
Abstract
Objective:
A diagnosis of a congenital craniofacial condition can have a significant impact on the psychological well-being of the affected family. As the first health professionals likely to come into contact with families, nonspecialists, such as diagnostic sonographers, midwives, and health visitors play a crucial role in facilitating familial adjustment. Yet, previous research has demonstrated parental dissatisfaction with the care delivered by nonspecialists. The aim of this study was to investigate the provision of care for families affected by craniofacial conditions from the perspective of nonspecialist health professionals, with a view to informing the development of educational materials.
Design:
Individual semistructured telephone interviews (n = 14) were conducted with 3 diagnostic sonographers, 2 fetal medicine consultants, 3 midwives, 4 health visitors, and 2 children’s nurses.
Results:
Participants identified a range of barriers to the delivery of optimal care, including dealing with parental reactions, time pressure, hospital protocols and resources, a lack of contact with specialist craniofacial teams, and the emotional impact of delivering a diagnosis. Most participants had received no prior training in the area of congenital craniofacial conditions, while those who had felt current training materials were insufficient. All participants expressed a desire for further training and provided guidance regarding preferred content and format.
Conclusions:
This study provides insight into the challenges faced by nonspecialists, as well as a range of information and training needs that could improve their knowledge and confidence. Suggestions for the development of educational materials for nonspecialist health professionals are made.
Introduction
In high-income countries, fetal anomaly screening at 18 to 21 weeks gestation now routinely includes screening for a cleft lip (eg, Public Health England, 2013). Other craniofacial anomalies may also be detected during this scan. If identified, expectant parents are usually given a second appointment to confirm the diagnosis and to discuss options with a fetal medicine consultant. A cleft palate is rarely detected during antenatal screening, and therefore almost all are diagnosed following the birth. A visual assessment of the palate should be carried out, and additional craniofacial anomalies should be screened for (Royal College of Paediatrics and Child Health, 2014). In all cases, a referral should be made to the specialist cleft/craniofacial team within 24 hours of the diagnosis (Public Health England, 2013).
Whether identified antenatally or postnatally, a diagnosis of a congenital craniofacial condition can have a significant impact on the psychological well-being of the parents and the family unit as a whole (Nelson et al., 2012a; Feragen and Stock, 2017). Parents have reported complex emotional responses to the diagnosis, including grief, shock, anger, guilt, and worry (Nelson et al., 2012a), in addition to raised levels of stress, anxiety, and depression (Stock et al., 2019a). Parents must grapple with feeding difficulties, process a wealth of new medical information, and embark on a daunting, long-term multidisciplinary health-care pathway (Nelson et al., 2012b), which often involves surgical intervention within the first year of the child’s life.
As the first health professionals likely to come into contact with expectant or new parents, diagnostic sonographers, fetal medicine consultants, and midwives play a crucial role in facilitating parental adjustment to the diagnosis. These nonspecialists must impart the news of the diagnosis to the family, explain the prognosis of the condition, discuss the option of further screening tests and termination of the pregnancy, and make the appropriate referrals. Midwives are also important in the delivery of a comprehensive feeding plan. Later, health visitors will take over responsibility for postnatal care from the midwives, and children’s nurses will be on hand to support the family through early medical treatment.
Satisfaction with health care is a key predictor of parental well-being and familial adjustment (Stock et al., 2019a). Prior research has indicated that families value health professionals’ expertise and interpersonal skills, as well as the continuity and coordination of care (Knapke et al., 2010; Nelson and Kirk, 2013). Although the service provided by the specialist craniofacial teams is consistently highly rated (Nelson and Kirk, 2013; Feragen et al., 2017), previous research has demonstrated parental dissatisfaction with the care delivered by nonspecialist health professionals. During the diagnostic experience, parents have reported a lack of knowledge among nonspecialists about these conditions and their long-term implications, and/or the delivery of inaccurate, inconsistent, or overwhelming information (Stock and Rumsey, 2015; Searle et al., 2016; Searle et al., 2018; Costa et al., 2019; Stock et al., 2019b). In the case of an antenatal diagnosis, parents have also reported feeling rushed to make decisions regarding further screening tests and/or termination of the pregnancy (Searle et al., 2016; Stock et al., 2019c). Following the birth, the late diagnosis of cleft palate, conflicting information surrounding feeding methods, and a lack of support during home-based care have also been described by parents (Lindberg and Berglund, 2014; Stock and Rumsey, 2015; Tierney et al., 2015; Searle et al., 2016; Costa et al., 2019). In addition, specialist health professionals working within craniofacial teams have communicated that much of their initial consultations with parents are spent trying to dispel myths, correct inaccuracies, and reduce parental distress, as a result of negative interactions with nonspecialist health professionals (Stock et al., 2019d).
