
Abstract
Objective:
The purpose of this study was to determine whether performing mandibular distraction osteogenesis (MDO) during the neonatal period increased inpatient complications as measured through health-care burden.
Materials and Methods:
This was a retrospective cohort study of the Kids’ Inpatient Database from 2000 to 2011. Infants receiving MDO prior to 12 months of age were included. The primary study predictor was distraction age, classified as either neonatal or non-neonatal. Secondary predictors were patient demographics, hospitalization characteristics, diagnoses, and procedures. The outcomes were the number of procedures performed, postoperative length of stay (pLOS), hospital charges, and the discharge transfer rate. Outcomes were compared between the primary predictors using χ2 and independent 2-sample t tests. Multiple linear and logistic regression models were created using clinically relevant predictors to assess the independent effect of neonatal age on each outcome.
Results:
The study sample contained 102 patients, of who 50 (49.0%) were distracted in the neonatal period. Neonatal MDO patients were more likely to have a cleft palate (86.0% vs 55.8%; P < .001) and present with feeding difficulties (38.0% vs 19.2%; P = .036) that were treated through total parenteral nutrition (26.0% vs 9.6%; P = .030) but otherwise did not have significantly different characteristics compared to non-neonatal patients. The multiple regression models confirmed that neonatal age did not influence any of the study outcomes, although other secondary predictors were found to influence the pLOS, hospital charges, and number of inpatient procedures.
Conclusions:
Neonatal MDO was not associated with increased complications. At experienced centers, neonatal status should not be considered a contraindication to treatment.
Introduction
Robin sequence (RS) is a congenital anomaly that is characterized by micrognathia, glossoptosis, and upper airway obstruction (Robin, 1934; Breugem et al., 2016). Infants with RS often present early in life with varying degrees of respiratory distress and feeding difficulty. Nonoperative measures for relieving obstruction include prone positioning, oral appliances, positive airway pressure, and nasopharyngeal or endotracheal intubation (Scott et al., 2012). These temporizing options are appropriate when mild anatomic differences can be compensated through catch-up growth. Tongue-lip adhesion is a relatively safe procedure that tethers the anterior tongue to the lower lip; however, it has fallen out of favor at some centers due to inconsistent outcomes (Resnick et al., 2019). Tracheostomy and gastrostomy tube insertion are the gold standards for definitively bypassing both supraglottic and subglottic obstruction, but their associated morbidity restricts their routine use. Over the past 20 years, mandibular distraction osteogenesis (MDO) has emerged as a highly successful treatment option for infants with RS. Mandibular distraction osteogenesis predictably advances the tongue base by correcting the primary morphologic deficiency (Zellner et al., 2017) and is generally safe and well tolerated, although infrequent complications include surgical site infection, hardware failure, and facial nerve injury (Murage et al., 2014). Long-term disruptions to the primary and permanent dentition have also been reported (Paes et al., 2016; Peacock et al., 2018).
The “Rule of 10s” stipulates that surgery be performed only when a child is 10 weeks of age, weighs at least 10 pounds, and has at least 10 g/dL of hemoglobin. Early studies showed that deviating from these values exponentially increased postoperative complication rates (Wilhelmsen et al., 1966). These criteria were initially developed for cleft lip repair; however, they have since been applied more broadly to other elective procedures (Scott et al., 2011; Tahiri et al., 2015). Because symptoms from RS frequently present at birth, the timing of MDO is often a difficult decision that is made following an appraisal of the relative risks and benefits. For these cases, teams must decide whether the potential complications from intervening during the first days of life are preferable to prolonging upper airway obstruction.
Previously, our institution found that patients who were intubated or received a tracheostomy preoperatively were significantly older at the time of MDO (Lee et al., 2019). It was unclear whether the need to delay MDO increased the rate of definitive airway placement or whether MDO was delayed because the airway had already been secured. In either case, MDO has been shown to both reduce tracheostomy rates and increase subsequent decannulation (Denny et al., 2002; Tahiri et al., 2014). Therefore, early intervention is preferable if it does not contribute to increased harm.
