
Abstract
Objective:
(1) To explore orthodontists’ perceptions of nonadherence and related factors in their patients with craniofacial conditions; (2) to examine differences in adherence perceptions by provider characteristics; (3) to evaluate current adherence interventions.
Design:
Cross-sectional.
Setting:
United States-based orthodontists affiliated with a nonprofit association for providers treating oral cleft and craniofacial conditions received survey invitations via list-serv, e-mail, and social media.
Participants:
Thirty-eight orthodontists participated (mean age = 50.5 ± 10.7 years; 76% Caucasian; 55% male; 54% private practice).
Main Outcome Measure:
An 80-item survey assessed demographic characteristics; frequencies of various adherence problems and adherence-related prolonged or terminated treatment; importance of adherence to treatment outcomes; factors that may impact adherence; interest in improving adherence; and use of adherence-enhancing interventions.
Results:
Adherence problems were common, yet 80.6% of participants rated adherence as “very important” to cleft treatment outcomes. Child behavior and motivation, caregiver reinforcement of behavior, and provider communication with the family were identified as factors that greatly impact adherence. Orthodontists in university-affiliated programs were more likely to rate individual, family, health-care system, and community factors as impacting adherence compared to private practice orthodontists; 80.6% used adherence interventions; these strategies were all rated as “sometimes successful.”
Conclusions:
Nonadherence to cleft lip/palate-related orthodontic care is common and potentially detrimental to care. Current interventions are not uniformly successful and could be better tailored. Understanding provider, patient, and family factors that affect adherence can inform individualized treatment planning to improve adherence and ultimately, treatment outcomes.
Introduction
Craniofacial conditions, including cleft lip and palate (CLP), are commonly occurring birth defects affecting the form and function of the head and face. In addition to risks for poor oral health (Wells, 2013), these conditions are associated with disruptions in tooth formation and eruption and problems with dental occlusion (Shetye, 2016). As a result, orthodontic treatment is typically an integral component of the overall habilitation of craniofacial conditions (Long and Deacon, 2009). Orthodontic treatment is frequently conducted in preparation for surgical procedures including alveolar bone grafting and orthognathic surgery (Mercado and Vig, 2009; Shetye, 2016), and it is not uncommon for youth with craniofacial conditions to undergo several courses of orthodontic treatment with each course lasting an average of 2 years (Long and Deacon, 2009).
Orthodontic treatment requires significant responsibilities for children and their families including attending frequent appointments, daily tooth brushing and maintenance of good oral hygiene, and dietary restrictions. Poor adherence to orthodontic treatment (eg, missed appointments, poor oral hygiene, broken appliances, and noncompliance with wear of prescribed elastics or removable appliances) can result in complications including decalcifications on the teeth, uncorrected malocclusion, negative psychological and social outcomes because of the appearance of their teeth and mouth, prolonged course of treatment, premature treatment termination, and wasted family and provider resources (Albino, 2000; Skidmore et al., 2006; Apajalahti and Peltola, 2007). For youth with CLP, adherence to these regimens is thought to additionally be important to the patient’s ultimate treatment outcome given that timing and completion of surgery can hinge on completion of orthodontic treatment (Mercado and Vig, 2009).
To date, exceedingly few studies have examined adherence to orthodontic treatment in craniofacial populations. Wysocka et al., 2014 examined eating habits and oral hygiene in 125 patients with CLP undergoing orthodontic treatment; 57.6% did not change their eating patterns during treatment, and only 42.7% reported changes in their oral hygiene habits.
In the general population, adherence to orthodontic treatment is also problematic, with rates of treatment termination due to poor adherence ranging from 43% to 50% (Mandall et al., 2008; Martin et al., 2017). Several studies have found that orthodontists perceive adherence as vital to orthodontic treatment outcomes (Bos et al., 2005) and believe a variety of factors contribute to adherence (eg, personality traits, motivation for treatment, maintenance of oral hygiene, communication between orthodontist and patient) (Mehra et al., 1998; Bos et al., 2005; Al Shammary et al., 2015). Interventions intended to improve orthodontic adherence and oral hygiene have been developed for use in the general population (eg, sensing devices, mobile applications, and text messaging campaigns) (eg, Epright et al., 2014; Schafer et al., 2015; Zotti et al., 2016), but it is unknown if orthodontists treating patients with craniofacial conditions use these methods in their practices.
Though findings suggest that adherence to orthodontic treatment can be problematic, the lack of empirical research about factors that may impact adherence in craniofacial populations and limited understanding of what strategies are used to improve adherence are detrimental to effectively intervening and improving outcomes. Furthermore, while some studies (eg, Bos et al., 2005) have implicated patient characteristics that may be associated with adherence behaviors, most studies have not used a theoretical framework to understand contributing patient, family, and provider characteristics.
Adherence, commonly defined as the degree to which an individual’s behavior aligns with medical advice (Haynes, 1979; Modi et al., 2012), has been studied extensively across a variety of pediatric medical conditions and related treatments (eg, type 1 diabetes) (Rapoff, 2010; Drotar, 2013). A Pediatric Self-Management Model has been developed to explain mechanisms and processes that influence adherence and health outcomes (Modi et al., 2012) and to provide a theoretical foundation for developing evidence-based interventions (see Figure 1). Accordingly, self-management is defined as the interaction of health behaviors and related processes that patients and families engage in to care for a chronic condition, and poor self-management is thought to be a contributing factor to nonadherence to treatment regimens (Modi et al., 2012). In this model, self-management behaviors operate within individual, family, community, and health-care domains (see Figure 1), and there are both modifiable (eg, treatment knowledge) and nonmodifiable influences (eg, sex) on self-management behaviors within these domains. This model, if applied to adherence behaviors in youth with craniofacial conditions, may offer a useful framework for understanding adherence problems and identifying targets for intervention.
