
Abstract
Objective:
The study addresses whether the growth of the nasal dorsum is disturbed by cleft treatments, for cleft lip only (CL) and cleft lip with cleft palate (CLP).
Design:
A total of 576 patients with cleft (278 CL, 298 CLP) and 333 individuals without orofacial clefts were retrospectively enrolled. Cleft lip only group was treated with a modified Millard technique combined with Tajima incision for rhinoplasty at 3 to 6 months. The CLP group underwent the same lip repair technique and then underwent a Sommerlad palatoplasty at 9 to 12 months. Lateral cephalometric radiographs of all individuals were taken to evaluate the nasal length and nasal dorsum height. Dunn test was used to analyze the difference (P < .001).
Results:
Compared with control, in CL, nasal bone angle and nasal dorsum angle increase by age similarly (5-18 years, P > .05); the total dorsum is significantly shorter (5-18 years, P < .001), while the upper nasal dorsum length is similar (except in 5-6 years), and the lower nasal dorsum is shorter (5-18 years, P < .001). In CLP, nasal bone angle develops insufficiently as children grow (8-18 years, P < .001); the nasal dorsum angle is notably smaller (5-18 years, P < .001); nasal bone length is not significantly different except 11 to 13 years (P < .05); nasal dorsal length is similar at skeletal maturity (17-18 years, P > .05), although it is shorter during 8 to 16 years (P < .05); the upper nasal dorsum is overdeveloped (14-18 years, P < .05), whereas the lower nasal dorsum is underdeveloped (5-18 years, P < .001).
Conclusion:
Treatments in both CL and CLP could be the important factors in disturbing the growth of cartilaginous portion of the nasal dorsum (including nasal tip) and the nasal dorsum height.
Introduction
Cleft lip (CL) is frequently accompanied by nasal deformities. The congenital anatomic deficiency or aberrancy, potential changes related to growth, the cleft itself, and even scarring from previous procedures are the main factors which lead to a wide variability in secondary cleft nasal deformities and the complexity of surgical techniques over the past few years (Pawar and Wang, 2014). Subsequently, secondary surgery for the cleft nasal deformity undeniably presents a formidable challenge to the plastic surgeon, and the results are not as ideal as expected due to the interaction between multiple complex factors that contribute to nasal and facial growth and the cleft nasal deformity.
Since early nasal repair may cause a detrimental effect on the growth of the nose and the maxilla, many surgeons still remain reluctant to perform primary rhinoplasty at the time of primary unilateral CL repair despite publications in the literature that refute any growth disturbance caused by a simultaneous nasal procedure. Due to its central location, the nose plays a prominent role in facial aesthetics (Krane et al., 2017). How does one distinguish the different factors that contribute to the cleft nasal deformity, including cleft type, intrinsic potential changes, or surgical damage? Nowadays, surgeons mainly define the cleft nasal malformation with regard to the alar base, columella, nostril, nasal tip, nasal floor, and nasal septum, attaching more importance to the dysmorphia of the nasal tip (Henry et al., 2014; Sykes et al., 2016). However, because of the complexity of this anatomic structure, it is so difficult to define the key factors, which could lead to the contradictory conclusions. As an important part of nose, the nasal dorsum plays a major role in nasal and facial harmony (Pereira et al., 2017). Analysis of rhinoplasty results has shown that even slight differences in nasal shape can transform the look of an individual’s face (Aston and Guy, 1977), the key point being that one might be able to distinguish the effect of the different factors on nasal dorsum deformity because of its simpler anatomic structure.
Based on the above reasons, this study focused on evaluating morphologic characteristics of the nasal dorsum, on addressing the question of whether the growth of the nasal dorsum is disturbed by cleft treatments in CL patients with and without CP. Any differences in growth might help characterize nasal dorsum development and provide a better understanding of the characteristics of the secondary nasal deformity in patients with clefts following different treatments.
