
Abstract
Objective:
Maintaining and improving patients’ quality of life (QOL) are regarded as the most important aims in health-care systems. These are directly associated with intervention of health-care providers across the world. The aim of the present study was to evaluate the impact of teamwork on frequency of care provided to children with cleft lip and palate and their mothers’ QOL.
Methods:
This analytical epidemiology study was conducted on 101 children with cleft lip and palate and their mothers who were divided into 2 groups: a multidisciplinary team and a group of individual providers. Data were collected using convenience sampling. Quality of Life Questionnaire (Short Form-36) was assessed. The statistical analysis was performed using the χ2 test, independent t test, and Mann-Whitney U test in SPSS (20).
Results:
Both groups were matched. There was a significant statistical difference among the members of multidisciplinary team who received surgery, genetic counseling, and dental care (P ≤ .043) and the individual providers groups. The 2 groups did not have significant difference in receiving the hearing test, speech therapy, and dental care 12 months before the interview. There were significant differences in QOL scores between the multidisciplinary team and the group of individual providers (P = .013).
Conclusions:
The services provided as a multidisciplinary team leads to a better outcome and improves the QOL of our patients and their families. It is recommended that services should be provided in the team approach for patients with cleft lip and palate.
Introduction
Cleft lip and palate is a common craniofacial anomaly being prevalent 1 in 711 live births (Noor and Musa, 2007). Children with cleft lip and palate experience various difficulties during the course of growth in different areas, and a heavy burden is incurred on their health, quality of life (QOL), and socioeconomic well-being as well as on their families (Wehby and Cassell, 2010). The quality of family life of these patients may be reduced due to increased financial and personal and social costs associated with the management of medical and nutritional issues for their children (Kramer et al., 2007). Accordingly, patients with cleft lip and palate need a wide range of care for more than several years (Semb et al., 2005). Consequently, treatment unification and efficacy for these patients is of great importance and is highly expected to happen in any well-organized and unified cleft palate team (Furr et al., 2011).
A cleft palate team includes the patient, their family, and a group of specialists, including an audiologist, a pediatric dentist, a geneticist, a neurosurgeon, an ophthalmologist, a nurse, an oral surgeon, an orthodontist, an otolaryngologist, a pediatrician, a plastic surgeon, a prosthodontist, a psychologist, a social worker, a speech and language pathologist, and a team coordinator working collaboratively to provide medical care and treatment for the patient (Peterson-Falzone et al., 2006; Kasten et al., 2008; Kummer, 2008). The teamwork treatment for patients with cleft palate has been widely accepted in most regions of the world as a standard approach (Louw et al., 2006; Furr et al., 2011). One of the advantages of this approach is that it can provide unique opportunities for parents to receive more information from doctors about their children’s health. Through establishing a close relationship with an interdisciplinary team of specialists, parents can alleviate their parental concerns regarding their children’s health and the treatment required to cure their children (Peterson-Falzone et al., 2001). In a teamwork approach, a comprehensive evaluation is carried out by specialists who work together and know each other’s field.
Protecting and improving patients’ lives is one of the most important objectives of health-care organizations in every society. In effect, enhancing the QOL for patients is deemed to be directly associated with services and treatments provided by health-care systems (Mir et al., 2012). In the meantime, it seems that comparing the results of group treatment and individual treatment of children with cleft lip and palate is a significant issue due to the fact that the QOL of families of these children is reportedly low because of the pressure caused by extra financial, personal, and social costs of nutritional and medical management of the disease (Semb et al., 2005; Furr et al., 2011). Team treatment of cleft palate is an approach recently adopted for the treatment of children with cleft lip and palate. This team treatment is only in 2 provinces of Iran namely, Esfahan and Fars, so this study is intended to compare the QOL of those children with cleft lip and palate who received teamwork treatment services with that of those children who received treatment individually and independently.
Methods
This analytical epidemiological study was carried out on 101 mothers who had children with cleft palate, cleft lip, or cleft lip and palate with the average age ranging from 2 to 7 years old. To identify the participants for the study, convenience sampling technique was used. In effect, in order to identify the mothers of children who were in the treatment team in Shiraz, the files and records of the patients with cleft lip and palate were studied. The treatment of children of the team members was done in a coherent form in a specialized skilled team of the Shiraz University of Medical Sciences. The children treatment process of cleft team members was pursued in an interdisciplinary team in which a group of professionals worked together in an integrated and coordinated manner. Team members held joint meetings to discuss and decide on the child’s assessment and treatment processes, and the ultimate child care and treatment program was followed up at joint meetings after a survey by all experts.