Although a breadth of research detailing parental dissatisfaction with the care provided by nonspecialist health professionals now exists, few studies have pursued potential solutions. Further, the perspective of nonspecialist health professionals has remained absent from the literature. The aim of the current study was to investigate the provision of care for families affected by craniofacial conditions from the perspective of nonspecialist health professionals, with a view to informing the development of educational materials.
Method
Design
This study utilized individual semistructured telephone interviews to elicit the views of nonspecialist health professionals working in a variety of disciplines.
Procedure
Ethical approval for the study was provided by the Faculty Research Ethics Committee at the University of the West of England. Health professionals were invited to participate in the study using a variety of different methods, including advertisements on social media and department-wide e-mails to university and hospital-based staff. Potential participants contacted the researcher by e-mail to express an interest in the study and were subsequently sent information about what the study would entail, as well as ethical considerations, such as their right to withdraw. A mutually convenient time to conduct the telephone interview was then agreed with each participant. Participants were given several opportunities to ask any questions throughout their involvement in the study. Verbal informed consent from each participant was audiorecorded before the interview began. All interviews were conducted by the first author, who is trained in interviewing methods. The interview itself consisted of 4 broad areas: health professionals’ training and employment history and their understanding of their role, experiences of working with families affected by craniofacial conditions, current approaches to service delivery for these families, and views on if and how services could be improved. Interviews lasted 57 minutes on average.
Participants
Participants in this study (n = 14) included 3 diagnostic sonographers, 2 fetal medicine consultants, 3 midwives, 4 health visitors, and 2 children’s nurses. Six participants also held an academic post at the time of the interview. Ten participants were female, and all participants were white British. The average length of time participants had spent working in their roles since qualifying was 13 years (range: 3-30 years). All participants were based in the United Kingdom and had prior experience of working with families affected by cleft lip and palate and/or other congenital craniofacial conditions.
Data Analysis
Interviews were transcribed verbatim and subjected to inductive thematic analysis. All transcripts were analyzed by the first and second authors, who are trained in qualitative analysis. The following steps were taken, in accordance with Braun and Clarke’s 2006 guidelines: (1) becoming familiar with the data, (2) identifying interesting features of the data, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) producing the report. Analysis was seen as a recursive process, and detailed notes were written throughout. A high degree of commonality was found between interviews, and 14 interviews were therefore deemed sufficient to address the research question effectively. Themes were chosen for their prevalence and/or their importance (or “keyness”) in relation to the research question.
Results
Thematic analysis identified 2 key themes within the data: (1) Barriers to the Delivery of Optimal Care, and (2) Nonspecialists’ Training Needs. Since themes were consistent across all disciplines, data were merged. Each theme, composed of several subthemes, is described in further detail below and illustrated using exemplar quotes.