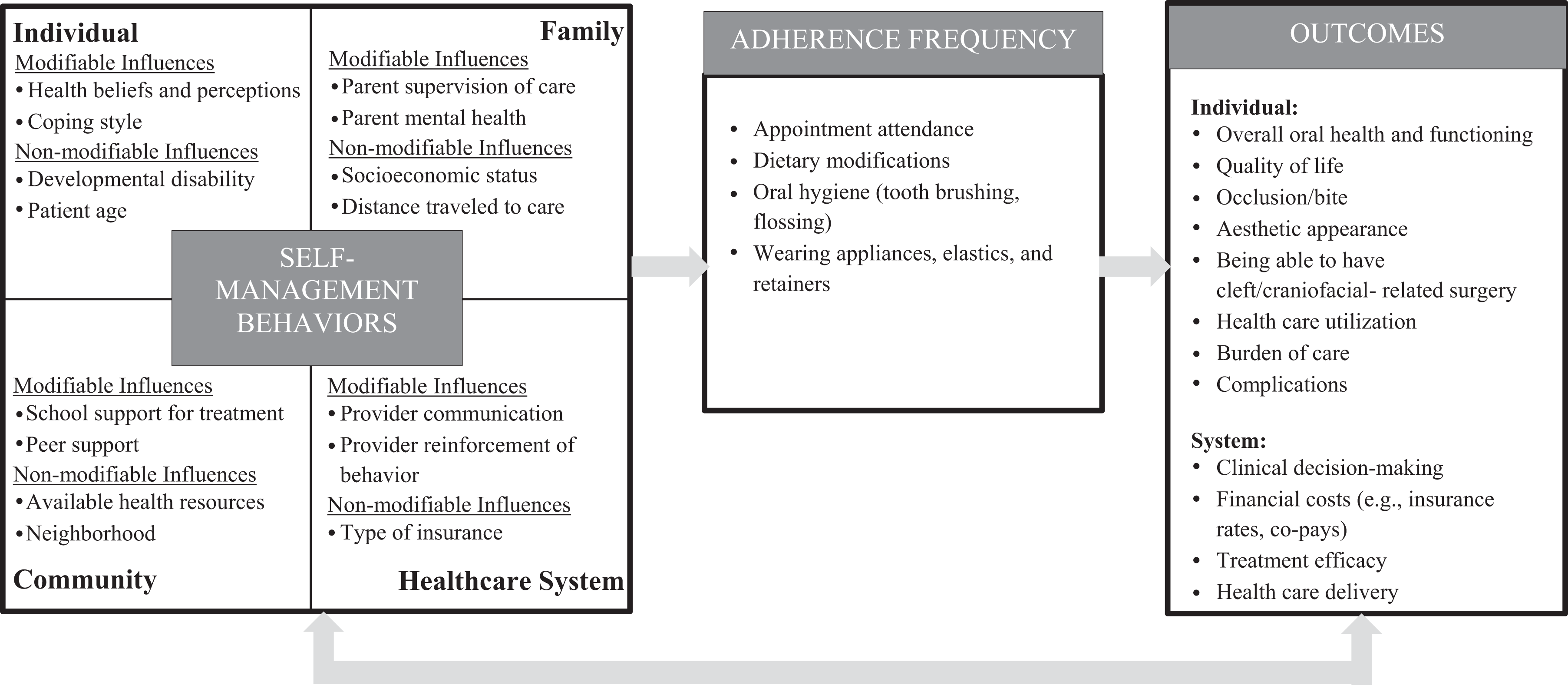
Pediatric self-management model adapted from Modi et al., 2012 for individuals with craniofacial conditions who require orthodontic treatment.
As a step toward improving our understanding of adherence to orthodontic treatment in craniofacial populations, this study explored orthodontists’ perceptions of nonadherence in their patients with craniofacial conditions and its consequences. Providers were also queried about modifiable and nonmodifiable factors from the Pediatric Self-Management Model believed to contribute to adherence problems in youth with craniofacial conditions. A secondary aim was to examine differences in perceptions of factors contributing to adherence problems by type of practice setting. A third aim was to evaluate adherence intervention strategies orthodontists currently employ in their practices along with their perceived success.
Method
Attending level orthodontists treating patients with cleft and/or craniofacial conditions in the United States who were able to complete a survey in English were eligible to participate. After obtaining Institutional Review Board (IRB) approval, several modes were used to recruit participants. An invitation and link to the survey was posted by the American Cleft Palate-Craniofacial Association (ACPA), a nonprofit of professionals who treat or research cleft and craniofacial conditions, in their online community. American Cleft Palate-Craniofacial Association orthodontists were also directly solicited via e-mail by the principal investigator. Lastly, the survey was advertised through a Facebook group for orthodontists. Orthodontists were encouraged to share the survey link with colleagues who also treated patients with craniofacial conditions.
Participants self-screened for eligibility. Prior to beginning the questionnaire, they were presented with an IRB-approved study information sheet outlining risks and benefits of participation. Beginning the survey was considered implied consent. All surveys were completed through the Research Electronic Data Capture system (REDCap), a secure web-based application (Harris et al., 2009), and estimated time to complete the questionnaire was less than 15 minutes. Subjects optionally provided their name, birth date, and address at the end of the survey to have a 10 USD incentive mailed to them. A deidentified data set was exported from REDCap for analysis to ensure subject confidentiality.