Similarly, to identify mothers with children who had cleft lip and palate, but were not members of any treatment team, we visited speech therapy clinics and otolaryngology Ear, Nose, Throat (ENT) offices in Ahvaz, where they were receiving treatment for their children individually and independently. Thus, the samples for this study were selected based on several inclusion and exclusion criteria. Mothers whose children were not members of the team, received treatment in a haphazard manner without general coherence. For these non–team children, there was no referral to specialists who have established specific, stable relationships and cooperation with each other. Experts from different fields did not have direct contact with each other, and referral to each specialist was carried out separately, not on the basis of a comprehensive and targeted referral plan to a group of specialists. In fact, the process of treating children of non–team members was managed as a multidisciplinary team. In this team, each of the professionals, assessed and treated the children independently, and there was no consistency between the information and the advices of different experts.
The inclusion criteria were willingness of parents to participate and acquiring the score 1 SD above the mean score in the parental stress scale to homogenize the studied participants.
Moreover, the parental stress scale was used to homogenize the samples. This was a self-report tool with 18 items, each item representing enjoyable, positive, and negative themes of parenthood. In the scale, 8 positive items are scored inversely, higher scores indicating higher stress. This scale was used to evaluate parental stress in clinical and nonclinical population. Its validity was calculated using Cronbach α, equaling 0.83. Its internal reliability was found to be from 0.84 to 0.56.
The exclusion criteria were mothers with children who had microtia, craniosynostosis, genetic, or chromosomal disorders (Dott et al., 2010; Rasmussen et al., 2003; Austin et al., 2010).
Having selected the participants, we gathered information about mothers’ age, income, education status, services, and the kind of child care (including speech therapy, hearing test, dental care, and genetic counseling) their children had already received. Then, their QOL was evaluated by the Quality of Life Questionnaire including 36 questions (SF-36). The questionnaire was first translated into Persian by Montazeri et al. (2005) under the supervision of International Quality of Life Assessment. Its Cronbach α changes were found to be in the range of 0.77 and 0.9, and its reliability was calculated as 0.65 (Montazeri et al., 2005). The questionnaire included 36 questions and 8 subscales each having 2 to 10 participants. The subscales are physical functioning (PF), role-limitation physical (RP), role-limitation emotional (RE), energy/vitality, emotional welfare (EW), social functioning (SF), pain (P), and general health (GH). Moreover, 2 overall subscales of physical health and mental health were obtained by combining other subscales. Physical health subscales are as follows: general health, physical functioning, pain, energy/vitality. Mental health subscales are as follows: social functioning, role-limitation physical, role-limitation emotional, emotional welfare. Each question had 0 (the lowest score) to 100 score (the highest score). A score was assigned to each individual based on their answer to each question. By calculating the sum of each individual’s scores for all questions, their mean score related to that scale was obtained. Receiving a lower score in the questionnaire by the mothers indicated a lower QOL and vice versa.
The data garnered throughout this study were analyzed by the independent t test to compare the average scores of QOL in the 2 groups, namely, the mothers of children with cleft lip and palate who were in the teamwork treatment and those mothers who were not part of any teamwork treatment. The significance level was set at 0.05, and the analyses were performed using SPSS (version 20). Moreover, to compare the variables’ frequency, the χ2 test was used.
The current study has a code of ethics IR. AJUMS.REC.1394.276 from the ethics committee of Ahvaz Jundishapur University of Medical Sciences.
Results
The current study involved 101 mothers whose children had cleft palate, lips, or palate and lips. Table 1 shows the demographic characteristics of mothers and their children. Variables such as sex, cleft type, mother’s education, income, maternal, and child’s age were compared for the participants of the 2 groups (team members and nonteam members) using χ2 and independent t tests. Statistical analysis showed that there was no significant difference between demographic variables in this 2 groups (Table 1; at the time of the study, the income below 1 million Tomans, in Iran, approximately 300 USD, was considered to be below the poverty threshold). Participants of the 2 groups (team members and non–team members) were compared in terms of the amount of benefit and use of health services. Services that were studied in 2 groups included: a hearing test in the last 12 months, the number of surgeries, speech therapy, genetic counseling, and having dental care in the last 12 months.
