
Abstract
Objective:
To examine the reciprocal relationships between parenting stress and psychosocial adjustment of children with congenital craniofacial anomalies (CFAs) at 2 time points: school entry and approximately 2.5 years later, after children had time to adjust to school.
Design:
Retrospective review of medical charts of children with CFAs.
Setting:
Department of reconstructive plastic surgery at an urban medical center.
Participants:
Parents of 42 children aged 3.9 to 6.5 years at time 1 and 6.5 and 9.8 years at time 2.
Main Outcome Measures:
Parenting Stress Index/Short Form and Child Behavior Checklist (CBCL), both completed by parents at time 1 and time 2.
Results:
Compared to norms, more parents scored in the clinical range on parenting stress both at time 1 and time 2. Parenting stress remained stable across the 2 time points. Although rates of psychosocial problems for boys were comparable to those of the CBCL normative sample, higher-than-expected rates of clinically significant internalizing and externalizing were found for girls at time 2. Parenting stress at time 1 was associated with child internalizing and externalizing problems at time 2. Whereas child externalizing problems at time 1 predicted parenting stress at time 2, child internalizing at time 1 showed trivial effects on time 2 parenting stress.
Conclusions:
Early school years may be a period that is particularly stressful for parents of children with CFAs. There appears to be a transactional relationship between parenting stress and child psychosocial adjustment during the early school years.
Although most children with congenital craniofacial anomalies (CFAs) do not have significant psychopathology (Hunt et al., 2005; Cloonan et al., 2013; ), there is evidence that this population has increased risk for social deficits and attention problems (Pope and Snyder, 2005). Internalizing problems, such as depression, anxiety, and withdrawal, also afflict children in this population at above-average rates (Hunt et al., 2005; Brand et al., 2009; Murray et al., 2009).
Parents of children with congenital CFAs face considerable challenges. They may question why this happened to them and their child, and they may feel grief, disappointment, or guilt (Pope, 1999; Nelson et al., 2011 ). Parents in this population may feel distressed about their child’s atypical appearance and about functional differences affecting their child’s feeding, smiling, cooing, or vocalizing (Endriga and Speltz, 1997; Pope et al., 2005; Despars et al., 2011; ). These caregivers typically contend with multiple surgeries and postsurgical care involved in treating the child, a range of specialty and ancillary care services, the financial cost of this medical care, and a concern about future medical care or developmental problems (Krueckeberg and Kapp-Simon, 1993; Pope, 1999; Gray et al., 2015).
Given the challenges they face, parents in this population may experience increased stress related to their role as caregivers. Parenting stress arises when an individual perceives a discrepancy between the demands of parenting and the resources available to address the demands (Spinelli et al., 2013). All parents experience parenting stress to some degree (Deater-Deckard, 1998); however, challenging life events may lead to an increase in the discrepancy between demands and available resources, and this has been shown to exacerbate parenting stress (Östberg and Hagekull, 2000). According to Abidin’s (1990) conceptualization, parenting stress stems from both child and parent characteristics. That is, parenting stress may arise due to caregivers’ perception of the child as being difficult to parent or due to concerns about their own deficiencies in the parenting role (Spinelli et al 2013). The literature thus far has yielded mixed results about whether caregivers of children with CFAs do, indeed, experience greater levels of stress than those of unaffected children. Whereas some studies have found that, relative to norms, parents of children with CFAs experience elevated levels of stress (Speltz et al., 1990; Pope et al., 2005; ), others have not found these effects (Krueckeberg and Kapp-Simon, 1993; Cloonan et al., 2013; Gray et al., 2015). The mixed findings may indicate that caregivers of children with CFAs vary widely in their experience of stress.
It is critical to understand parental stress because it has the potential to impair the quality of caregiving. Experiencing stress, especially early in the child’s life, may compromise the ability to be sensitive and responsive to the child (Endriga and Kapp-Simon, 1999); high sensitivity and responsiveness have been associated not only with positive parent–child attachment (Ainsworth et al., 1978) but also with the child’s adaptive development of emotion regulation and the child’s future psychological adjustment (Eisenberg et al., 1998; Endriga and Kapp-Simon, 1999; Pope, 1999). A stressed parent of a child with a CFA may have decreased responsiveness to her child, as she may be less available (physically or emotionally) during medical and postmedical care, may have trouble recognizing the child’s emotional cues due to facial disfigurement, or may be generally emotionally depleted (Field and Vega-Lahr, 1984; Krueckeberg and Kapp-Simon, 1993; Speltz et al., 1994).
