
Abstract
Objective:
We highlight a major study that investigated the impact of reconfigured cleft care in the United Kingdom some 15 years after centralization. We argue that centralization as an intervention has a major impact on outcomes.
Setting:
Audit clinics held in Cleft Centers in the United Kingdom.
Patients, Participants:
Five-year-olds born between April 1, 2005, and March 31, 2007, with nonsyndromic unilateral cleft lip and palate.
Interventions:
Centralization of cleft care.
Main Outcome Measure(s):
We collected routine clinical measures (speech recordings, hearing, photographs, models, oral health, psychosocial factors) in a very similar way to a previous survey.
Results:
We identified 359 eligible children and recruited 268 (74.7%) to the study. Overall, their outcomes were better post-centralization. There have been marked improvements in dentoalveolar arch relationships and in speech whereas the prevalence of dental caries and hearing loss are unchanged.
Conclusions:
Centralized cleft care has changed UK outcomes considerably and there is no argument for returning to a dispersed model of treatment.
In this brief article, we highlight the impact of changes in United Kingdom cleft services over a 15-year period. In 1996, we collected data that informed the Clinical Standards Advisory Group (CSAG) report published in 1998 (CSAG, 1998). The organization and outcomes of cleft care across the United Kingdom at that time were described in a series of publications (Bearn et al., 2001; Sandy et al., 2001; Sell et al., 2001; Williams et al., 2001). Subsequently the government acted to centralize cleft care by reducing the 57 cleft units down to 8 to 15 centers (Sandy et al., 2012). We now highlight a repeat of this study (called Cleft Care UK [CCUK]) which has had an impact on outcomes for these children.
Treatment for children with cleft lip and palate in the United Kingdom is now provided through interdisciplinary teams in 11 centers or managed clinical networks. Surgeons in these teams operate on at least 35 cases each year (Fitzsimons et al., 2012; Scott et al., 2014; Scott et al., 2015). The process of centralization of care was variable in relation to speed and implementation, with not all teams having essential team members or facilities immediately available (Scott et al., 2014). Some teams, following the recommendations of CSAG, were able to very rapidly change their personnel and structures, as well as addressing shortfalls in staffing. This was not true for all of these teams, and since the initial centralization, with increasing financial pressures some centers have found it difficult to maintain staffing. The other challenges were in reducing the number of centers and clinicians involved in cleft care (Sandy et al., 2012). Training of surgeons was also an issue (Bearn et al., 2001), and through the Royal Colleges of Surgeons, the Training Interface Group, comprising Oral and Maxillofacial Surgery, Otolaryngology and Plastic Surgery, recognized a number of national advanced training posts in cleft surgery. These posts are open to trainees of these 3 specialties for the last 2 years of their training. Despite these variations and perturbations, there have been major changes in the way that care is provided in the United Kingdom and this centralized interdisciplinary model is effective with demonstrable improvements in outcome 15 years after centralization took place.
To examine the impact of this change, we conducted a United Kingdom – wide cross-sectional survey (CCUK) of 5-year-old children with unilateral cleft lip and palate (UCLP), between January 2011 and December 2012 (Al-Ghatam et al., 2015; Ness et al., 2015; Persson et al., 2015; Sell et al., 2015; Smallridge et al., 2015; Waylen et al., 2015). We based the study design on the original survey. CCUK followed principles outlined in the Declaration of Helsinki with ethical approval from the Local Institutional Review Board (REC reference number: 10/H0107/33, South West 5 REC) and appropriate informed consent from participants. There were some differences in the studies despite trying to use the same methodologies, but we believe that these studies were similar enough to allow us to evaluate the impact of the centralized interdisciplinary service (Persson et al., 2015).
We have now reported the results of this nationwide survey and compared these with the results of the previous survey. Table 1 summarizes the study demographics and outcomes. There were differences in practice between the 2 surveys with less variation in the types of surgical procedures used, more frequent treatment of dental caries, more hearing aids used, and fewer grommets placed. Overall the treatment outcomes were better, with the most obvious improvements in speech (Sell et al., 2015) and dentoalveolar relationships (Al-Ghatam et al., 2015). Fewer parents in CCUK perceived their children as having poor self-confidence than in the previous study. At least 81% of parents reported that they were happy with their child’s facial features after surgery and parental satisfaction with service was high. Interestingly, families did not report that it was any more difficult to attend the cleft center despite inevitable increased distances to travel when care is centralized (Waylen et al., 2015). The reason for this is that many of the repeat visits for care (orthodontics, dentistry, speech and language therapy) are delivered locally and the central clinics are very focused and decisive on future care pathways. However, not all outcomes improved, the prevalence of dental caries and hearing loss were unchanged (Smallridge et al., 2015). Furthermore, a proportion of children (approximately 20%) still have difficulties with speech and poor dentoalveolar relations. So further service improvements are required if the United Kingdom is to achieve outcomes similar to those reported from the best European centers (Lilja et al., 2006; Lohmander, 2011; Sinko et al., 2008).
