
Abstract
Objective:
This report describes the case of a male patient with a complete unilateral cleft lip and palate who presented with midface deficiency and an anteroposteriorly constricted maxilla.
Design:
Case report Interventions: Correction involved anterior distraction of the segmented maxilla.
Results:
The present case demonstrates that elongation of the maxilla with anterior distraction is an effective way to develop a proper dental arch, correct anterior and posterior crowding, and improve a midface deficiency.
Introduction
Impaired maxillary growth, which is often found in patients with cleft lip and palate (CLP), can result in serious skeletal and/or dental pathological conditions. Approximately 10% to 25% of patients with CLP require orthognathic surgery (Cohen et al., 1995; DeLuke et al., 1997; Schnitt et al., 2004). Maxillary advancement is achieved through either LeFort I osteotomy (Posnick and Dagys, 1994) or total maxillary distraction osteogenesis (total DO; Scolozzi, 2008). Total DO uses LeFort I as a bone cutting line, leading to gradual advancement of the whole maxilla (Scolozzi, 2008). However, both LeFort I osteotomy and total DO techniques may pull the velum forward, potentially inducing velopharyngeal incompetence (VPI; Janulewicz et al., 2004); this can cause nasal resonance (hypernasality) and reduced speech intelligibility. To overcome this potential speech disorder, our clinical team recently developed maxillary anterior segmental distraction osteogenesis (MASDO), a technique that facilitates the forward advancement of the anterior maxillary segments without affecting the patient’s velopharyngeal function (Iida et al., 2007; Aikawa et al., 2010). This technique can also correct a flattened or collapsed arch (Aikawa et al., 2010; Hirata et al., 2016). A relapse rate of 10% has been reported for the elongated bone (Tanikawa et al., 2018). Consequently, MASDO is becoming a new alternative to conventional total DO or LeFort I osteotomy in patients with CLP exhibiting suspected VPI after surgery and/or a flattened dental arch. To date, orthodontic considerations regarding the management of the elongated arch (prosthodontic treatment or space closure for tooth movement) have not been thoroughly discussed in the literature. It is considered that the constricted arch in patients with CLP is related to anterior and/or posterior crowding.
The purpose of this report is to describe the case of a patient with unilateral CLP and severe maxillary hypoplasia who received orthodontic treatment after MASDO that successfully eliminated anterior/posterior dental crowding and achieved the development of a proper dental arch.
Case History
A Japanese boy (age: 13 years 10 months) with a right-sided unilateral cleft lip, alveolus, hard palate, and soft palate presented with an aesthetic complaint of an anterior crossbite. He had undergone cheiloplasty and palatoplasty at the age of 3 months and 15 months, respectively. Phase I orthodontic treatment, which the patient underwent at age 7 years 4 months, consisted of maxillary lateral expansion with an expansion plate and protraction of the maxilla with reverse headgear. Due to his abnormal velopharyngeal function, he received continuous pronunciation therapy with a speech appliance, beginning at age 4 years 9 months, to assist with the acquisition of communication skills.
Clinical Examination
The patient’s facial profile was concave with severe midface deficiency (Figure 1A). Scar tissue was observed intraorally on the palate (Figure 2A), and aberrant arch form with decreased anterior–posterior length was observed (Figure 2A). The patient had an Angle Class III molar relationship with an overjet of −9.0 mm and an overbite of −3.0 mm in the incisor region (Figure 2A). The upper left and right permanent lateral incisors were congenitally absent (Figure 3A). The upper left first premolar had ectopically erupted into the position of the absent lateral incisor. The upper left canine and second premolar showed distal rotation. Both the maxillary and mandibular dentition were mildly crowded (arch length discrepancy = −4 mm and −0.5 mm, respectively).

Facial photographs: A, Pre-2nd phase treatment (13 years 10 months); (B) pre-MASDO (15 years 11 months); (C) post-MASDO (16 years 8 months); (D) postactive treatment (18 years 11 months); (E) postretention (20 years 11 months). MASDO indicates maxillary anterior segmental distraction osteogenesis.

Intraoral photographs: A, Pre-2nd phase treatment (13 years 10 months); (B) pre-MASDO (15 years 11 months); (C) post-MASDO (16 years 8 months); (D) postactive treatment (18 years 11 months); (E) postretention (20 years 11 months). MASDO indicates maxillary anterior segmental distraction osteogenesis.
