
Abstract
Objective:
To examine word reading performance between boys with isolated cleft lip and/or palate (iCL/P), unaffected average reading (uAR), and unaffected impaired reading (uIR), using the dual-route model.
Design:
Case/control study.
Setting:
University children’s hospital.
Participants:
Males, between the ages of 8 to 11 years, with iCL/P (n = 26), uIR (n = 33), or uAR (n = 28).
Methods:
Single word reading and achievement were evaluated. Analyses of variance and analyses of covariance evaluated group differences in achievement. Medical records were reviewed for iCL/P participants for audiology and speech history. Spearman ρ correlations were calculated between hearing, speech, and reading achievement for the iCL/P group.
Main Outcome Measure(s):
Reading performance was evaluated using select subscales from the Woodcock Johnson Reading Mastery Test, 3rd Edition and the Test of Orthographic Competence.
Results:
Participants with iCL/P had higher than expected rates of reading impairment, differing across cleft type (0% iCL, 50% isolated cleft lip and palate [iCLP], 71.4% isolated cleft palate only [iCP]). On measures of word reading accuracy, iCL/P participants outscored uIR participants, with uAR participants scoring the highest. This pattern was specific to nonlexical reading tasks. Participants in the uAR and iCL/P groups outscored uIR participants on lexical tasks, with no significant differences between uAR and iCL/P. Evaluation of speech and hearing revealed no significant relationship to single word reading or achievement measures in the iCL/P group.
Conclusions:
Boys with iCL/P are at a higher risk of reading impairments, particularly within the iCP subset. Regular screening should be encouraged, with skills from both lexical and nonlexical routes assessed.
Introduction
Isolated Clefts
Isolated orofacial clefts have no known genetic cause or association with a diagnosed syndrome. Even without known syndromic impacts, multiple variables potentially contribute to physical, cognitive, academic, behavioral, and emotional outcomes in children with isolated cleft lip and/or palate (iCL/P). Children with iCL/P are known to be at higher risks for hearing, speech, and language problems, which may especially impact them academically.
Isolated Clefts and Academic Performance
Academic performance, achievement, and special education
Although the iCL/P population has been found to have an overall average intelligence (Conrad, 2015), they still demonstrate issues in academics. While their overall IQ falls in the average range, some research has identified relatively lower performance on IQ and achievement tests than unaffected peers, with differences apparent as early as 12 months old (Jocelyn et al., 1996). Children with isolated clefts have also been shown to exhibit school performance up to half a grade level behind peers of the same age (Wehby et al., 2014). Academic impairments have been displayed across all school subjects and grade levels (Wehby et al., 2014), with lower achievement seen in children with iCL/P in all measured academic areas compared to national averages, even as young as 5 years old (Fitzsimons et al., 2017). Children with clefts display trends of not meeting grade-level requirements throughout elementary school, with increased risk of poorer academic performance extending through middle school (Watkins et al., 2018).
Yazdy and colleagues (2008) found that children with iCL/P were reported to have higher usage of special education services with rates between 20% and 30%, up to 3 times higher than rates found in unaffected children. Although speech and language services were the most common type of special education service utilized, referrals for special education due to learning disabilities and behavioral disorders were also prevalent. After excluding speech and language services, children with orofacial clefts were still more likely to use special education services than unaffected children. Even with an average intelligence, the isolated cleft population remains at a higher risk for academic and achievement issues compared to their unaffected peers. The specific cause of academic underachievement is currently unclear, but identifying earlier and more accurate treatments of academic problems in children with iCL/P would benefit the far-reaching impacts seen in this population.
Learning disability and reading disability
Previous work has reported rates of learning disorders in children with iCL/P to be as high as 46%, with especially high rates of disorders in reading and language (Broder et al., 1998). Because reading disabilities are so prevalent in children with isolated clefts, a series of research studies starting in the 1980s was conducted by Richman and colleagues to examine the nature of these disabilities. Higher rates of reading disabilities in children with cleft were found to be associated with additional deficits in verbal fluency, rapid naming, memory, and processing speed (Richman and Eliason, 1984; Richman and Ryan, 2003; Richman et al., 2005).
More recent work has found that isolated reading in iCL/P was associated with auditory memory issues, but not related to speech or hearing issues (Conrad et al., 2014). Rapid naming and memory have been measured alongside functional brain imaging in the isolated cleft populations to gain more insight into reading impairments. Boys with isolated cleft palate only (iCP) were found to have reading fluency correlated with phonological awareness and visual memory, with increased activation in dyslexic reading–associated brain regions (Conrad et al., 2015). Children with CL/P have also demonstrated poorer nonword spelling related to poorer phonological awareness (Mei Lee et al., 2015).
Speech and hearing
Some research has shown the impact of speech and hearing issues on academics, but results have been mixed. Children with clefts are at risk for speech and language disorders (Broen et al., 1998). Eighty-one percent of children with an oral cleft who utilized special education were involved with speech and language services for at least 1 year, a rate that is 4 times higher than that of unaffected children (Yazdy et al., 2008). Speech issues are a risk factor for reading impairments and dyslexia in general, but research for children with iCL/P is mixed. Some studies have found relationships between speech and reading impairments (Chapman, 2011; Særvold et al., 2019), while others have not (Conrad et al., 2014; Conrad, 2018).
In addition to the risk for speech issues, middle ear disease is significantly more common in children with CL/P than controls, but not necessarily hearing loss, which could be due to common treatments like ventilation tubes (Jocelyn et al., 1996). By the age of 2, children with clefts have had more abnormal tympanograms or ventilation tubes than controls (Jocelyn et al., 1996). More hearing loss at 12 months of age has been shown to be related to lower comprehension scores and lower expressive language scores later on (Jocelyn et al., 1996). However, like with speech issues, there are exceptions—some children with cleft lip and palate have shown low language scores and normal hearing, or hearing loss and normal language scores (Jocelyn et al., 1996). While speech and hearing may negatively affect language skills and have some influence on academic problems in children with iCL/P, other factors may have an equal or greater effect on language, cognition, and intellectual development.
Cleft type and academics, achievement, and special education
There appears to also be some influence of cleft type on academic underachievement and risk for reading impairments within the iCL/P population, although research has been mixed. Children with iCP have previously demonstrated more academic problems according to both teacher and parent report (Millard and Richman, 2001) and poorer academic achievement in all measured academic areas when compared to children with isolated cleft lip only (iCL), isolated cleft lip and palate (iCLP), or unaffected children (Wehby et al., 2015; Fitzsimons et al, 2017). Children with iCP have also demonstrated lower grade point averages than other cleft types (Persson et al., 2012), higher rates of special education utilization (Collett et al., 2014; Wehby et al., 2014; Fitzsimons et al., 2017), more frequent classification into low achievement trajectories than other cleft types (Wehby et al., 2015), and are the group most likely to repeat a grade (Broder et al., 1998). Children with iCP less frequently received speech therapy than controls, although not significantly (Collett et al., 2010). Children with isolated clefts involving the palate had higher odds of not passing and the highest odds of receiving the lowest grades in some subject areas (Persson et al., 2012). However, a recent study found children with iCLP to have the poorest grade-level performance (Watkins et al., 2018).
