
Abstract
Introduction:
Children born with a cleft palate ± lip are at risk of developing speech and language difficulties, which may require intervention from a speech and language therapist (SLT). To date, there is no strong evidence to support one approach to intervention over another, neither is it clear which approaches or methods of provision are commonly used.
Objectives:
To describe the range of speech and language therapy interventions being used with children born with cleft palate in the United Kingdom up to 5 years of age. To explore the different ways, interventions are being delivered.
Design:
A prospective study to conduct 9 semi-structured focus groups. Iterative content analysis was completed.
Setting:
Regional Cleft Lip and Palate Centers in the United Kingdom.
Participants:
Sixty-two speech and language therapy professionals from specialist cleft teams and community services.
Results:
Four main codes were identified: “intervention approaches,” “service delivery models,” “decision-making and rationale,” and “patient-centered care.” Participants frequently discussed how they adopt an eclectic style when delivering intervention, the importance of an individualized approach for each child and service delivery constraints, such as a lack of resources.
Conclusion:
Insight into the multitude of intervention approaches used by SLTs, aspects which influence their decision-making and the variability of service delivery models were gained. Uncertainty regarding which intervention approaches and methods for delivery are most effective provides rationale for future research, to improve the effectiveness of speech and language intervention for children with cleft palate ± lip.
Introduction
Children born with a cleft palate, with or without a cleft lip (CP ± L), are at risk of developing speech, language, and communication difficulties (Vallino-Napoli, 2011). Although a CP is usually repaired during the first year of life, atypical speech patterns may prevail, with the potential for impact on intelligibility and consequences for a child’s future social and educational progress (Richman et al., 2012).
Across the United Kingdom, speech outcomes are audited at the age of 5 for children with CP ± L. This is for the purpose of measuring the impact of interventions which have been provided at an individual and service level (Britton et al., 2014). Analysis of this audit data has shown that 38.8% of the population do not achieve normal speech by age 5 (Deacon et al., 2018). What constitutes “normal speech” is subjective and may vary from one person to another, but work by Sell et al. (2015) provides more objective data and shows that for some children, their speech is severely affected. They reported that 17.2% of children born with CP ± L are classified as “only just intelligible to strangers” or “impossible to understand” at 5 years of age. These figures are reflected in data which record the need for speech and language therapy in this population. Evidence from the literature indicates that more than 50% of children born with CP ± L require intervention from a speech and language therapist (SLT) during childhood (Hardin-Jones and Jones, 2005; Peterson-Falzone et al., 2009), suggesting that problems with speech are often persistent and have a significant impact for the child concerned.
Interventions delivered by SLTs may target a range of difficulties including speech sound substitutions, comprehension, and expressive language and social communication skills. Improvement in speech, language, and communication skills is expected to impact positively on other aspects, such as the child’s literacy skills, confidence, participation, and well-being (McCormack et al., 2009; Chapman, 2011; Bercow, 2018).
Speech and Language Therapy for Children With CP ± L in the United Kingdom
Children born with CP ± L may have multiple speech, language, and communication needs, some of which could be unrelated to their cleft (Vallino-Napoli, 2011). The interventions delivered by the SLT primarily focus on outcomes related to the child’s speech and language skills, for example, articulating specific sounds, the expression of ideas and information, or the processing and understanding spoken words.
Children with CP ± L who require speech and language therapy intervention typically receive this from the government-funded National Health Service (NHS); though in recent years, the availability and uptake of privatized, independent speech, and language therapy have become increasingly popular (Bercow, 2008). Within the NHS, both regional specialist services and community-based services coexist and often work in unity, although disparity regarding provision is widely recognized (Bercow, 2008; Bercow, 2018). A report by the Lead SLT Group and Chair of the Cleft Clinical Reference Group (2016) found inequity in care due to local and regional variations in how speech and language therapy interventions for children with CP ± L are funded and delivered, following a survey of specialist SLTs across the United Kingdom. This group concluded that speech and language therapy provision aligns with costs rather than evidence-based practice or national recommendations. They raised concerns regarding reductions in skills and expertise of cleft specialist SLTs due to downgrading of posts, which the report considered would negatively impact upon the quality of intervention and speech outcomes.
Evidence for Speech and Language Therapy Interventions for Children With CP ± L
A systematic review of speech and language therapy interventions for children with CP ± L found little evidence to support any specific approach (Bessell et al., 2013). Included in their analysis was a consideration of the different types of speech impairment for which children might need intervention. They summarized that cleft speech difficulties can include both articulation and phonological disorders. An articulation disorder is defined as an inability to produce specific speech sounds, whereas a phonological disorder is characterized by pattern-based speech substitutions as a result of cognitive–linguistic difficulties (McLeod and Baker, 2017). They suggested that future intervention studies should investigate and compare approaches including speech-related motor techniques (aiming to elicit a sound by practicing the physical movement of the articulators) and linguistic techniques (targeting the child’s understanding and production of their rule-based sound system). The review by Bessell et al. (2013) highlighted the need for further methodologically rigorous studies to inform the intervention evidence base for children with CP ± L.
In addition to speech difficulties, children born with CP ± L often have delayed language development (Pamplona et al., 2015; Lancaster et al., 2020). In their recent meta-analysis, Lancaster et al. (2020) concluded that deficits in both expressive and receptive language functioning are apparent in young children with nonsyndromic CP ± L. However, language interventions for this population have been under-researched compared to speech interventions (Pamplona et al., 2015). Pamplona et al. (2015) suggested this might be because speech disorders related to velopharyngeal incompetence are most prominent when treating these children, hence research has been driven by this clinical priority. Nevertheless, a systematic review of early language intervention for children with CP ± L has been carried out (Meinusch and Romonath, 2011). While the authors concluded that findings were limited due to flaws in the design of the previous research, they acknowledged that inclusion of the mothers in the therapeutic setting appeared to positively influence the language abilities of children with CP ± L, supporting the use of behavior training programs for caregivers.