The purpose of this study was to determine whether performing neonatal MDO leads to an increased risk of complication. In this study, the presence of additional complications was indirectly measured through increased health-care burden. To achieve our aims, we compared study outcomes (postoperative length of stay [pLOS], hospital charges, inpatient procedure count, and discharge transfer rate) between infants who had MDO performed in the neonatal and non-neonatal periods. Due to modern advancements in anesthetic and surgical planning, we hypothesized that early intervention would not increase complications and therefore would not be a contraindication to treatment.
Materials and Methods
This is a retrospective cohort study evaluating data from the Kids’ Inpatient Database (KID), which is part of a family of databases provided through the Healthcare Cost and Utilization Project. The KID is the largest publicly available all-payer pediatric inpatient care database in the United States, and it contains data from approximately 3 million pediatric discharges each year. Only patients younger than 21 years of age are included. Per our medical center’s policy, research involving the analysis of de-identified data in publicly available data sets does not qualify as “research” with “human subjects” (per applicable federal regulation) and therefore does not require institutional review board review.
From January 2000 to December 2011, infants with RS were included if they received MDO prior to 12 months of age. Patients were excluded if their records did not provide the age at the time of surgery. Information was recorded pertaining to patient demographics, hospitalization characteristics, inpatient diagnoses, and procedures. Patient demographics included gender, race, insurance, and median income quartile of the patient’s ZIP code. Hospitalization characteristics included transfer status either into or out of the hospital, age at admission, age at MDO, pLOS, and hospital charges. An admission transfer was defined as an intake from a different acute-care hospital or another type of health facility. Newborn admissions were not considered transfers, and data regarding transfers into the hospital were only available beginning in 2009. A discharge transfer