Additional reports demonstrate children with iCL had the fewest academic problems (Persson et al., 2012). When compared to unaffected children, children with iCL displayed no significant difference in academic achievement in some areas (Fitzsimons et al., 2017), scored at or above the level of their unaffected siblings on state assessments (although not significant) (Collett et al., 2014), and showed lower rates of special education services utilization (Yazdy et al., 2008). Children with iCL were also least likely to have special education needs compared to other cleft types (Fitzsimons et al., 2017) and have even been found to be less likely to use special education than their unaffected siblings (Collett et al., 2014).
Cleft type and learning disability
Cleft type may also influence specific reading impairments. Richman and colleagues have found differences in reading skills and achievement for different isolated cleft types. Reports include children with iCP scoring lower than children with iCLP on measures of early literacy skills like auditory memory and verbal fluency (Richman and Eliason, 1984). The increased likelihood of children with iCP to have general language disorders also led to rates of reading disabilities that were much higher than the general population, at 33% (Richman et al., 1988). Other research has found the highest rates of learning disability in males with iCP, with rates as high as 79% (Broder et al., 1998). Additionally, in boys with iCL, rates of reading impairments were found to be normative (Conrad, 2018).
Cleft type and speech and hearing
One reason for a higher incidence of reading disability in children with iCL/P at younger ages could be due to peripheral speech deficits (Richman et al., 1988). Children with iCLP and iCP have a higher prevalence of speech and language disorders, which may be related to the increased likelihood of having a reading disability (Richman, 1980). Some research has shown that children with iCLP who also have reading disabilities may have peripheral speech problems related to phonetic errors; this group may benefit from corrective speech interventions, an emphasis on sight word skills, and a focus on story context (Richman and Eliason, 1984). Comparatively, children with iCP who also have reading disabilities may have more sight word errors due to a more language-based reading disability; this group may benefit from more general comprehension and language association skills (Richman and Eliason, 1984). Additional effects of cleft type on speech and hearing issues require further investigation. Recently, measures of hypernasality and reduced intelligibility were associated with a higher risk of reading and language problems, including poorer comprehension (Særvold et al., 2019).
Currently, there is no widely accepted reason or consistent findings that explain the higher incidence of reading impairments in boys with differing cleft types, and it is difficult to generalize results of studies of isolated CL/P without separating by cleft type and sex. Additionally, little research on isolated clefts and reading ability has been done in recent years to incorporate variables related to reading, such as spelling, speech, and language abilities. There is a need for better identification and application of targeted interventions for specific reading impairments seen within isolated cleft subtypes. Using models of developmental dyslexia has been beneficial to iCL/P reading impairments in the past. Applying additional reading development models to research involving children with iCL/P may provide additional insight on the presence of reading disabilities within this population and allow for more accurate targeting of diagnosis and treatment.
The Dual-Route Model
The dual route model has historically been used to demonstrate 2 separate but interactive pathways involved in early reading development—the nonlexical and lexical routes (Coltheart and Leahy, 1996; Rapscak et al., 2007). The nonlexical route allows children learning to read to decode letters (graphemes) into their corresponding sounds (phonemes) and combine them into whole words (Beech and Awaida, 1992). The nonlexical route provides the ability to correctly read pseudowords—nonsense words that can still be sounded out by following phoneme–grapheme conversion rules (Coltheart and Leahy, 1996; Rapscak et al., 2007) (eg, CHED). The nonlexical route can also read regular words—words that follow normal, expected English spelling rules (Rapscak et al., 2007) (eg, CRATE). However, the nonlexical route fails at reading exception words—words which do not follow traditional spellings (Coltheart and Leahy, 1996; Rapscak et al., 2007) (eg, CHOIR). The lexical route is connected to the “sight vocabulary,” which develops once printed words are associated with their correct pronunciations (Beech and Awaida, 1992). The lexical route allows readers to correctly read familiar regular or exception words by accessing letter combinations and even some whole words (lexical representations) that are stored with their correct mental pronunciations (Rapscak et al., 2007) and meaning (Dehaene, 2009). This route fails at reading pseudowords or unfamiliar words, as these words don’t yet have lexical representations formed (Coltheart and Leahy, 1996; Rapscak et al., 2007).
The Dual-Route Model and Reading Impairments
The dual-route theory hypothesizes that skilled reading depends on mastering and then properly applying both routes (Coltheart and Leahy, 1996). Both routes are necessary to be able to read all types of words proficiently. Disruptions in one or both routes, or overreliance on one route over the other, can cause different reading impairments depending on where the disruption falls (Coltheart and Leahy, 1996). A disruption in the nonlexical route may present as phonological dyslexia, with difficulty decoding pseudowords and a lack of phonological awareness (Temple and Marshall, 1983; Coltheart and Leahy, 1996; Zorzi et al., 1998; Cestnik and Jerger, 2000). Children with nonlexical impairments can still usually read familiar regular or familiar exception words, as the lexical route is normally left intact (Rapscak et al., 2007). Alternatively, a disruption in the lexical route may present as surface dyslexia (Coltheart et al., 1983; Zorzi et al., 1998; Cestnik and Jerger, 2000; Rapscak and Beeson, 2004), displayed as difficulty reading exception words (Coltheart et al., 1983; Rapscak and Beeson, 2004). Surface dyslexia can lead to regularization errors, or incorrectly reading irregular words using incorrect phonological “codes” (Coltheart et al., 1983), leading to difficulties with whole word recognition. Children with lexical disruptions are generally still able to read regular and pseudowords due to an uninterrupted nonlexical route (Coltheart, 2005; Rapscak et al., 2007).
Understanding how dual route impairments contribute to different types of dyslexia may shed light on similar reading impairments within children with iCL/P. Comparing children with isolated clefts to unaffected children with dyslexia using the dual-route model may help evaluate how using models of reading can improve understanding of reading impairments within the isolated cleft population. Could one explanation for the higher incidence of reading impairments in boys with iCL/P be related to an overreliance on one of these reading routes over the other? Is reading in boys with iCL/P similar to the way unaffected (noncleft) impaired readers read? The purpose of this study was to examine single word reading ability using the dual-route model by using 3 different groups of boys—unaffected average readers, unaffected impaired readers, and boys with iCL/P. Reading skills were assessed through single word reading tasks to capture reliance on or disruption within the nonlexical and lexical routes. Pseudoword reading tasks were used to assess nonlexical competency, and exception word reading tasks were used to assess lexical route reliance.
Methods
Participants
A total of 87 boys, ages 8 to 11 years, were recruited into 3 separate groups—unaffected boys with average reading ability (uAR), unaffected boys with impaired reading (uIR), and boys with iCL/P at any reading level. Potential participants were excluded for history of head trauma or injury, mental health diagnoses, or major medical conditions (aside from having a cleft in the iCL/P group).