Speech and Language Therapy Intervention in the Non-Cleft Population
Studies investigating intervention approaches used in speech and language therapy in populations of children with non-cleft-related speech and language needs have highlighted some of the challenges that arise in carrying out such research (Roulstone et al., 2012). These include variation in how interventions are described and labeled, a mismatch between the evidence base and clinical practice and an awareness that interventions are complex and typically consist of multiple elements.
It was hypothesized that this variability may impact upon the delivery of intervention, as SLTs may alter specific named approaches from the way they were originally conceived and delivered in trials or exploratory investigations. This may not be a conscious action but nevertheless, the lack of consensus between SLTs in how interventions are labeled and described may pose challenges when comparing approaches. Similar issues were observed in studies of intervention for children with speech sound disorder (Baker et al., 2018) and with primary speech and language impairment (Roulstone et al., 2015).
Another challenge facing investigators is the presence of a lag between the publication of research and its implementation in practice (Olswang and Prelock, 2015; Hegarty et al., 2018). Hegarty et al. (2018) in their survey of practitioners on commonly used intervention approaches for children with phonological disorder found evidence of a “research-practice gap.” Specifically, they found that frequently used interventions were not those which were identified as the most effective according to the evidence in the literature. The findings of Hegarty et al. (2018) highlighted the challenge clinicians face when implementing research findings into practice. Olswang and Prelock (2015) discussed these challenges and introduced implementation science principles, which promote the researchers’ awareness of real-world settings, community engagement, and consideration of behavior change theories. Conducting research which is driven by clinicians’ priorities, a bottom-up approach, may positively influence the implementation of findings into everyday practice.
The complexity of speech and language therapy interventions has been highlighted as a challenge in both research and clinical practice. Further analysis of specific intervention approaches has proposed that some techniques encompass multiple elements (Baker et al., 2018). Baker et al. (2018) advocated establishing which elements drive positive treatment effects and considered the complexities of individual intervention approaches. The authors highlighted the importance of collecting detailed information related to how intervention approaches are delivered when conducting research.
Delivery of Interventions
While determining the critical components of an intervention approach is important, variation in how individual SLTs deliver interventions must also be considered, given the potential for additional impact on outcomes. Roulstone et al. (2015) in the “Child Talk” Study, a large-scale qualitative study of children with primary speech and language impairment, investigated how interventions are delivered in terms of the organization of services and individual SLTs’ decision-making in the management of the children’s needs. Child Talk found that SLTs individualize therapy, often using the phrase “it depends” to illustrate how intervention management is influenced by various factors (Roulstone et al., 2015; Morgan et al., 2019). Some of these factors have been discussed in the paper by Furlong et al. (2018, pp1135); namely, “child factors (eg, age, severity of communication disorder), family factors (eg, cultural differences, engagement and attendance), and contextual factors (eg, staffing pressures, access to published programs).” “Environmental factors” were also discussed in the study by Cronin et al. (2020) which reported on interviews with specialist SLTs who work with toddlers with CP ± L.
Comparisons of service delivery options have been addressed in the studies described above (Roulstone et al., 2015; Furlong et al., 2018; Morgan et al., 2019). The study of intervention intensity by Sugden et al. (2018) for the population of children with non-cleft-related speech sound disorder considered service delivery options. They concluded that detailed reporting of intervention intensity is required in future research to determine the optimal levels for effective treatment. Factors such as the frequency, dosage, location, duration, and person delivering the intervention are all recognized to be crucial when investigating how intervention is delivered (Roulstone et al., 2012; 2015; Hegarty et al, 2018; Sugden et al., 2018).
Consideration of the content of interventions and the manner of delivery are equally relevant in the management of children with CP ± L. To date, it has been mainly gathered through the audit process described above. What has proved more challenging, however, is how to gather robust data on the type of interventions, dosage, and manner of delivery that could be used alongside outcome data to measure the impact of speech and language therapy intervention.
The aim of the present study was to understand expert opinions from clinicians, a key component of the evidence-based practice triangle (Sackett et al., 1996), in order to complement the existing evidence base.
Method
Ethics
Ethical approval for this study was provided by Central Bristol NHS ethics committee (IRAS Number: 135015).
Design and Setting
An iterative qualitative method (Berkowitz, 1997; Srivastava and Hopwood, 2009) was used to obtain information about the types of interventions and patterns of service delivery offered by speech and language therapy services for children born with CP ± L and to capture variations in service provision. The role of iteration, not as a repetitive mechanical task but as a deeply reflexive process, is key to sparking insight and developing meaning. Reflexive iteration is at the heart of visiting and revisiting the data and connecting them with emerging insights, progressively leading to a refined focus of data collection and understanding.
Nine focus groups with speech and language therapy professionals were carried out in England and Wales. This approach, described by Robson (2002a), was selected following discussion with the cleft speech and language therapy teams as the best way to gather detailed information on the range and type of interventions being offered currently. Focus groups were scheduled at their regional cleft center site.
Participants
Sixty-two professionals participated in the focus groups: 43 cleft center specialist SLTs, 16 SLTs from community speech and language therapy services (8 with a specialism in cleft), 3 speech and language therapy assistants, and 1 student SLT (Table 1). No participants dropped out of the study. All cleft teams involved in recruiting to the Cleft Collective Study,1 a large prospective clinical cohort study of children born with CP ± L, were invited to participate in the focus groups but not all were able to do so within the time available for data collection. During the focus groups, only researchers and participants were present.