Methods
The study population included healthy individuals, patients with CL only, and patients with cleft lip and cleft palate (CLP), who underwent different treatments, respectively. The soft and hard tissue of the nasal dorsum was analyzed through lateral cephalometric radiographs to obtain objective data of the hard and soft tissue morphology of the three groups of different ages, then compared. Lateral cephalometric radiographs of all individuals were taken to evaluate the nasal length, including the length of the nasal bone, the nasal dorsum, upper nasal dorsum, and lower nasal dorsum. The angulation of the nasal bone and the nasal dorsum were evaluated as the indices of nasal dorsum height.
Sample
The study sample comprised a total of 909 Chinese children aged between 5 and 18 years at the our cleft center between 2011 and 2016, who were divided into a control group, CL only, and CLP since the 2 cleft groups were treated differently. The CL group was composed of 278 children with CL, and the CLP group was comprised of 298 children with combined cleft lip and palate. They were non-syndromic and had no other congenital anomalies. Following our cleft center protocol, the CL group was treated with a modified Millard technique combined with Tajima incision for rhinoplasty at 3 to 6 months (He et al., 2009). The CLP group underwent the same lip repair technique and then underwent a Sommerlad palatoplasty at 9 to 12 months. None received any other secondary surgery such as lip revision, fistula repair, rhinoplasty, or orthopedic treatment except for bone grafting at 9 to 12 years of age. The control group was composed of 333 healthy children without cleft or any other congenital anomalies of the same age range as the CL and CLP groups randomly chosen from Department of Orthodontics in our medical center. These children underwent simple orthodontic treatment and clinically appeared to have normal skeletal relationships, symmetric faces, and no history of craniofacial surgery. All groups were divided by age from 5 to 7 years, 8 to 10 years, 11 to 13 years, 14 to 16 years, and 17 to 18 years (supplementary data).
Cephalometric Analysis
Lateral cephalometric radiographs were taken for each subject under standardized conditions with the head oriented along the Frankfort horizontal plane (FH) parallel to the floor. Subjects were asked to relax their lips in a resting position and to place their teeth in centric occlusion. An EASYMTIC 3298-125 Cephalometry X-ray machine (Chemetron Co) was used for all subjects. In order to reduce the influence of maxillary hypoplasia, a reliable craniofacial reference plane “Sella–Nasion (S-N)” was selected, and maxillary and nasal parts were separated by a vertical line through point nasion. Three hard and 3 soft tissue landmarks were digitized by one observer. Anthropometric landmarks on the nose were defined (Bookstein, 1991; Hasanzadeh et al., 2014). Nasal Dorsum was measured by its length and angular of the hard and soft tissue. Figure 1 shows the landmarks that were used in the cephalometric analysis directly and indirectly, including 4 linear measurements and 2 angular measurements. The angulation of the nasal bone and the nasal dorsum were evaluated as the indexes of nasal dorsum height. The parameter measurements are shown in Figure 2. Each parameter was measured 3 times repeatedly and the median, P25 (first quartile), and P75 (third quartile) were recorded.