Parental stress has been demonstrated to be a powerful predictor of children’s later psychosocial functioning, both for typically developing children (Anthony et al., 2005; Barry et al., 2005; Crnic et al., 2005; Stadelmann et al., 2015) and for pediatric samples (Mullins et al., 2004; Colletti et al., 2008), including samples of children with CFAs (Goldberg et al., 1997; Pope et al., 2005). Among caregivers of children with CFAs, parenting stress sustained throughout the period of infancy into toddlerhood was found to be associated with increased child internalizing and externalizing behavior problems (Pope et al., 2005). Although parenting stress occurring later than toddlerhood theoretically has a similar potential to obstruct responsiveness and detract from adaptive parenting, there is limited research exploring the ways in which parenting stress experienced in the school years affects the psychological adjustment of children with CFAs.
Parental stress fluctuates in relation to the child’s stage in development and the environmental demands placed on the child and parents (Baker et al., 2003). When children begin school, caregivers may experience increased stress, as their children are contending with new developmental demands, including increased autonomy, academic expectations, and peer interactions. School entry is an important developmental task for all children, with a complex set of challenges, including formation of positive attitudes toward school and development of positive relationships with peers and teachers; a successful transition to school is a precursor to academic success and positive social and psychological functioning (Ladd, 2009). Given that children with CFAs are at increased risk of cognitive and social problems (Broder et al., 1998; Hunt et al., 2005; Pope and Snyder, 2005; Collett et al., 2014; Knight et al., 2015; ), concerns about learning disabilities and positive peer socialization may be a significant source of stress for parents in this population whose children are first entering school (Gray et al., 2015). Parents of children with CFAs may be especially worried at this juncture about how their child will be perceived by peers, teachers, or even other caregivers (Pope, 1999; Zeytinoglu and Davey, 2012), resulting in elevated levels of parental stress.
Although parenting behavior is predictive of child adjustment, child adjustment also influences parenting, with reciprocal influences over time (Bornstein, 2002; Neece et al., 2012). Child problem behavior can increase parenting stress, disrupting the quality of caregiving and further exacerbating child problems (Hastings, 2002; Zaidman-Zait et al., 2014). Therefore, it is important for studies examining links between parenting stress and child adjustment to consider bidirectional models of effect using longitudinal designs.
Given the dearth of information on parenting stress occurring after toddlerhood in the CFA population, the goal of the current study was to evaluate whether parents experience elevated levels of stress at school entry and whether that parenting stress has longitudinal associations with child adjustment. We examined parental stress and child psychosocial adjustment at 2 time points, at school entry (time 1; school entry) and 2.5 years later, after children had time to adjust to the academic and social demands of school (time 2; postentry). First, we hypothesized that caregivers would report higher levels of parenting stress at time 1 than at time 2, reflecting the expected heightened concerns at school entry. Second, we hypothesized that across both time points, caregivers in our study would report more clinically elevated levels of stress than those in the Parenting Stress Index/Short Form (PSI/SF; Abidin, 1990) standardization sample. Third, we hypothesized that (1) elevated stress levels reported by parents at time 1 would predict elevated child psychosocial problems at time 2 and (2) elevated psychosocial problems at time 1 would predict elevated parental stress at time 2, given the transactional nature of the parent–child relationship.
Methodological decisions were made to favor external validity. The sample contained a wide range of CFA diagnoses; our interest was in understanding general trends across this broad patient population rather than isolating the impact of more limited, specific factors (eg, timing of surgery, type of facial difference). Similarly, we selected a relatively wide range of ages for our school entry group, given our understanding that entry to schooling can involve a lengthy process of anticipation and preparation prior to starting school (Pope, 1999). As the typical age of entry into formal schooling (kindergarten) for US children is 5 to 6 years (Stipek, 2009), we set our age period for school entry at age 4 to 6.5 years. This wide time frame allows for variability across individuals in the timing of their actual school entry, including accommodating for the likelihood that some children may enter preschool before attending kindergarten (Love and Raikes, 2009). The postentry group was assessed at an average of approximately 2.5 years later, a time frame for assessing adjustment to school entry that is consistent with methodological decisions made for the Pathways project, a National Institutes of Health-funded longitudinal study of children’s transition to school and subsequent academic and social–emotional functioning (Ladd, 2009).