Participants.a
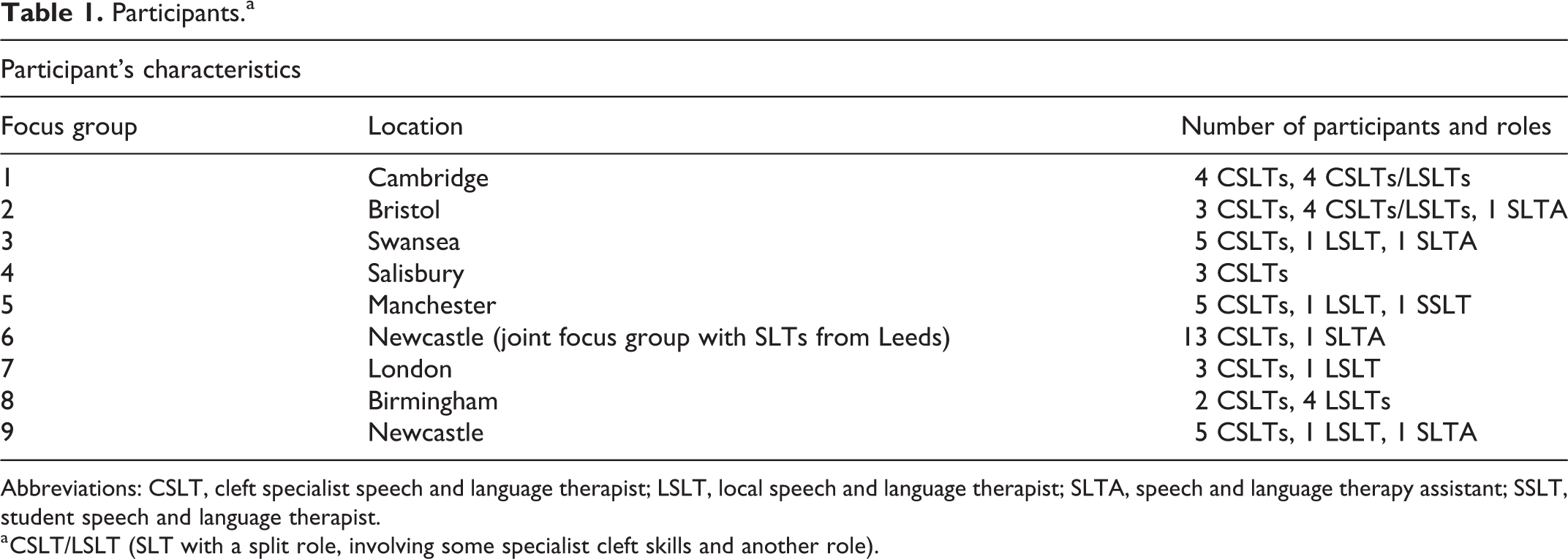
Abbreviations: CSLT, cleft specialist speech and language therapist; LSLT, local speech and language therapist; SLTA, speech and language therapy assistant; SSLT, student speech and language therapist.
a CSLT/LSLT (SLT with a split role, involving some specialist cleft skills and another role).
Procedure
Convenience sampling (Robson, 2002b) was used whereby invitations to participate in focus groups were emailed to the Lead SLTs of the regional Cleft Lip and Palate Services across the United Kingdom. A presentation about the study with eligible SLTs of a Cleft Speech Clinical Excellence Network meeting also drove recruitment. A team of 5 female researchers were involved in data collection, with research and clinical experience in the fields of speech and language therapy and psychology. Three of the researchers had PhDs and 1 worked part-time clinically as a cleft specialist SLT. All of the authors were involved in leading 1 or more focus groups.
Two researchers attended each focus group; 1 researcher acted as facilitator, while the other supported facilitation and recorded field notes. The research was undertaken from an ethnographic stance (Ten Have, 2004; Reed-Danahay, 2009), with the aim to obtain scientific descriptions of SLTs’ service cultures and practice when working with the parents of and children with CP ± L. Professional working relationships were already established between some researchers and participants prior to the focus groups, as a result of previous involvement in research projects and clinical liaison. The researchers’ clinical and research roles were shared with participants prior to the commencement of the focus groups.
Each focus group lasted 2 hours. Detailed notes were taken during each group, as were audio recordings using Olympus DS-2400 dictaphones. Technical difficulties meant audio recordings were not captured during 3 of the groups and as a consequence, quotes are not available from those sites. The focus groups took place over a 15-month period to allow a realistic timescale for clinicians to be freed from clinical commitments for attendance.
Researchers developed a topic guide to encourage dialogue related to intervention provision (Supplemental Appendix 1). Participants were asked: “which are the important aspects of service delivery in speech and language therapy intervention for children with CP ± L?” Once identified, the researcher probed further: “which are the options available for these service delivery choices?” Intervention provision variations were considered from both the specialist and community services. Following a semi-structured format, questions were open-ended, allowing participants to draw on their experiences.
Researchers initiated discussions about how intervention provision varies according to age, between birth and 5 years. The participants defined age categories and subsequently discussed how intervention provision varies for each age category in turn.
Throughout the session, the researchers probed for additional detail and clarification for example, “could you describe it?” “what do you mean by…?” If required, the researchers suggested examples of intervention options raised in previous focus groups to stimulate discussions. The researchers checked their understanding of responses from participants by repeating comments back to participants using alternative vocabulary.
Once no new data were provided, the focus groups incorporated knowledge elicitation activities (Shadbolt and Smart, 2015) to enable participants to reflect in detail on their clinical practice and to make explicit the knowledge that they access in certain clinical contexts. Clinicians have specialist expertise and knowledge, which become second nature to them in daily practice and their rationale for decision-making can be difficult to articulate to nonspecialist listeners. During knowledge, elicitation activities responses to stimulus questions were probed to ensure that clear and unambiguous data were collected. Where specific terms or labels were used to describe interventions, participants were asked to explain and elaborate on what they meant by the term to ensure that there was consistency in how interventions were described in the data set. Examples of these activities are shown in Appendix 2.