Recruitment for the uAR group occurred through local advertisements. Additional eligibility criteria for this group included average reading ability (ie, no participation in any remedial or accelerated reading programs or talented/gifted programs). Recruitment for the uIR group occurred through advertisements by a statewide dyslexia association. Additional eligibility criteria for the uIR group included having a diagnosis of dyslexia or participation in tier 3 (special education) services for reading. For participants without a formal diagnosis, reading assessment scores were reviewed to ensure significant impairments in early literacy measures (like phonological awareness or rapid naming) and reading achievement measures (like decoding and fluency). Recruitment for the iCL/P group took place through the patient registry at the cleft clinic at a university hospital. Boys in the iCL/P group could participate no matter their reading level, as long as they did not have any diagnosed syndrome, additional major medical condition, or other congenital anomalies.
The final sample included 87 male participants; 28 uAR, 33 uIR, and 26 iCL/P (7 iCL, 12 iCLP, 7 iCP). No group differences were found in age (F 2,84 = .082, P = .922). The majority of participants were from non-Hispanic (87.4%), white (88.5%) ethnic/racial backgrounds. All 3 groups had an average or higher mean cognition score (measured by Global Ability Index [GAI]). Although uAR participants were excluded from participation if they had been involved with talented and gifted programming (TAG) or the extended learning program (ELP), this group still had significantly higher GAI than both the uIR and iCL/P groups, Welch Statistic (2, 48.33) = 9.511, P < .001. Participants within the iCL/P group had significantly higher socioeconomic status (SES) scores (based on modified Hollingshead rating scale where a higher score reflected lower parental SES) compared to uAR, Welch Statistic (2, 51.97) = 5.301, P = .008. Neither age (F 2,23 = .719, P = .498), GAI (F 2,22 = 1.093, P = .353), nor SES (F 2,23 = 1.017, P = .377) were found to be significantly different between cleft types (see Table 1).
Mean Demographics (95% Confidence Interval) and Rates of Preexisting Diagnoses and School Services by Participant Group and Cleft Type.
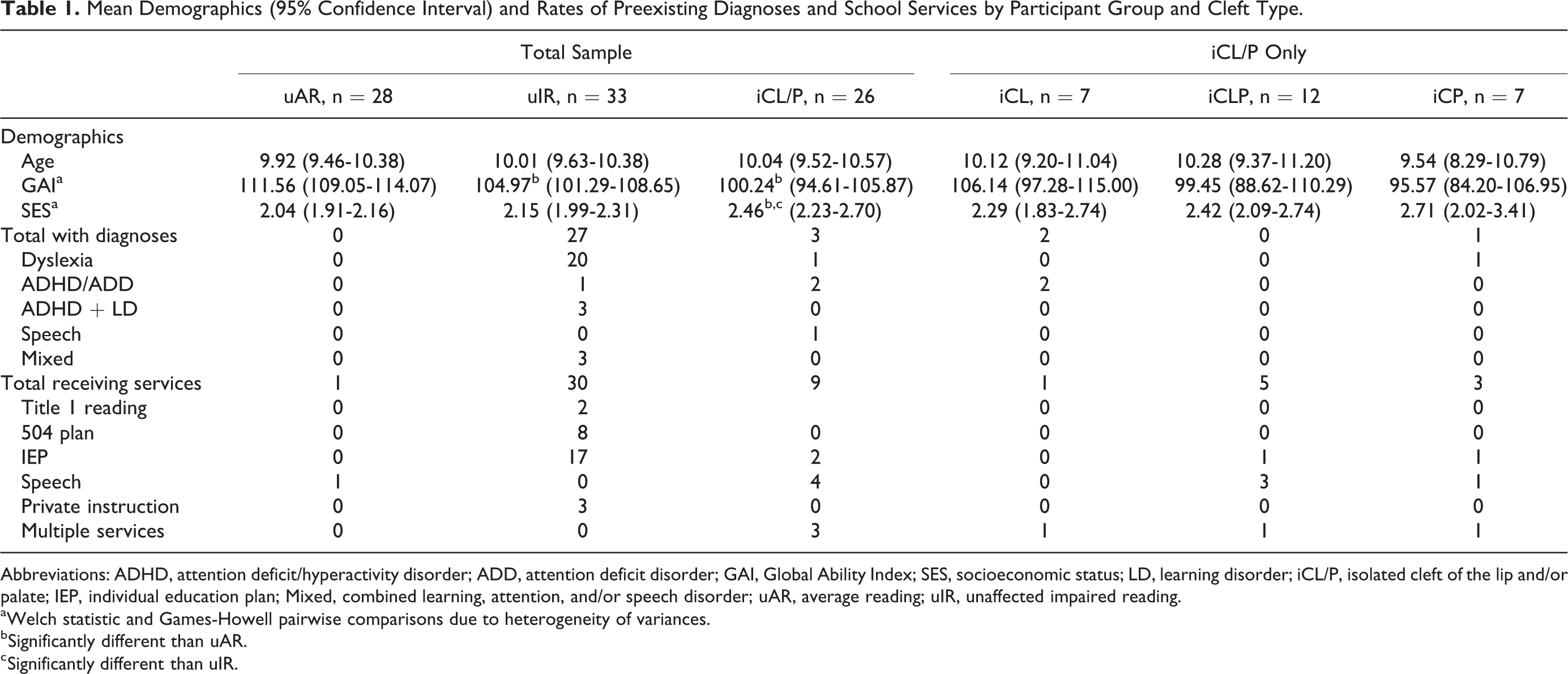
Abbreviations: ADHD, attention deficit/hyperactivity disorder; ADD, attention deficit disorder; GAI, Global Ability Index; SES, socioeconomic status; LD, learning disorder; iCL/P, isolated cleft of the lip and/or palate; IEP, individual education plan; Mixed, combined learning, attention, and/or speech disorder; uAR, average reading; uIR, unaffected impaired reading.
a Welch statistic and Games-Howell pairwise comparisons due to heterogeneity of variances.
b Significantly different than uAR.
c Significantly different than uIR.
Due to group design and inclusion criteria, no participants in the uAR group had a preexisting diagnosis of a learning or attention disorder, and only 1 uAR participant had previously received speech therapy from school. Logically, a majority of uIR participants had preexisting diagnoses (n = 27) and received school services (n = 30). However, only 1 participant in the iCL/P group had preexisting learning disability diagnoses (dyslexia with dysnomia), no iCL/P participants had a speech disorder diagnosis, and only 3 iCL/P participants had a preexisting attention disorder diagnosis. A total of 5 iCL/P participants received school services for reading, with some participants receiving multiple services in other areas such as speech. Only 1 iCL/P participant had a formal learning disability diagnosis and was receiving services, 8 iCL/P participants were receiving services without any learning or attentions diagnoses, and 3 iCL/P participants had an attention disorder diagnosis but were not receiving any services (see Table 1). Although the inclusion of boys with attention deficit/hyperactivity disorder could be a confounding variable, they were included due to a limited available sample and the high prevalence of co-occurring issues with dyslexia. Exploratory analyses of iCL/P participants comparing those with a preexisting learning or attention diagnosis and/or receiving school services (n = 12) compared to those without either (n = 14) did not display any significant differences in age, SES, GAI, or achievement measures (see Table 2).