was defined as a disposition planned for any nonhome facility. Inpatient diagnoses and procedures that were included in this study are listed in Table 1. All diagnoses and procedures were derived from International Classification of Disease, Ninth Revision (ICD-9) codes. Of note, procedural codes were not limited to major interventions and encompassed both therapeutic and diagnostic procedures, such as electrocardiograms, radiographic imaging, and venous catheterization. Congenital anomalies were recorded pertaining to the nervous (NS), cardiovascular (CV), lower respiratory (larynx and bronchi), and gastrointestinal (GI) systems. For this study, the outcomes of interest were the number of procedures performed, pLOS, hospital charges, and the frequency of transfer at discharge.
ICD-9 Codes for the Diagnoses and Procedures Included in This Study.
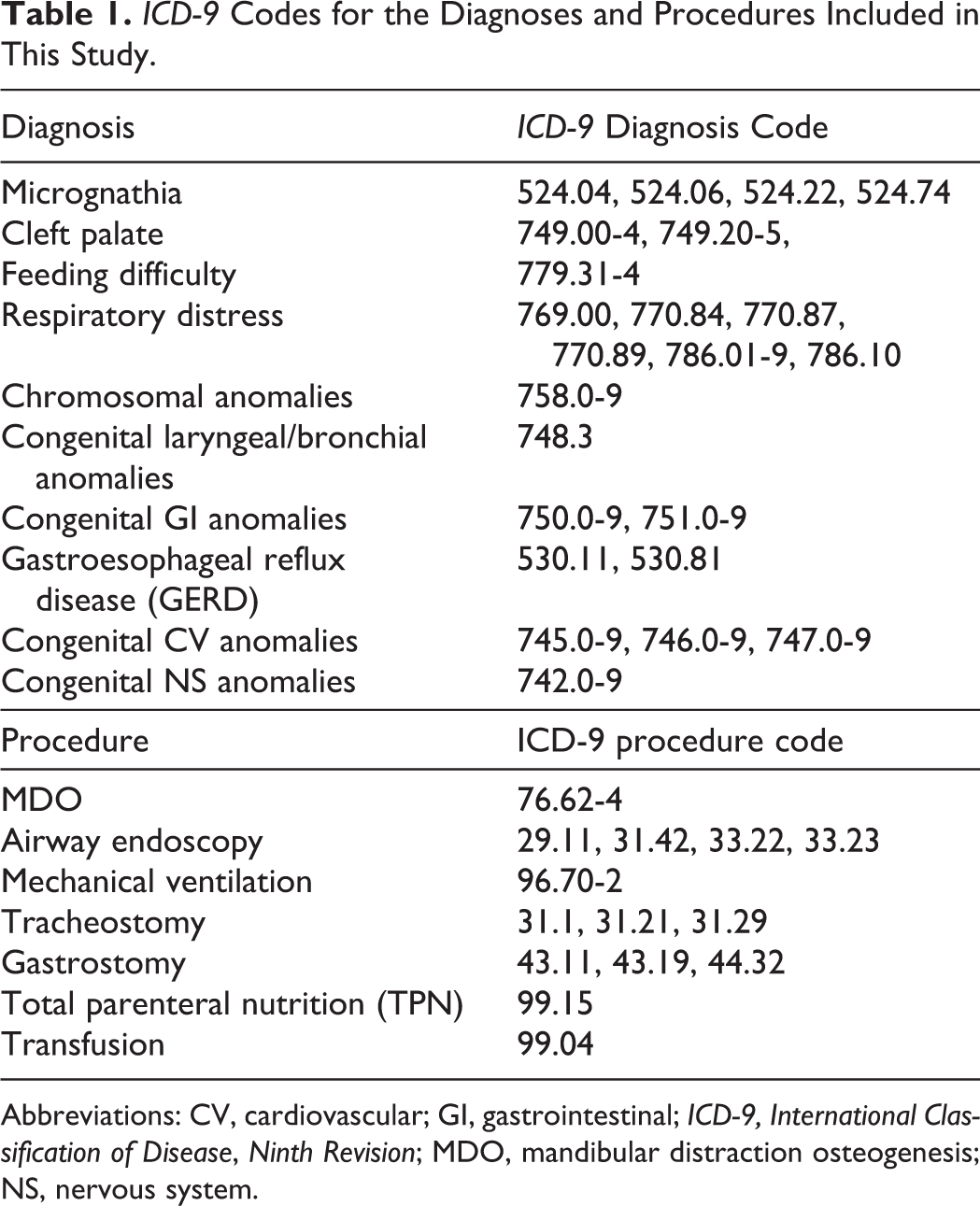
Abbreviations: CV, cardiovascular; GI, gastrointestinal; ICD-9, International Classification of Disease, Ninth Revision; MDO, mandibular distraction osteogenesis; NS, nervous system.
Descriptive statistics were calculated for all study variables. Patients were divided between those who had MDO performed during the neonatal period (28 days of age) and those who did not (between 28 days and 1 year of age). Neonatal age was defined according to the World Health Organization (WHO) as the “first 28 days of life” (WHO, 2019). Patient characteristics, diagnoses, procedures, and outcome variables were compared between neonatal and non-neonatal distractions using χ2 tests and independent 2-sample t tests where appropriate. For continuous outcome variables (pLOS, hospital charges, number of procedures), multiple linear regression models were created using clinically meaningful predictors (age at MDO, respiratory distress, feeding difficulty, cleft palate, NS/CV/GI/laryngeal/bronchial anomalies, tracheostomy, mechanical ventilation, gastrostomy tube placement, and transfusion). For the binary outcome of discharge disposition, a multiple logistic regression model was created using the same set of predictor variables. All t tests were 2-sided, and a P < .05 was considered statistically significant. All analyses were performed with SAS 9.4 (SAS Institute, Cary, North Carolina).