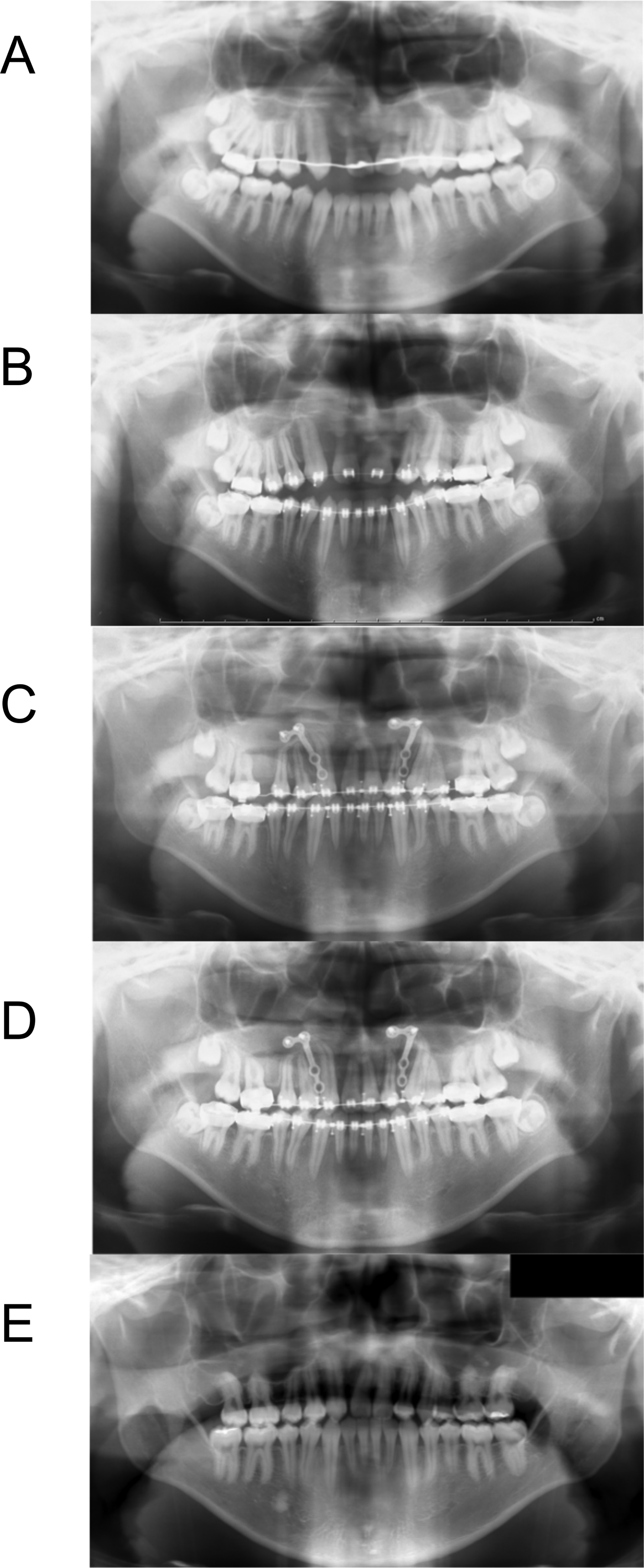
Panoramic radiographs: A, Pre-2nd phase treatment (13 years 10 months); (B) pre-MASDO (15 years 11 months); (C) post-MASDO (16 years 4 months); (D) post-space closure (16 years 8 months); (E) postretention (20 years 11 months). MASDO indicates maxillary anterior segmental distraction osteogenesis.
We observed no clinically discernible signs of clicking or pain in the temporomandibular joints or any limitation or deviation of jaw movement. The patient was in good general health with no significant medical history.
Radiographic Examinations
Lateral cephalometric analysis (Figure 4A and Table 1) revealed skeletal Class III malocclusion due to aberrant arch form with anterior–posterior constriction. The maxillary length (pterygomaxillary fissure–subspinale palatal plane [Ptm-A/PP]) was much shorter than the normative mean (Wada, 1977). Panoramic radiograph revealed that the upper left and right second molars were distally inclined and the right third molars tended toward impaction with the inclined second molar, indicating posterior crowding (Figure 3A).
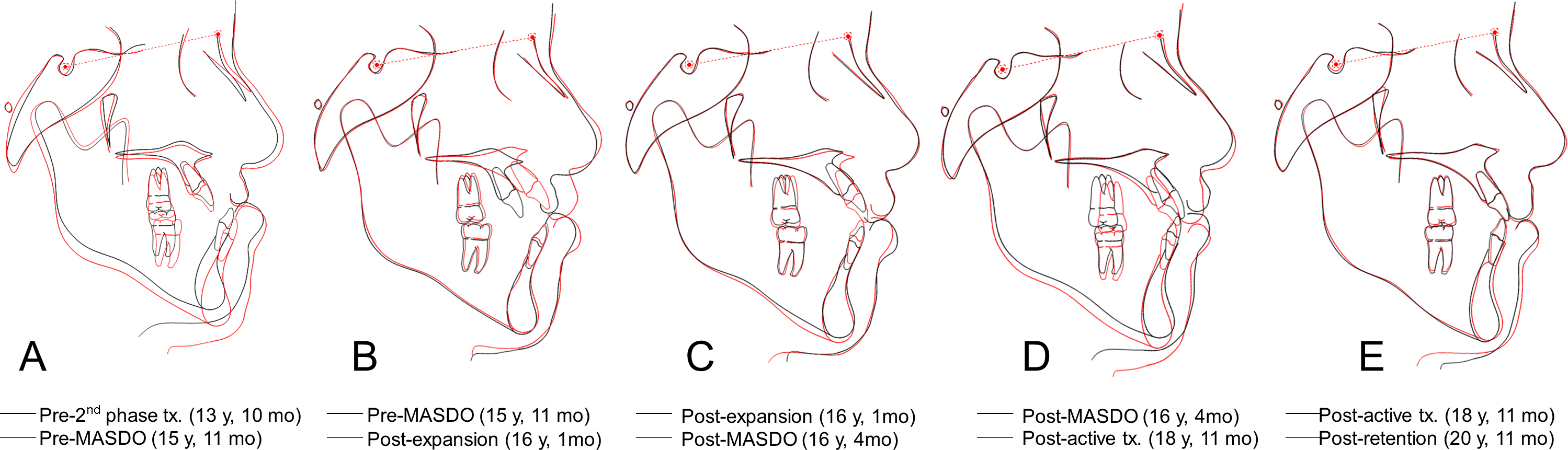
Superimposed lateral cephalometric tracings on the SN plane at S: A, Pre-2nd phase treatment (black line) and pre-MASDO (red line); (B) pre-MASDO (black line) and postexpansion (red line); (C) postexpansion (black line) and post-MASDO (red line); (D) post-MASDO (black line) and postactive treatment (red line); (E) postactive treatment (black line) and postretention (red line). MASDO indicates maxillary anterior segmental distraction osteogenesis; N, nasion; S, sella; SNA, sella-nasion.