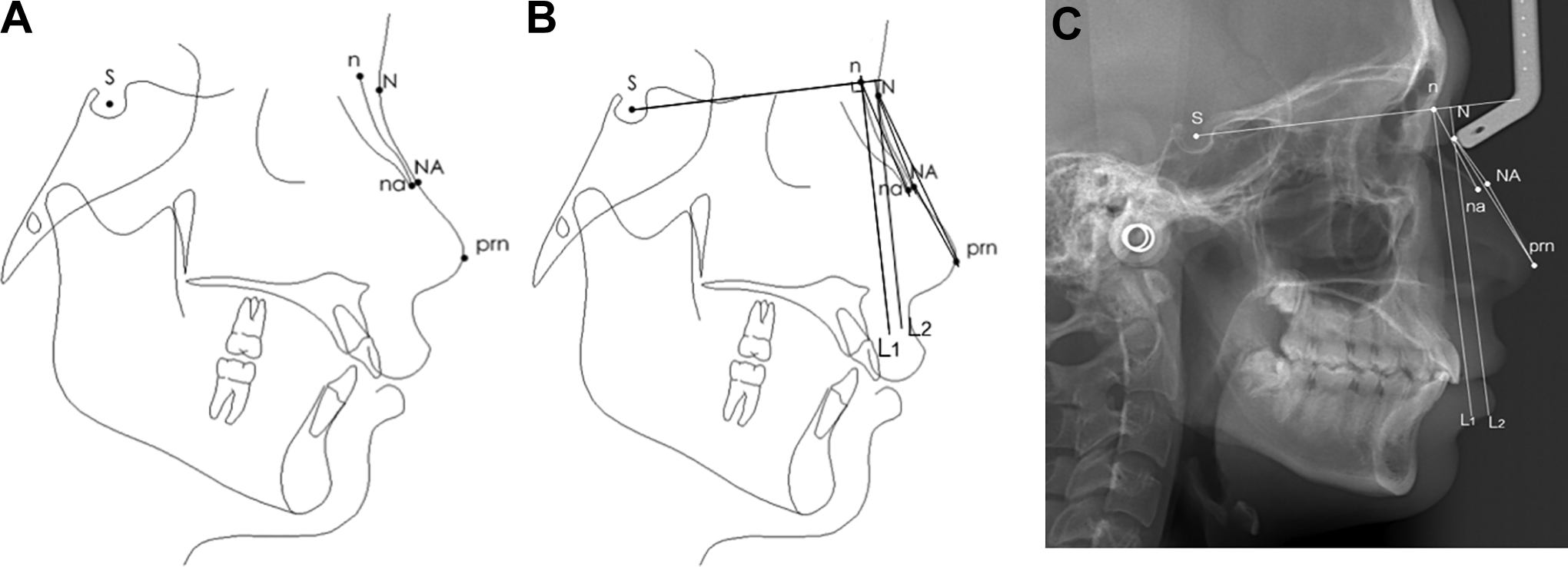
The profile cephalometric radiographs and the cephalometric radiographs. A, Reference points on the profile cephalometric radiographs. S = sella, the center of sella turcica; n = nasion, junction of frontal, maxillary, and nasal bones; N = soft nasion, closest point on soft tissue outline from hard tissue nasion; na = nasale, point at the most anterior inferior part of the nasal bone; NA = soft nasale, closest point on soft tissue outline from hard tissue nasale; Prn = pronasale, most anterior point on the contour of nose. B, Measurements of angles and lines on the profile cephalometric radiographs. L1 = vertical line of S to n, n is the foot point; L2 = parallel to L1; na-n-L1 (degrees): angulation of nasal bone; the angle between na-n-L1; prn-N-L2(degrees): angulation of nasal dorsum; the angle between prn-N-L2; n-na (mm): length of nasal bone, from the nasion to nasale; N-prn (mm): length of nasal dorsum, from soft-tissue nasion to pronasale; N-NA (mm): upper nasal dorsum; NA-prn (mm): lower nasal dorsum. C, Measurements of angles and lines on the lateral cephalometric radiograph.