Adherence Survey
The survey developed for this study was constructed by the investigators. Content was informed by both clinical experience with craniofacial populations and an extensive review of the literature about orthodontic adherence. The survey was divided into 4 main sections. The first section assessed orthodontists’ demographic and practice characteristics. The second section assessed adherence perceptions including the following: percentage of patients who have a prolonged treatment course (eg, more than 2 years) because of poor adherence, definition of “prolonged course” (1-3 months, 3-6 months, 6-9 months, 9-12 months, greater than 12 months beyond the agreed-upon treatment end); percentage of patients who have their treatment terminated prematurely because of poor adherence. The third section assessed child, family, community, and health-care factors from the Pediatric Self-Management Model which may impact adherence (see Figure 2). Participants used a 3-point Likert scale (not at all to a great deal) to indicate how much each factor contributed to adherence. The fourth section assessed types of adherence problems (yes/no) encountered including broken brackets; no shows, frequently cancelled appointments, poor hygiene, poor motivation, lack of patient/family knowledge about orthodontic care, poor cooperation during visits, unrestored decay, recurrent decay, and poor use of removable treatment adjuncts (eg, head gear, elastics, bite planes). Participants could also detail other problems not already listed. In the final section, participants were asked to identify what strategies they use to enhance adherence, if any, from a list of common interventions (eg, offering small rewards or incentives, appointment reminders, charging money for broken brackets/wires/bands, reviewing oral hygiene with patient) and how successful they think the strategy is on a 5-point Likert scale (not at all successful to very successful). Participants could also write in other strategies utilized not already mentioned on the survey. Finally, they were asked to rate how important adherence to orthodontic treatment is to obtaining good overall treatment outcome for the patient’s cleft/craniofacial condition (4-point Likert scale ranging from not at all important to very important); their interest in learning about ways to improve adherence (3-point Likert scale ranging from not at all interested to very interested); and ways that nonadherence affects providers and their practices as well as patients and families (eg, lost time, lost money, professional burnout).
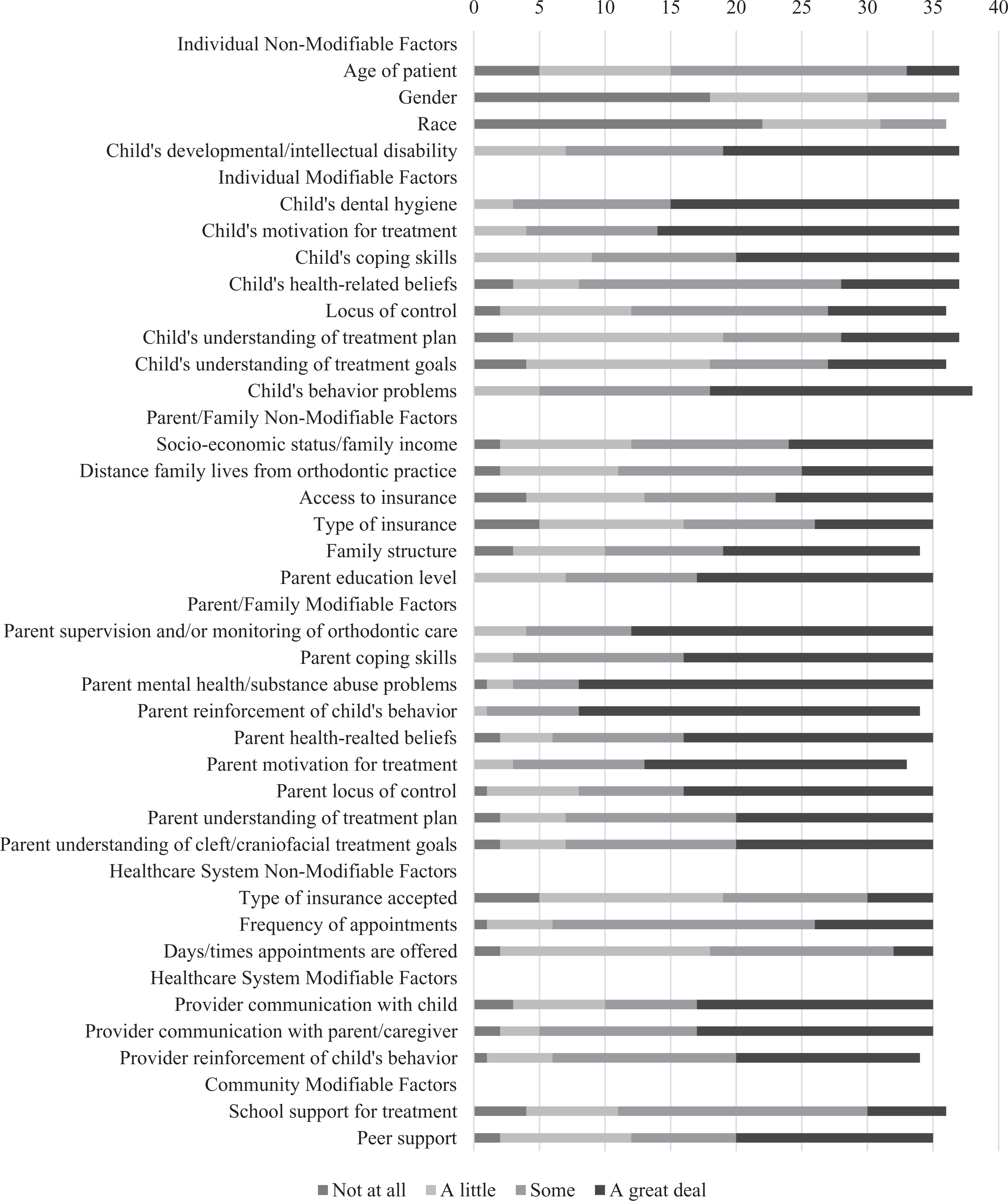
Individual, family, health-care system, and community factors contributing to nonadherence.
