in the nasal layer at the posterior septum (typically equating to the hard-soft palate junction), which has to be left to heal by secondary intention with the resulting increased risk of fistula formation and the potential deleterious long-term effect on speech due to cicatricial migration of the reconstructed levator sling anteriorly. We describe our experience in the use of the sphenoid flap to obtain tension-free primary closure of the nasal layer.
Methods:
A retrospective multi-center study assessing all sphenoid flap procedures undertaken at both Birmingham Children’s Hospital and Great Ormond Street Hospital. Key demographic and medical data was collected pre-, peri-, and postoperatively across the 2 sites.
Results:
A total of 66 patients underwent the use of a sphenoid flap to aid closure of the nasal layer. The average age at time of repair was 9.7 months. More than half (55%, n = 36) were isolated cleft palates, and 35% (n = 23) were BCLPs. Forty-two percent of all patients had Robin sequence. The average cleft width was 14.4 mm. The overall fistula rate was 25.8% (n = 17).
Conclusions:
We describe the operative technique, indications, and our experience in the use of the sphenoid flap in wide cleft palate repair.
Introduction
Closure of a wide cleft palate presents a considerable operative challenge. Commonly employed surgical techniques include extended Von Langenbeck releasing incisions for the oral layer and unilateral or bilateral vomerine flaps to facilitate closure of the nasal layer. However, despite the use of vomerine flaps, there often remains an inevitable small defect under tension at the posterior limit of the septum that typically equates to the hard-soft palate junction. This nasal layer defect is therefore left to heal by secondary intention that can result in 2 problems. First, as this area heals by contracture, there may be cicatricial migration of the reconstructed levator sling anteriorly leading to a potential negative long-term effect on speech. Second, there is a high risk of fistula formation and the subsequent morbidity that this may cause.
A recent meta-analysis of fistula incidence in 9294 cleft palate repairs from 44 worldwide studies reported the only variable that had a significant effect on postoperative oronasal fistula formation was the initial width of the palatal defect: the overall fistula incidence of 8.9% rose to 17.9% in wider clefts (Hardwicke et al., 2014). Similar outcomes have been reported from other studies examining fistula rates after repair of wide palatal clefts. Parwaz et al. (2009) demonstrated this to be a statistically significant predictor of oronasal fistula formation: in 7 cases that had a wide cleft (measured as >15 mm), 5 developed fistulae (71%). Landheer et al. (2010) reported a significantly increased risk of fistula formation with cleft width of ≥13 mm (P = .04) in a study examining 275 patients undergoing cleft palate repair. The UK Bilateral Cleft Lip and Palate (BCLP) Audit, which examined a cohort of patients that by definition would have a wider palatal defect reported a fistula rate of 51% from the 71 patients included in the study (Thomas et al., 2011).
In an attempt to address the apparent higher rate of fistula formation in wide cleft palate repair, the “sphenoid flap” was developed at Birmingham Children’s Hospital to allow for an improved tension-free closure of the nasal layer. The sphenoid flap is a pedicled extension of the vomerine flap that is based on the right or left side and named due to the area of underlying bone from which it is raised. There have been isolated previous descriptions in the literature of using an extended vomerine flap (Hodges, 2010; Kobus, 1984), and the sphenoid flap is an extension of the same principle. We present the operative technique and our initial experience in the use of sphenoid flap in wide cleft palate repair.
Materials and Methods
Operative Technique
All patients were appropriately consented for the procedure. At the time of cleft palate repair, an intraoperative decision is made to use the sphenoid flap based upon the width of the palatal cleft, the width of palatal shelves, and the general tissue quality and anatomy of the cleft. The sphenoid flap is marked with methylene blue ink (Figure 1). The flap is a continuation of the vomerine flap posteriorly and can be pedicled on either the right or left side depending upon local anatomy and any previous surgery. The posterior extent is the commencement of adenoidal tissue. The area is infiltrated with local anesthetic (lignocaine or bupivacaine titrated to patient weight in kilograms) with adrenaline for hemostatic effect, hydro-dissection, and postoperative analgesia. The incision begins at the vomerine process anteriorly, extending posteriorly to raise the flap in the subperiosteal plane, back cutting as necessary to allow tension-free mobility (Figure 2 and Video 1 demonstrating maneuverability and vascularity of raised sphenoid flap). All bleeding areas are cauterized as required. The nasal mucosa is then dissected free from the cleft margin per standard technique for cleft palate closure. The soft palate nasal mucosa is closed from posterior to anterior until undue tension is encountered. The closure then proceeds from anterior (incisive foramen) to posterior, approximating the vomerine flap(s) to the nasal mucosa unilaterally or bilaterally and continuing to inset the sphenoid flap tension free into the V-shaped defect that is commonly encountered (see Figures 3, 4, and Video 2 demonstrating tension-free inset of flap). Sutures are tied on the nasal side of the mucosa. Following tension-free nasal mucosa closure using the sphenoid flap, intravelar veloplasty is performed followed by closure of the oral layer mucoperiosteal flaps and/or use of Von Langenbeck releasing incisions.