Comparison of Demographics and Outcomes Between the Cleft Care UK Study (CCUK, 2015) and the Clinical Standards Advisory Group study (CSAG, 1998).a
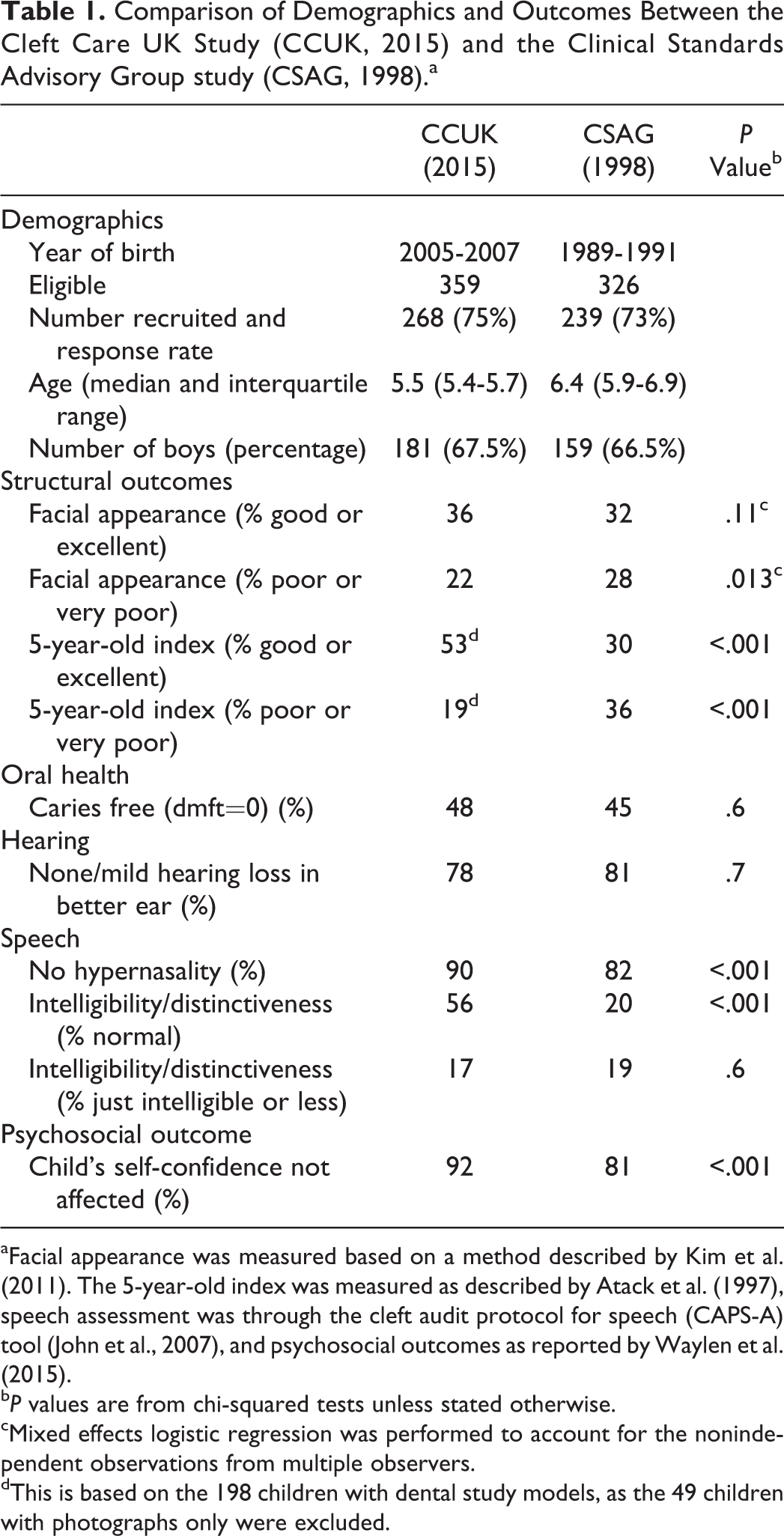
aFacial appearance was measured based on a method described by Kim et al. (2011). The 5-year-old index was measured as described by Atack et al. (1997), speech assessment was through the cleft audit protocol for speech (CAPS-A) tool (John et al., 2007), and psychosocial outcomes as reported by Waylen et al. (2015).
b P values are from chi-squared tests unless stated otherwise.
cMixed effects logistic regression was performed to account for the nonindependent observations from multiple observers.
dThis is based on the 198 children with dental study models, as the 49 children with photographs only were excluded.
In the United Kingdom, outcomes for children born with a cleft have improved as a result of the introduction of a centralized interdisciplinary service. These improvements probably reflect a combination of better surgical training, increased number of surgical procedures per surgeon with the elimination of low volume operators (Fitzsimons et al., 2012; Scott et al., 2014; Scott et al., 2015), an investment in support staff including clinical nurse specialists, clinical psychologists and specialist speech and language therapists, and the implementation of interdisciplinary team working. The relative importance of these factors needs clarification but this is not a reason to delay rationalizing services. We believe that the argument for a dispersed model of care is no longer tenable and that centralization should now be introduced in other countries. We would further argue that local comprehensive surveys are not required to justify or guide this change. Establishing base levels of outcomes before centralization will delay, unnecessarily, the improvements that these children and their families can and should expect. Thereafter comprehensive national surveys that describe care and outcomes are needed to refine and monitor service improvements. These surveys can also help build research expertise and understanding in cleft teams. A research-led evidence-based (centralized) service for children born with cleft lip and palate will not only offer better care but the infrastructure to conduct much needed adequately powered trials and robust serial cross-sectional and longitudinal studies.
Footnotes
Author Note
This publication presents independent research commissioned by the UK National Institute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (RPPG-0707-10034). The views expressed in this publication are those of the author(s) and not necessarily those of the National Health Scheme, the NIHR, or the Department of Health.
Acknowledgment
We would like to thank the families that took part in this study. We would also like to thank the clinicians and staff in the cleft centers that supported this project.
This research was grant funded by the NIHR.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.