Analysis
Qualitative analysis using iterative content analysis, as described by Elo and Kyngäs (2008), enabled the researchers to form codes and subcodes. The content analysis uses a descriptive approach in both coding of the data and its interpretation of quantitative counts of the codes (Downe-Wamboldt, 1992; Morgan, 1993, Vaismoradi et al., 2013), supporting the use, interpretation, and integration of the data from the knowledge elicitation activities. This approach provides an advantage over thematic analysis which is a purely qualitative, detailed, and nuanced account of data (Braun and Clarke, 2006).
Transcripts from the audio recordings and field notes were read several times to ensure the researcher (C.W.) was immersed in the depth and breadth of the content. Transcripts were not returned to participants for corrections or comments. Codes and subcodes were discussed with all authors to check consensus of interpretation. NVivosoftware version 10 (QSR International Pty Ltd, 2014) was used to support the data analysis.
Results
Four codes were identified which covered what intervention is currently delivered and how this is accomplished: “intervention approaches,” “service delivery models,” “decision-making and rationale,” and “patient-centered care.” Each code was populated with four subcodes (Table 2).
Codes and Subcodes.
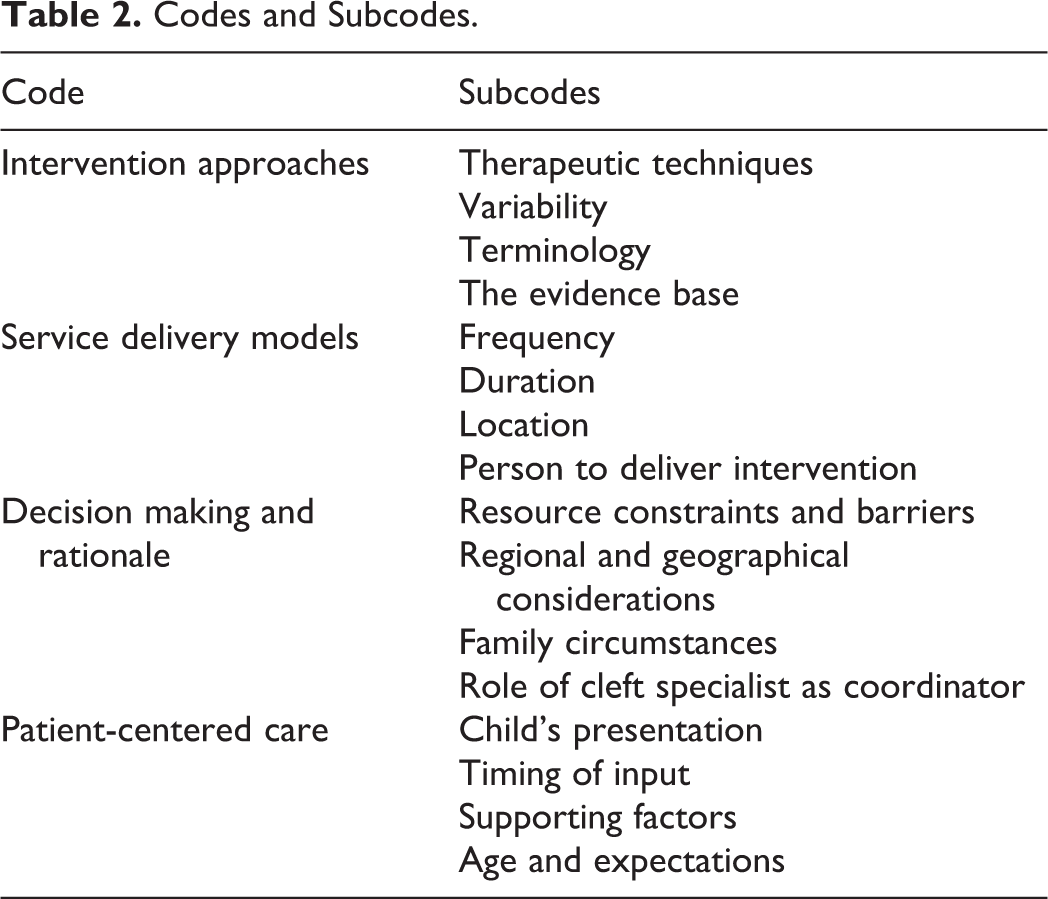
Each of the codes are described in sequence below, together with examples of data which were used to identify the codes. Where relevant and to aid interpretation of the findings, references to the existing literature are included within the results section.