Barriers to the Delivery of Optimal Care
Handling Parents’ Reactions
Particularly in the case of the 20-week anomaly scan, participants reported that parents could often be unprepared for hospital appointments and/or unaware of the purpose of an appointment. Very often parents want pictures and they want to know the gender…Sometimes they bring their whole family and it’s very much a social event. That’s the problem really because it’s an anomaly scan…they don’t always know why they are there. (Diagnostic Sonographer #2) Every family is different, so every visit is different…We try to judge what each family understands and what information or support they might need…We have to assess on the spot and adapt quickly and that can be a real challenge…Even when you think you have a formula that works, you will find that it still doesn’t work for everyone. (Health Visitor #3)
Time Pressure
Participants stated that the limited time allocated to each of their patients could be a barrier to delivering information sensitively and to providing personalized care. Within 30 minutes we have to do the precounseling, the scan itself, take pictures, assess the gender of the baby, and deal with any anomalies, as well as fill out the paperwork and get a second opinion…You might also be running late and have the next patient waiting outside, so you are always under a fair amount of pressure. (Diagnostic Sonographer #2) We might only get a small handful of opportunities to see the families before and after their child has surgery…so you want to build that rapport and get as much information in that time as you can, so you can work out how best to support them. (Children’s Nurse #1)
Hospital Protocols and Resources
Participants described how the delivery of a suspected diagnosis was affected in part by the hospital environment. To be honest it’s a minefield because…we don’t have an environment which is conducive to counselling parents when they’re distressed…You just can’t do it in a scan room. (Diagnostic Sonographer #2) It could be a Friday evening or Saturday morning when I’m scanning these women, and hardly any other staff are around…If Monday is a [national holiday] too or if someone is off sick then it won’t even get to the doctor’s desk until Wednesday. That’s an unacceptable waiting time in my opinion. (Diagnostic Sonographer #3) How efficiently families get referred on can depend on whether you have a fetal medicine department within the hospital where the scans are performed. (Fetal Medicine Consultant #2) The 2 other hospitals I’ve worked in, they did things very differently to the hospital I’m in now…I know from speaking to colleagues that they approach situations in different ways…We don’t always agree on what is the best approach. (Health Visitor #2)
Working Alongside Specialists
Participants described how it could sometimes be a challenge to make contact with specialist craniofacial teams. The parents mentioned that I may be able to do a joint visit with the specialist cleft nurse…I thought “fantastic!” so the parents gave me the number and it just took weeks and weeks until I was able to speak to somebody…I know they’re as busy as anyone…but it was really frustrating because I knew the parents were relying on me. (Health Visitor #4) I think there is a risk of conflicting advice…What can happen sometimes is that babies who struggle to feed go straight onto formula milk…I appreciate they may not be able to breastfeed, but my biggest concern is that clefts teams don’t fully appreciate the nutritional benefits that come with breast milk…and the importance of baby–parent bonding. (Midwife #1)
Emotional Impact on Nonspecialist HPs
Finally, participants described the emotional impact that can sometimes occur when working with a family affected by a congenital condition. I’ve always got a fear that the family are going to remember me as the lady who ruined their pregnancy…Especially for newly qualified sonographers, the 20-week scans can be very daunting. (Diagnostic Sonographer #1) I can get so worried thinking “is this family missing out?” because there’s something they need to know that I don’t know…I get quite frustrated and anxious…You also don’t want to go to somebody’s house and for it to be obvious that you don’t know what you’re talking about. (Health Visitor #1)
Nonspecialists’ Training Needs
Experiences of Prior Training
The majority of participants reported that they had received no training on congenital craniofacial conditions. In terms of training, there was absolutely nothing. It all comes down to self-inquiry and how self-driven you are…A lot of the time I’ll just be improvising based on something I’ve read. (Midwife #2) While I was a student the curriculum was focused on conceptual holistic nursing…You might be lucky to learn about individual conditions on placement, but otherwise they don’t really feature. (Children’s Nurse #2) One example is the ‘Breaking Bad News’ training, which tends to be centered around telling parents that their baby has died…It’s never usually about breaking news in other circumstances, such as anomalies…There are some skills you can transfer across but [the training] definitely doesn’t cover all aspects. (Diagnostic Sonographer #1) What’s interesting about craniofacial conditions is that sometimes they can be isolated, and sometimes they can be part of an underlying genetic abnormality…The level of complexity can vary considerably, so we don’t necessarily know the significance of the diagnosis until after the birth, which makes delivering balanced information all the more difficult…I haven’t come across any training that addresses the nuances of that. (Fetal Medicine Consultant #2)
Information Needs