Results
There were 219 patients who fulfilled the inclusion criteria. Of these, only 102 had complete records documenting the timing of MDO and were included in the final sample. The majority of patients were white (64.8%) and males (56.9%). Half of the patients were insured through Medicaid, and 43.1% were insured through private insurance. The distribution of ZIP code income quartiles from lowest to highest earners was 20.4%, 28.6%, 33.7%, and 17.4%, respectively. Cleft palates (70.6%) were commonly observed, and 6.9% of patients presented with a known chromosomal abnormality. Congenital anomalies of the NS (6.9%), CV (34.3%), GI (13.7%), and/or laryngeal/bronchial (12.8%) systems were reported in a subset of patients. Respiratory distress (42.2%), feeding difficulties (28.4%), and acid reflux (23.5%) were prevalent.
Overall, 38.5% were admitted as transfers from outside facilities, while 9.8% were received as in-hospital births. The mean age at admission was 6.6 weeks (standard deviation [SD]:11.1). The mean time from admission to distraction was 12.3 days (SD: 17.2), and the mean pLOS was 23.0 days (SD: 18.3). On average, 7.2 (SD: 4.5) ICD-9 procedures were performed during each admission. Less than half of patients had their obstruction visualized with airway endoscopy (43.1%). Mechanical ventilation (58.8%), and less so tracheostomy (10.8%), were used to secure a definitive airway. Gastrostomy tube placement (18.6%) and total parenteral nutrition (TPN; 17.7%) were used to meet nutritional requirements. Blood transfusions were required in 20.6% of cases. At discharge, 22.6% were transferred to an outside facility, and there were no inpatient deaths reported. From admission to discharge, the average LOS was 35.2 days (SD: 29.2), and the mean hospital charge per admission was US$246 176.65 (SD: $197 789.06).