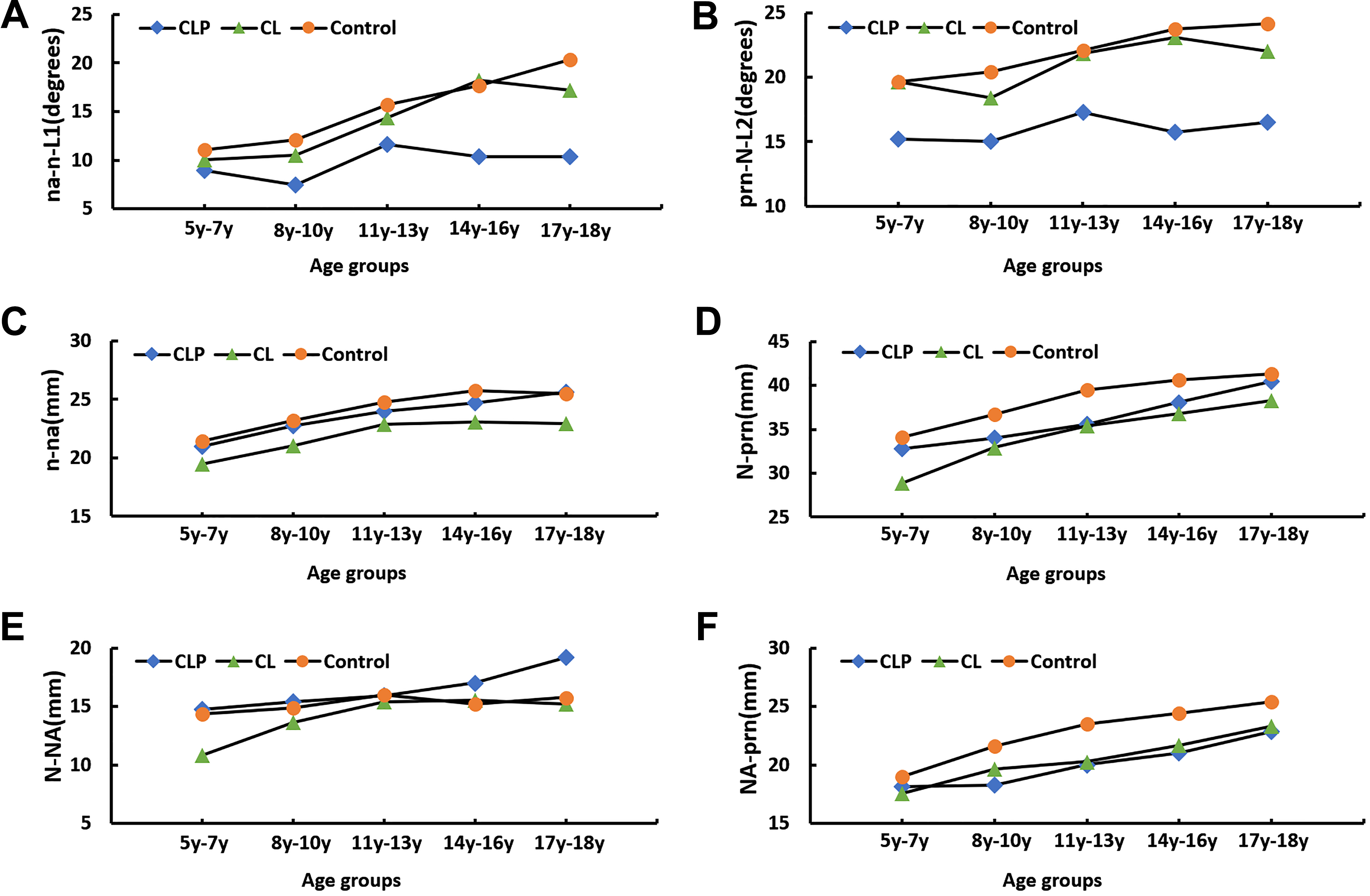
A, Angulation of the nasal bone changes with age in different groups; (b) angulation of the nasal dorsum changes with age in different groups; (C) length of the nasal bone changes with age in different groups; (D) length of the nasal dorsum changes with age in different groups; (E) length of the upper nasal dorsum changes with age different groups; (F) length of the lower nasal dorsum changes with age in different groups.
Statistical Analysis
All statistical analyses were performed with Statistical Package for Social Sciences (SPSS) software version 22.0. Analysis of variance was used to determine the differences of age distribution in the 3 groups. Differences in the cephalometric results among the 3 groups were based on Dunn test. The significant difference was defined at 95% level.
