
Abstract
Objective:
There are minimal data available on nutrition after early repair of cleft lip and the factors influencing initiation of breastfeeding. This study assessed the impact of the length of surgery, length of ventilation support, and duration of hospital stay on breastfeeding rates after early cleft lip surgery.
Design:
This is a prospective observational cohort study comparing 2 hospitals providing early surgical repair of facial clefts from January 2014 to December 2016. Both hospitals are designated as Baby-Friendly Hospitals. Demographic and anthropometric data from mothers and newborns were recorded.
Setting:
Tertiary neonatal and pediatric surgery center.
Patients:
Hospital A: 61 newborns, Hospital B: 157 newborns.
Interventions:
Early (day 5 to 14) cheiloplasty in newborns with cleft lip or cleft lip and palate.
Main Outcome Measures:
Influence of duration of hospital stay, length of operation, and artificial ventilation on the rate of breastfeeding.
Results:
Significantly, more newborns were breastfed following early surgical repair of an isolated cleft lip compared to those with both cleft lip and palate, in both hospitals (hospital A 82% vs 0%, P = .0001, hospital B 66% vs 5%, P = .0001). Duration of hospital stay, length of operation, and duration of artificial ventilation did not significantly affect the rate of breastfeeding.
Conclusions:
The factors associated with early cleft lip repair (length of operation, length of ventilation support, and duration of hospital stay) do not affect breastfeeding rate.
Introduction
Cleft lip (CL) and cleft lip and palate (CLP) result from inappropriate facial fusion during the fetal period of development. The most appropriate timing of CL repair is still the subject of expert discussions (Hammoudeh et al., 2017). The operation can be divided according to its timing into early repair (neonatal), which is carried out in the first 2 weeks after birth, most often several days after birth and the late repair (around the age of 3 months of life).
The advantages of early CL repair are faster healing, better acceptance of surgery by parents and better nasal and cleft repair (Calteux et al., 2013, Hammoudeh et al., 2017). There are, however, some variations in timing depending on the specialized center. Most plastic surgery centers postponed the primary repair of the lip to the age of 10 to 12 weeks. The main reason for this is the presence of associated anomalies that may not be noticeable immediately after childbirth (Kummer, 2018).
The total unilateral cleft includes hypoplastic maxilla, concave middle third of the face, and deformed tooth arch. According to some authors, the lip surgery generally inhibits the sagittal growth of the maxilla (Normando et al., 1992). Whether early repair has a negative effect on the growth of the upper jaw is still not quite clear (Huang et al., 2002). A number of authors dealt with the influence of cheiloplasty on the development of the upper jaw, and the conclusions of their studies are not consistent (Kramer et al., 1994; Liao and Mars, 2005).
There are also limited data on the potential neurotoxicity of anesthetics used during early repair but no study has demonstrated a negative effect on neurodevelopment (Bang, 2015, Petrackova et al., 2015). After the exclusion of associated anomalies and careful preoperative examination, the risk of complications is minimal (Bang, 2015; Hammoudeh et al., 2017; McCann et al., 2019).
The American Cleft Palate-Craniofacial Association considers multidisciplinary treatment and strategy of nutrition very important (Farronato et al., 2014). Infants with orofacial cleft require the nutritional care and support of lactation specialists as early feeding difficulties in this population are very common. The major difficulty is the inability to create sufficient negative pressure during sucking (Smedegaard et al., 2008; Abbot, 2014; Boyce et al., 2019). During the feeding, infants’ lips flange firmly against the areola, sealing the oral cavity. The soft palate rises up and the oral cavity increases in size creating the necessary negative pressure important for sucking milk from the breast. Infants with CP or CLP have difficulty creating that negative pressure because the oral cavity cannot be adequately separated from the nasal cavity during feeding (Weber et al., 1986; Reid et al., 2007). This is related to the size and type of cleft (Reid, 2004). Infants with CL and a small soft CP can generate adequate negative pressure; however, infants with larger soft and/or hard CP may not (Mizuno et al., 2002; Masarei et al., 2007; Reid et al., 2007). Negative consequences may include prolonged feeding times, nasal regurgitation, reflux, and insufficient milk transfer (Kaye et al., 2017). Newborns with large clefts need special feeding methods, nutritional follow-up focusing on adequate weight gain, and prevention of dehydration (Cohen et al., 1992; Matsunaka et al., 2015; Gailey, 2016). There is no systematic review covering orofacial clefts and breastfeeding rates, and there is limited literature describing early cheiloplasty and breastfeeding outcome (Cohen et al., 1992; Harris et al., 2010; Gailey, 2016). The early cheiloplasty may cause delay in breastfeeding initiation, and disruption of skin-to-skin contact may decrease the breastfeeding rates as well (Moore et al., 2016). Separation from the mother negatively influences breastfeeding initiation and milk supply. The skin-to-skin care intervention improves breastfeeding outcomes, cardiorespiratory stability, and decreases infant crying (Crenshaw, 2019). We expected that general anesthesia, artificial lung ventilation, and prolonged hospital stay in the neonatal period could be the reason for impairment in the process of breastfeeding (McFadden et al., 2017; Crenshaw, 2019). The aim of our study was to determine the influence, if any, of the length of ventilation, length of surgery, and hospital stay on the rate of breastfeeding.