Demographic Features of the 2 Groups (Teamwork Treatment Group and Non–Teamwork Treatment Group).
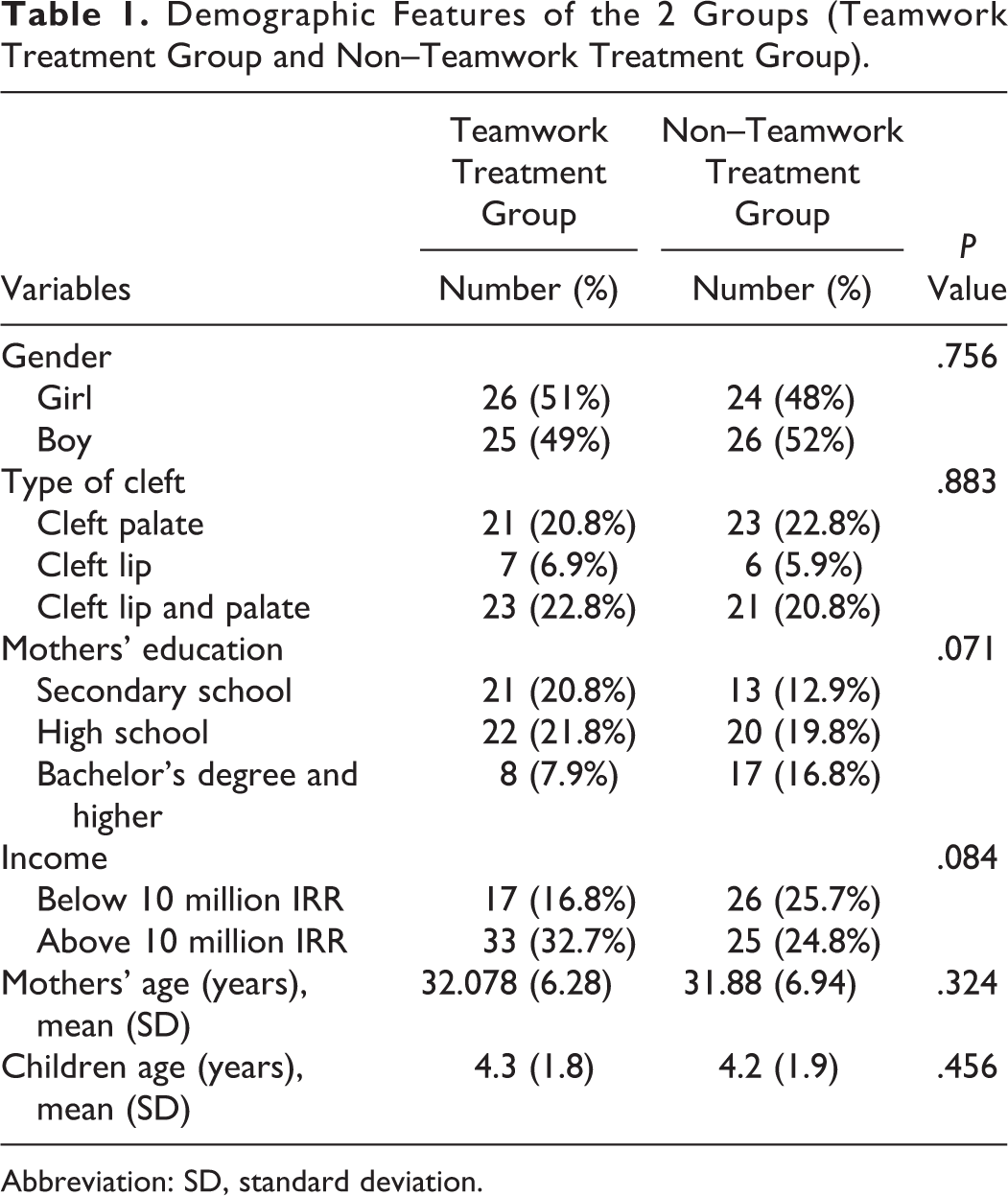
Abbreviation: SD, standard deviation.