Cephalometric Analysis at Pre-2nd Stage Treatment, Pre-MASDO, Postexpansion Phase, Post-MASDO, Postactive Treatment, and Postretention Stages.
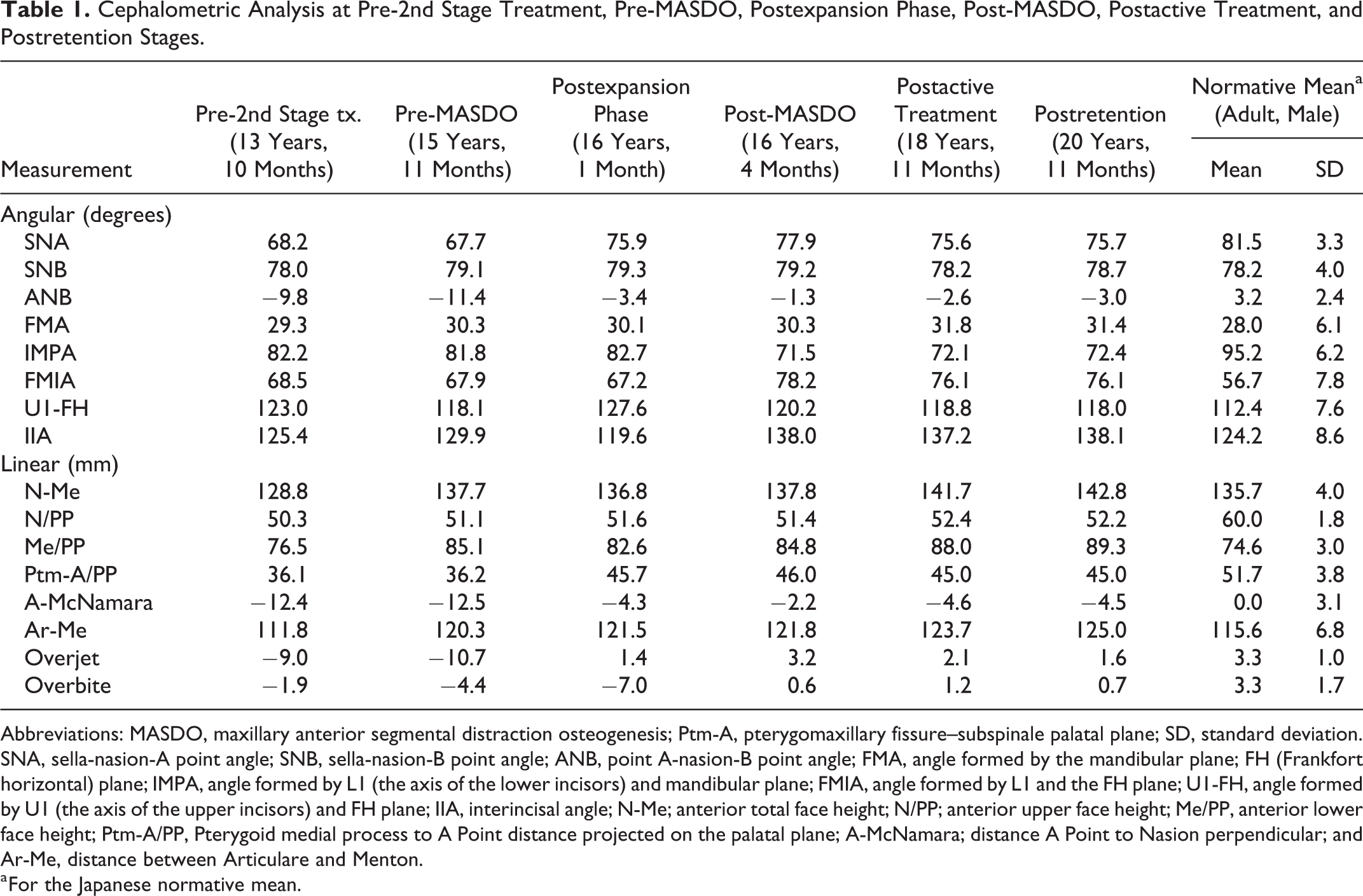
Abbreviations: MASDO, maxillary anterior segmental distraction osteogenesis; Ptm-A, pterygomaxillary fissure–subspinale palatal plane; SD, standard deviation. SNA, sella-nasion-A point angle; SNB, sella-nasion-B point angle; ANB, point A-nasion-B point angle; FMA, angle formed by the mandibular plane; FH (Frankfort horizontal) plane; IMPA, angle formed by L1 (the axis of the lower incisors) and mandibular plane; FMIA, angle formed by L1 and the FH plane; U1-FH, angle formed by U1 (the axis of the upper incisors) and FH plane; IIA, interincisal angle; N-Me; anterior total face height; N/PP; anterior upper face height; Me/PP, anterior lower face height; Ptm-A/PP, Pterygoid medial process to A Point distance projected on the palatal plane; A-McNamara; distance A Point to Nasion perpendicular; and Ar-Me, distance between Articulare and Menton.