Intervention Approaches
Therapeutic Techniques
Participants discussed which therapeutic techniques they use with children with CP ± L between birth and 5 years. They categorized the type of intervention provided into 2 broad categories: direct intervention and indirect intervention. Direct intervention is delivered by the SLT, whereas indirect intervention is often consultative, guided by the SLT but delivered by another person, such as school staff or a speech and language therapy assistant. We always do indirect therapy whatever we do. (FG 2)
Intervention Approaches.a,b,c
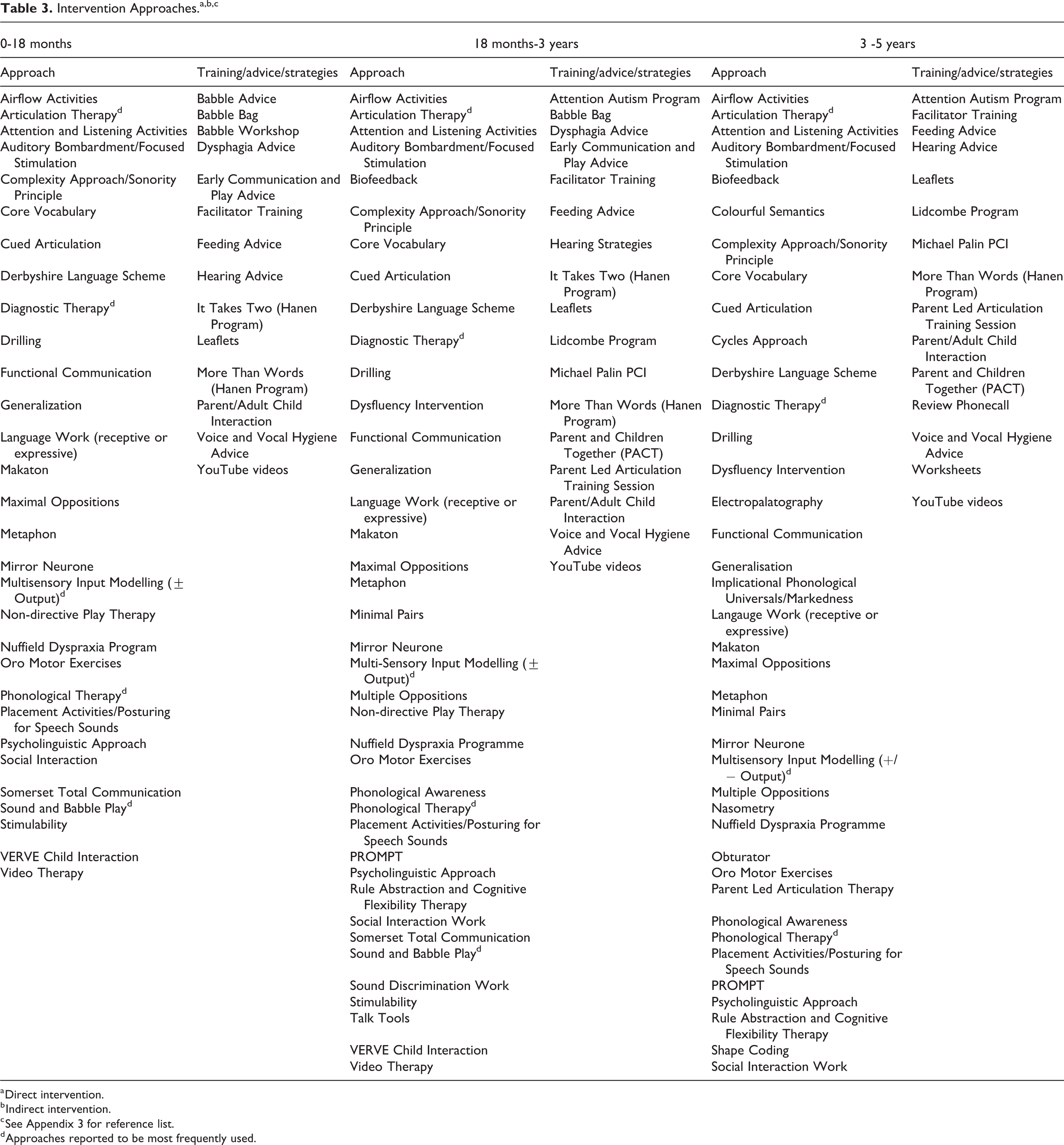
a Direct intervention.
b Indirect intervention.
c See Appendix 3 for reference list.
d Approaches reported to be most frequently used.
The practice of many SLTs was characterized by an eclectic approach, which incorporates aspects of a few different intervention approaches rather than rigidly following one approach as it has been originally described. These findings are comparable to the non-cleft population (Baker et al., 2018; Hegarty et al., 2018) and suggests most SLTs use an eclectic approach to intervention. That eclectic approach, we all do it. (FG 4) We don’t tend to use a set, specific programme. (FG 6)
This eclectic approach recognizes that children with CP ± L can experience various speech and language difficulties and participants are motivated to deliver patient-centered care.
Variability
Participants were aware of similarities and differences in the range of interventions provided by their service, making comparisons between community speech and language therapy services and regional cleft centers. That’s not dissimilar to other teams. (FG 7) Every therapist will be different from another therapist and then every child will have a different need and require different tools on the whole. (FG 4)
Terminology
As participants discussed how interventions varied, they were mindful of their use of terminology and how SLTs may describe the same techniques or processes but use different labels. These terminology variations were observed between and within focus groups, suggesting that SLTs within teams may vary in their use of terminology as well as those across teams. I’m just concerned that one person’s indirect is another person’s direct. (FG 2)
The Evidence Base
When discussing intervention approaches, participants did not routinely mention the evidence base. Some comments suggested SLTs feel that replicating methods from intervention research papers does not always work in their clinical practice. Nobody follows one approach, no, ever ever, not unless you are doing a research project. (FG 5) Where is the evidence base that says putting them on review for 3-6 months allows them to consolidate. (FG 1)