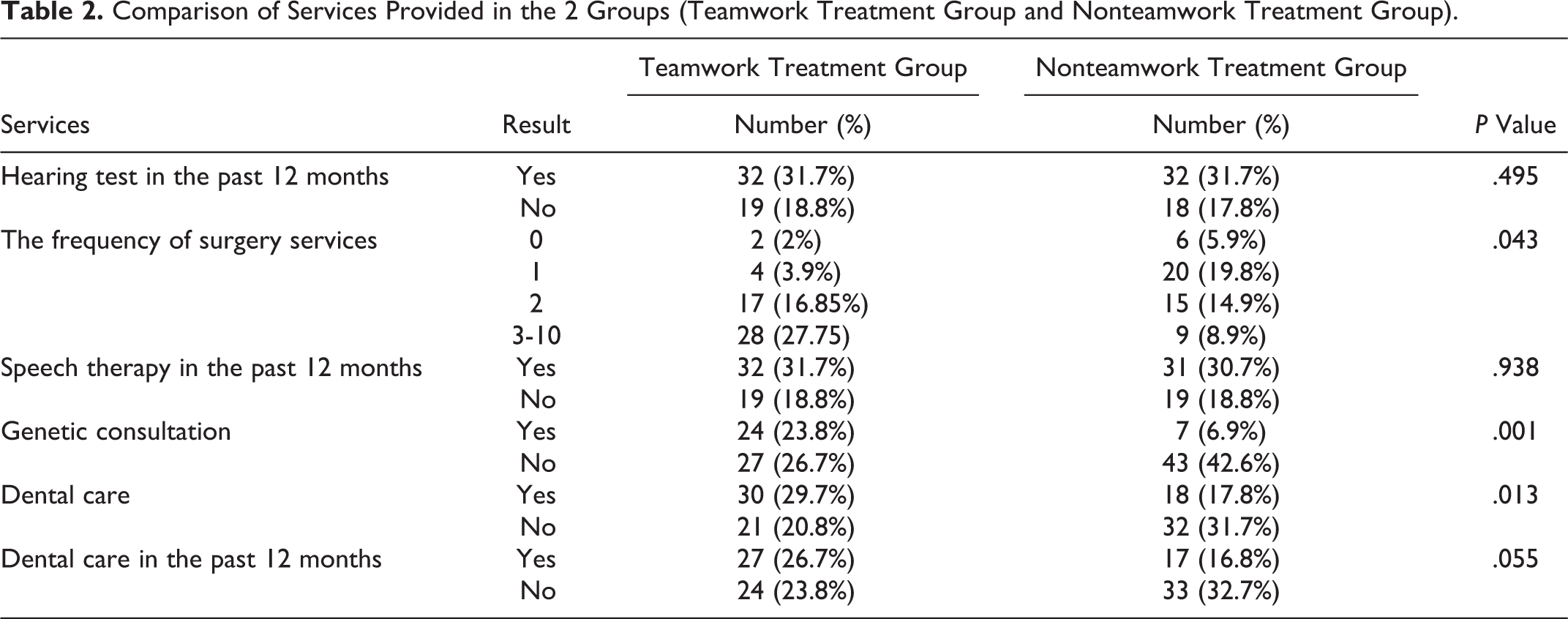
Statistical analysis showed that there was a difference between team members and non–team members in terms of the frequency of receiving services in the number of surgery, genetic counseling, and dental care. However, there was no significant difference between the 2 groups in terms of frequency of receiving services in the hearing test, speech evaluation, and dental care in the last 12 months before the study (Table 2).
Comparison of Services Provided in the 2 Groups (Teamwork Treatment Group and Nonteamwork Treatment Group).