a For the Japanese normative mean.
Diagnosis and Treatment Plan
The surgical approach involved correction of the small maxilla, in the horizontal sagittal plane using MASDO. The plan was to completely close the space created by MASDO on the right side through mesial movement of the molars and on the left side through distal movement of the second premolar and mesial movement of the molars.
Treatment Progress
Pre-MASDO orthodontic treatment began when the patient was aged 15 years 9 months with 0.022-inch-slot preadjusted edgewise appliances (Figures 1B, 2B, 3B, 4A, and 5A). At the age of 16 years 1 month, MASDO was performed on both sides between the second premolar and the first molar using a single palatal distractor from the DynaForm Intraoral Distraction System (Stryker Leibinger, GmbH & Co. KG, Freiburg im Breisgau, Germany; Figure 6A and B). Two L-shaped titanium miniplates (Stryker Leibinger, GmbH & Co. KG) were also positioned on the labial side of the anterior segment of the maxilla for skeletal anchorage. The distraction was initiated 7 days after surgery with an expansion of 1.0 mm per day. The activation was performed by surgeons in-house. The required expansion was estimated to be 8.0 mm based on the A-McNamara evaluation (McNamara, 1984). We expanded an additional 2.0 mm, for a total of 10.0 mm, due to the clinical observation of counter-clockwise rotation of the transport segment during expansion (Figures 4B, 5B, 6C, and 6D). As an additional measure to prevent this unwanted upward movement during the distraction phase, we provided orthodontic elastic protraction (250-350 g force) from the facemask to the edgewise appliance located on the anterior segment, while the edgewise appliance was connected to the skeletal anchorage by wire ligatures.
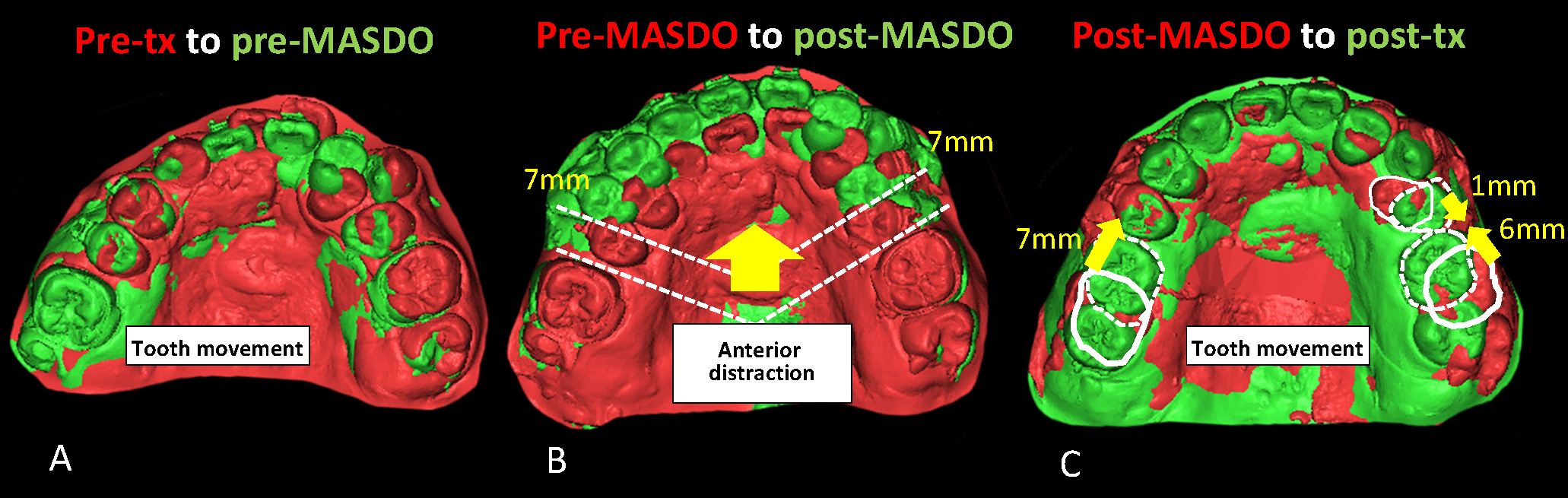
Superimposed 3-dimensional models: A, Pre-2nd phase treatment (red) and pre-MASDO (green); (B) pre-MASDO (red) and estimated post-MASDO (green); (C) and estimated post-MASDO (red surface and white dotted line) and postactive treatment (green surface and white solid line). MASDO indicates maxillary anterior segmental distraction osteogenesis.