Demographics, Nonlexical Achievement, and Lexical Achievement Measures for iCL/P Participants With or Without Diagnoses/Services.a
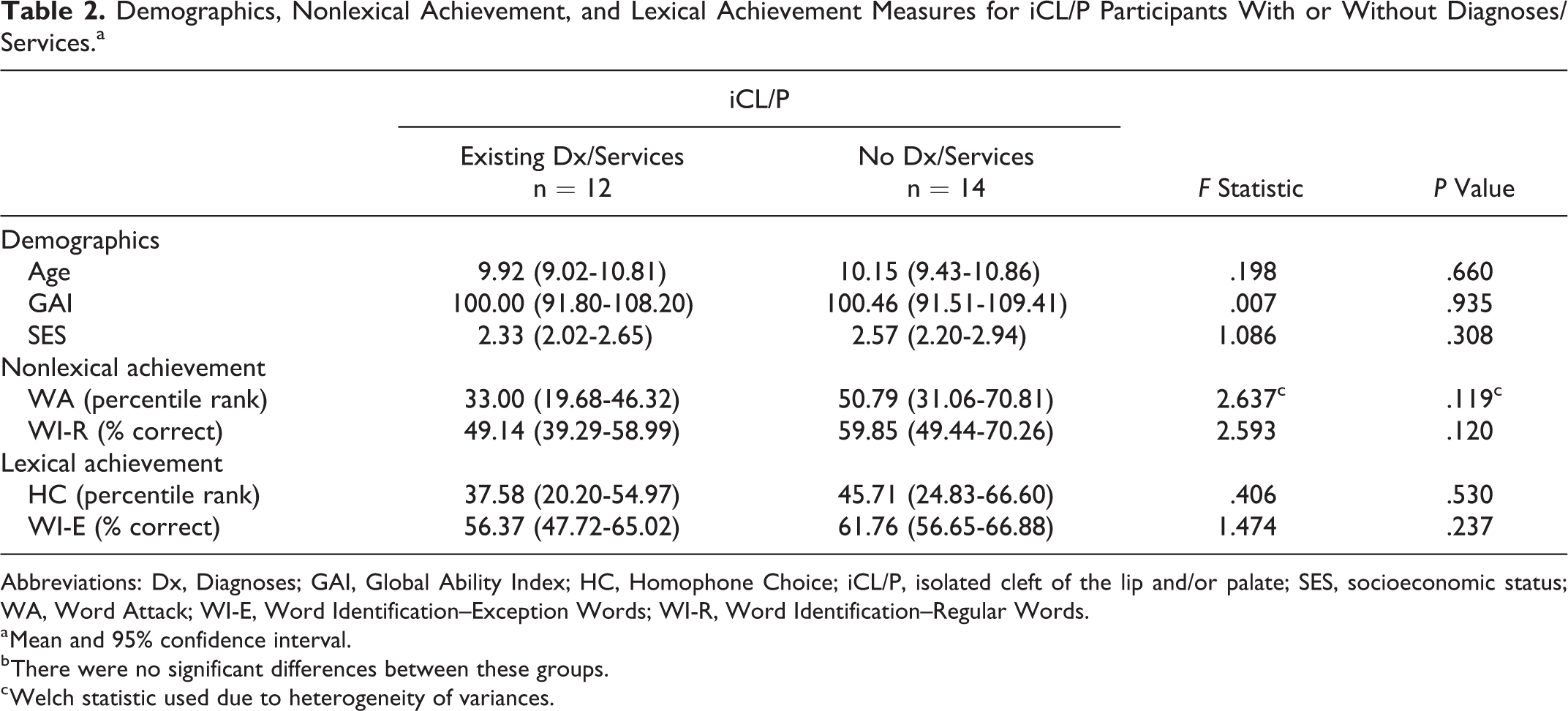
Abbreviations: Dx, Diagnoses; GAI, Global Ability Index; HC, Homophone Choice; iCL/P, isolated cleft of the lip and/or palate; SES, socioeconomic status; WA, Word Attack; WI-E, Word Identification–Exception Words; WI-R, Word Identification–Regular Words.
a Mean and 95% confidence interval.
b There were no significant differences between these groups.
c Welch statistic used due to heterogeneity of variances.
Protocol and Measures
All study procedures were approved by the local institutional review board. A trained research assistant met with families to describe the study and obtain informed consent. Written consent was provided by a legal guardian, and participants provided written and verbal assent. Participants received compensation for participating in the study, and guardians received reimbursement for travel expenses. Participation involved a daylong visit to the hospital, where all groups completed a neuropsychological and achievement assessment battery as part of a larger study (Conrad, 2018). Selected assessments from this larger study are discussed in this article.
Intelligence testing
Selected subtests from the Wechsler Intelligence Test for Children, 5th Edition (Wechsler, 2014) were administered to obtain a GAI. This measure was used for group descriptive purposes.
Dual-route measures
Selected subtests from the Woodcock Reading Mastery Test, 3rd Edition (WRMT-III) (Woodcock, 2011) were administered to assess reading achievement. Woodcock Reading Mastery Test, 3rd Edition Word Identification (WI) was used to assess single word reading accuracy by having participants read real words. The WI subtest was coded by a local dyslexia expert into 2 separate word lists—a Regular Word Identification List (WI-R) and an Exception Word Identification List (WI-E). The WRMT-III Word Attack (WA) subtest was also used to assess single word reading accuracy, but measured pseudoword reading instead of real word reading. A selected subtest from the Test of Orthographic Competence (TOC) (Mather, 2008), TOC Homophone Choice (HC), was used to assess sight spelling and whole word recognition. Percentage correct was used to report performance on WI-R and WI-E as these lists do not have normative scores, while index and standard scores were used to report performance on WA and TOC based on available normative data. See Figure 1 for more information about the relationship between these subtests and nonlexical and lexical routes and skills.