Service Delivery Models
Frequency
Frequency denotes how often speech and language therapy intervention is provided. Kaipa and Peterson (2016) used the term “dose frequency” similarly, to describe the number of times intervention sessions are delivered per unit of time, for example, twice a week or twice a month. Participants mostly interpreted frequency in relation to direct intervention rather than indirect intervention. Variation was reported between services (Figure 1), for reasons such as the child’s needs and availability of resources. They have therapy for as long as they need it because they might be alternating between us and the community. (FG 3 – regional cleft team) As they become more engaged and more able you might increase the frequency. (FG 2)
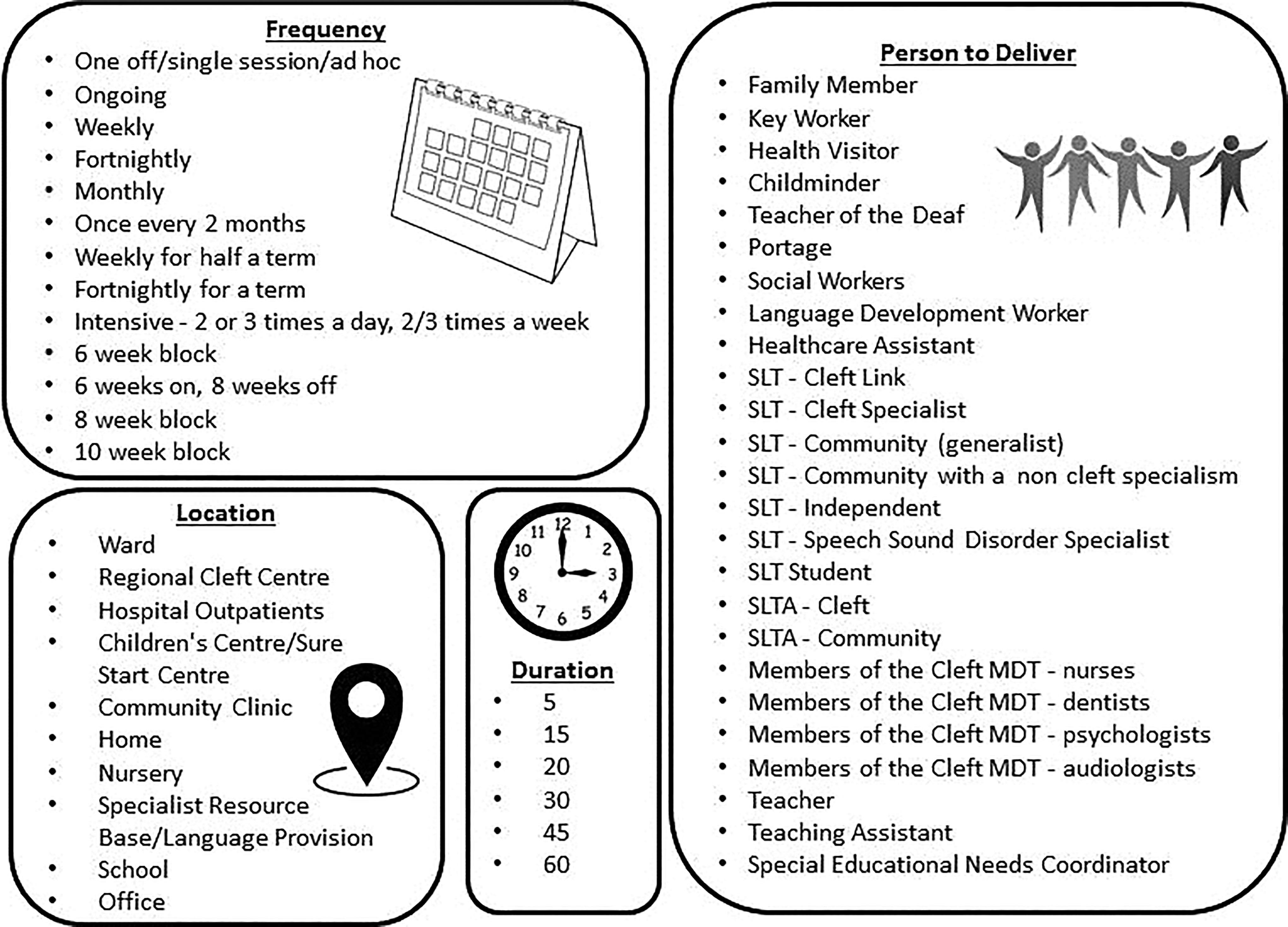
Service delivery models.
Duration
Duration refers to the length of time an intervention session lasts, defined by Kaipa et al. (2016, p508) as “the total time period during which the intervention is provided.” Depending on the intervention targets, the session length varied; however, the average duration for an individual therapy session was agreed to be between 30 and 45 minutes (Figure 1). Participants described adapting the duration of sessions depending on the individual child and commented that they worked flexibly. Even with the really compliant children, when you try and go over the half hour, you notice that the accuracy of their productions just tail off. (FG 3) When you are working with them and getting used to the session you might do longer and longer with them. (FG 5)
Location
The location in which intervention was provided is widely variable (Figure 1). It was reported that numerous aspects influenced this, such as service protocols and the presenting needs of the child and family. There are some really interesting things that you miss if you don’t get the opportunity to do a home visit. (FG 1) Everything is done in centre, we don’t do outreach at all. (FG 7)
Person to Deliver Intervention
Participants listed a variety of people who would deliver intervention to children with CP ± L (Figure 1), although they did not define whether each person was perceived to be a direct or indirect contact. The SLTs reported that the person with a duty of care for a child decides who will deliver the intervention, based on service protocols, intervention targets, and factors such as the geographical location, support networks, and whether the child attends an educational setting.