All participants expressed a desire for further training in the area of congenital craniofacial conditions. Specifically, participants discussed a need to better understand the patient journey as a whole, in order to feel more confident during consultations. Anatomically and genetically I know what the condition is, but I’d like to be more confident in knowing what the surgery will involve, the treatment pathway…what comes next for the family. (Fetal Medicine Consultant #1) I see families around the time of surgical admission, but that’s 6 months down the line already…I’d like to know more about what happens in that first 6 months…the screening and the preparation for surgery…so I can understand the journey [the family] has been on before they get to me. (Children’s Nurse #2) There are things outside the normal guidelines that I don’t know…For example, cleft lip is going to have a huge impact on the weaning process…and it’s also done earlier because the baby needs to be prepared for surgery…My nightmare would be to walk in and give a family our standard advice, only to find out that it’s completely wrong. (Health Visitor #1) I understand what the conditions are, but it’s also about what the diagnosis will mean for the parents…How do you assess how they’re coping with their baby’s upcoming surgery?…How do you make sure they can handle other people’s reactions if they go out [in public]? What’s the best way to check on the mental health of the mums and dads and check how their relationship is doing? (Health Visitor #4) One of the main challenges for me is when parents see their child after surgery and suddenly their child looks different…I’m well versed in reassuring parents about the operation, any side effects, recovery times, etc but actually preparing them for the appearance change is quite a unique thing. (Children’s Nurse #1) At the moment we’ve got nothing…It would be fantastic to have a leaflet or something to give the parents, so they didn’t go home waiting for their next appointment and wondering what this was…Some families don’t understand very much English, so there’s also a need for information to be translated. (Diagnostic Sonographer #1) I recently found out about the Cleft Lip and Palate Association website and Facebook page, which I think could be great resources for parents and would potentially stop them from using “Doctor Google”. (Health Visitor #3)
Training Preferences
When asked about the ideal training format, participants felt that face-to-face contact would be preferable but also acknowledged the difficulties of delivering this. You’d get the best buy-in from in-person sessions…running workshops for health professionals or coming to staff meetings…but of course that raises questions regarding people’s time and hospital resources…Another option would be delivering a lecture to students while they’re still training, although again it might be difficult to get it into the curriculum. (Health Visitor #4) In the absence of a study day, or in the case of focusing on specific conditions, I think online resources would be really good…Something you could look at as and when a case arises. (Midwife #3) I think it’s got to be bite-sized…It might be videos, tutorials…but it would have to be 4 to 5 minutes maximum on each topic area. (Children’s Nurse #1) Getting feedback from the families would be immensely beneficial…What were the things that helped them? What could we have done better? What language should we be using? (Children’s Nurse #2)
Discussion
The aim of this study was to investigate the provision of care for families affected by craniofacial conditions from the perspective of nonspecialist health professionals, with a view to informing the development of educational materials. The findings provide important insight into the challenges faced by nonspecialists, as well as a range of information and training needs which could improve nonspecialists’ knowledge and confidence, and the patients’ experience. Participants also provided guidance regarding the preferred content and format of educational materials.
Synthesis of Findings and Recommendations
Previous research has demonstrated parental dissatisfaction with the service provided by nonspecialist health professionals, such as sonographers, midwives, and health visitors, in the context of congenital craniofacial conditions. This has predominantly included a perceived lack of knowledge and empathy and has been reported to impact considerably on medical decision-making and long-term parental well-being (Lindberg and Berglund, 2014; Stock and Rumsey, 2015; Tierney et al., 2015; Searle et al., 2016; Searle et al., 2018; Costa et al., 2019; Stock et al., 2019a). The current study investigated these findings from a novel perspective and identified a number of barriers faced by nonspecialist health professionals.
First, nonspecialists are unlikely to have received training on the long-term implications of craniofacial conditions or the typical treatment pathway, which may affect their ability to accurately portray the significance of the diagnosis to parents. Existing training on how to “deliver bad news” may not comprehensively cover the skills needed to discuss the detection of an anomaly and the options that are subsequently available to parents. In addition, nonspecialists may not have access to guidance on how to deliver a diagnosis when the etiology is complex and the prognosis is uncertain. Expectant parents may be unaware that the purpose of the 18- to 21-week antenatal scan is to screen for anomalies, which may add to the shock experienced if an anomaly is detected. Participants acknowledged that nonspecialists may lack the skills required to judge parental need and provide appropriate counseling in the moment, particularly if they are early on in their career. Further, nonspecialists may be under pressure to keep to time and may be juggling competing demands, including ensuring they have satisfied the requirements of the full scan or postnatal assessment. Hospital protocols and resources may also play a significant role in the diagnostic experience. For example, the timing of assessments and the geographical location of the hospital may impact on the availability of senior staff who are able to provide a second opinion, and may result in a delay in referral. Some participants commented that their hospital lacked a separate, private room, conducive to supporting distressed parents, where the diagnosis could be discussed in more detail. Midwives and health visitors discussed the challenge of not knowing when and how to deviate from the usual care guidelines, for example, in the case of feeding and weaning infants. Participants also lacked understanding of the social and emotional impacts common to affected families and how to address the unique challenges posed by a congenital craniofacial condition, such as the child having a visible facial difference and undergoing appearance-altering surgery. Finally, participants described discrepancies between and within different hospitals in the approaches used to diagnose and treat affected families, resulting in variations in national care delivery.