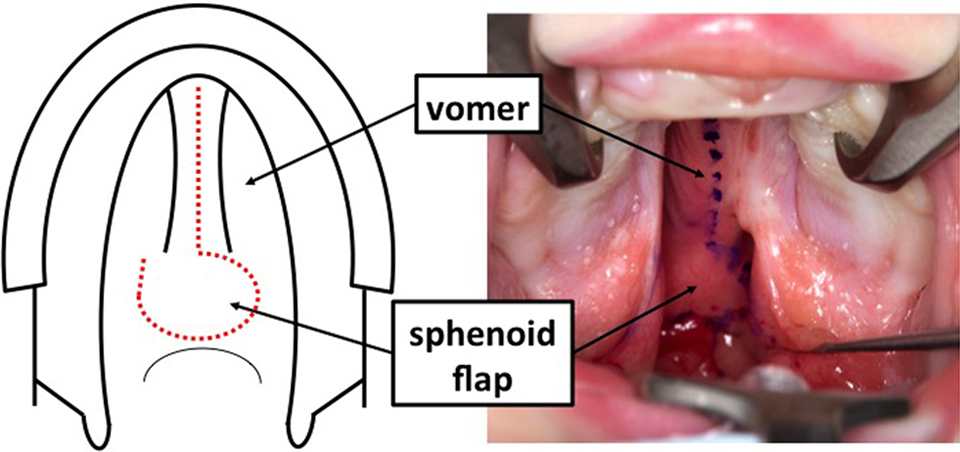
Diagrammatic representation of sphenoid flap (left side, marked with red dotted line) and intraoperative view (right side, marked with blue ink) prior to dissection in a patient with Robin sequence undergoing cleft palate repair.
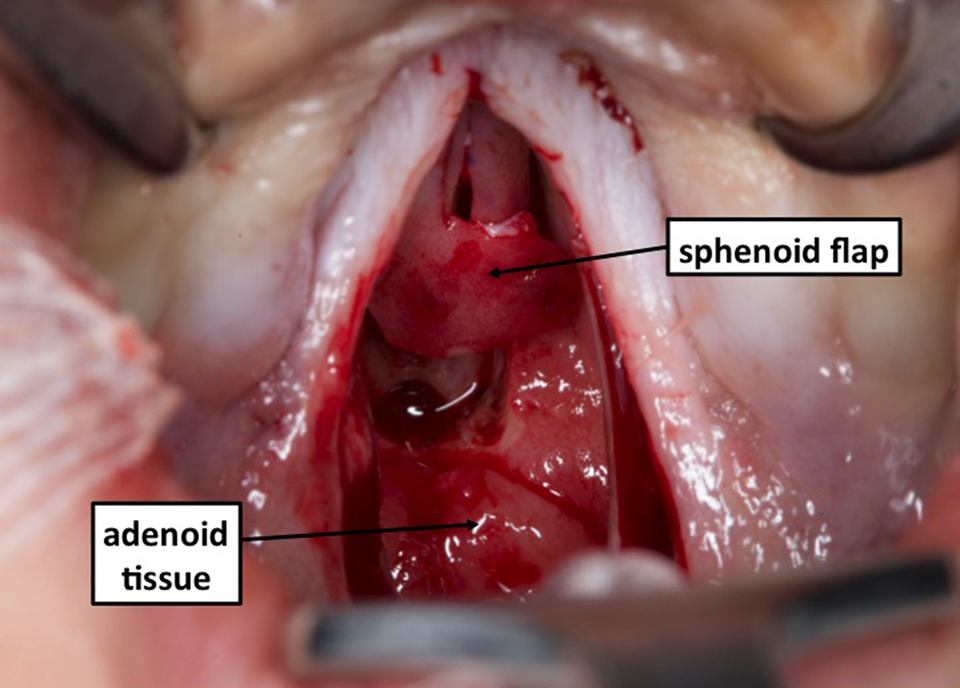
Sphenoid flap raised prior to inset in nasal layer closure.