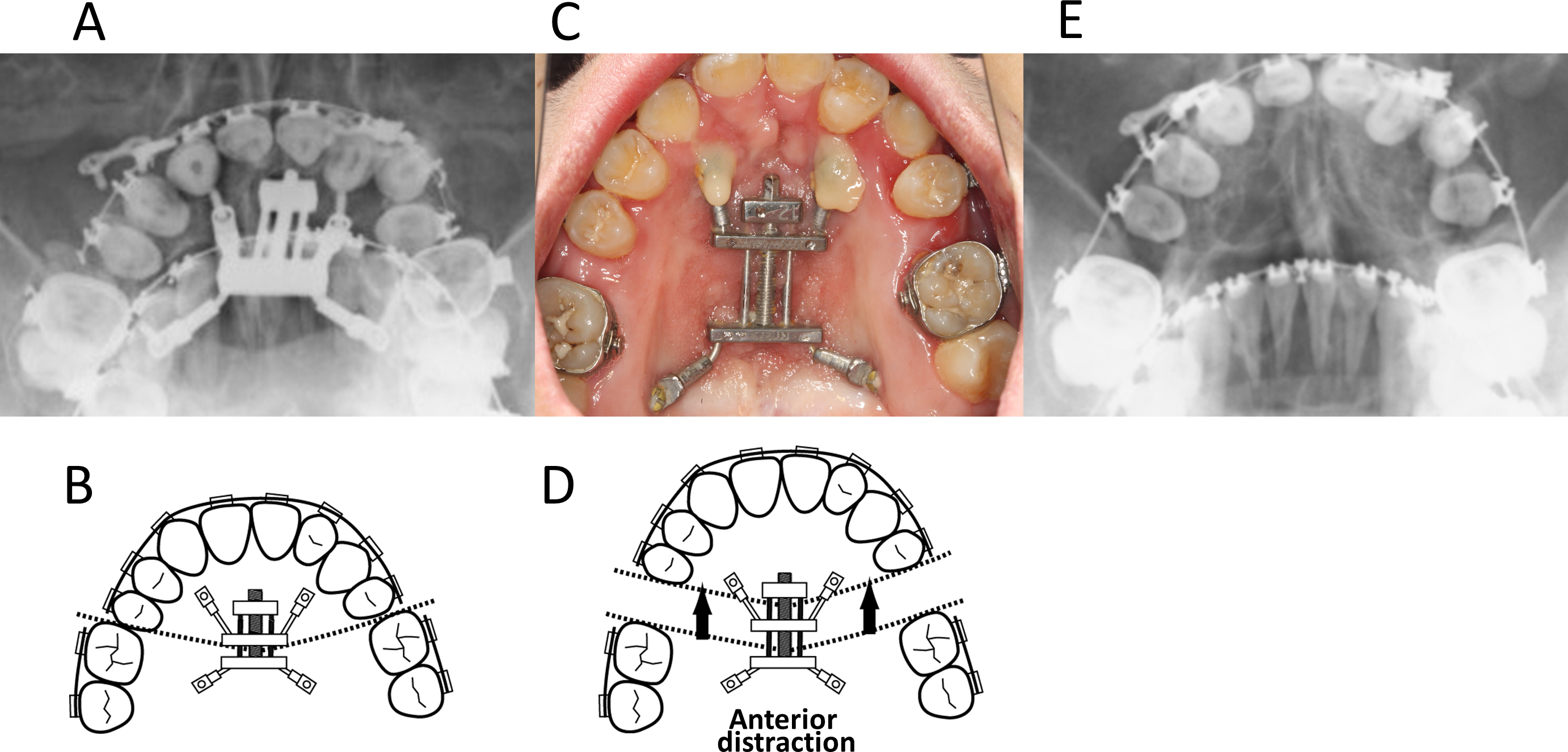
Occlusal radiograph (A) and schematic illustration (B) at pre-expansion (16 years 1 month); intraoral photograph (C) and schematic illustration (D) at postexpansion (16 years 2 months); and occlusal radiograph (E) at post-MASDO (removal of the distractor; 16 years 4 month). MASDO indicates maxillary anterior segmental distraction osteogenesis.