Fifty (49.0%) patients were distracted during the neonatal period (Table 2). These patients were frequently received as outside transfers (66.7% vs 19.4%; P < .001). They were also more likely to have a cleft palate (86.0% vs 55.8%; P < .001) and present with feeding difficulties (38.0% vs 19.2%; P = .036) that were treated through TPN (26.0 vs 9.6%; P = .030). There were no significant differences in the prevalence of organ system anomalies. Given that they were treated in an earlier window, these patients had shorter delays to MDO (8.7 vs 15.7 days from admission; P = .040). Mandibular distraction osteogenesis in the neonatal period did not adversely affect the study outcomes. The number of procedures coded for, the pLOS, the hospital charges, and the discharge transfer rate was found to be similar between the different age-groups (Table 3).
Comparison of Patient Characteristics, Diagnoses, and Procedures by Neonatal Status.
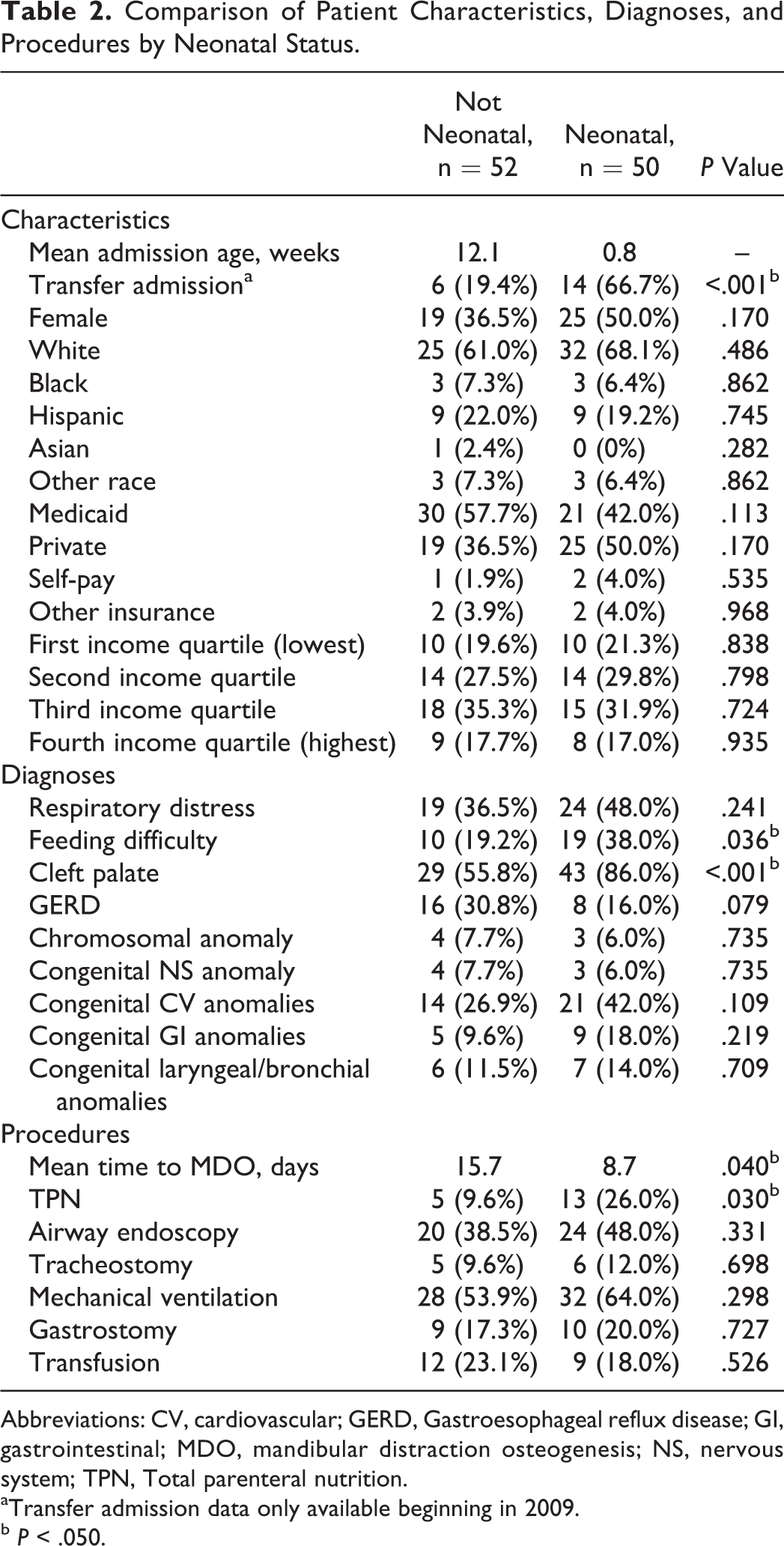
Abbreviations: CV, cardiovascular; GERD, Gastroesophageal reflux disease; GI, gastrointestinal; MDO, mandibular distraction osteogenesis; NS, nervous system; TPN, Total parenteral nutrition.
aTransfer admission data only available beginning in 2009.
b P < .050.
Comparison of Outcome Variables by Neonatal Status.
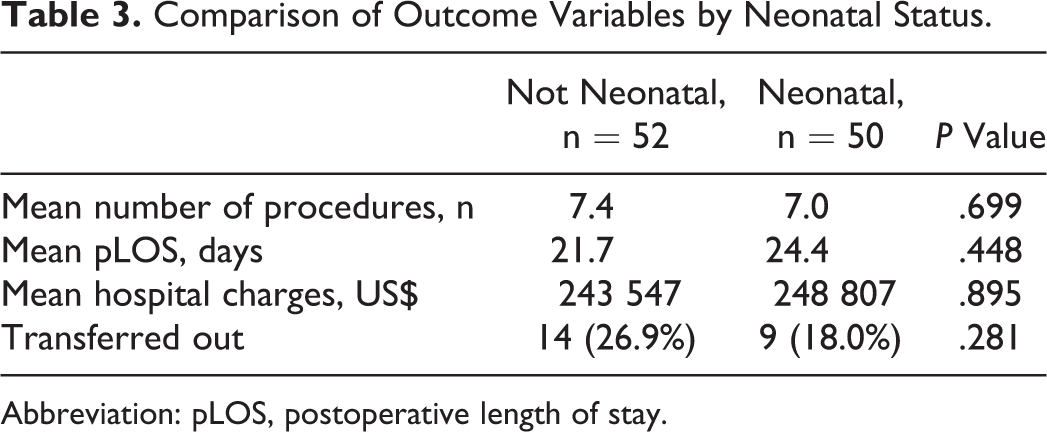
Abbreviation: pLOS, postoperative length of stay.