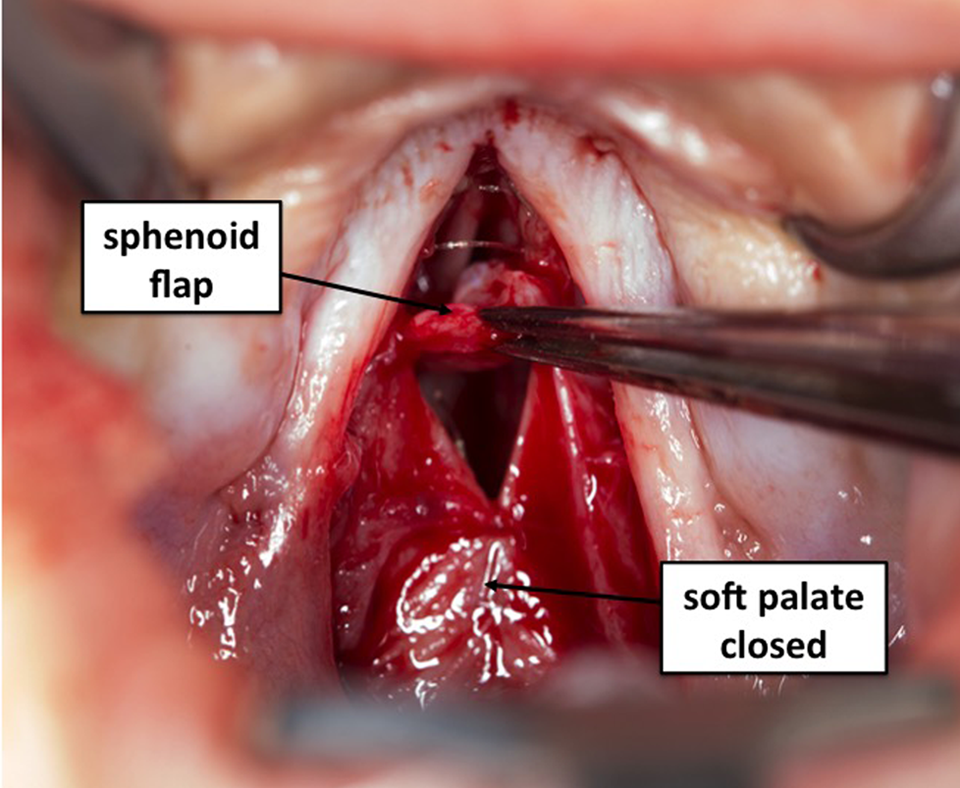
Sphenoid flap being rotated into the V-shaped defect in nasal layer closure typically encountered during wide cleft palate repair. The nasal layer has already been closed anteriorly with bilateral vomerine flaps and posteriorly with direct closure at the level of the soft palate.