Statistical Analyses
SPSS version 24 (IBM Corp, Armonk, New York) was used for all analyses. Demographic descriptions of the sample and their treatment populations were first prepared. For the first 2 aims, means (standard deviation) or frequencies (%) were calculated for frequency of adherence problems; types of adherence problems; frequency of patients with prolonged or terminated treatment course due to poor adherence; perceived importance of adherence, individual, family, health-care system, and community factors that may influence adherence; interest in improving adherence; and consequences for patients and practices of nonadherence. Chi square or Fisher exact tests and Mann-Whitney U tests were used (as appropriate) to evaluate differences in adherence perceptions and strategies by provider demographics (practice type and sex). Addressing aim 3, frequencies (%) were calculated for use of adherence-enhancing strategies, types of adherence strategies used, and success of adherence strategies.
Results
Demographic Characteristics
Table 1 presents demographic, practice, and patient characteristics for the 38 orthodontists who completed the survey. The majority of participants were recruited via the ACPA Online Community (73.7%, n = 28), and most had been practicing for 15 years or more (63%, n = 24). The mean age of the respondents was 50 years. Fifty-five percent (n = 21) were male, and most of the sample identified as Caucasian and non-Hispanic.
Sample Demographic and Practice-Related Characteristics.
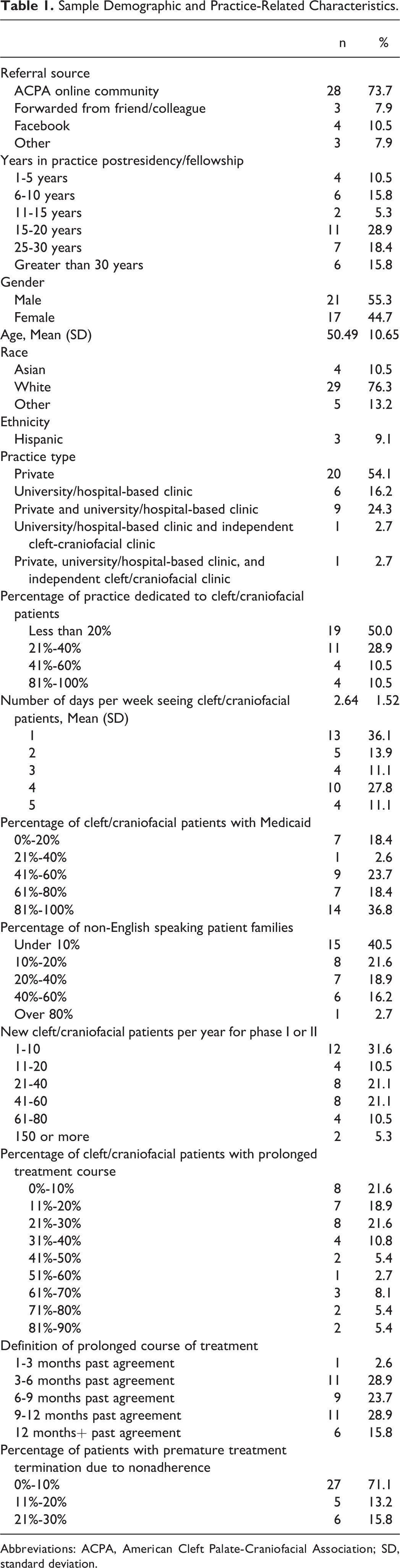
Abbreviations: ACPA, American Cleft Palate-Craniofacial Association; SD, standard deviation.
Over half of the sample (54%, n = 20) was based in a private practice setting, and 29.7% (n = 17) reported that they had some affiliation with a university or hospital-based clinic. Half of the sample (n = 19) reported that 20% or less of their practice was dedicated to patients with cleft or craniofacial conditions. The majority of providers reported that their patients were primarily English speaking. As shown in Table 1, about half of the sample (n = 21) reported that 60% or more of their patients with craniofacial conditions have Medicaid insurance. Nearly a third of providers (n = 12) reported having 10 or fewer new cleft/craniofacial patients per year for phase I or II orthodontics, although providers with a range of patient volumes were represented in the sample.
Prolonged Treatment Definition and Rate of Treatment Termination due to Nonadherence
As shown in Table 1, there was diversity in how orthodontists defined a prolonged treatment course, though most commonly providers defined a prolonged course as 3 to 6 months (28.9%, n = 11), 6 to 9 months (23.7%, n = 9), or 9 to 12 months (28.9%, n = 11) beyond the agreed treatment end. With respect to adherence-related treatment termination, 71.1% (n = 27) observed termination 10% or fewer of their patients; however, 15% (n = 6) reported that termination occurred in 21% to 30% of their patients.
Types of Adherence Problems
All orthodontists reported observing adherence problems in their craniofacial patient populations. Poor hygiene was the most commonly observed (100%, n = 35), followed by broken brackets, bands, or wires (97.2%, n = 35); no shows for appointments (94.3%, n = 33); and frequently cancelled appointments (88.9%, n = 32). Recurrent and unrestored decay were also common (79.4%, n = 27 and 73.5%, n = 25 respectively), as well as low patient/family motivation (76.5%, n = 26) and patient or family lack of knowledge about orthodontic care (70.6%, n = 24). About half of orthodontists (47.1%, n = 16) endorsed poor cooperation during appointments. Other adherence-related problems cited by orthodontists included delays in securing appointments for their patients with oral surgeons or general dentists, poor parent cooperation with treatment plan, and language barriers.