Method
Participants
This longitudinal study was based on a retrospective review of medical charts of children with congenital CFAs who were patients of a department of reconstructive plastic surgery at a large urban medical center serving a regional population. During the years 1994 to 2000, parents were asked to complete psychosocial assessments on an approximately yearly basis as part of their child’s ongoing care; virtually all families participated. Psychological consultations were provided at the request of families. This chart review was approved by the medical center’s institutional review board.
The chart review yielded 42 patients (20 girls) having a PSI/SF (Abidin, 1990) completed when they were between 3.9 to 6.5 years old (time 1, mean age = 5.3 years), as well as when they were between 6.5 and 9.8 years old (time 2, mean age = 8 years). On average, the time elapsed between participants’ time 1 and time 2 was 2.7 years. Of the 42 patients, 35 had a Child Behavior Checklist (CBCL; Achenbach, 1991) completed at time 1 and 41 had a CBCL completed at time 2; 34 had CBCLs at both time 1 and time 2. Primary diagnoses included cleft lip and/or palate (n = 20), hemifacial microsomia (n = 4), craniofacial microsomia (n = 2), metopic synostosis (n = 2), Crouzon syndrome (n = 2), and Treacher Collins syndrome (n = 2). Additional conditions included coronal synostosis, frontonasial dysplasia, Goldenhar syndrome, Pfeiffer syndrome, Pierre Robin sequence, sagittal synostosis, and unidentified facial anomalies.
Demographic information in the medical charts provided the following information about the sample: ethnicity (61% Caucasian, 2% black, 12% Hispanic, 12% Asian, 13% other or missing), mother’s highest level of education (2% grade school, 29% high school, 37% college, 27% graduate/professional school, 5% missing), and father’s highest level of education (5% grade school, 27% high school, 17% college, 39% graduate/professional school, 12% missing).
Measures
Parenting Stress Index/Short Form
The PSI/SF is a measure of stress experienced within the parenting role and consists of 36 items derived from the full-length PSI through factor analysis (Abidin, 1990). The total stress score—which was used as our measure of parenting stress—represents a summary score of the 36 items. Scores were computed as mean item scores, potentially ranging from 1 to 5; higher scores represent higher levels of stress, with scores above the 90th percentile considered clinically significant. This measure can be used both to designate clinical groupings (based on the 90th percentile cutoff) and as a continuous assessment of parents’ experience of stress. The PSI/SF has evidence of validity due to its high correlation with the full-length PSI, which has previously been correlated with measures of family functioning, maternal adjustment and coping, and child adjustment (Abidin, 1990). The PSI/SF has been shown to have adequate test–retest reliability and internal consistency (Cronbach α = 0.91 for Total Stress Scale; Abidin, 1990).
Child Behavior Checklist/4-18
The Child Behavior Checklist/4-18 (CBCL/4-18) is a measure of psychosocial adjustment in children ages 4 through 18; it contains 113 items in which caregivers rate the frequency of children’s problem behaviors (0 = not true, 1 = somewhat or sometimes true, or 2 = very true or often true; Achenbach, 1991). Scores yield 2 broadband scales: internalizing problems (anxious–depressed, withdrawn, and somatic problems) and externalizing problems (aggressive behavior, delinquency, and attention problems). Raw scores are converted into T scores (mean of 50, standard deviation of 10), which are normed based on age and gender, with a cutoff for clinical significance at the 90th percentile. Higher scores indicate greater severity of child problems; thus, this measure provides a means for assessing a continuous range of problems. The CBCL/4-18 has acceptable validity and reliability (Cronbach α ranges from 0.88 to 0.96 for internalizing and externalizing scales) and has been used extensively with pediatric samples (Achenbach, 1991).
Results
Descriptive Analyses
Means, standard deviations, and ranges of scores are reported in Table 1 for all study variables.