Reliability
To calculate the method error, 100 cephalograms were selected randomly and measured twice to examine the intra-class correlation coefficient (ICC; Hopkins, 2000). The ICC results for test–retest reliability ranged between 0.90 and 0.98, suggesting dependable reliability and reproducibility of the adopted measuring strategy (Table 1).
Reliability Analysis.a
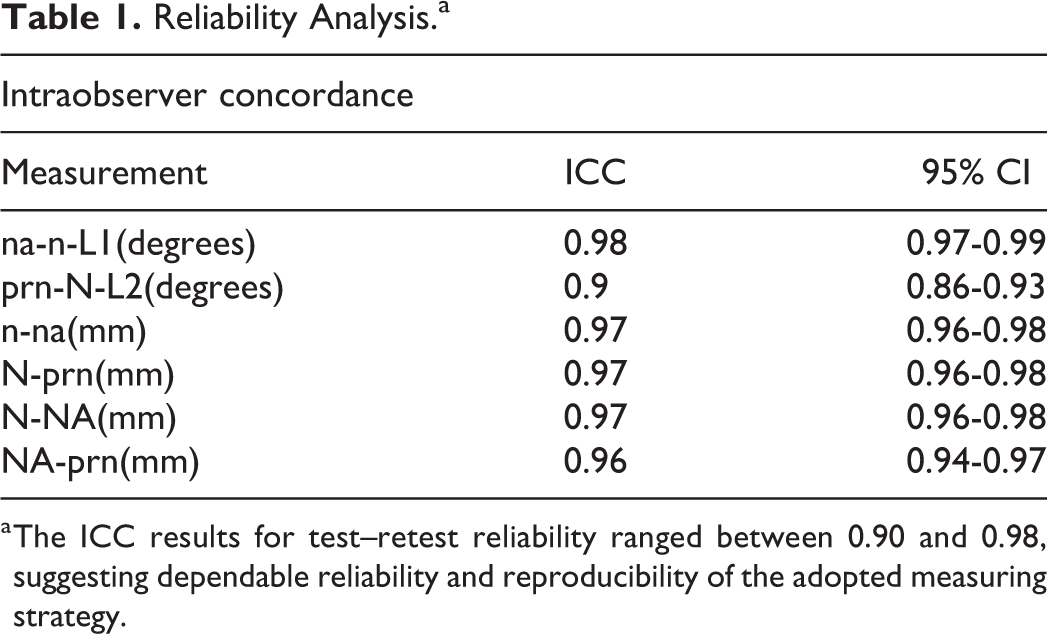
a The ICC results for test–retest reliability ranged between 0.90 and 0.98, suggesting dependable reliability and reproducibility of the adopted measuring strategy.
Results
There was no significant difference in the age composition of CL, CLP, and control groups. Nasal morphology in three groups was comparable (Table 2). However, our results suggest that the growth of the cartilaginous part of the nasal dorsum (including the nasal tip) was disturbed by prior CL and CLP surgery. Even more striking is the decreased nasal dorsum height (decreased nasal angle) in these patients. Figure 2 shows the growth tendency of each index in the CL, CLP, and control group. Figure 3 is the nasal profile map of 3 groups in 17 to 18 years.

The characteristic features of the nose for CL, CL/P, and control groups in 17 to 18 years are shown in profile view. CL indicates cleft lip; CL/P, cleft lip or palate.
Statistical Descriptions of the Angle of Nasal Bone, the Angle of Nasal Dorsum, the Length of Nasal Bone, the Length of Nasal Dorsum, the Length of Upper Nasal Dorsum, and the Length of Lower Nasal Dorsum by Ages and Results of Dunn Test Between CLP, CL, and Control, Separately.