Use of Adherence-Enhancing Strategies and Perceived Success
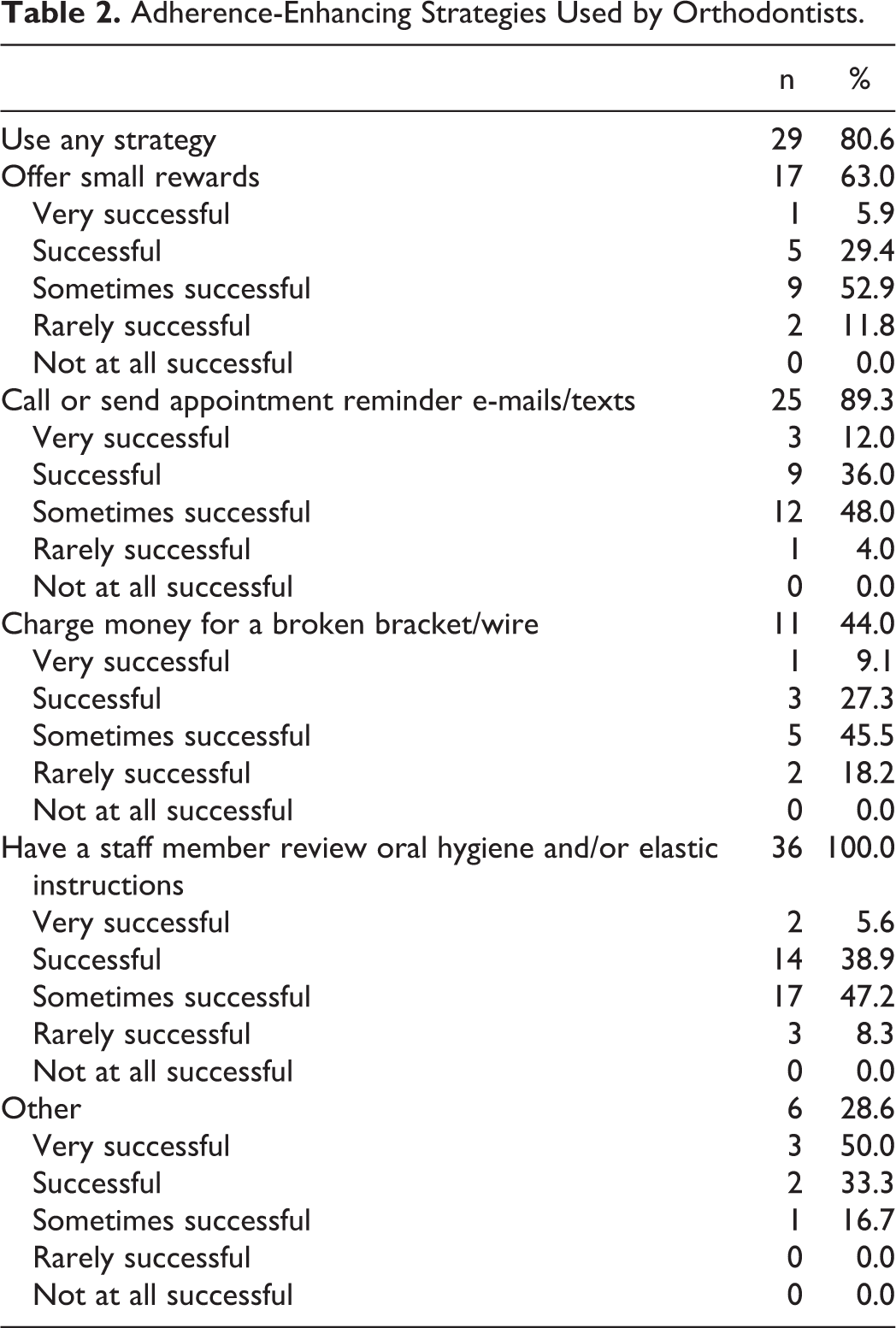
Table 2 presents the strategies orthodontists used to enhance adherence along with the perceived successfulness of each strategy. The majority (80.6%, n = 29) reported using some type of adherence strategy, most commonly having a staff member review oral hygiene and/or elastic instructions (100%, n = 36); calling or sending appointment reminder e-mails or texts (89.3%, n = 25); offering small rewards (63%, n = 17); and charging a fee for broken brackets or wires (44%, n = 11). As shown in Table 2, perceptions of success varied for each strategy, with the most common response being “sometimes successful” for all strategies. Other strategies orthodontists shared included requiring Medicaid patients to accept special terms for treatment (a signed memorandum of understanding, nonpeak hour appointments, adherence-related dismissal); fees for more than 3 broken or no-show appointments; calls to the patient’s dentist regarding adherence concerns; review of progress photos and goal setting with the patient in advance of craniofacial team appointments; and having older patients with cleft/craniofacial conditions mentor younger patients during their active treatment. Direct, clear provider communication with the patient and parent were mentioned by 2 providers including careful review of reasons for treatment and treatment expectations; updates on treatment progress and time to completion; and emphasis on follow-up after active treatment and its relationship to team care.
Adherence-Enhancing Strategies Used by Orthodontists.