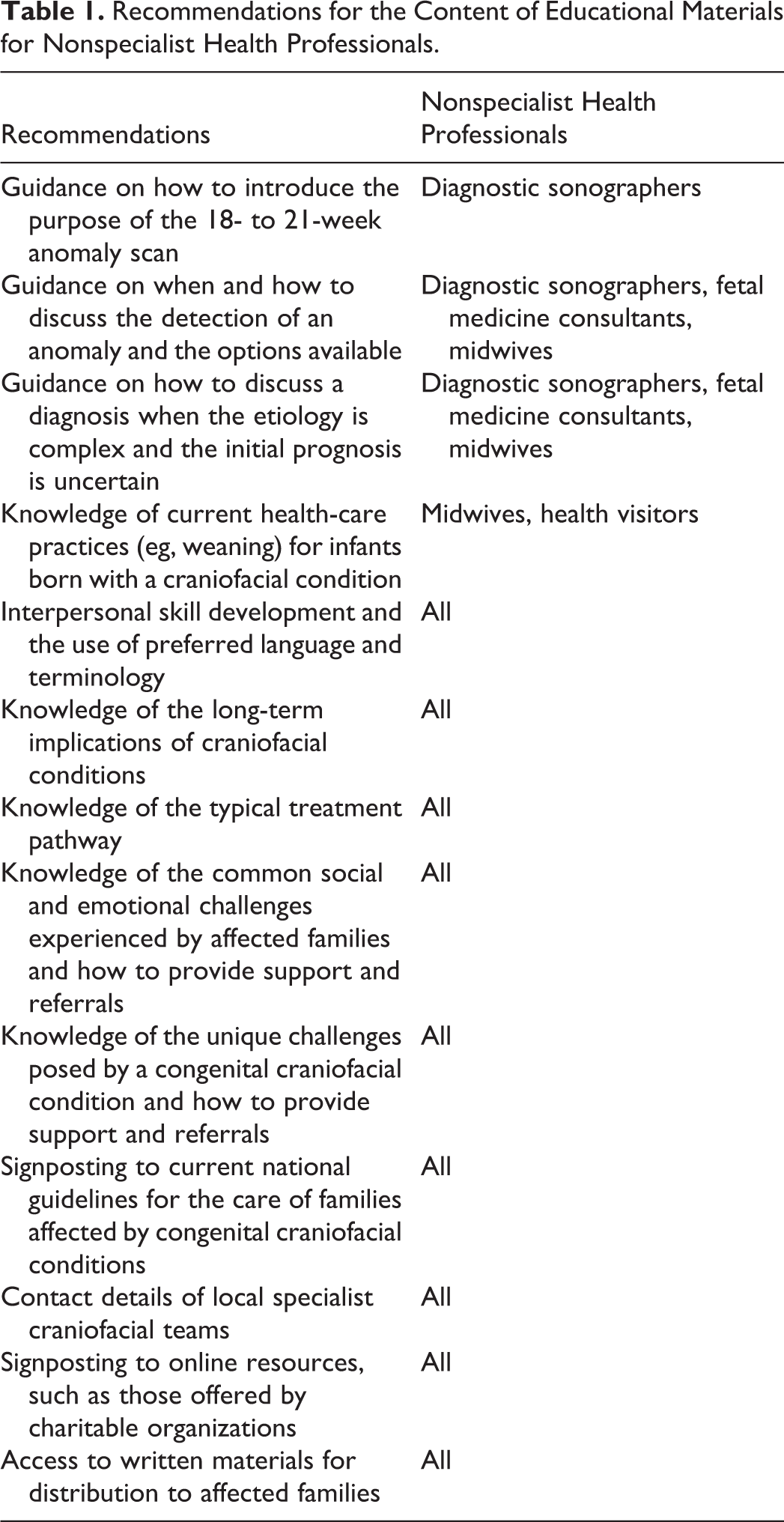
Although prior literature has suggested the need for training for nonspecialist health professionals (Searle et al., 2016; Costa et al., 2019; Stock et al., 2019b; Stock et al., 2019c), the current study is the first to examine the preferred content that such educational materials might include (see Table 1 for a summary). The provision of such guidance may also alert staff to the hospital resources that are required and reduce overall variations in the delivery of care over time. Further, access to educational materials may help to increase nonspecialists’ confidence and reduce the emotional impact described by some participants, which had resulted from a lack of knowledge and uncertainty surrounding the best approach to care. The present study has also highlighted a preference among nonspecialists for in-person training sessions, delivered to both students and qualified professionals. Where in-person sessions are less feasible, or if content needs to be condition-specific, then brief, complementary online training resources were requested. Participants also wanted access to written materials which they could give to parents in order to bridge any gaps between referrals and to prevent families accessing unreliable information via the Internet. This echoes previous research, which has demonstrated the importance of written resources for families following a diagnosis, during postnatal care, and in preparation for medical treatment (Knapke et al., 2010; McCorkell et al., 2012; Searle et al., 2016). Resources produced by various charitable organizations, such as the American Cleft Palate-Craniofacial Association (United States), the Cleft Lip and Palate Association (United Kingdom), and the Antenatal Results and Choices group (United Kingdom) could be ideal, but local hospitals do not always seem to be aware of these resources. One way of overcoming this challenge could be increased contact between local hospitals and specialist craniofacial teams. Participants felt that both parties could benefit from an increase in joint working, through the sharing of knowledge and resources, and by conducting combined visits with families where indicated. Such an approach may also help to improve the continuity of care and avoid the potential for conflicting advice to be given to families (Searle et al., 2016; Costa et al., 2019; Stock et al., 2019c; Stock et al., 2019d).