The multiple regression models confirmed that, after controlling for all other predictors, neonatal age did not significantly influence any of the study outcomes (Table 4). The presence of CV anomalies independently added an estimated average of +9.83 days to the pLOS (P = .001), +US$115 372.77 to the hospital bill (P <0.001), and +1.60 to the number of inpatient procedures (P = .033). Similarly, lower airway anomalies on average added +15.13 days (P < .001), +US$112 807.44 (P = .017), and +3.69 procedures (P < .001). Nervous system anomalies contributed +17.79 days (P = .002) and +US$149 661.10 (P = .022), while GI anomalies only affected the number of procedures (+2.85; P = .007). Another significant predictor of pLOS was gastrostomy tube placement (+19.24; P < .001). Additional significant predictors of hospital charges were respiratory distress (+US$84 454.03; P = .014) and gastrostomy (+US$197 599.17; P < .001). Additional significant predictors of procedure count were mechanical ventilation (+1.72; P = .023), gastrostomy (+3.56; P < .001), and transfusion (+2.51; P = .005). None of the predictors were found to be associated with rate of discharge transfer.
Multiple Regression Models for Study Outcomes (LOS, Charges, Number of Procedures, and Discharge Disposition).a
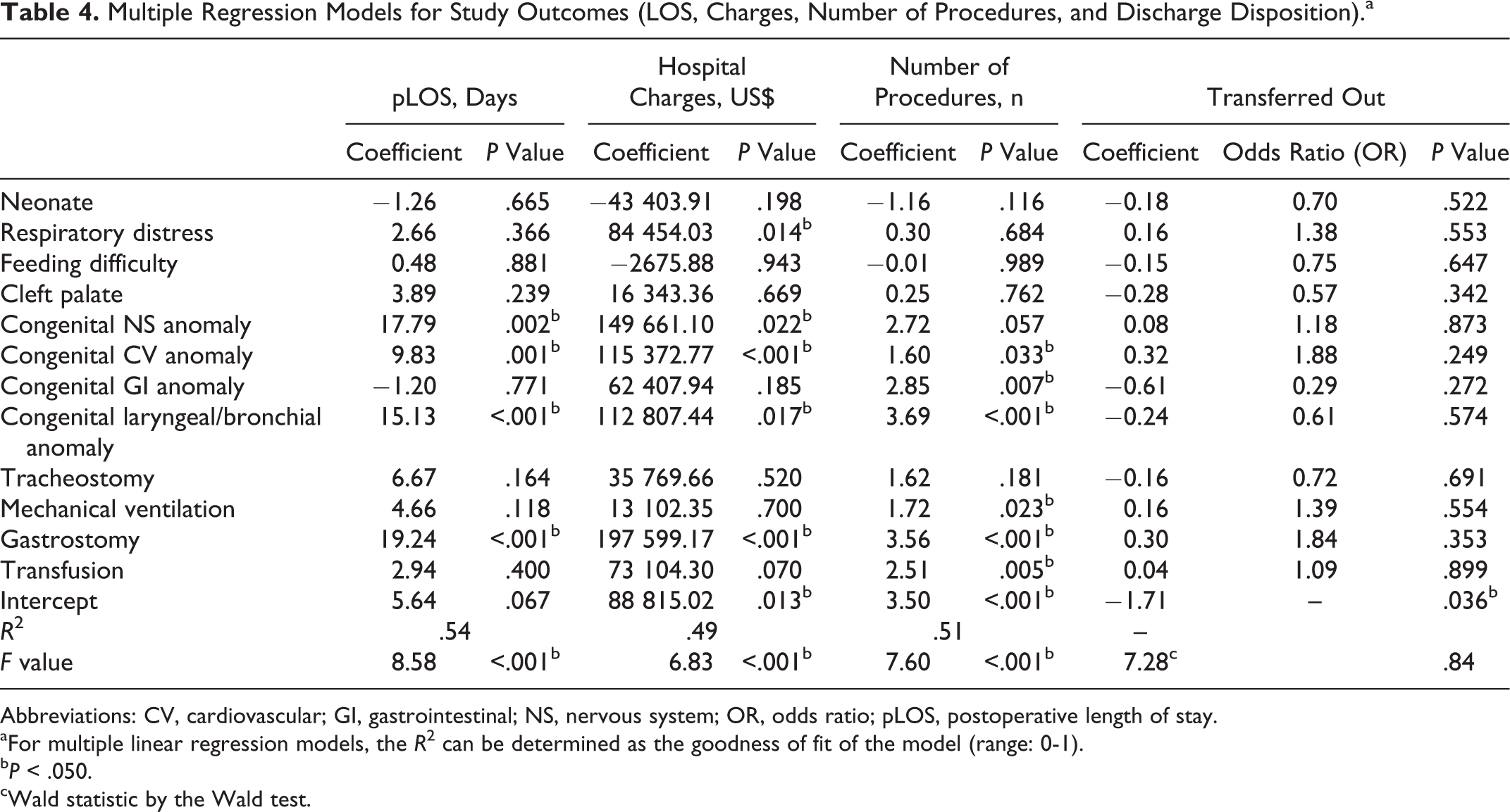
Abbreviations: CV, cardiovascular; GI, gastrointestinal; NS, nervous system; OR, odds ratio; pLOS, postoperative length of stay.
aFor multiple linear regression models, the R 2 can be determined as the goodness of fit of the model (range: 0-1).
b P < .050.
cWald statistic by the Wald test.
Discussion