Individual, Family, Health Care, and Community Factors Affecting Adherence
Figure 2 provides data about orthodontists’ perceptions of the degree that individual, family, health care, and community factors as described by the Pediatric Self-Management Model (Modi et al., 2012) contribute to nonadherence. Both modifiable and nonmodifiable factors were endorsed, although overall, more modifiable child, family, health care, and community factors were deemed as contributing “some” or “a great deal.” Nonmodifiable factors from the individual domain thought to have some or great impact on adherence were child’s developmental or intellectual disability (81.0%, n = 30) and patient age (59.4%, n = 22), whereas gender and race were not endorsed as having significant impacts on adherence. Modifiable individual domain factors selected as having some or great impact on adherence were the child’s dental hygiene (91.9%, n = 34); motivation for treatment (89.2%, n = 33); behavior problems (86.8%, n = 33); and coping skills (75.6%, n = 28).
In the family domain, nonmodifiable factors were more frequently endorsed than in the individual domain, though modifiable factors were still perceived as having greater impact on adherence. Nonmodifiable factors like family structure, parent education level, socioeconomic status, distance traveled by families for appointments, and access to insurance were endorsed as having some or great impact on adherence by 62.6% to 80.0% of the sample (n = 19 to n = 28). Several modifiable factors were perceived to have some or great impact on adherence including parent reinforcement of child’s behavior (endorsed by 97.1%, n = 33), parent mental health or substance abuse problems (91.4%, n = 32), parent coping skills (91.4%, n = 32), parent motivation for treatment (90.9%, n = 30), and parent supervision and/or monitoring of orthodontic care (88.6%, n = 31).
In the health-care system domain, orthodontists rated modifiable factors including provider communication with the parent or caregiver (85.7%, n = 30), provider reinforcement of the child’s behavior (82.4%, n = 28), and provider communication with the child (71.4%, n = 25) as having some or great impact on adherence. For nonmodifiable factors, frequency of appointments was rated as having some or great impact by 82.8% (n = 29) while type of insurance accepted was rated as having little or no impact by 54.3% (n = 19). Finally, in the community domain, 2 modifiable factors were identified as impacting adherence including school support for treatment (endorsed by 52.8%, n = 19 to have some impact) and peer support (endorsed by 42.9%, n = 15 to have great impact).
Provider Demographics and Adherence
No significant differences were found by practice type (private vs. university-affiliated) with respect to types of adherence problems experienced (as described above). However, as shown in Table 3, perceptions of modifiable and nonmodifiable individual, family, community, and health-care system factors that may affect self-management and adherence differed significantly between private versus university-affiliated orthodontists for these factors, such that orthodontists affiliated with universities reported significantly greater impacts on adherence compared to those in private practice for the following factors: child intellectual/developmental disability, locus of control, and understanding of craniofacial treatment goals; distance family lives from orthodontic practice; parent–child interactions; parent mental health/substance abuse, reinforcement of child’s behavior, health-related beliefs, motivation for treatment, locus of control; days/times appointments are offered; and school support for orthodontic treatment. For use of adherence enhancing strategies, those in private practice were significantly more likely to use small rewards to incentivize adherence than those in practices affiliated with universities (100%, n = 12 vs 35.7%, n = 14, P = .001).
Perception of Degree That Factors Contribute to Adherence by Practice Type.a
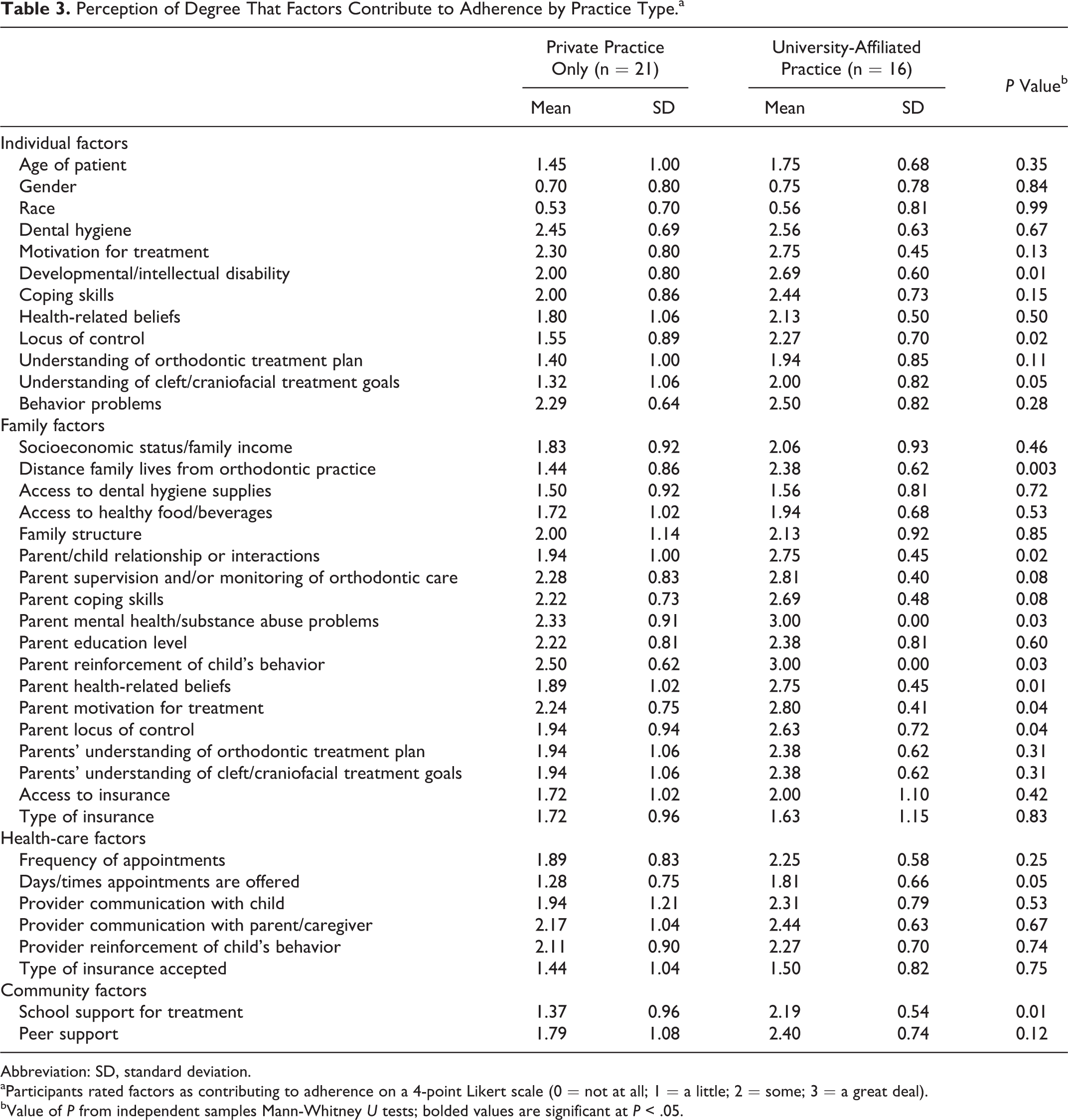
Abbreviation: SD, standard deviation.