Methods
Design
This is a prospective multicenter observational cohort study performed on term infants and near-term infants (gestational age from 36 + 0 to 41 + 6 weeks of gestation) in 2 hospitals from January 2014 to December 2016. Both centers are members of the Baby-Friendly Hospital Initiative (BFHI). The study was approved by the Ethics Committees in both institutions.
Setting
Characteristics of both Baby-Friendly hospitals participating in the study: Hospital A—level 2 neonatal center with 2.200 deliveries per year, Hospital B—level 3 neonatal center with 3.100 deliveries per year. Hospital A was designated as BFHI in 1993, Hospital B in 2013.
Sample
The inclusion criteria for participants in the study were newborns with a CL or CLP having cleft lip surgery in the first 14 days of life. Infants with major congenital malformations, birth weight below 2 kg, those with a gestational age below 36 weeks, and infants of parents refusing early operation were excluded from this study. After delivery, all mothers were followed by medical teams promoting breastfeeding. All operations (in both hospitals) were done by the same surgeon within the first 14 days of life.
General anesthesia was done by inhalation of sevoflurane combined with intravenous sufentanil and midazolam. After intubation and fixation of the tube, the tamponade was done in order to prevent aspiration. The surgical method was described in a study by Borsky et al. (2012). To perform the primary cleft surgery, the original Tennison’s technique was modified (Gundlach et al., 1982). The marginal parts of the cleft were cut and 2 tissue flaps were prepared: the first one for deepening the upper oral vestibule (VF), the second one for deepening the base and the lateral side of the nasal passage (NF). The Tennison’s flap was used to complete the shortened philtrum on the cleft side. The orbicularis oris muscle was isolated and the repositioning of the nasal septum was completed. In the next stage, the suturing of the deepening of the upper vestibule with the prepared VF and the suturing of the base and the lateral side of the nasal passage with the NF were completed; simultaneously the partial closure of the alveolar defect with soft tissues was finished. The Tennison’s flap was pushed into a separate cut, and finally the red part of the upper lip was sutured. The rotated and dislocated nasal alar cartilage on the cleft side was released and its position and shape corrected. The incisions were closed with Vicryl 6/0 and covered with a sterile tape on the exterior side of the lip and silicon nostrils were inserted.
Care Following Surgery
After the repair, all newborn infants were transferred to the neonatal intensive care units (NICUs). The second day the plastic surgeon checked the surgical site. Scar care was provided by parents (cleaning of silicone nostrils and pressure massages). Nutrition after repair was provided by standard parenteral nutrition. Enteral nutrition was initiated within 10 hours after surgery (nasogastric tube feeding was commenced). Breastfeeding was initiated 24 hours after surgery.