The purpose of this study was to determine whether neonatal MDO increased inpatient complications as measured through health-care utilization. Our results suggest that performing early MDO in the neonatal period is an acceptable option for infants with RS. Although these patients had a higher prevalence of cleft palate and feeding difficulty at baseline, the overall comorbidity profile and outcomes were similar. There were no increased risks of transfusion, tracheostomy, or mechanical ventilation. Only 1 previous study indirectly compared MDO outcomes by surgical age (Tahiri et al., 2015). Those authors found that low distraction weight (<4 kg) did not decrease clinical success or increase complications (Tahiri et al., 2015). In that study, the mean age of low-weight patients was 23 days, whereas the mean age of controls was 2.7 years. Multiple other studies have reported clinical success with neonatal distraction; however, their results were not directly compared to those of older infants (Goldstein et al., 2015; Scott et al., 2011). Although early intervention appears to be safe and beneficial when performed at experienced centers, it is important to realize that this approach has not been universally adopted. An international survey conducted by Resnick et al. found that non-US physicians, nonsurgeons, and low-volume centers were more likely to delay operative treatment in favor of conservative management (Resnick et al., 2019). In our study, patients who received neonatal distraction were more likely to be received as admission transfers. This suggests that the centers which are performing early intervention are high-volume tertiary-care facilities. Neonatal MDO is certainly not appropriate in all settings, and it should not be performed unless pediatric anesthesia and critical care teams are able to provide adequate levels of support.