Descriptive Statistics for PSI/SFa and CBCL Scales.b
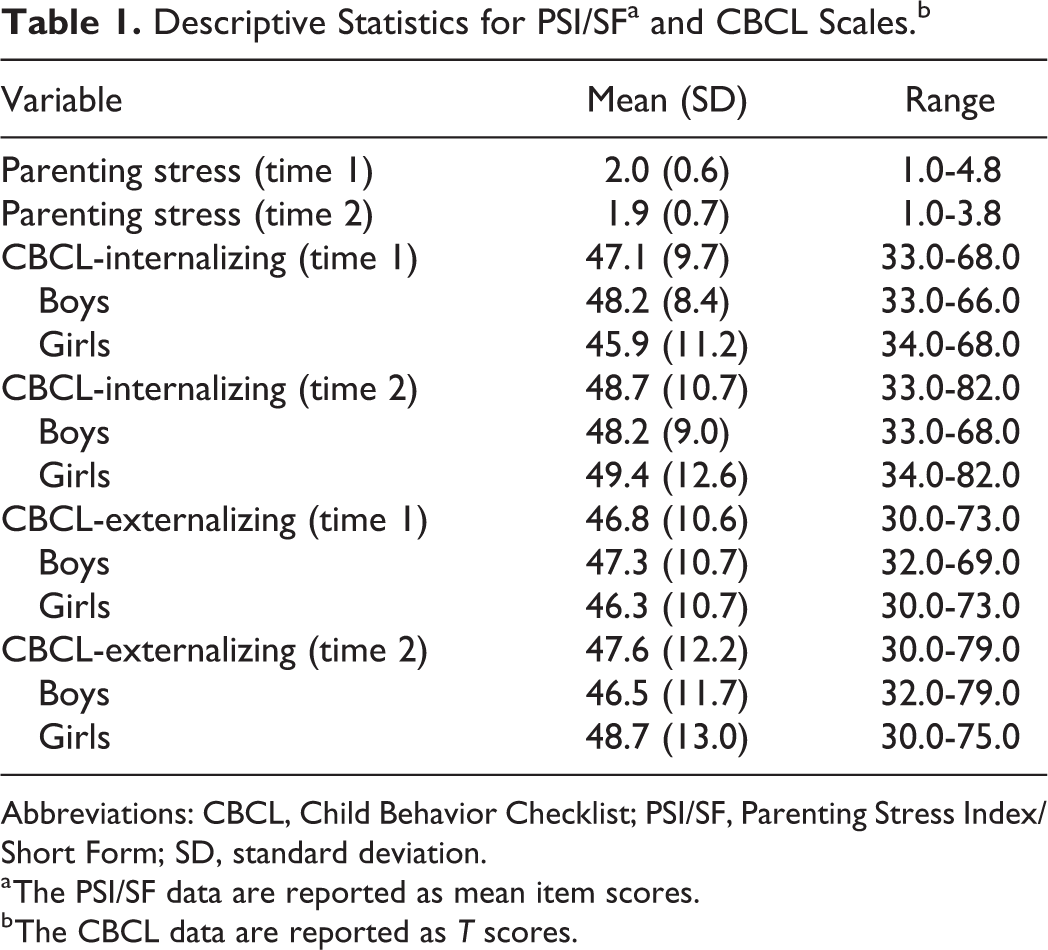
Abbreviations: CBCL, Child Behavior Checklist; PSI/SF, Parenting Stress Index/Short Form; SD, standard deviation.
a The PSI/SF data are reported as mean item scores.
b The CBCL data are reported as T scores.
Parenting Stress Index/Short Form
A paired samples t test showed that parent-reported stress was not significantly higher at time 1 than at time 2, in contrast to our hypothesis (t 41 = 1.062, P = .29, d = 0.15). When compared to total stress scores reported from the PSI/SF standardization sample (summed score average = 71, mean item score average = 1.97; Abidin, 1990), there was no significant difference for parents in the CFA sample at time 1 (t 840 = 1.0, P = .32, d = 0.13) or at time 2 (t 840 = 0.42, P = .067, d = 0.05); parents in our sample did not differ from norms when considering mean levels, contrary to our hypothesis. However, compared to the standardization sample, a higher percentage scored above the 90th percentile clinical cutoff for parenting stress at both time 1 (19%; χ2[1] = 3.82, P = .05) and time 2 (21%; χ2[1] = 6.10, P = .01), indicating higher-than-expected rates of clinically significant levels of stress for this CFA sample, as predicted.