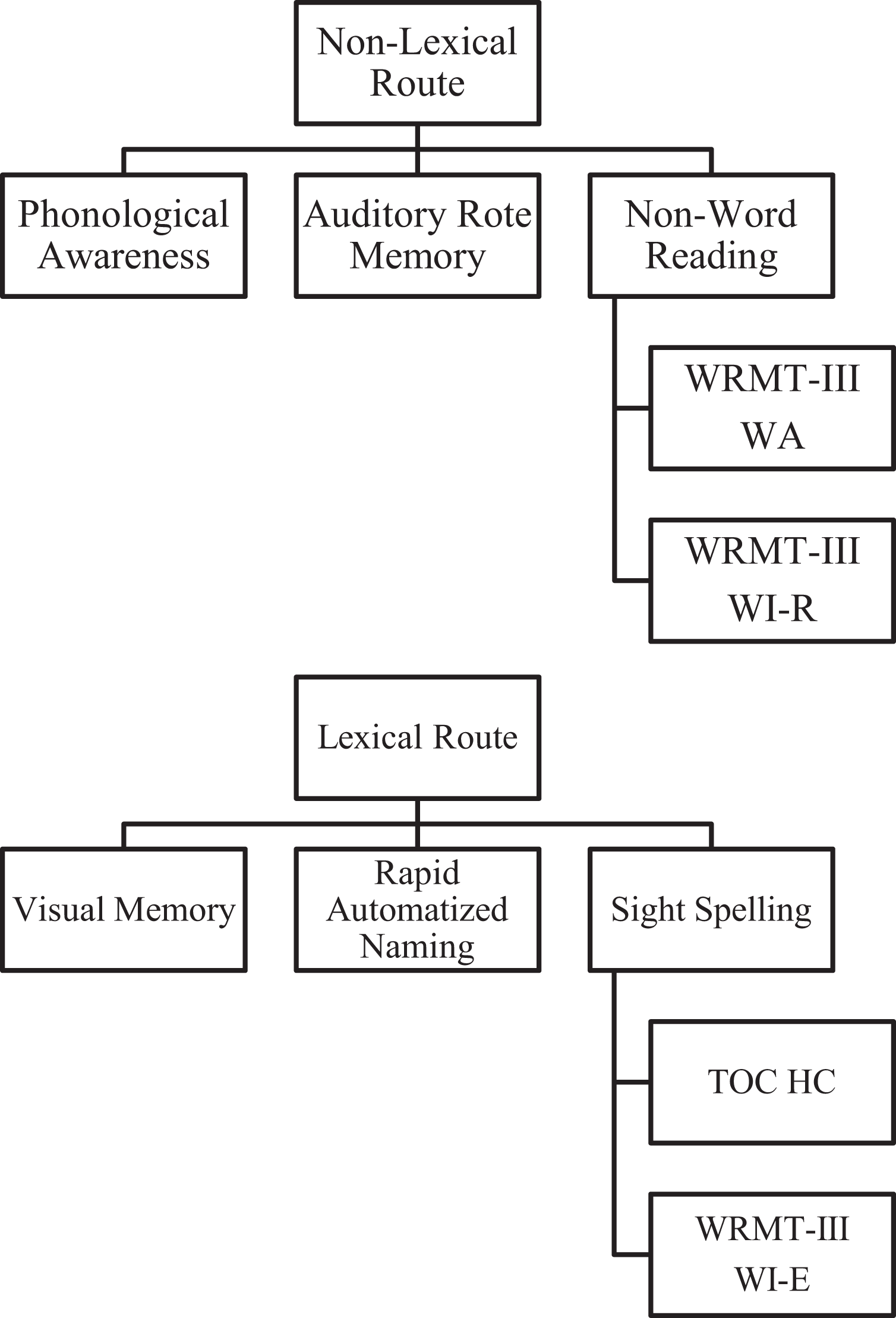
Lexical versus nonlexical route skills and assessments.
Medical chart review
For participants with iCL/P, medical charts were systematically reviewed for information on hearing and speech history. Audiology and speech records were available for 25 participants.
Hearing
Audiology scores were collected from iCL/P participants’ medical records. Worst audiology score was used as the measure of interest to capture the potential impact of hearing impairment on early literacy and reading outcomes. Audiology records were available for 25 participants.
Speech
Speech information was also reviewed from iCL/P participants’ medical records. Information collected included common speech errors (developmental errors, compensatory errors, obligatory errors) and velopharyngeal insufficiency (VPI). Among participants with iCL/P, VPI was classified as marginal to inadequate in 52% of the iCL/P sample. Ranked severity scores (none, one, some/mild, and multiple) for common speech errors were also obtained. Similar to audiology measures, worst speech score for each variable of interest was used in analyses. Speech records were available for 25 participants. Cleft type differences in speech ratings could not be calculated due to low cell sizes.
Analyses
Rates of impairment
The WRMT-III WI subtest was used as an indicator of single word reading performance. To examine clinical levels of concern, “impaired reading” was operationally defined as a score at or below the 25th percentile on this subtest. The 3 participant groups were compared using χ2 analyses to evaluate specific clinical risks for impairment, with descriptive rates calculated for the 3 cleft types due to low expected cell sizes. Observed counts were compared with expected rates of 75% no risk and 25% at risk.
Dual-route measures
Separate univariate analyses of covariance (ANCOVA) were run to assess group differences in performance on the nonlexical and lexical reading tasks. The independent variable was group membership across the 3 groups (uAR, uIR, and iCL/P). Socioeconomic status was included as a covariate. Dependent variables included the 5 achievement scores: WI, WI-R, WI-E, WA, and TOC. Welch statistics were used if homogeneity of variance was violated.
Cleft type differences were examined by separate univariate analyses of variance (ANOVA) for the same nonlexical and lexical reading tasks. No covariates were included in the analyses of performance for different cleft types. The independent variable was isolated cleft type (iCL, iCLP, and iCP). Dependent variables included the same 5 achievement scores: WI, WI-R, WI-E, WA, and TOC. Again, Welch statistics were used if homogeneity of variance was violated.
Speech and hearing measures
Spearman ρ correlations were calculated between hearing, speech, and reading achievement measures.
Results
Rates of Impairment
The WRMT-III WI test was used as an indicator of single word reading performance. Scores were interpreted based on clinical at-risk determinant percentiles. Scores at or below the 25th percentile were considered “clinically at risk” for reading impairments, while scores above the 25th percentile were considered proficient.
Consistent with the parent study (Conrad, 2018), χ2 analyses revealed fewer than expected uAR participants in the at-risk range (n = 1; χ2 = 6.857, P = .009) and more than expected uIR participants in the at-risk range (n = 23; χ2 = 35.162, P < .001) on the WI—expected results given the group inclusion criteria, although the uAR group had better than expected average reading skills even though none had participated in any talented/gifted reading programs. Boys in the iCL/P group also showed significantly more than expected participants in the at-risk range (n = 11; χ2 = 4.154, P = .042). While cleft type numbers were too low to conduct cleft type comparisons, examining cleft types revealed no risk for iCL (n = 0 at risk) and higher than expected rates of impairment for iCLP (n = 6 at risk) and iCP (n = 5 at risk) participants in the at-risk range (see Figure 2).