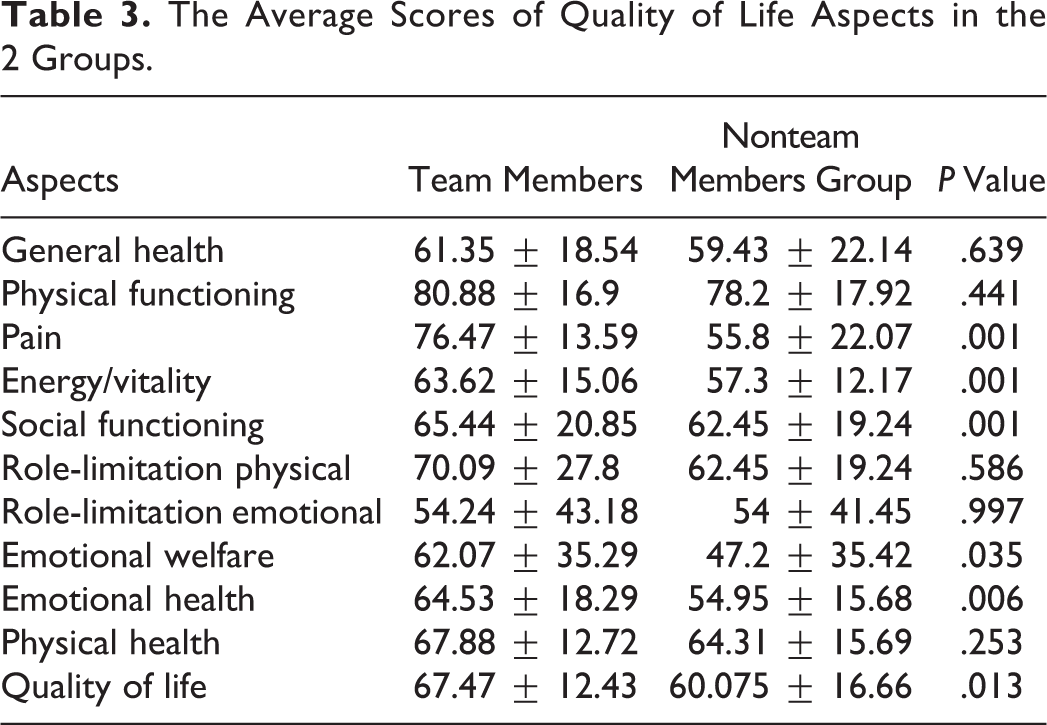
After assessing the QOL of the participants using the SF-36 Quality of Life Questionnaire, the data distribution of the 2 groups was reported normal based on the Kolmogorov-Smirnov test. The mean scores in 2 groups were compared for 8 subscales of QOL questionnaire based on the independent t test (Table 3). The statistical analysis showed that there was a significant difference between the 2 groups in terms of the mean scores in the items of pain, energy/fatigue, emotional well-being, the mental health variable, and QOL. There was no significant difference between the participants of the 2 groups in the mean scores of general health, physical function, social function, physical health, role-limitation physical, and role-limitation emotional.
The Average Scores of Quality of Life Aspects in the 2 Groups.
Discussion
This study was conducted to investigate the influence of teamwork treatment on the frequency of services provided to children with cleft lip and palate and also its effect on the QOL of their mothers. To that end, 101 children with cleft palate, lip, or both along with their mothers participated in the study.
According to Table 2, the results showed that the number of children who had a hearing test before the interview in the last 12 months were 32 participants in both team and non–team members groups (P = 0.495). The result showed no significant difference between the 2 groups in taking hearing tests in the past 12 months before the interview session. This finding is not in line with that of Austin et al. (2010). Since the cleft palate team in Iran is new and there is not enough executive experience, the results of teamwork and non–team work in the field of hearing tests are the same.
The results of this study showed that the number of children who had speech therapy sessions before the study in the last 12 months was 32 in the team members group and 31 in nonteam members group (P = .938). This finding also showed no significant difference in the speech therapy of the team and non–team members, which conforms to the findings of Austin et al. (2010) which were based on receiving speech therapy services between team and non–team members. Accordingly, it seems that speech therapy is more acceptable (more known) than other services. The appropriate time for the evaluation of speech-language outcomes is highly dependent on the kind of the cleft, surgeries, and teeth involvement in patients. American Cleft Palate-Craniofacial Association recommends yearly speech-language evaluation for children with cleft palate and cleft lip and palate up to 4 years old. It is also recommended to continue the evaluation of the children if problems persist. Moreover, when children’s speech and language are not appropriate for their age or when they have deviation in their speech patterns, they should be referred to a speech therapist.