Child Behavior Checklist
Sample means for internalizing and externalizing scales were compared with mean scores from Achenbach’s (1991) normative sample. Scores were compared separately by gender to be consistent with Achenbach’s (1991) normative reference groups (males, internalizing: M = 50.2; males, externalizing: M = 50.0; females, internalizing: M = 50.0; females, externalizing: M = 50.0). Child Behavior Checklist scores in the CFA sample for both boys and girls were not significantly different from those in the normative sample at time 1, but they were significantly different for girls at time 2. Rates of boys with CFAs scoring above the 90th percentile clinical cutoff were comparable with norms at time 1 on internalizing (5.3%, χ2(1) = 0.47, P = .49) and externalizing (10.5%, χ2(1) = 0.01, P = .94) as well as at time 2 on internalizing (4.5%, χ2(1) = 0.73, P = .39) and externalizing (9.1%, χ2(1) = 0.02, P = .89). Rates of girls with CFA scoring above the 90th percentile clinical cutoff were also comparable with norms at time 1 on internalizing (12.5%, χ2(1) = 0.11, P = .74) and externalizing (6.3%, χ2(1)= 0.25, P = .62). However, at time 2, there were significantly more girls in our sample with internalizing scores above the clinical cutoff than expected (15.8%, χ2(1)= 4.00, P = .045). Similarly, there were significantly more girls in our sample with externalizing scores above the clinical cutoff than expected at time 2 (21.1%; χ2(1) = 13.44, P = .0002).
Longitudinal Analyses
Plan of analyses
Multiple regressions were used to evaluate (1) the contribution of parental stress at school entry to child internalizing and externalizing problems 2.5 years later and (2) the contribution of child internalizing and externalizing problems at school entry to parental stress 2.5 years later. All analyses were conducted with full sample (not separated by gender) to preserve power. Initial regression models controlled for gender and age; because these variables were nonsignificant in every model, they were removed to preserve power. In each regression model, the time 1 variable for the outcome was included as a control variable. Semipartial correlations, indicating incremental variance beyond that contributed by the control variable, are presented for purposes of demonstrating effect sizes, which are more precise and interpretable indicators of obtained relations than is statistical significance, due to its dependence on power derived from sample size (Cohen et al., 2003). In keeping with Cohen (1992), we considered magnitudes of effect sizes as follows: <0.10 as “trivial”, 0.10 to 0.30 as “small to medium”, 0.30 to 0.50 as “medium to large”, and >0.50 as “large to very large.”
Correlations among parenting stress and child adjustment scores
Table 2 presents bivariate correlations between time 1 and time 2 study variables. Time 1 to time 2 stabilities were large to very large for parenting stress and for internalizing and externalizing. Medium to large effect sizes were seen in the relations between time 1 parenting stress and time 1 adjustment (internalizing and externalizing), as well as between time 1 parenting stress and time 2 adjustment (internalizing and externalizing). Time 1 internalizing and externalizing both showed medium to large effect sizes in their associations with time 2 parenting stress.