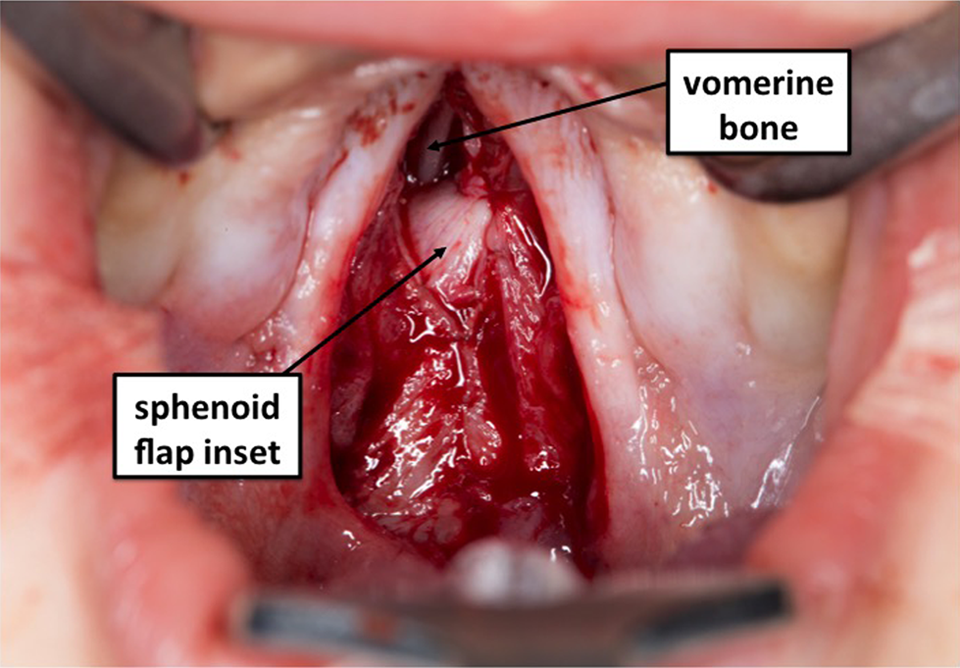
Sphenoid flap fully inset.
In cases where use of the sphenoid flap is not immediately apparent, dissection will begin with freeing the nasal mucosa from the cleft margin and attempting direct closure: if undue tension is encountered, then the sphenoid flap can be raised secondarily in continuation with the vomerine flap.
Patient Selection
All patients that underwent a cleft palate repair using a sphenoid flap to assist in closure of the nasal mucosa at Birmingham Children’s Hospital (Birmingham, UK) and Great Ormond Street Hospital (London, UK) were retrospectively identified over a 10.5-year period between January 1, 2004, and June 31, 2014. The study was approved by at both hospital sites by the respective institutional review boards, and informed consent was obtained. Data were collected for patient demographics, peri- and postoperative findings and outcomes, and any complications. Numerical data are presented as the mean ± standard deviation or range. Statistical analyses were performed using Fisher test.
Results
A total of 66 patients underwent repair of the nasal layer of the palatal cleft using a sphenoid flap. The mean age at time of primary cleft palate repair was 9.7 months (range 5.8 months–4.3 years). With the outlier removed (4.3 years old, delayed presentation), the mean age at repair was 9.2 months (±3.7 months).
The mean cleft width (measured at the maxillary tuberosity intraoperatively) was 14.4 mm (range 9-23 mm). In 12 patients, the cleft width had not been recorded intraoperatively, but only subjectively described as “wide.” More than half of the patients (n = 36, 55%) included in this study were isolated cleft palates, with a further 23 bilateral cleft lip and palates (BCLP, 35%) (Figure 5). The mean length of postoperative follow-up was 2.6 years (range 2.0-9.3 years). Nearly half (n = 28, 42%) of all patients undergoing sphenoid flap closure had a diagnosis of Robin Sequence. Other known diagnosed syndromes at the time of palate repair included Van der Woude (n = 2), SHOX deletion (n = 1), Emmanuel syndrome (n = 1), and Stickler syndrome (n = 1).