Immediately after the distraction phase, gradual mesial movement of the first molars was started using elastic protraction from the facemask to the upper first molars. Intermaxillary elastic traction for continued downward rotation of the segment was used during the 3-month consolidation period. After the consolidation period (age: 16 years 4 months), the distractor was removed under general anesthesia (Figures 3C, 4C, and 6E). The spaces created by the distractor on both sides were closed by using a combination of elastic chains located on the edgewise appliances and elastic protraction from the facemask. Three months after the removal of the distractors (age: 16 years 7 months), the spaces (7.0 mm following the consolidation phase) on both sides were nearly closed (Figures 1C, 2C, and 3D; Table 1). Thus, in total, the space closure took 6 months, beginning immediately following distraction; the majority of the spaces were closed after the consolidation phase. After the spaces closed completely, the face mask was discontinued.
Due to the sustained velopharyngeal dysfunction after the MASDO procedure, the patient underwent pharyngoplasty at age 18 years 1 month. As a result of the surgery, the patient’s speech was improved. All appliances were removed when the patient was aged 18 years 11 months (Figures 1D, 2D, 4D, and 5C; Table 1). For the next 2 years, a wrap-around-type retainer was used for the upper dental arch, and a spring retainer was used for the lower arch (Figures 1E, 2E, 3E, and 4E; Table 1).
Results
Clinical examination revealed that MASDO resulted in satisfactory facial aesthetics and intercuspation of the teeth. The facial profile had changed from concave to straight (Figure 1D). Panoramic radiographs (Figure 3B) showed bone formation in the distraction gap between the upper second premolar and the first molar bilaterally after MASDO. Mesial movement of both upper molars was achieved using skeletal and dental anchorage in the anterior regions, and the spaces created by MASDO were completely closed bilaterally. The second molars were successfully uprighted following mesial movement of the first molars, indicating elimination of posterior crowding. After the termination of active treatment, the patient had a Class II molar relationship bilaterally with an overjet of +2.1 mm and an overbite of +1.2 mm (Figure 2D). No tooth root resorption was observed in the upper molars that were moved into the new bone created by MASDO.
Comparing the cephalometric tracings (Figure 4) and measurements (Table 1) before and after active orthodontic treatment demonstrated the following changes: the sella-nasion-A point angle increased from 68.2° to 75.6°, thus improving the point A-nasion-B point angle from −9.8° to −2.6°. The Ptm-A/PP increased from 36.1 to 45.0 mm. Although the results still indicated a skeletal Class III malocclusion, positive overjet and overbite were successfully achieved with the extrusion and lingual inclination of the lower incisors.
After a 2-year retention period, the patient’s occlusion and facial profile became stable with positive overjet and overbite (Figures 1E, 2E, and 4E).
Using the 3-dimensional superimposition method with models before and after treatment, we were able to accurately assess the change in the patient’s arch form. The maxillary dental arch form had changed from an anteroposteriorly constricted arch form to a symmetrical U-shaped arch form. There was a 7-mm space on both the left and right side created by the MASDO procedure, which was successfully closed by orthodontic tooth movement (Figure 5).
Discussion
The patient in this case presented with an anteroposteriorly constricted maxillary arch form with midface deficiency and dental crowding. After surgical intervention using MASDO and subsequent orthodontic treatment, the patient’s concave facial profile, skeletal class III malocclusion with a retruded maxilla, anterior crossbite, and dental crowding were successfully repaired; no additional surgery or prosthodontic treatment was required.
In this case, we employed a single palatal distraction appliance. Cephalometric superimposition shows that there was rotation of the anterior segment by approximately 9.5° (Figure 4B, changes of U1-FH from 15 years 11 months to 16 years 1 month) in the counterclockwise direction immediately following the expansion phase for which we provided elastic protraction from the facemask. We assumed that a single palatal distractor placed below the center of resistance of the anterior segment of the maxilla in addition to soft tissue tension caused the vertical counterclockwise rotation; this result is consistent with that of a previous study (Tanikawa et al., 2018). To correct this upward rotation, we utilized the intermaxillary elastics in the consolidation phase, generating a downward rotational movement of the anterior maxilla. Conversely, we did observe an adverse effect, which was that the intermaxillary elastics caused extrusion of the lower incisors by approximately 3 mm in the consolidation phase. The treatment results in the present case might have been improved by the use of elastics directly from anterior mandibular skeletal anchorage to avoid this problem.
The patient in this case had a significantly small maxilla, and we determined that approximately 8 mm of maxillary advancement would be needed to reestablish a normal anteroposterior skeletal relationship. In treatment planning, conventional surgical procedures (ie, 2-jaw surgery for maxillary advancement by a LeFort I osteotomy and mandibular setback by bilateral sagittal segment osteotomy) were also considered. Previous reports describing conventional LeFort I osteotomy suggest that an advancement greater than 6 to 10 mm is difficult to achieve with a LeFort I osteotomy because of the potential for speech deterioration and/or the challenges presented by soft-tissue intensity and scarring (Cheung et al., 2006; Alkan et al., 2008; Choi et al., 2012). In contrast, a recent report (Watts et al., 2015) showed that final maxillary advancements of more than 10 mm were achieved successfully using a LeFort I osteotomy. Thus, in the present case, 1 or 2-jaw surgery could have been chosen for treatment. However, MASDO was selected for several reasons as described below.