Breastfeeding Support
Breastfeeding support was comparable in both hospitals, focusing individually on each mother and baby until discharge from hospital. Breastfeeding support and positioning were given pre- and postoperation. We followed The Academy of Breastfeeding Medicine clinical protocols for managing medical problems that may impact breastfeeding and human milk feeding (pre- and postoperatively). The protocol (ABM Clinical Protocol: Guidelines for Breastfeeding Infants with Cleft Lip, Cleft Palate, or Cleft Lip and Palate) is an updated guideline for the care of breastfeeding mothers and infants with orofacial cleft (Reilly et al., 2013; Boyce et al., 2019). All newborns were put to the breast immediately after delivery. Mothers had open access to a health professional specialized in orofacial cleft management, such as a clinical nurse specialist for advice on feeding and were educated on feeding cues and breastfeeding. Mothers were able to “room in” with their infants, having the infant taken to NICU for only 24 hours after repair. The following breastfeeding positions were recommended: For infants with CL: position was kept so that the CL was orientated toward the nipple. Football or twin style position was also preferred. For bilateral or extensive CL, a straddle position was used when appropriate. To decrease regurgitation and reflux of milk, semi-upright position was advised. For infants with CLP—even with a large cleft palate it is useful to position the breast toward the “greater segment”—the side of the palate that has the most intact bone. This position facilitates better compression of the breast. The nipple could not be pushed into the cleft. In infants with CL or CLP where direct breastfeeding was unlikely (wide clefts), the need for breast milk feeding was encouraged. Although no specific dimensions are reported, a wide cleft is associated with an increased risk of difficulty achieving intraoral pressure, thus reducing the likelihood for successful