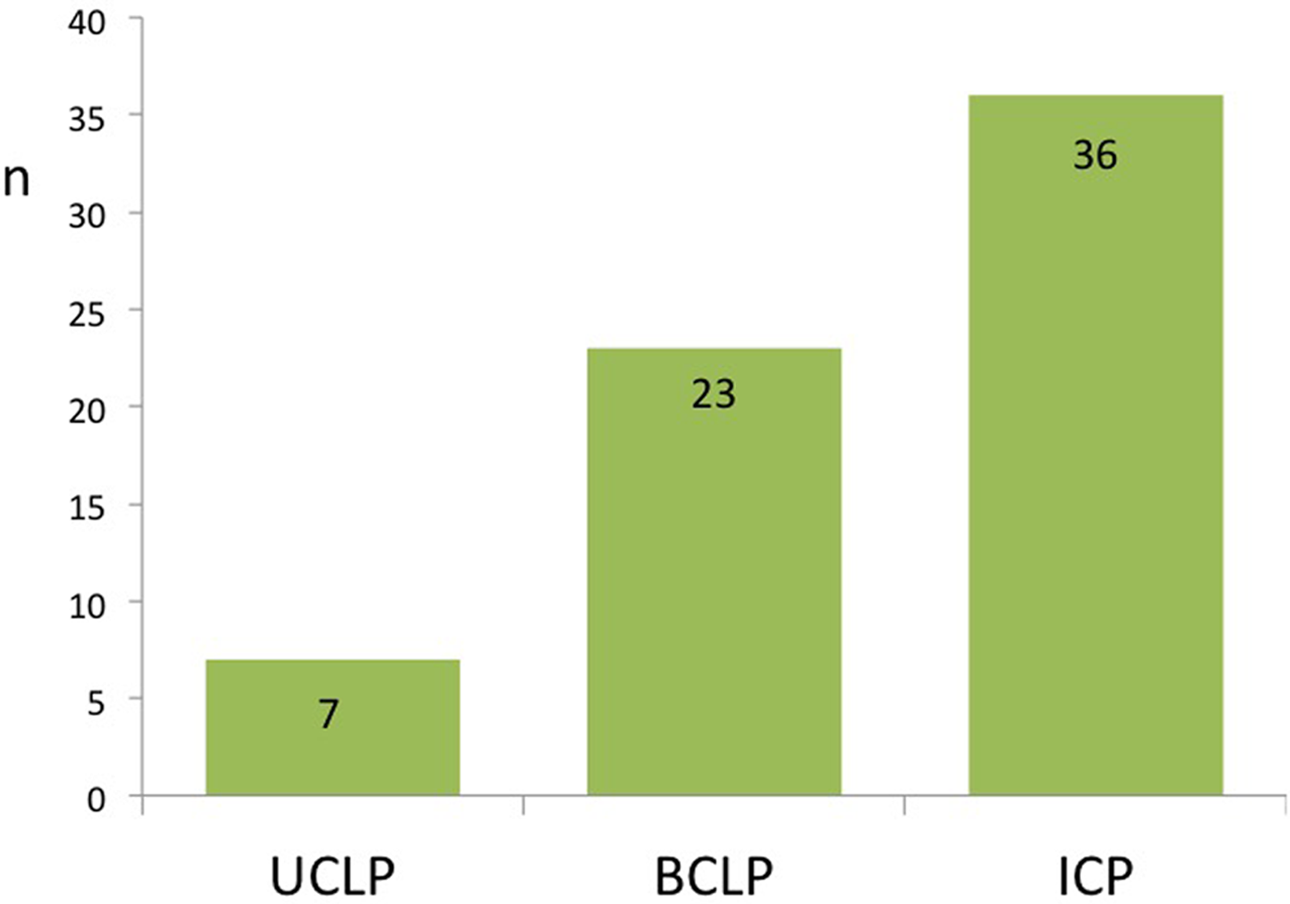
Use of sphenoid flap by primary cleft pathology. BCLP, bilateral cleft lip and palate; ICP, isolated cleft palate; UCLP, unilateral cleft lip and palate.
The overall fistula rate was 25.8% (n = 17). Eleven of these patients underwent further surgery for symptomatic fistula repair during the follow-up period of this study. Examining the BCLP’s alone (n = 23), a total of 30.4% (n = 7) were found to have a fistula at follow-up.
The use of releasing incisions to assist in closure of the oral layer mucoperiosteal flaps was required bilaterally in two-thirds of cases (n = 45, 68.2%) and unilaterally in 2 cases (3.0%). Five patients underwent secondary palatal rerepair procedures for speech. There were no other significant intraoperative or postoperative complications: specifically, no recorded use of nasopharyngeal airway devices or bleeding-related morbidity.
Discussion
This paper reports our experience with an operative technique that facilitates repair of wide palatal clefts. When closing a wide palatal defect, closure of the nasal layer can be extremely challenging. The use of the sphenoid flap provides a tension-free approximation of the nasal layer in an otherwise difficult area to close. In this multicenter case series of 66 patients who underwent wide cleft palate repair using a sphenoid flap, we report an overall fistula rate of 25.8%. This rate is higher than the published overall fistula rates in the literature (Bykowski et al., 2015; Hardwicke et al., 2014); however, this particular cohort of patients had by definition a wide cleft palate (mean width 14.4 mm, range 9-23 mm), making them a higher than average risk group for fistula formation. Reviewing the literature for wide palatal clefts alone is difficult as the width is often not reported and these are heterogeneous populations.