Figure 7A is an illustration that simulates the arch coordination when selecting 2-jaw surgery. In this case, the maxillary right and left molars need to be moved lingually, and the maxillary right premolars need to be moved labially, in order to generate a symmetric arch form. In contrast, Figure 7B represents the preorthodontic treatment prior to performing MASDO. In this case, the distorted anterior region is elongated forward, which enables arch coordination with medialization of the molars. Relapse has been reported, especially in the upper canine and first premolar region, when expanding the cleft palate (Li and Lin, 2007); therefore, avoiding the premolar expansion with preorthodontic treatment as illustrated in Figure 7B is preferred. Furthermore, the patient in the present case showed sparse bone formation in the molar region (Figure 8), which highlighted the difficulty of arch coordination during tooth movement. Thus, as a result of these orthodontic considerations, we selected MASDO for this patient.
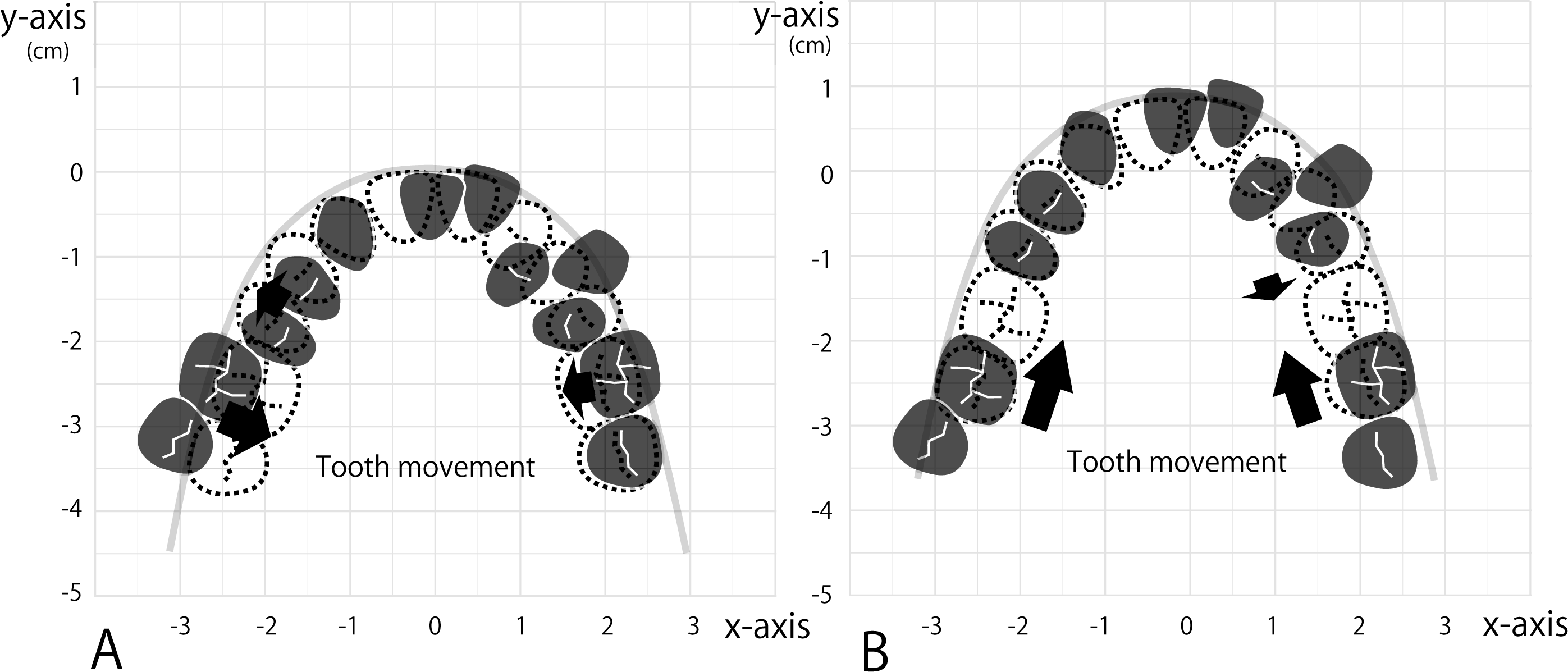
Schematic illustration of the tooth alignment. A, Tooth alignment at the pre-2nd phase treatment for the conventional 2-jaw surgery; (B) That for elongation by MASDO. Black filled tooth shape denotes pretreatment tooth alignment. Dotted line, tooth movement needed for each method. The y-axis shows the midsagittal plane. MASDO indicates maxillary anterior segmental distraction osteogenesis.