Bivariate Correlations of PSI/SF and CBCL Scores at Time 1 and Time 2.a
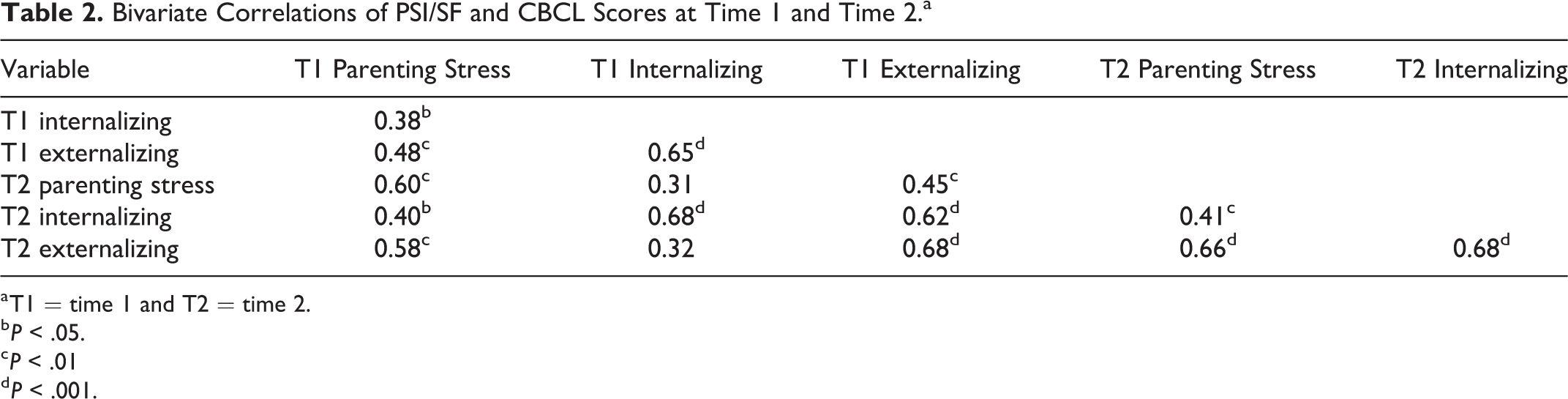
a T1 = time 1 and T2 = time 2.
b P < .05.
c P < .01
d P < .001.
Predicting postentry child adjustment from parenting stress at school entry
Table 3 presents multiple regression models predicting time 2 child adjustment from parenting stress at school entry (time 1). Medium effect sizes were seen in the prediction of time 2 internalizing (sr = 0.31) and time 2 externalizing (sr = 0.39) from time 1 parenting stress, showing that elevated parental stress was associated with later emotional and behavioral problems in children.
Multiple Regression Models.a
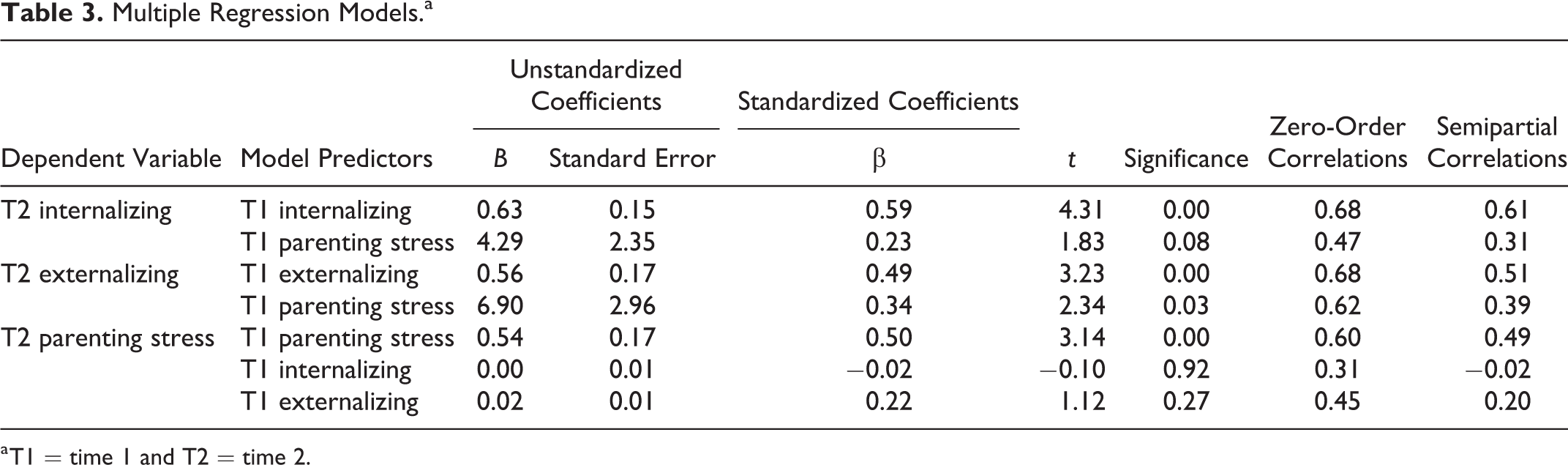
a T1 = time 1 and T2 = time 2.