Previous studies examining outcomes specifically after wide cleft palate repair report fistula rates ranging from 51% to 71% (Parwaz et al., 2009; Thomas et al., 2011). In this study, the use of the sphenoid flap in wide cleft palate repair has demonstrated a lower fistula rate of 25.8% (P = .051 when compared to the UK BCLP Study Group population). When comparing just BCLP patients with wide cleft palates who underwent use of the sphenoid flap (n = 23) we report a fistula rate of 30.4% (n = 7). This is again much lower than the UK BCLP Study (2011), which reported a fistula rate of 51% (n = 36) in 71 BCLP patients, but is not a statistically significant difference (P = .21). Alternative options to assist in the closure for wide palatal clefts include using interpositional materials such as acellular dermal matrix to augment the repair (Aldekhayel et al., 2012), and/or staged closure of the palate. However, a staged palatal closure means a guaranteed further general anesthetic and the morbidity that may result from this, and in addition Landheer et al. surprisingly reported in a comparison of 154 two-stage repairs versus 121 one-stage repairs a fistula rate of 27% versus 14%, respectively (P = .08) (Landheer et al., 2010).
The authors routinely use the sphenoid flap if the cleft palate width is >15 mm measured at the maxillary tuberosity. It is generally accepted that a wide cleft palate is classified as greater than 15 mm. However, as stated previously, the mean cleft width in this study was 14.4 mm (range 9-23 mm), indicating that the use of the sphenoid flap was not simply based upon a numerical measurement. Rather, the sphenoid flap was employed by the operating surgeon based on intraoperative findings, which would typically include an assessment of the width of the palate, the width of the palatal shelves, the local anatomy of the vomer and sphenoidal area, the tension in the nasal layer, and the general tissue quality. Though this means that the use of the flap was in some cases subjective, a notable advantage of the sphenoid flap is that it can be raised as an extension of the vomerine flap later on in the dissection if the operating surgeon encounters unanticipated difficulty in closing the nasal layer.
In 12 patients included in this study, the cleft width had not been recorded intraoperatively, but only subjectively described as “wide.” Of these 12 patients, 25% (n = 3) went on to develop fistulae. When this subgroup is excluded from the overall analysis, the fistula rate is 25.9% (14 fistulas in 54 patients). As this value is almost identical to the overall fistula rate found among all 66 patients (25.8%, not statistically different), we do not believe this to be a significant source of bias.
Use of the sphenoid flap reduces the surface area left to heal by secondary intention within a cleft palate repair. This in theory should result in a reduction in overall scarring and scar contracture within the healing palate and hence less cicatricial migration of the reconstructed levator sling and improved motility. Furthermore, the inset of the sphenoid flap could in theory act to splint the soft palate in a more superior position, further optimizing speech production. The cohort of patients in the current study are still too young for formal speech evaluation (at age 5 years using Cleft Audit Protocol for Speech Augmented [CAPS-A] per UK Cleft Care guidelines) (Jones et al., 2014); however, we would anticipate an improvement in outcome though comparison to a suitable similar matched cohort of wide cleft palate patients may prove difficult.
In the results from this study, no significant additional morbidity was encountered intra- or postoperatively with the routine use of the sphenoid flap in wide cleft palate repair. As it is a pedicled continuation of what would otherwise be routinely used as a vomerine flap, it added minimal additional operating time and has been relatively straightforward to teach and learn. We would however caution its use in cases where additional pathology may be involving the skull base such as encephalocele or when holoprosencephaly may be suspected, and would recommend either digital palpation of the sphenoidal area prior to raising the flap (alternatively, one can use the hypodermic needle at the time of local anesthetic infiltration to evaluate the area).
In our experience, the sphenoid flap is a useful adjunct that can be employed where necessary in repair of the wide cleft palate. The flap is straightforward to raise and inset and causes little to no additional morbidity.
Footnotes
Author Note
This study was presented orally at the Annual Craniofacial Society of Great Britain & Ireland (CFSGBI) Meeting, Nottingham, United Kingdom, April 2016.
Acknowledgments
With thanks to Mr Sandy McKee and Ms Stephanie Rowe, Medical Photography Department, Birmingham Children’s Hospital, Birmingham, United Kingdom.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.