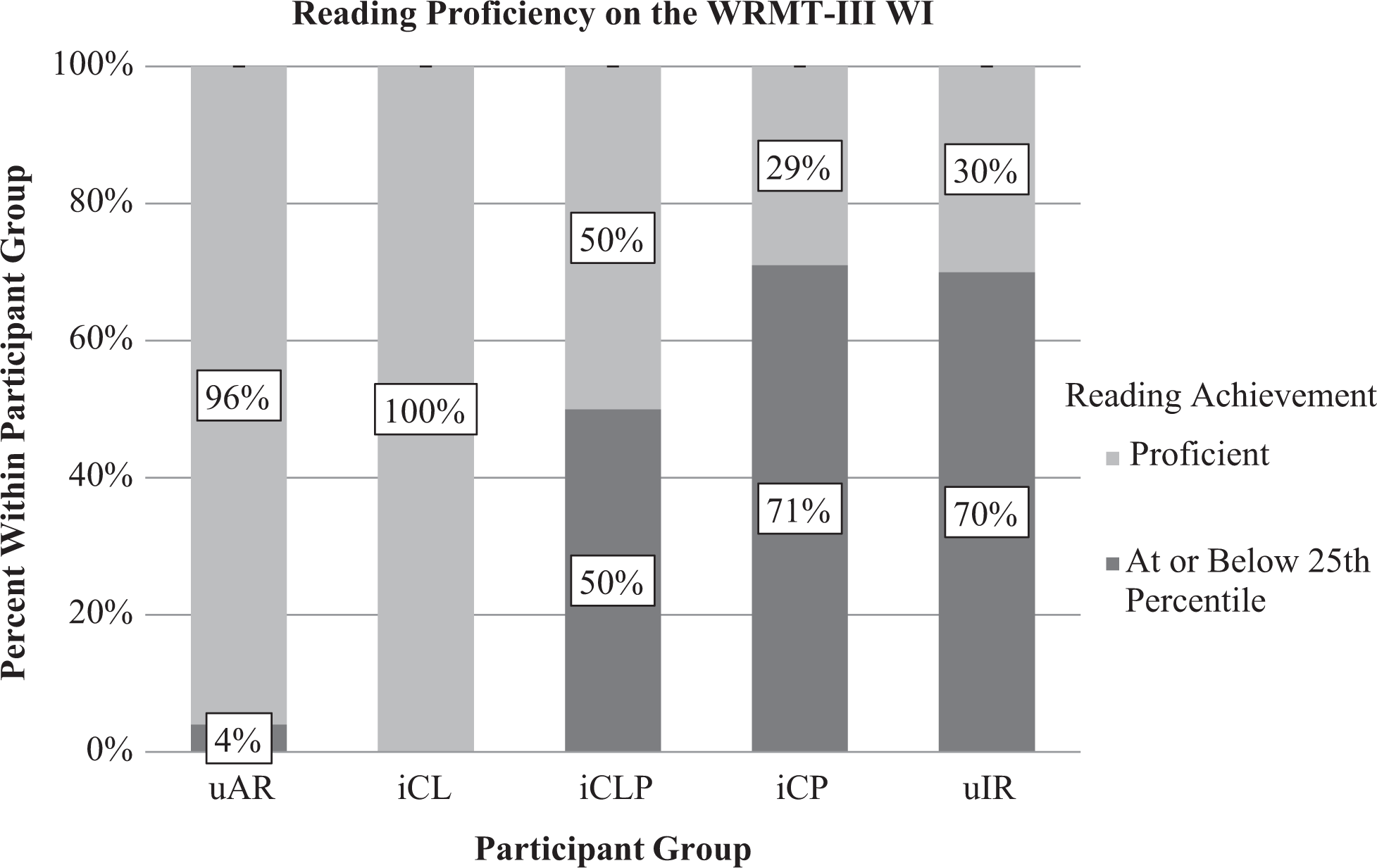
Comparison of participant groups by reading achievement level on the Woodcock Reading Mastery Test, 3rd Edition Word Identification (WRMT-III WI).
Dual-Route Measures
See Table 3 for all means, confidence intervals, and statistics related to the ANOVAs conducted in the following analyses.
Mean (95% Confidence Interval) Performance on Dual Route Measures Across Groups.
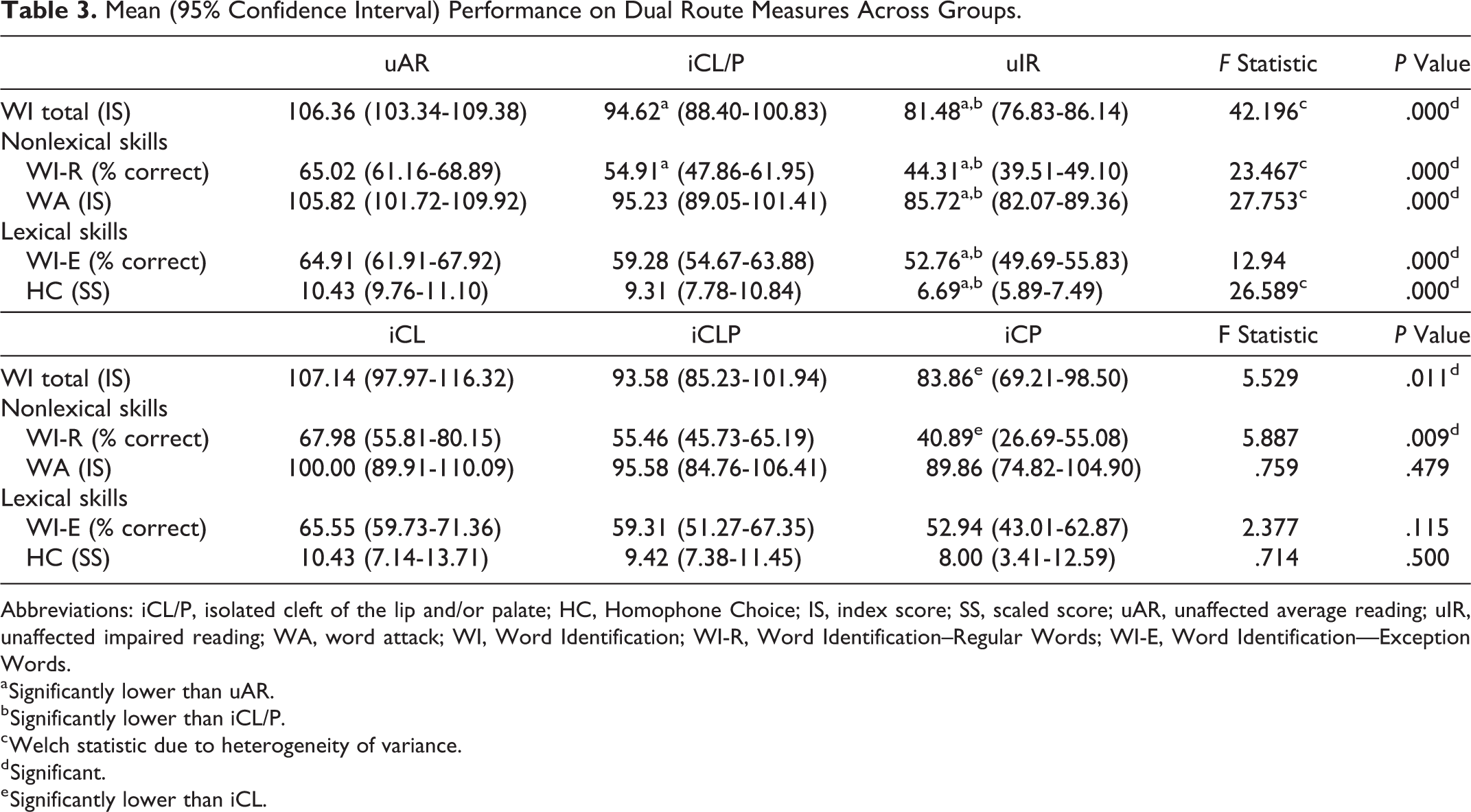
Abbreviations: iCL/P, isolated cleft of the lip and/or palate; HC, Homophone Choice; IS, index score; SS, scaled score; uAR, unaffected average reading; uIR, unaffected impaired reading; WA, word attack; WI, Word Identification; WI-R, Word Identification–Regular Words; WI-E, Word Identification—Exception Words.
a Significantly lower than uAR.
b Significantly lower than iCL/P.
c Welch statistic due to heterogeneity of variance.
d Significant.
e Significantly lower than iCL.