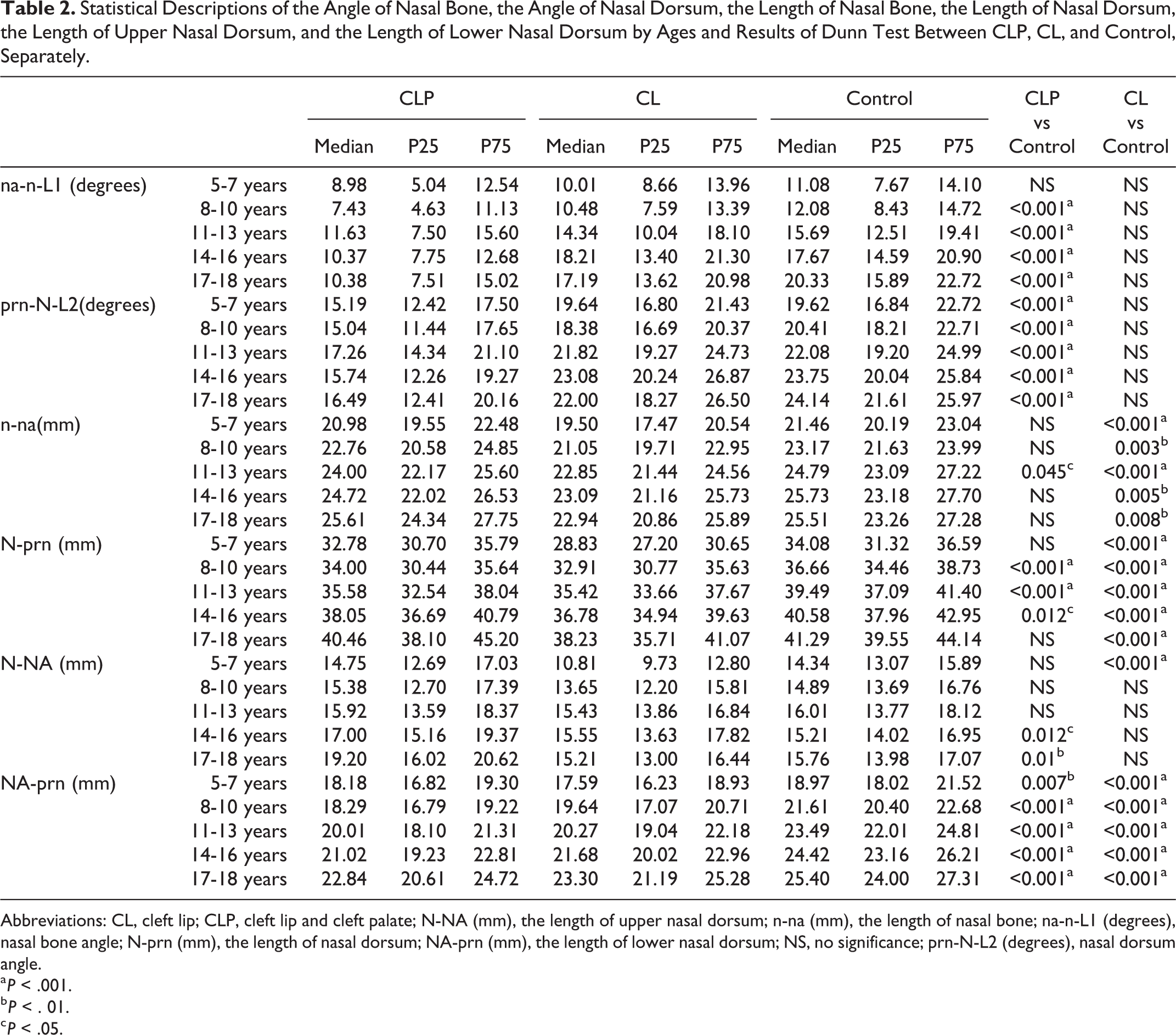
Abbreviations: CL, cleft lip; CLP, cleft lip and cleft palate; N-NA (mm), the length of upper nasal dorsum; n-na (mm), the length of nasal bone; na-n-L1 (degrees), nasal bone angle; N-prn (mm), the length of nasal dorsum; NA-prn (mm), the length of lower nasal dorsum; NS, no significance; prn-N-L2 (degrees), nasal dorsum angle.
a P < .001.
b P < . 01.
c P < .05.