The importance of involving communication partners such as parents/carers and school or nursery staff in intervention delivery was discussed, raising questions regarding whose responsibility it was to consistently deliver intervention for a child with CP ± L. You get the parents and be like oh can you have a go now and that’s what I want you to do at home, give them things for homework. (FG 2)
Decision-Making and Rationale
Resource Constraints and Barriers
A shortage of resources, finances, staffing, equipment, and overstretched services were issues that were repeatedly raised in all focus groups. These shortfalls were reported to impact negatively on intervention provision. We’ll be doing more than community therapists because they have just got longer wait times. (FG 3) I don’t have the equipment anymore to be able to tape, video and make it into a DVD. (FG 1) It would be capped, you can only see this child once, some areas there is no therapy, that’s what happens. (FG 4)
Regional and Geographical Considerations
The phrase “postcode lottery” is well known in UK health care; participants described how children with CP ± L may be disadvantaged in terms of the frequency of intervention as a result of where they live. Depending on where the children live, there isn’t always a cleft specialist there. (FG 1)
Living further from a regional cleft center was reported to reduce access to intervention in some areas, with SLTs commenting they would be less likely to offer frequent direct intervention if they had to travel a substantial distance to deliver intervention for a child. If some children can’t come to me, I can’t offer weekly therapy because it would be just too much of my time spent travelling. (FG 1)
Family Circumstances
Many participants considered the importance of the wider needs of the child’s family when delivering intervention. I do try and accommodate the parents as much as possible with regards to day and time. (FG 3) Siblings, looking after their children, school drop off, that kind of stuff is often a barrier to coming, chaotic families with lots going on. (FG 1)
Role of the Cleft Specialist SLT
Intervention for children with CP ± L is provided by regional cleft centers, community speech and language therapy services and independent SLTs. Participants explained that when making decisions regarding intervention for this population, it is crucial to liaise and collaborate with other services to ensure that care is cohesive. Our priority is to get them having effective therapy and we get whoever we can, wherever they are to deliver that. (FG 3) Helping set targets and monitor so you are supporting. (FG 2)
Patient-Centered Care
Child’s Presentation
Intervention delivery options and selection of approaches are informed by the child’s progress and their developmental level. Participants highlighted the importance of conducting a thorough assessment prior to the commencement of intervention, in order to ensure appropriate targets are set. Would depend on what they were working on and how they coping with it. (FG 1) The priority when you first meet that cleft child, the cleft like characteristics or is it the attention levels, the language levels and which comes first and when are all kind of key. (FG 1) It’s all about the individual basically. (FG 2)
Timing of Input
An awareness of the child’s cleft care treatment pathway affects how intervention is delivered, ensuring that the timing and type of intervention are appropriate. Speech and language therapist reported timing of surgeries, multidisciplinary care, and the child’s psychological adjustment as factors they include in their decision-making. What’s happening with them in terms of their cleft care as a whole, other interventions, surgeries…how they are coping with the diagnosis and any other health issues. (FG 1) Depending on the child’s motivation, the parent’s commitment, progress in therapy…it’s all those areas we take on board. (FG 3)
Supporting Factors
Participants suggested that speech and language therapy intervention provision is more effective when support and carry over work are completed by other agencies and family members. Participants described their role in ensuring support networks were established for the child when receiving intervention and the challenges that present when a support network breaks down.
Flexibility in service delivery models was reported to be beneficial for intervention provision. Speech and language therapists from specialist services or regional cleft centers described an ability to work with greater flexibility and more resources (time, staffing, and equipment) compared to community services, however, this was not the case for all. That’s the luxury of our service is that we can be very bespoke…not one size fits all. (FG 2) We see them when they are coming in for another appointment to reduce the burden. (FG 4)
Age and Expectations
Although some speech and language therapy services have care pathways for children at specified ages, SLTs mentioned how they create packages of intervention taking into account the child’s developmental stage and cognitive abilities, not just their chronological age. It’s not actually about the age it’s about their developmental stage. (FG 1)
Discussion
This study aimed to investigate what intervention is currently provided by SLTs for children born with CP ± L until the age of 5 and how it is delivered. Nine focus groups were carried out and subsequent iterative content analysis identified 4 main codes with corresponding subcodes.
This study revealed that a wide range of intervention approaches are used by SLTs with this population and that variability exists in service delivery models. The variability described may be explained by the lack of evidence for speech and language interventions, leading to uncertainty for SLTs. Focus group participants were able to share examples of factors which they believed impacted positively on intervention provision, while acknowledging issues and constraints faced. It was clear from the content analysis that, while discrete codes and subcodes could be identified, these were not independent of each other but rather were closely interconnected, as discussed below.
Intervention Approaches and Service Delivery Models
Inconsistencies regarding the use of terminology have been reported in previous studies (Roulstone, 2012; Baker et al., 2018). Inconsistent terminology, in particular, the use of one label for more than one type of intervention or multiple labels for a single intervention, can be problematic in research and clinical practice. Without a full appreciation of the degree of variation in terminology, there is the potential for confusion and a misplaced belief that practice is evidence-based.
Participants reported using direct and indirect intervention with children with CP ± L. Indirect intervention may be offered due to resource shortages, limited availability for direct intervention provision, and to support the consolidation of skills after direct intervention sessions. Indirect intervention was valued equally to direct intervention by most participants in the current study.
Sugden et al. (2018) in their review of the literture regarding intervention for children with phonology-based speech sound disorder, found that in over 80% of 206 studies, intervention was delivered by an SLT. However, the survey of Australian SLTs also reported in showed that a wide range of people, including parents and teachers as well as SLTs, were involved in delivering intervention to this population in clinical practice. Similar results were found in the present work where particiapnts named a range of people delivering intervention alongside the LT. Specifically, school staff and caregivers were reported to deliver intervention for children born with CP±L under the supervision of an SLT.
Participants described a multitude of service delivery options and reported that as clinicians they often work flexibly. This is advantageous when delivering the intervention in a climate with stretched resources, striving to meet the needs of the individual, while balancing service-level restrictions.
In the present study, the authors followed the advice of Baker et al. (2018) who advocated for the use of explorative methodologies when investigating speech and language therapy interventions. Participants listed intervention approaches delivered at specified ages and it is noted that there is a high level of overlap between the age categories, for example, diagnostic therapy and articulation therapy were in common use with all children up to 5 years of age. The notion that intervention is delivered in an eclectic style has been identified in the previous literature (Baker et al., 2018; Hegarty et al., 2018) and participants described how they rarely use one approach in isolation, favoring the use of multiple approaches concurrently to achieve a specific goal.
Meinusch and Romonath’s (2011) systematic review of early language interventions for children with CP ± L concluded that the involvement of caregivers in the therapeutic setting enhanced the child’s language abilities. Other studies (Ha, 2015; Dobbelsteyn et al., 2014) have demonstrated positive intervention treatment effects when parents have delivered intervention in the home setting. Participants in this study provided examples of liaison with caregivers, providing them with advice and therapeutic activities to support the child’s development in the home environment.
Previous research has investigated intervention factors such as the frequency, dosage, location, duration, and the person to deliver intervention, which are recognized to be important when studying how the intervention is delivered (Roulstone et al., 2012; Roulstone et al., 2015; Hegarty et al., 2018). Participants described a multitude of intervention factors that reflect resource availability and consideration of the individual needs of the child and their family.