breastfeeding (Smedegaard et al., 2008). For formula or human milk feeding, various feeding devices were used. On an individual basis and dependent on maternal compliance, Haberman feeder, spoon, syringe, or bottle were used. Mothers were continuously supported to express milk by provision of an electric breast pump (Meier et al., 2016).
Measurement
The breastfeeding patterns were described according to the World Health Organization 1991 classification. Breastfeeding was defined as exclusive breastfeeding at the time of discharge; it means that the infants received only breast milk and no other liquids/formula. Human milk feeding was defined as feeding with human milk which is not given to the infant directly from the breast (Noel-Weiss et al., 2012). The type of feeding was assessed in all infants at discharge from hospital. Parameters regarding the surgery, anesthesia, and ventilation support were recorded in both hospitals and compared to breastfeeding rates in CL and CLP groups.
Data Collection
Demographic data from mothers and newborns were systematically recorded from maternal and neonatal charts.
Data Analysis
Data were analyzed using SPSS 13.0 software’s values of less than 0.05 were counted as statistically significant. For the quantitative parameters, the nonparametric Mann-Whitney test was used because the observed parameters did not have a normal distribution and the parametric and χ2 dependency tests could not be used. For the qualitative parameters, the χ2 dependency test or Fisher test (in small sample sizes) was used.
Results
A total of 218 newborns were recruited into the study (hospital A group included 62 infants, hospital B 156 infants). Maternal and neonatal demographic data are presented in Tables 1 to 3. No significant differences between hospital A and hospital B were found in terms of demographic variables (Table 1). On the contrary, surgical characteristics (length of operation, anesthesia, and duration of hospital stay) of hospital A and hospital B revealed significant differences (Table 1).