aParticipants rated factors as contributing to adherence on a 4-point Likert scale (0 = not at all; 1 = a little; 2 = some; 3 = a great deal).
bValue of P from independent samples Mann-Whitney U tests; bolded values are significant at P < .05.
Impact of Nonadherence on Treatment, Patients, and Providers
Table 4 summarizes participant responses with respect to the impact of nonadherence on treatment outcomes, providers, and patients/families. The majority of the sample (80.6%, n = 29) rated adherence as being “very important” for a patient to obtain a good overall treatment outcome for their cleft or craniofacial condition. No providers rated adherence as being unimportant or unrelated to treatment outcomes. Over three-fourths reported being interested in learning about adherence-improving strategies. Lost time, feelings of frustration, lost money, and disruption to clinic routine/flow were seen as the main negative impacts on providers. Over a third (n = 13) reported that adherence problems contribute to feelings of professional burnout. Adherence problems were also rated as being detrimental to patients and families, with lost time, feelings of frustration, poor orofacial aesthetics, and uncorrected problems with the child’s bite being cited as problematic by the majority of orthodontists. Other consequences of nonadherence included staff developing negative feelings toward patients with Medicaid insurance; less time to care for noncleft patients due to extra time required for cleft care preparation; delayed or indefinitely postponed treatment (eg, surgery); loss of benefits before treatment is complete; and undermined relationships with families who do not accept personal responsibility for nonadherence. Participants identified additional impacts of poor adherence on patients and families, including affecting outcomes of dental implants and restorative and esthetic treatments and poor oral hygiene leading to caries and periodontal disease.
Impact of Nonadherence on Treatment, Patients, and Providers.

Discussion
This is the first study to our knowledge to survey orthodontists who treat patients with craniofacial conditions about their experiences and perceptions of orthodontic treatment-related adherence. Of note, there was no clear consensus about how to define a prolonged course of treatment, although most thought that at a minimum, 3 months beyond the agreed upon end of treatment constituted a prolonged course. However, a minority (15.8%) defined this as treatment extending a year or more past the agreed-upon end date. With respect to treatment termination due to poor adherence, while the majority (71%) reported that this occurred in fewer than 10% of their cases, 29% reported that it occurred more regularly (between 11% and 30% of patients). By comparison, Mehra et al. (1998) reported that 95% of orthodontists (n = 420) prematurely terminated treatment due to adherence problems in less than 5% of their patients from the general population, with a minority (5%) reporting early termination in 5% to 10% of patients. Our findings suggest that adherence-related treatment termination may be more common among patients with craniofacial conditions, although more empirical study is warranted.
Consistent with studies in craniofacial (Paynter et al., 1993; Wysocka et al., 2014; Crerand, et al., in press) and general populations (Mehra et al., 1998; Bos et al., 2005; Al Shammary et al., 2015), all orthodontists surveyed reported adherence problems, including challenges with oral hygiene, missed appointments, and broken bands, wires, and brackets. Low motivation for treatment was cited by 76%. As patients with craniofacial conditions frequently undergo several courses of orthodontic treatment, motivation levels may wane over time or patients may experience burnout with treatment. Strategies that target motivation may be indicated (Lalic et al., 2012).
The majority of orthodontists surveyed use adherence-enhancing strategies, most commonly, review of oral hygiene or elastic wear instructions, appointment reminders via text or e-mail, small rewards for adherence, and fees for broken brackets or wires. However, success ratings mostly fell in the “sometimes successful” range. The success of a particular intervention likely depends on its match with the adherence problem being experienced (eg, reminder calls may not help in the case of a patient with poor motivation for treatment). To successfully tailor interventions, orthodontists may need to implement a variety of strategies.