Recommendations for the Content of Educational Materials for Nonspecialist Health Professionals.
Methodological Considerations
When analyzed as a whole group, this study meets the sample size criteria recommended for this type of qualitative research (Braun & Clarke, 2006). However, participation from each individual discipline was small and cannot be deemed to be representative of nonspecialist health professionals as a whole. Nonetheless, commonality in the themes reported across disciplines was observed, and consensus on the preferred content and format of educational resources was reached. In order to ensure the relevance of resources for all nonspecialist health professionals, the future development of educational materials should involve close collaboration with nonspecialists, in addition to comprehensive evaluation of any resources that are produced.
Conclusions
This study investigated the provision of care for families affected by craniofacial conditions from the perspective of nonspecialist health professionals, with a view to informing the development of educational materials. The findings demonstrate a high degree of concordance between the experiences of nonspecialist health professionals and previously published reports provided by parents and craniofacial specialists. Current training for nonspecialist health professionals in the area of congenital craniofacial conditions appears to be insufficient, and opportunities for the development of further resources have therefore been suggested.
Footnotes
Authors’ Note
For access to any resources associated with this manuscript, please contact the corresponding author.
Acknowledgments
The authors are grateful to all the participants, and to the charitable organizations who helped to facilitate this study. The VTCT Foundation Research Team at the Centre for Appearance Research are Dr Amy Slater, Dr Heidi Williamson, Dr Nicola Marie Stock, Dr James D Kiff, Mr Nicholas D Sharratt, Mr Fabio Zucchelli, Ms Ella Guest, Ms Claire Hamlet, Ms Bruna Costa, Ms Jade Parnell, Ms Maia Thornton, Professor Emerita Nichola Rumsey, and Professor Diana Harcourt.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Vice Chancellor’s Early Career Researcher Development Awards (2016-17), granted by the University of the West of England, Bristol, and by the Vocational Training Charitable Trust Foundation (registered charity 1155360).