Predicting postentry parenting stress from child adjustment at school entry
Table 3 presents a multiple regression model predicting time 2 parenting stress from child adjustment at school entry. This model included time 1 internalizing and time 1 externalizing entered together as predictors of time 2 parenting stress. It demonstrated trivial independent effects in the prediction of time 2 parenting stress from time 1 internalizing (sr = −0.02). A small to medium effect size was seen in the independent prediction of time 2 parenting stress from time 1 externalizing (sr = 0.20), indicating that early behavior problems were associated with later elevations in caregiver stress.
Discussion
The aim of the current study was to assess whether parents of children with CFAs experience elevated levels of stress when their children begin attending school and whether such parenting stress shows longitudinal associations with child adjustment. Although caregivers in this population have been shown to be at risk for experiencing increased stress during infancy and toddlerhood, existing research neglects questions about parenting stress occurring in early school years for the CFA population. It is critical to build our understanding of parenting stress because it has the potential to compromise caregiving, which in turn may affect child adjustment; increased knowledge about periods likely to heighten stress will enable the provision of sensitive targeted interventions.
One goal of the study was to test the hypothesis that school entry is a period of heightened stress for parents of children with CFAs. Caregivers in our sample scored above the clinical cutoff on parenting stress at double the rates of norms from typically developing samples; this was seen both at school entry and 2.5 years later, supporting the idea that caregivers in this population are at risk for experiencing clinically significant levels of parenting stress when their children are in elementary school. Contrary to our hypothesis, parental stress did not decrease after children had time to adjust to school.
This finding that heightened parental stress is present at school entry and continues into early elementary school is concerning and suggests that parenting challenges may be stable during this developmental period. The transition into entering school is developmentally challenging for all children, as they face new academic and social demands and learn to contend with increasing independence (Cowan and Cowan, 2009). Consequently, caregivers of typically developing children may experience increased stress as their children navigate this transition (Baker et al., 2003). For children with chronic illness or disabilities, developmental tasks may be challenging throughout elementary school, as differences with peers are highlighted and skill acquisition may be limited (Simeonsson and Rosenthal, 2001). Children with CFAs, who are at risk for learning disorders and social problems, may struggle more than their unaffected counterparts during this period (Pope and Snyder, 2005; Collett et al., 2014; Knight et al., 2015). Even before children exhibit learning problems, their parents may worry that they will struggle more (Pope, 1999), potentially increasing parenting stress. The associations seen between parental stress and child adjustment suggest that parents in this population may experience concerns during early schooling that are exacerbated in the presence of significant adjustment problems in their children.
A goal of the current study was to evaluate child adjustment as a function of parenting stress. Before examining the parent–child influences, we compared psychological adjustment to Achenbach's (1991) norms to identify any elevations within our sample. Boys’ adjustment was comparable to norms at both time points, as was the case for younger (time 1) girls. However, the older (time 2) girls showed greater prevalence of clinical levels of problems for both internalizing and externalizing disorders. These findings, except for those regarding girls at time 2, are mostly consistent with the literature suggesting that children with CFAs do not generally have significant problems in psychological adjustment (Pope and Snyder, 2005; Ruff et al., 2016). Studies that have found increased prevalence of disorder tend to be specific to internalizing problems (Hunt et al., 2005; Pope and Snyder, 2005; Brand et al., 2009; Murray et al., 2009; Richman et al., 2012), with mixed findings reported for the prevalence of externalizing problems in this population (Richman et al., 2012). Our finding that girls developed more adjustment problems over time is concerning and indicates the need for more longitudinal studies examining the unfolding of causal processes.
Our examination of the role of early parent stress in predicting later child adjustment problems resulted in medium-sized associations for both internalizing and externalizing problems. This suggests that stress could compromise caregiving, in that stressed parents may have depleted emotional resources and may not be able to meet the emotional needs of their children or be able to manage difficult acting-out behaviors (Pope, 1999). The children, in response, may experience worry, distress, and social withdrawal or develop problems with behavioral control.
The current study also assessed whether adjustment problems at school entry among children with CFAs were associated with parenting stress 2.5 years later. Internalizing problems were not associated with subsequent parenting stress. However, child externalizing predicted future parenting stress, consistent with the well-established transactional relationship between parenting stress and child behavior problems (Neece et al., 2012). This bidirectional relationship can turn into a vicious cycle; child behavior problems can lead to increased parental stress, which compromises caregiving, and results in more child behavior problems and an increasingly stressful home environment.