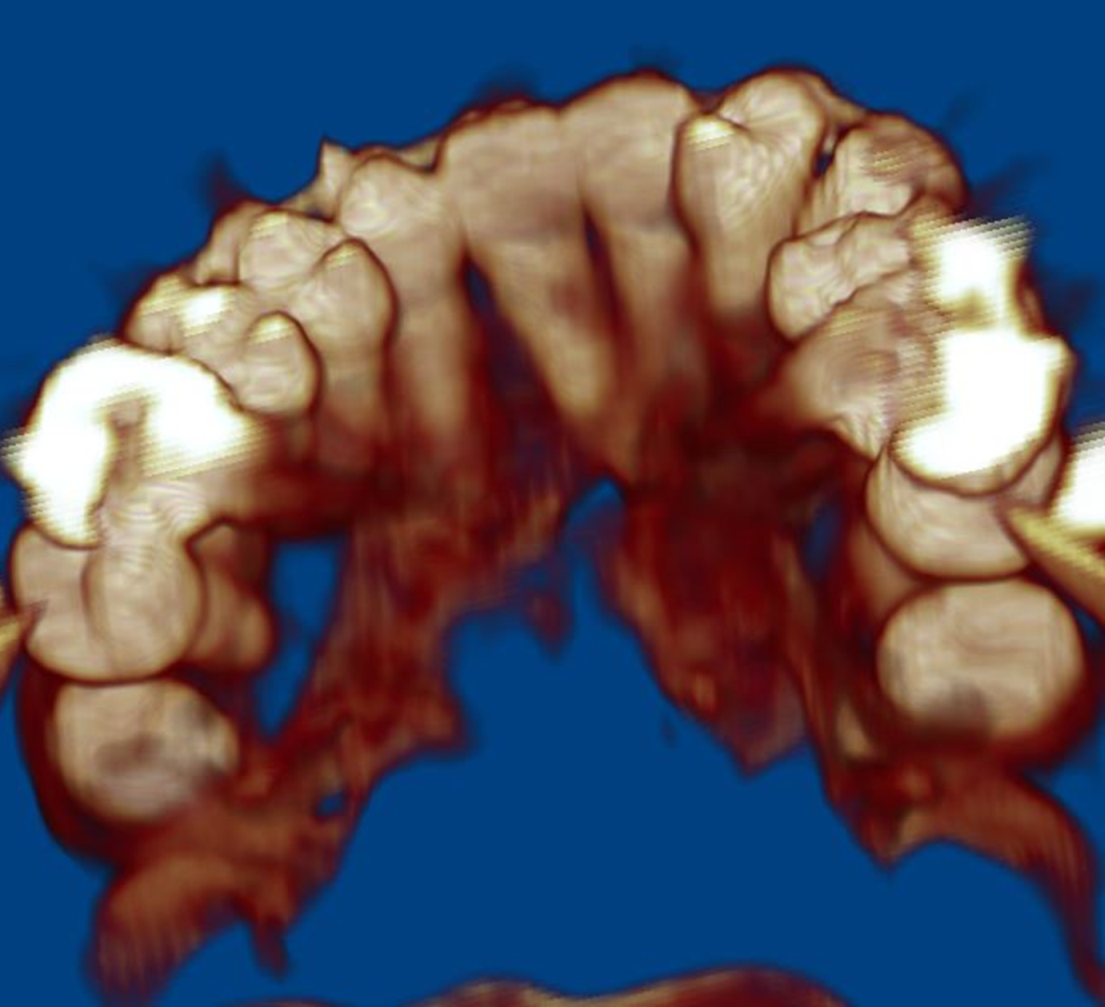
A pre-MASDO 3-dimensional computed tomography image of the maxilla (15 years 11 months). MASDO indicates maxillary anterior segmental distraction osteogenesis.
In this case, successful tooth movement was observed in the new bone created by the distraction. The space created by the MASDO procedure (7.0 mm following the consolidation phase) was completely closed bilaterally, and the patient did not require any additional prosthetic treatment. Furthermore, the molar roots showed no evidence of resorption or other issues (Figure 3C and D). Because MASDO can create the spaces required for tooth alignment, this procedure can be advantageous in cases with dental crowding.
The orthodontic tooth movement attained within the first 3 months after the consolidation phase was 7 mm. Therefore, the rate of tooth movement was approximately 2.3 mm/month. A research suggests that the rate of canine retraction in human beings is 1.1 mm/month (Janulewicz et al., 2004); hence, the rate of tooth movement in the present case was almost twice that seen under normal conditions. In general, after DO, bone turnover is considered to be accelerated (Frost, 1989). This could be explained by a regional acceleratory phenomenon, that is, the osteoclasts and osteoblasts increase via local multicellular mediator mechanisms. We therefore believe that the increased velocity of orthodontic tooth movement observed, which was influenced by accelerated bone turnover after DO (Verna et al., 2000; Verna and Melsen, 2003). Further, in the present case, we attempted a gradual mesial movement of almost 1 to 3 mm through the use of intermaxillary elastics during the consolidation period without obvious periodontal problems. This is coincident to a pilot study, the results of which suggested a possibility of tooth movement through bone regenerate during the consolidation period (Cope et al., 1999). More extensive studies are required to further investigate rapid tooth movement in the consolidation phase and the possibility of root resorption and/or periodontal complications.
Conclusions
Elongation of the maxilla with anterior distraction was shown to be effective in improving an anteroposteriorly constricted arch form and midface deficiency. Successful tooth movement in the new bone created by the distraction was achieved, which may avoid the need of the further prosthodontic treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.