Although MDO is a safe and well-tolerated procedure, any neonatal intervention carries additional risk. Over the last 50 years, considerable improvements in surgical care have reduced mortality rates (Rowe and Rowe, 2000); however, postoperative complications still remain particularly high (Michelet et al., 2017). Certain patient features, including cardiac malformation, have been found to increase the likelihood of subsequent cardiac arrest (Ramamoorthy et al., 2010) and mortality (Lillehei et al., 2012) in infants <1 year of age. These adverse events are further magnified in the context of high-risk open abdominal and thoracic procedures (Stey et al., 2015). Our study found that neonatal MDO did not prolong the LOS or increase hospital costs. Compared to other locations, the face represents a relatively low-risk surgical site, and therefore, MDO may contribute minimally to the inherent anesthetic risk. Although this additional risk is non-negligible, neonatal surgery does have its benefits. Neonatal interventions are cost-effective in the long term (Poley et al., 2008). Early curative surgery may also avoid unnecessary procedures later on. In the context of RS, tracheostomy avoidance is not insignificant and can drastically reduce patient morbidity (Mahida et al., 2016) and health-care costs (Runyan et al., 2014). With appropriate experience and patient selection, we propose that MDO should not be delayed on account of neonatal status alone. It is important to note that the precise timing of MDO is unclear. In general, early distraction may be preferred in cases of prolonged intubation to reduce the risk of stenosis. Milder presentations may be better managed with symptomatic treatment and watchful waiting to monitor for catch-up growth.
Surgical age did not impact our study outcomes; however, other comorbid features were independently found to influence pLOS, hospital charges, and inpatient procedure count. Goudy et al previously found that CV and neurologic anomalies were associated with increased health-care utilization among patients with RS (Goudy et al., 2017). Regardless of age, syndromic patients with complex medical profiles have a significantly increased cost of care (Scott et al., 2014; Simmonds et al., 2018). Notably, in our study, congenital anomalies involving the nervous system and lower airways prolonged hospital stays by +17.42 and +14.84 days, respectively. In comparison, CV anomalies prolonged the postoperative course by less (+9.56 days). Patients with micrognathia in the setting of seizures, hypotonia, or laryngomalacia may have additional contributions to their respiratory symptoms, and in these cases, mandibular advancement serves to only address 1 component of obstruction. These patients therefore experience longer delays to discharge. The only procedure that impacted pLOS was gastrostomy placement (+19.54 days). Distraction improves nutritional status and reduces feeding tube requirement (Susarla et al., 2017). In fact, high-volume MDO centers have been shown to have lower rates of gastrostomy tube placement (Scott et al., 2014). Along with early intervention, our analysis supports the practice of reducing gastrostomy at the time of distraction unless truly indicated for nutritional support. Airway interventions, such as tracheostomy and mechanical ventilation, did not affect pLOS. This implies that they were used as temporizing measures prior to surgery and that these patients achieved a common clinical end point. In agreement with prior studies, hospital charges largely mirrored lengths of stay (Scott et al., 2014). The exception was respiratory distress diagnosis which did not impact discharge planning but did add to the expenses of care. Between 1 and 3 additional procedures were required to address other congenital anomalies of the CV, GI, and lower airways. Neurologic deficits were costly but did not require additional procedures to correct.
There were certain limitations to our analysis that prior authors using similar methods have noted. Although the KID provides a large stratified sample of all inpatient admissions, our study size was limited because less than half of the eligible records provided the timing of MDO. International Classification of Disease codes standardize the medical vocabulary, but as a result, they are often unable to relay the full details of a hospital course. Our study relied on the accurate and consistent coding of diagnoses and procedures by hospital administrators. All patients presumably presented with respiratory distress; however, only 42.2% of records submitted the associated diagnosis code. It is unclear if this discordance represents a true data gap or denotes a symptomatology separate from the expected positional respiratory distress seen in all infants with RS. Similarly, only 43.1% of records had an airway endoscopy coded. This value likely underestimates the true practice prevalence, as bedside examinations may have been lost in the documentation. Variables such as patient age and pLOS are thought to be less prone to coding error since the values are well-defined and easily verified. We were unable to directly measure parameters such as intraoperative time that would have given us insight into the technical difficulty of performing early surgery. Outpatient and emergency department costs are not included in this data set, and their contribution was not factored into the health-care burden.
In conclusion, neonatal MDO was not associated with increase health-care burden. At experienced centers with proper patient selection, neonatal status should not be considered a contraindication to treatment. Our study only evaluated inpatient factors, and future studies on neonatal distraction should compare the technical difficulty as well as the outpatient burden.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.