Demographic and Surgical Characteristics of All Patients From Group A—Thomayer Hospital and Group B—University Hospital Motol.a,b
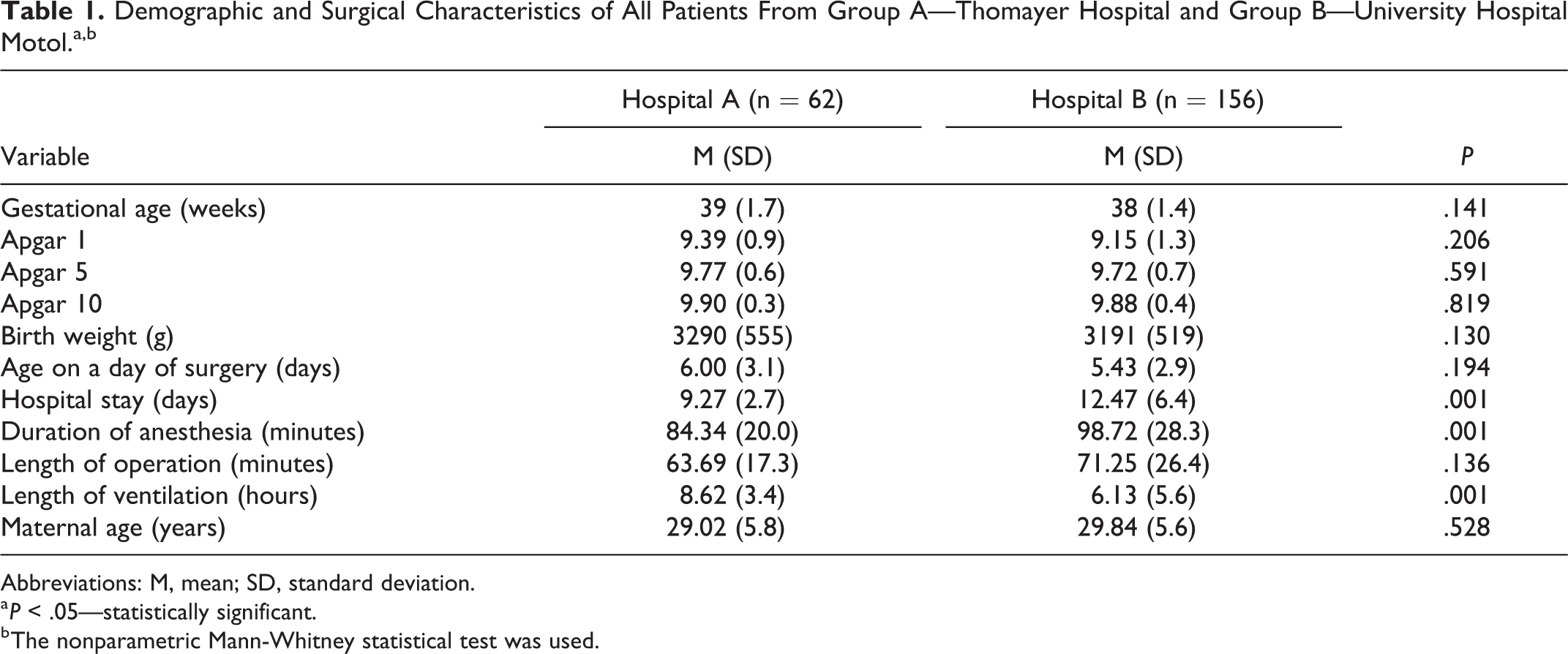
Abbreviations: M, mean; SD, standard deviation.
a P < .05—statistically significant.
b The nonparametric Mann-Whitney statistical test was used.
Demographic and Surgical Characteristics of Patients With CL and CLP From Group A—Thomayer Hospital and Group B—University Hospital Motol.a,b
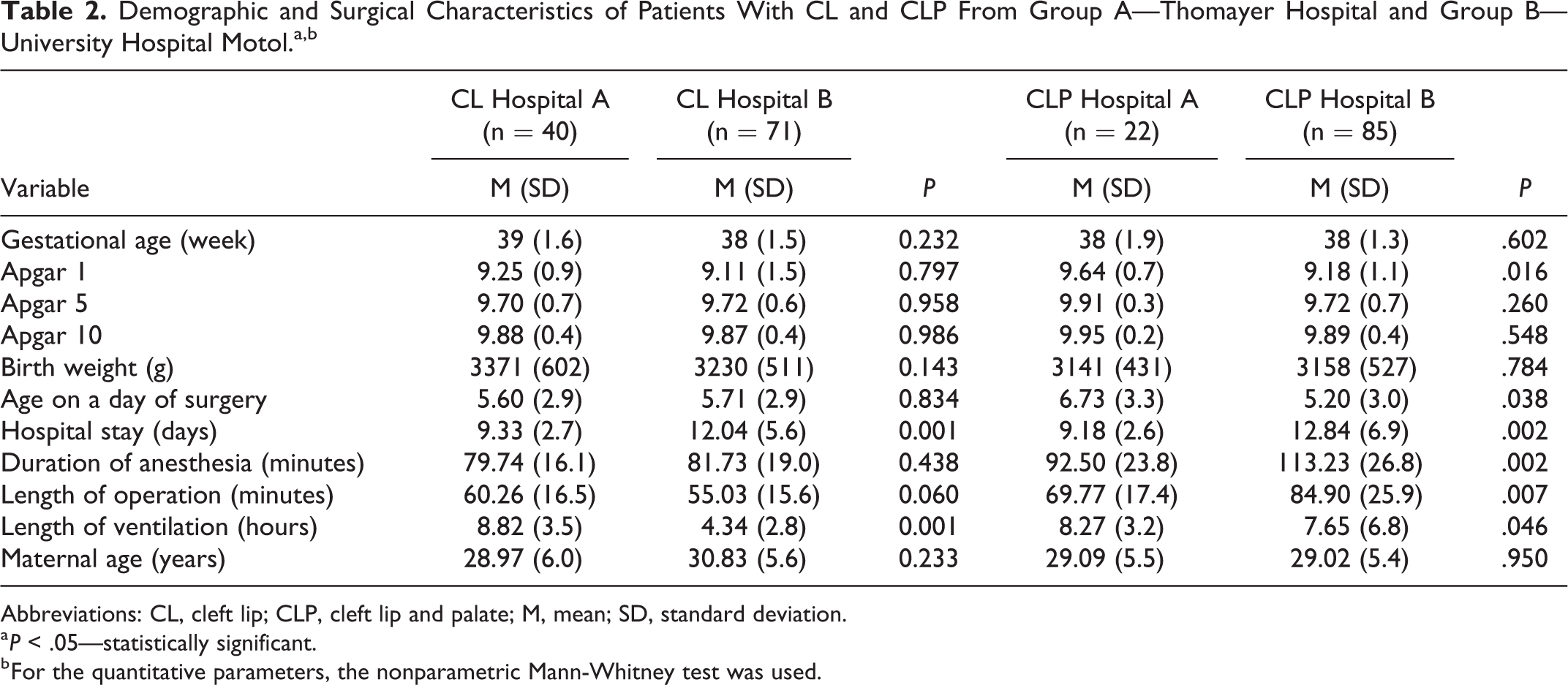
Abbreviations: CL, cleft lip; CLP, cleft lip and palate; M, mean; SD, standard deviation.
a P < .05—statistically significant.
b For the quantitative parameters, the nonparametric Mann-Whitney test was used.
Demographic and Breastfeeding Characteristics of Patients With CL and CLP From Group A—Thomayer Hospital and Group B—University Hospital Motol.a,b,c
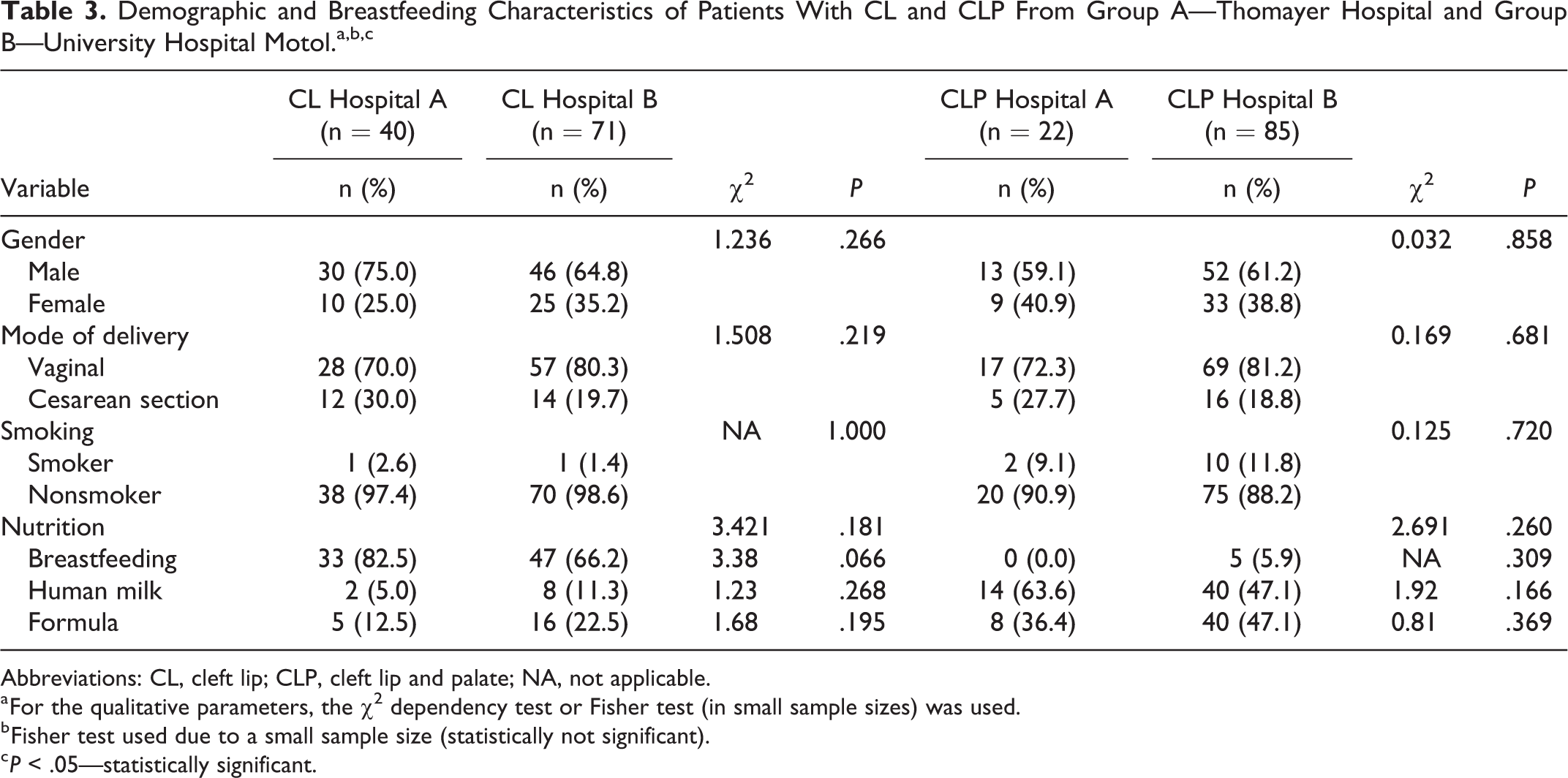
Abbreviations: CL, cleft lip; CLP, cleft lip and palate; NA, not applicable.
a For the qualitative parameters, the χ2 dependency test or Fisher test (in small sample sizes) was used.
b Fisher test used due to a small sample size (statistically not significant).
c P < .05—statistically significant.
Table 2 presents demographic and surgical characteristics of CL and CLP subgroups. Significant differences in demographic variables between hospital A and B were found in Apgar scores in the first minute in the CLP group and age on day of surgery in the CLP group. Surgical characteristics of CL and CLP subgroups showed significantly shorter hospital stay and prolonged time of ventilation in both CL and CLP groups and shorter duration of anesthesia and length of operation in the CLP group in hospital A (Table 2).
Significant differences between hospital A and hospital B in breastfeeding rates at discharge were not found (P = .309). For CL groups, the breastfeeding rate at discharge was higher in hospital A, but not statistically significant (P = .066; Table 3). Significantly more newborns were breastfed following early surgical repair of an isolated CL compared to those with both CLP, in both hospitals (hospital A 82% vs 0%, P = .0001, hospital B 66% vs 5%, P = .0001; Table 3).