Given that the early school years seem to be a period of heightened stress for parents of children with CFAs and that parental stress at school entry is predictive of later child internalizing and externalizing problems, future research should focus on interventions to alleviate parental stress during this important developmental period. This period is, indeed, critical for children, because their initial adjustment to school is a strong predictor of their academic, social, and emotional functioning throughout high school (Cowan and Cowan, 2009). Among typically developing children, adjustment to school has been shown to be positively impacted by caregiver-based interventions during the preschool period (Cowan and Cowan, 2009). For the CFA population, interventions should provide parents with concrete steps to take to facilitate their child’s adjustment at school, including strategies for discussing the child’s condition with teachers and finding a suitable classroom placement for the child (Pope, 1999). Interventions should also teach parents how to modulate their own anxiety surrounding concerns about peer socialization and should preemptively teach them how to help their child problem-solve during instances of teasing (Pope, 1999).
In addition, the findings of the current study elucidate the potential need for interventions to address the influence of child behavior problems on parenting stress. Such programs should validate parental concerns about problematic child behavior, while also teaching caregivers how to respond effectively to behavior problems through the use of evidence-based interventions (eg, parent management training, which has been shown to improve child behavior problems and simultaneously reduce parenting stress; Colalillo and Johnston, 2016). The finding that rates of clinical levels of internalizing and externalizing problems largely did not exceed norms—which is good news—should not detract from the implication that improved parental functioning will likely lead to improved child functioning and that children’s acting-out behaviors can compromise the quality of the parenting they receive.
Interpretation of the study findings is qualified by methodological limitations. By prioritizing external validity—using a heterogeneous CFA sample and a broad time frame for our school entry and postentry stages—we necessarily sacrificed internal validity. Thus, although our results might be generalizable to a broad range of families with children having CFAs, our design does not permit us to make inferences about specific aspects of the CFA experience (eg, medical or appearance factors) or influential factors within school (eg, type or quality) or family (socioeconomic status, parent education, number of siblings, etc) contexts that could potentially play a role in the processes we studied. It is a fair criticism to suggest that our 2 longitudinal time points do not precisely indicate school entry or adjustment to schooling. However, school entry represents a developmental period rather than a moment in time. The beginning of schooling has been conceptualized as occurring as early as preschool (Baker et al., 2003), up until first grade (Egeland and Kreutzer, 1991). The impact on families likely begins prior to the first day of school, when parents are anticipating this transition and making preparations with their children. The point at which adjustment to school has been achieved also varies widely across individuals and must be broadly specified in order to capture the phenomenon for all children. Therefore, the age ranges chosen in our study were intended to encompass the breadth of these 2 developmental periods.
The use of single-informant sources presents another limitation to this study, potentially leading to inflated effects. Future studies should include teacher reports or behavioral observations of child functioning for added objectivity. Our use of published standardization samples, rather than a between-group design with a typically developing child comparison group, precludes our ability to make inferences about processes that are unique to the CFA population; as a first study of these questions, the obtained findings would support further research that might identify specific factors involved in parenting children with CFA.
Because our design assessed only 2 time points, we are unable to determine whether the observed elevations in clinical levels of parenting stress are related to the timing of schooling or instead may have been stable from early childhood. Providing early and ongoing support to caregivers of children with CFA would be prudent as an effort to promote high-quality parenting. Although it is concerning to see that 20% of our sample (when compared to 10% of the standardization sample) experienced clinical levels of parenting stress, the great majority of parents in the sample were within normative levels. Research focused on the adaptive capabilities of this majority might yield important insights into productive avenues to guide struggling parents.
Future research should investigate the factors that influence stress levels among caregivers of children with CFAs, as these still remain unclear; the relatively small amount of variance contributed by children’s adjustment variables indicates that unmeasured factors play a substantial role in parenting stress. For instance, social support, parent personality, or parent coping style may affect the extent to which parents experience stress at school entry, and a closer focus on specific risk factors associated with the management of child CFA is warranted. Achieving a more complete understanding of these factors will lead to improved interventions for parents and children in the CFA population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.