Word reading accuracy
Results of the ANCOVAs evaluating group differences indicated significant difference between the 3 participant groups on the WRMT-III WI overall score. Pairwise comparisons displayed uAR participants with the highest scores and iCL/P participants outscoring uIR participants. Analyses of variance results also showed significant differences between the 3 cleft types on the WRMT-III WI subtest. Pairwise comparisons showed iCL scored higher than iCP participants, but no significant difference was seen between iCL and iCLP, or iCLP and iCP.
Nonlexical performance
Significant differences were found between the 3 participant groups for percentage of correct words on WI-R (F = 23.467; P < .000). Pairwise comparisons showed uAR participants had higher percent regular words correct than both iCL/P and uIR participants. Mean index score on the WRMT-III WA subtest demonstrated the same pattern, with a significant difference between the 3 participant groups (F = 27.753, P < .000). Pairwise comparisons revealed uAR participants had higher scores than both uIR and iCL/P participants. Participants with iCL/P also scored higher than uIR.
Analyses of variance cleft type comparisons also found significant differences between groups for the percentage of correct words on the WI-R subtest (F = 5.887, P = .009). Pairwise comparisons for WI-R showed no difference in performance between the iCP and iCLP groups, but iCL participants significantly outscored iCP participants. No significant differences were seen between the 3 cleft types for WA performance (F = .759, P = .479).
Lexical performance
For WI-E subtest ANCOVAs, significant differences were found for percentage of words correct between the 3 participant groups (F = 12.94, P < .000). Pairwise comparisons showed uAR participants and iCL/P participants outscored uIR participants, but there was no significant difference in performance between uAR and iCL/P. Standard scores on the TOC HC subtest showed significant differences in performance between the 3 participant groups (F = 26.589, P < .000). Pairwise comparisons showed no difference in performance between uAR and iCL/P participants, but uAR and iCL/P participants both outscored uIR participants.
Analyses of variance for cleft type comparisons showed no significant differences in performance of words correct on the WI-E between difference cleft types (F = 2.377, P = .115). Pairwise comparisons showed no significant differences in performance of correct words on the WI-E between different cleft types, but iCL participants trended better than iCP participants. The same pattern was observed on the TOC, with no significant difference in performance found between the 3 cleft types (F = .714, P = .500).
Speech and Hearing
Among participants with iCL/P, Spearman ρ correlations between audiology and speech ratings and reading achievement measures yielded few significant correlations. Worse VPI rating was correlated with worse performance on the WI total score and WI-R, but this did not remain significant after Bonferroni correction (see Table 4).
Spearman ρ for iCL/P Participants Between Hearing/Speech Ratings and Early Literacy and Achievement Measures.
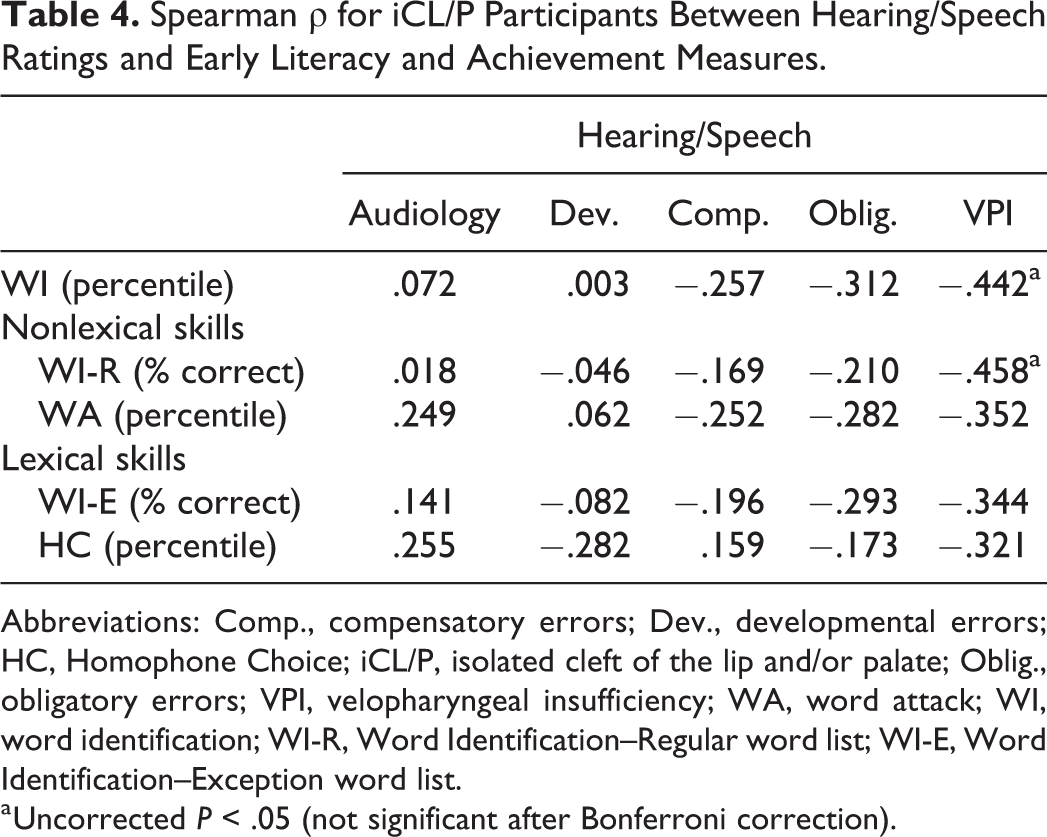
Abbreviations: Comp., compensatory errors; Dev., developmental errors; HC, Homophone Choice; iCL/P, isolated cleft of the lip and/or palate; Oblig., obligatory errors; VPI, velopharyngeal insufficiency; WA, word attack; WI, word identification; WI-R, Word Identification–Regular word list; WI-E, Word Identification–Exception word list.
a Uncorrected P < .05 (not significant after Bonferroni correction).
Discussion
The purpose of this study was to evaluate reading route differences in boys with isolated clefts compared to their unaffected peers with either average or impaired reading ability using the dual-route model. Aspects of the dual route were captured using specific subtests and coding on well-known achievement measures to measure lexical and nonlexical reading abilities.