Discussion
In babies with orofacial cleft, surgery may negatively impact the process of breastfeeding because of disruption of skin-to-skin contact and pain after operation. Nevertheless, breastfeeding in newborns with CL in our study was successful in hospital A and B (82.5% vs 66.2%, respectively). We do not have an exact explanation for this difference between hospital A and B (although not statistically significant). Hospital A has historically more breastfeeding experience than hospital B (hospital A was designated as BFHI in 1993, hospital B in 2013). We may speculate that even with the same guidelines the experience of the staff may play a role in specific cases. The length of hospital stay, surgery, and artificial ventilation during and after surgery differed significantly. The longer ventilation time in hospital A (in both the CL and CLP groups) can be explained by different hospital settings. Hospital B has a shorter distance between the NICU and the operating theater; hence, the transport of the baby after the operation and consequently the ventilation period was not as long as in hospital A. The second reason could be the different weaning policy according to institutional guidelines in both neonatal departments. Longer duration of surgery in hospital B could be due to the fact that there was a special otolaryngology team in hospital B and before every surgery 3 dimensional measurements of the palate were done (Valentova-Strenacikova and Malina, 2016). Although the differences in length of surgery and artificial ventilation during and after surgery were statistically significant, these may not probably have a significant influence on clinical outcome. Nevertheless, these differences and their potential impact were not addressed in clinical studies so far.