Decision-Making and Rationale
The current study found that intervention provision was variable between individual SLTs and across services. Roulstone et al. (2015) reported similar findings in “Child Talk” and both studies highlight that participants use the phrase “it depends” when discussing intervention. This illustrates how multifactorial intervention management is and the factors SLTs consider when delivering the intervention. The work by Furlong et al. (2018) supports this by categorizing factors as “child factors,” “family factors,” and “contextual factors.” The present study identified a number of additional factors which need to be considered for children with CP ± L including the timing of surgery, comorbidities such as hearing loss and syndromic status, and location of the intervention provision.
Patient-Centered Care
Factors that were felt to influence decision-making regarding intervention were service-level constraints, the needs of the child and family, and previous clinical experience, comparable to the findings by Furlong et al. (2018). The current study reported geographical challenges as a factor, for participants working in the regional cleft centers, a finding that was not identified in the study by Furlong et al. (2018). Cronin et al. (2020) reported “physical geography/population density” was an important consideration for speech–language pathology practice when working with children with CP ± L.
In the current study, participants from regional cleft centers described their role in the multidisciplinary team and how they incorporate supporting the child and family through their cleft treatment journey into their intervention provision. This was viewed as an additional aspect of intervention provision when compared to local speech and language therapy services and the non-cleft population. This multidisciplinary role demonstrates how intervention is delivered in a holistic manner and contributes to wider public health care, endorsed by Public Health England (Hindle and Charlsworth, 2019).
Limitations
The present study has some limitations which should be acknowledged. This study aimed to investigate intervention provision across the United Kingdom; however, participation from Scottish and Irish sites was not possible within the time available, and findings may not therefore accurately reflect service provision in these geographical locations.
It is recognized that there was less participation representing community speech and language therapy services in this study, therefore findings could be biased toward specialist service intervention provision. A further limitation of this study is that transcripts were not checked by participants for misinterpretations following the focus groups. Additionally, the researchers’ prior clinical experience and existing relationships with participants may have influenced the data, as participants may have experienced acquiescence bias, responding positively in order to please the researchers (Winkler et al., 1982). Due to technical difficulties audio recordings were not obtained from 3 focus groups and consequently quotes were not available from those sites.
Clinical Implications
The aim of this study was to undertake exploratory work to understand interventions currently provided in clinical practice and usual patterns of dosage and delivery for children born with CP ± L up to 5 years of age across the United Kingdom. The findings from this work do not yet assist us in providing evidence to support interventions for children with CP ± L. New knowledge which can be used to inform clinical practice has nevertheless already been generated by this work and has informed the development of a survey of intervention received by participants in the Cleft Collective Cohort Study (Wren et al., 2018). Survey responses will be available for clinicians and academics to combine with other data collected by the study, for example speech outcomes data, to address clinically meaningful questions regarding the impact of SLT intervention. The Cleft Collective Cohort Study is a large prospective clinical cohort study of children born with CP ± L, investigating causes of cleft, the best treatments, and the impact of cleft on those affected and their families (http://www.bristol.ac.uk/cleft-collective/professionals/access/). Survey responses will be available for clinicians and academics to combine with other data collected by the study, for example, speech outcome data, to address clinically meaningful questions regarding the impact of SLT intervention.
We now have a clear picture of the range of interventions being used by SLTs in England and Wales for this population. We know at what ages each is being used and we have an understanding of the factors which affect clinical decision-making and choice of intervention. This repertoire of interventions will aid clinicians who are new to the field in their management and will provide a qualitative benchmark for services to compare themselves to.
This study’s objective to understand expert opinions from clinicians, a key component of the evidence-based practice triangle (Sackett et al., 1996), complements the existing evidence base. Discussion from participants in this study regarding the challenges they face implementing research findings into practice aligns with the previous findings from Hegarty et al. (2018). It is therefore important for future studies to adhere to implementation science principles (Olswang and Prelock, 2015), thus increasing the likelihood of research findings being incorporated into everyday practice. Inconsistencies related to terminology are important to consider in future research studies, to ensure a better understanding of the nature and content of intervention approaches used in speech and language therapy practice.
Conclusion
The present study has identified a large number of speech and language therapy interventions which are being delivered to children born with CP ± L across England and Wales. Exploration of service delivery models and the aspects which influence SLTs’ decision-making, with regard to intervention provision have illustrated both similarities and differences nationally. Many of the intervention approaches discussed in this study were not in the review by Bessell et al. (2013), either because they did not fulfill the eligibility criteria suggesting the evidence is low level or because they had not been reported in the literature at the time of the review. Current evidence for the latter remains at a low level, however, limited mostly to a single case or small group studies.
This study recognizes the uncertainty as to which interventions are effective for this population and which methods of delivery are the most appropriate. Determining which interventions and patterns of delivery are most commonly used within this population will help identify which are the most salient interventions to investigate in efficacy studies and in turn have the potential for impact on practice.
Supplemental Material
Supplementary_material - An Exploratory Study of Speech and Language Therapy Intervention for Children Born With Cleft Palate ± Lip
Supplementary_material for An Exploratory Study of Speech and Language Therapy Intervention for Children Born With Cleft Palate ± Lip by Caroline Williams, Sam Harding and Yvonne Wren in The Cleft Palate-Craniofacial Journal
Footnotes
Authors’ Note
This manuscript has been presented at the following professional meetings: Craniofacial Society of Great Britain and Ireland Annual Scientific Conference (April 2019, London). The Royal College of Speech and Language Therapy Annual Conference (September 2019, Nottingham). Credits and Appropriate Grant Numbers.
Acknowledgments
Thank you to Lucy Southby and Lydia Morgan for their assistance with the focus groups.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Above and Beyond Foundation [grant number 2018-Spr_03].
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.