The results showed that the number of dental care children was 30 in the teamwork group and 18 in the non–team group. These findings showed that those who were team members were more likely to receive dental care. Accordingly, the results of the present study about dental care of children with cleft palate, lip, or both accord with those of Austin et al. (2010). American Cleft Palate-Craniofacial Association emphasizes that primary dental care services for patients with orofacial cleft is highly important (Austin et al., 2010). Thomas reported that dental care services in children with orofacial should start at the age of 2 or 3 and should be provided every 6 months (Thomas, 2000).
As the results showed, there was no significant difference for dental care services between the 2 groups in the past 12 months. This finding doesn’t agree with those of Austin et al. (2010). In effect, it was revealed that the treatment team provided the patients with dental care services at first, but no follow-up was done for dental care in 1-year health control of the patients.
The results showed that the number of children with genetic counseling was 24 in the team member group and 7 in the nonmembers group. This revealed that children, who were team members, received more genetic consultation as it was also the case in the study conducted by Austin et al. (2010). Genetic consultation, as a basic element in the team treatment, is considered to provide families with information about detection, prognosis, the possibility of associated anomalies, and prevention from their recurrence (Kaufman, 1991; Auslander et al., 1993).
As far as the frequency of secondary surgeries was concerned, the results showed that children who were in the teamwork group had more secondary surgeries than the non–team members. These results also match with the results of Austin et al. (2010) concerning the number of surgeries. It was also found that referral to the teamwork treatment led to a timely secondary surgery in the patients.
It seems that the reason for the low frequency of secondary surgeries for the non–team members may be parents’ fear of secondary surgeries and not being able to decide to track and carry out the surgeries on time and being frustrated of improving child’s speech quality.
Another possible reason for reduced secondary surgeries may be presenting unnecessary, inappropriate, and prolonged speech therapy treatment sessions by speech therapists, who raise the issue of no need for surgery for the patient’s family in the hope of improving the speech condition of the referents and follow the treatment without consulting other professionals (Derakhshandeh et al., 2012).
Most of the studies believe that the most appropriate age to have secondary surgery is about 3 to 5 years old and immediately after the definitive diagnosis of incompetence of the velopharyngeal valve. In fact, the age at which the child begins to speak in a continuous speech and is well able to collaborate with the therapist during the diagnosis process can be a good time for recognizing the inadequacy of the velopharynx valve. The more chronic the compensatory productions are, success of the secondary surgery is less likely. Following the treatment process in specialized teams leads to receiving comprehensive counseling in different areas and may help families justify for the timely implementation of secondary surgeries (Derakhshandeh et al., 2011).
The results also revealed that the scores of the teamwork group in the 5 subscales of the QOL questionnaire are significantly higher than that of the non–team members. These findings are in line with the results of Rummans et al. (2006) on QOL of patients with cancer in teamwork and non–teamwork groups, and the results of Van den Berg et al.’s (2005) study on the effect of team care on patients’ QOL with amyotrophic lateral sclerosis (ALS), as a multidisciplinary team was found to improve the QOL of patients with ALS. The findings of this study also agree with those of Lang et al. (2003) about the effect of multidisciplinary rehabilitation on QOL of patients with chronic backache.
Conclusion
In the specialized teams of cleft palate and lips, the treatment decision-making process is based on information of several specialists, and there is a better follow-up and monitoring of care. Early referral to the treatment team leads to timely medical treatment, early evaluation of patient’s problems, and the full consideration of the disorder. It also increases family awareness of the treatment process, timely primary and secondary surgeries, and the necessary rehabilitation services for the treatment of their children.
The findings of this research also showed that presenting services in the teamwork treatment group provided children and their families with better and timely services which, in turn, could enhance the QOL of the patients and their families. Therefore, based on the results of several studies, providing services in a teamwork approach is highly recommended for the patients with cleft lip and palate, especially children with cleft orofacial.
Footnotes
Authors’ Note
This article is extracted from a thesis by Fatemeh Khanchezar. The new affiliation of Neda Tahmasebifard is Department of communication sciences and disorders. East Carolina university. Greenville. US.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the grant (PHT-9413) from the Vice Chancellor for Research Affairs of Ahvaz Jundishapur University of Medical Sciences.