Orthodontists largely identified modifiable factors across domains of the Pediatric Self-Management Model as potential contributors to adherence problems. Within the individual domain, the child’s motivation for treatment, behavior problems, dental hygiene, and coping skills were all rated as greatly contributing to adherence suggesting that these areas may intervention targets. Hygiene programs (Brasil et al., 2007) or collaboration with a psychologist who can address motivation, behavior problems, and coping skills may be indicated. Patients’ age and presence of an intellectual or developmental disability were noted as nonmodifiable factors. Other studies have noted that adherence may become more difficult over time and as children progress through adolescence (eg, Albino, 2000). As such, interventions for adolescents may be indicated particularly given that they likely assume more responsibility for oral hygiene and adherence to treatment. As one orthodontist noted, peer support from older youth who have been through the treatment process may be helpful. More specialized approaches may be indicated for youth with developmental or intellectual disabilities (eg, behavior therapy).
Similarly, in the family domain, parent’s mental health, beliefs, treatment motivation, supervision of orthodontic care, coping skills, and understanding of the treatment plan were believed to highly influence adherence. These findings suggest that interventions may need to target parental motivation, expectations, and behaviors (eg, monitoring of child’s oral hygiene). In the case of parent mental health problems, coordination with social workers and/or psychologists may be indicated to provide support and address adherence barriers. Access to and type of insurance were also identified as impacting adherence. In the general population, Medicaid insurance has been associated with nonadherence (Horsley et al., 2007; Wilson and Harris, 2015) although other studies have found no differences (eg, Dickens et al., 2008).
With respect to health-care system factors, provider communication with patients and caregivers and their reinforcement of the child’s behavior were rated as significantly influencing adherence. Interventions could target these areas (eg, developing patient/family orthodontic education programs). Within the community domain, peer support and school support were reported as contributing to adherence. These factors may reflect new areas for intervention (eg, developing peer mentors, evaluating school support for attending appointments and/or adhering to oral hygiene, and dietary restrictions).
There were some significant differences in perceptions of factors (both modifiable and nonmodifiable) based on practice type, with university-affiliated orthodontists reporting greater impact of individual, family, health-care system, and community factors on adherence than those based in private practice. These findings could reflect differences in the patient populations and/or their socioeconomic diversity. For example, university-affiliated orthodontic practices may also see children with other special health-care needs (hence rating presence of an intellectual disability/developmental disability as having more of an impact). Similarly, distance to the clinic may be a factor if families have to travel for specialized orthodontic care. These differences suggest that it may be important to consider practice location in developing and tailoring adherence interventions.
The majority of orthodontists rated adherence as “very important” to the patient’s overall treatment outcomes, and all but one orthodontist reported interest in learning about strategies to improve adherence. Adherence problems impact providers, particularly with respect to lost time and money. Frustration was noted as a consequence for patients, families, and providers alike, with feelings of professional burnout expressed by over a third of providers. For patients, poor orofacial aesthetics and functioning were also noted as consequences of poor adherence. These findings underscore interventions are needed to address adherence problems as their impact may be felt not just by patients and families, but by providers as well.
Limitations and Future Directions
The current study is limited by the cross-sectional design, modest sample size, and reliance on a provider-report survey which was developed specifically for this study. Further, we assessed provider perceptions which are inherently subjective as opposed to obtaining archival data about practice characteristics, actual rates of adherence problems, and use of adherence-enhancing strategies. However, the survey was informed by the extant literature, clinical expertise with the craniofacial population, and a theoretical model. Prospective studies should assess adherence and self-management behaviors in youth with craniofacial conditions as well as the impact of adherence on orthodontic and overall craniofacial treatment outcomes (eg, patient reported satisfaction with appearance, oral health, quality of life). Additionally, studies utilizing direct assessments of adherence are needed (eg, oral hygiene assessments, wear time for appliances) given that patient or caregiver self-report can be subject to bias and/or impression management. Orthodontic and related craniofacial treatment can impose significant burdens on families (eg, travel for appointments, financial cost) (Cassell et al., 2014), and a better understanding of the financial implications and the burden of care as they relate to adherence is needed. This study is also limited by a lack of patient or family-reported data about their orthodontic treatment experiences. Mixed methods studies (eg, qualitative interviews and surveys using psychometrically sound instruments) are needed to better understand factors that impact adherence to orthodontic care and ways to enhance patient, family, and provider experiences. Finally, although orthodontists who took part in the survey represented a variety of practice settings, the majority worked in private practices and had relatively low volumes of patients with craniofacial conditions which may limit the generalizability of the findings to other settings (and to those with more craniofacial experience).
Our findings have implications for both screening and intervention development. Factors identified in this study could be used during pretreatment screening to predict risk for poor adherence. Approximately 20% of surveyed orthodontists did not use any interventions, and the majority of the sample was interested in learning additional strategies. Accordingly, tailoring interventions or developing assessments to pinpoint specific areas of adherence risk may be indicated. Orthodontists’ responses about factors that contribute to adherence suggested new targets for intervention (eg, increasing peer or school support) that have yet to be systematically studied. While interventions have been developed (eg, mobile phone apps, reminders for tooth brushing), there is a need to either develop or systematically apply interventions to improve adherence in craniofacial populations.
Conclusions
This study documented orthodontists’ perspectives on adherence-related problems in patients with craniofacial conditions. Adherence problems were universally reported in this sample. Interventions are frequently used to improve adherence but with varied effectiveness. Modifiable influences on self-management behaviors were endorsed in individual, family, health-care systems, and community domains and may aid with assessing risks for poor adherence and tailoring and developing interventions to improve adherence for youth with craniofacial conditions.
Footnotes
Authors’ Note
Data contained in this manuscript was presented orally at the 75th Annual Meeting of the American Cleft Palate-Craniofacial Association, Pittsburgh, Pennsylvania; April 2018.
Acknowledgment
Authors acknowledge Drs Ana Mercado and Michelle Scott who reviewed content of survey items.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.