Boys with iCL/P performed worse than unaffected average readers (uAR) only on regular word reading tasks. Although we screened for no participation in talented and gifted reading programs as a way to recruit average readers, the uAR group still performed higher than average. While there is not a direct relationship between intelligence and academic achievement (eg, students described as “twice exceptional” have high intellectual functioning paired with significant academic deficits), the higher average GAI of the uAR group should be taken into consideration when interpreting their higher reading scores.
Differences in performance appeared to be driven by the iCP group, who demonstrated a specific difficulty with decoding words. Reading performance patterns that emerged suggest boys with isolated clefts (iCL/P) possess a single deficit in reading impairments, with a breakdown only in their nonlexical skills. Isolated cleft lip and/or palate performance on lexical route reading tasks was left uninterrupted. Although we found a low risk of single word reading impairment in the iCL group, this may be due to low numbers of cleft participants. Future research should include larger enrollment for cleft type comparison. Unaffected impaired readers performed worse than unaffected average readers and boys with isolated clefts on both the regular word reading and pseudoword reading tasks. They showed impairments suggesting a double deficit, with a breakdown in both lexical and nonlexical reading skills. While there is evidence for global reading impairments in the uIR participants, only one route appears to be impaired in the iCL/P group.
Our findings are consistent with previous work (Richman, 1980; Richman and Eliason, 1984; Richman et al., 1988; Broder et al., 1998) that demonstrated boys with iCP having the highest risk for reading impairments. Based on our findings, this risk appears to include a specific difficulty with decoding and a breakdown of nonlexical skills, demonstrated by significantly worse performance on only the nonlexical reading tasks. Participants with iCP showed worse performance than other cleft types, but overall, they performed better than uIR participants.
The most significant finding of this study was that boys in the iCL/P group showed significantly more than expected participants in the at-risk range of reading impairment. While only one (4%) of our iCL/P participants had a previous diagnosis of a learning disability, there were still 11 (42%) participants who scored in the clinically at-risk range. This was highest in the iCP group, with 5 (71%) out of 7 participants demonstrating reading impairments. Although only one participant in the isolated cleft group had a preidentified reading impairment, many scored in the clinically at-risk range on a single word reading task. These numbers are significantly higher than anticipated, indicating underdiagnoses and untreated reading deficits among children with iCL/P, especially in boys with iCP. These findings are in line with the parent study (Conrad, 2018), which found that issues with phonological awareness, rote memory, and auditory working memory were the strongest predictors of decoding, while rapid automatized naming (RAN) was a stronger predictor of reading fluency. Although this is somewhat discrepant from previous research which found RAN being the biggest predictor of reading achievement (Richman et al., 1988; Richman and Ryan, 2003; Chapman, 2011), these studies did not break reading into its components of decoding, recognizing sight words, and reading fluency.
A history of hearing and speech impairments did not appear to have a significant effect on reading measures. However, participants with VPI had a trend for worse word reading skills—driven by issues with regular word decoding (within the nonlexical route). While speech likely has a role in early reading skills, there are other factors that also appear to affect reading development and achievement. Speech and hearing findings should be interpreted with caution as they were measured through retrospective medical chart reviews of evaluations by speech therapists and audiologists, which limited the type, quality, and consistency of the data. Only a small subset of the sample had received assessment of receptive and expressive language skills; future research should include more in-depth speech and language evaluation.
Conclusion
These findings are based on small numbers included in cleft type subtypes, and more research should be done to include larger numbers in each subset. Larger population-based studies (Collett et al., 2010; Collett et al., 2014; Persson et al., 2012; Wehby et al., 2014; Wehby et al., 2015) help reflect variability and representative levels of reading difficulty. Still, smaller studies like this are helpful in identifying specific neurological correlates of reading that may contribute to differences seen in larger studies. Future directions for this work will include females, larger numbers of each cleft type, the inclusion of genetic information to examine sex effects, further cleft type differences, and the potential influence of genetics on isolated cleft type and ability. Additionally, this research would benefit from collecting more information about specific learning disability diagnoses, interventions, speech, and hearing impairments. Lastly, this study did not evaluate other measures of reading achievement such as fluency or comprehension, which are also valuable measures of reading ability in children, but this was evaluated in the parent study (Conrad, 2018).
Because reading impairments can involve different weaknesses in a variety of reading skills, multiple reading skills should be considered upon evaluating reading impairments, especially in boys with isolated clefts. Assessing single reading skills like phonological awareness or sight word reading may not be enough to detect a full picture of reading impairments because one route may be left intact even if the other is disrupted. Skills from both the nonlexical and lexical routes should be assessed so as not to miss impairments.
Additionally, this subsample replicated findings initially found in the parent study (Conrad, 2018) again demonstrates a higher risk of reading deficits in boys with isolated clefts that are largely undetected. This group, while not performing as poorly as the unaffected impaired readers, still had many participants perform in the clinically at-risk range, particularly within the iCP subset. This subsample reinforces previous work that suggests a difference in the risk of reading deficits among cleft types. Boys with iCP should especially be screened for reading impairments and monitored in early development by their schools and cleft care teams to identify and treat reading deficits.
Clinically, parents and practitioners should be aware of a potential increased risk for reading impairments in children with iCL/P. Results of this study support the importance of early and routine screening as reading impairments can be seen by the age of 8. Results also support the increased risk for impairments found in the isolated cleft population, particularly those with iCP, and suggest evaluating both lexical and nonlexical single word reading ability to better target interventions for the specific type of reading impairment.
Some research argues that children with oral clefts who demonstrate low academic achievement do not catch up with their peers with age (Wehby et al., 2015). Other studies have shown improvement in reading ability in children with cleft (Richman and Eliason, 1984; Richman et al., 1988), using specific recommendations for reading treatment including focusing on phonics within a story context and avoiding sight word approaches in the isolated cleft population to best target specific reading issues, as these have shown to be the most successful (Richman and Ryan, 2003). Interestingly, similar interventions are also effective in children with developmental dyslexia (Lyon, 1999). It is necessary to screen the isolated cleft population early for learning problems and academic deficits as part of routine cleft care (Wehby et al., 2015), especially those with iCP.
Whichever treatments may be the most effective for children with isolated clefts and reading impairments, it is important to conduct thorough, targeted reading screenings early on that capture reading skills from both lexical and nonlexical routes so as not to miss reading impairments. Early identification and targeted interventions are particularly important when it comes to reading deficits, and it is important to assess multiple reading skills from both the nonlexical and lexical routes to get an accurate picture of reading ability, especially if impairments are frequently being missed within the isolated cleft population.
Footnotes
Acknowledgments
The authors would like to acknowledge the contributions of Ian DeVolder, PhD, for assisting in data collection, as well as the chapter leaders at Decoding Dyslexia and the International Dyslexia Association who aided with successful recruitment. Additionally, the authors would like to thank Kathy Angel for coding our word list into regular and exception words. Finally, the authors wish to thank the families who participated in this study; their time and effort is greatly appreciated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute of Dental and Craniofacial Research (award number DE024511) and the National Center for Advancing Translational Sciences of the National Institutes of Health (award number UL1TR002537).