There are only a limited number of studies focused on the rates of breastfeeding in CL or CLP infants before and after surgery. A study by Cohen et al. (1992) presented breastfeeding rates of 32% in infants operated on within 28 days of birth. Harris et al. made a retrospective study of 99 babies and analyzed the safety of cleft repair. All repairs were undertaken within 28 days of birth, and the breastfeeding was achieved in 54 babies by the time of discharge (Harris et al., 2010). Study by Alperovich (patients with CLP) evaluated the rates of breast milk feeding among patients with CLP at a large Craniofacial Center. A total of 67% of infants received human milk for some period of time (Alperovich et al., 2017). Duarte et al. compared feeding approaches in children with CLP before and after operation. They did not focus on monitoring the rate of breastfeeding, but pointed out those alternative methods of feeding were beneficial (Duarte et al., 2016). Other studies focused on the growth outcome and the frequency of postoperative complications and did not determine mode of nutrition (Bessell et al., 2011; Zhang et al., 2017). Our data from one cohort of infants delivering in BFHI hospital showed a high breastfeeding rate in the CL group (78%; Burianova et al., 2017).
To demonstrate the level of breastfeeding in the healthy population, we present official data for Czech Republic from 2017. The Institute of Health Information and Statistics of the Czech Republic conducted a study in 2017 and showed that 83.5% of newborns from the healthy population were breastfed at the time of discharge from hospital (Czech Republic Institute of Health Information and Statistics, 2017). Higher breastfeeding rates in the study cohort compared to international data are probably due to BFHI setting in both hospitals. Czech Republic has generally high rates of breastfeeding due to government support of lactation consulting. The length of hospital stay of a mother and child is not strictly limited in cases of problems related to breastfeeding and also mothers are probably more motivated by their social environment than in other countries. We also addressed the weight gain of the study population. Mean weight loss during hospital stay was 6.9% of birth weight, median 6.9, and interquartile range (IQR) 2.1. Day of maximum weight loss was mean 3.4, median 3.0, and IQR 1.0. The weight at discharge was in 98% of babies equal or more than birth weight, this fact could be considered a positive marker of successful lactation.
The present study also confirmed the very low breastfeeding rate in the patients with CLP after repair of the CL. However, the number of patients with CLP receiving human milk was quite high in hospital A and B (63% and 53%, respectively). For this population with CLP, human milk can be especially helpful in providing protection against diseases of early childhood, mainly the risk of respiratory and ear infections later on (Sheahan et al., 2003).
We evaluated factors that would affect breastfeeding: the age of the mother, smoking, the mode of delivery, gestational age of the child, and the need for resuscitation (Regan et al., 2013; Maastrup et al., 2014; Kitanoet al., 2015; Napierala et al., 2016; Maharlouei et al., 2018). Unhealthy, immature newborns, and newborns with other congenital defects were excluded. We are aware that socioeconomic status may also influence breastfeeding rates. We did not have access to data regarding socioeconomic status (hospital policy). The possible limitation of this study is that we could not compare our results to another cohort from non-BFHI hospitals. Currently, there are no non-BFHI hospitals concentrating on patients with CL for early operation in the Czech Republic. As all infants in the Czech Republic undergo early lip repair, we are unable to compare breastfeeding outcomes of infants undergoing early repair with late repair.
In spite of these limitations, our study is the first to determine the impact of length of surgery, artificial ventilation, and length of hospital stay on breastfeeding in neonates after early CL closure in a large cohort.
Conclusion
The differences in length of surgery, artificial ventilation, and hospital stay did not have a significant impact on the rate of breastfeeding in newborns after early CL repair. Based on breastfeeding rates of patients after early operation of CL, we assume that BFHI hospitals approach may positively influence breastfeeding rates in these patients.
Footnotes
Acknowledgments
The authors would like to thank Alena Dohnalova, MSc, for statistics.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by Ministry of Health, Czech Republic—conceptual development of research (Thomayer Hospital—TH, 00064190).