Patients With CL Show Shorter Nose and Normal Nasal Angulation
In CL, compared with control, the angulation of the nasal bone and nasal dorsum increases similarly by age (5-18 years, P > .05; Figure 2A and B), while the total dorsum length is significantly shorter (5-18 years, P < .001; Figure 2C and D). In CL, the upper nasal dorsum is similar to control (except in 5-6 years), (Figure 2E), but the lower nasal dorsum is shorter (5-18 years, P < .001; Figure 2F).
Patients With CLP Have Flatter Angulation But Normal-Length Nose
In CLP, there is no significant difference in the angulation of the nasal bone compared with control in the 5 to 7 years age range. However, it develops insufficiently as children grow (8-18 years, P < .001; Figure 2A). The angulation of the nasal dorsum is notably smaller than that in non-cleft children (5-18 years, P < .001; Figure 2B). Nasal bone length is not significantly different from the control peers at all stages except the peers between 11 and 13 years (P < .05; Figure 2C). At skeletal maturity, the nasal dorsum grows as long as the control group (17-18 years, P > .05), although it is shorter before that (8-16 years, P < .05; Figure 2C).
The upper nasal dorsum is overdeveloped (14-18 years, P < .05), while the lower nasal dorsum is underdeveloped (5-18 years, P < .001; Figure 2D and E), the net effect being a total dorsum length similar to controls at skeletal maturity.
Discussion
The optimum timing of cleft treatment will vary depending upon the type and severity of the cleft deformity. Poorly timed interventions may lead to severe complications. Therefore, it is important to distinguish whether or not primary rhinoplasty at the time of primary lip repair has any adverse influence.
In this study, in patients with CL only, we found the nasal bone was significantly shorter (Figure 2C). This is consistent with prior studies that have demonstrated a significantly shorter nasal bone in fetuses, newborns, children, and male adults with isolated CL compared to healthy peers (Bo et al., 2005; Hansen et al., 2005). However, few studies have presented the data from our research, specifically that the nasal dorsum height in CL does not differ from controls (Figure 2A and B). Nasal tip position is one of the important indicators for the measurement of the length of the nasal dorsum. Compared with non-cleft subjects, CL (with or without CP) showed significant upward deviation in the nasal tip, and it appears that patients with CL have a congenital tendency toward a short nose (Miyamoto and Nakajima, 2010; Figure 2D). Cleft rhinoplasty deals predominantly with the cartilaginous portion of the nose, particularly the nasal tip. Analysis on the cartilage part showed significantly shorter in CL (with or without CP), and this raises concerns that nasal growth might be disturbed by the open incision Tajima procedure for rhinoplasty (Figure 2F).
With regard to the patients with CLP, our research showed interested results. The nasal bone length in CLP did not appear to differ significantly compared with controls (Figure 2C); however, if combined with cartilage part together, the length of the nasal dorsum of subjects with CLP showed initial growth retardation from 5 to 12 years, and subsequent catch-up growth from 12y to 18y (Figure 2B). Figure 2C and E suggests that the nasal bone plays the leading role in the catch-up growth. Observation is being be presented at the first time, as it is inconsistent with the published literature which has found that patients with CP ± CL have similar length of the nasal bone length (Bo et al., 2005; Hansen et al., 2005; Goyenc et al., 2008). To further evaluate this finding, additionally, for more details, nasal dorsum height was employed to evaluate the phenomenon examined. In order to reduce the influence of maxillary hypoplasia, we presented a new evaluation method by utilizing Bookstein and Nadia, H’s design (Bookstein, 1991; Hasanzadeh et al., 2014). The results showed nasal dorsum height in CLP to be lower than controls. Particularly in the 12 to 18 years age-group, where nasal dorsum height demonstrated inhibited growth with or without the cartilage part together (Figure 2A and B). The combination of nasal bone catchup growth combined with reduced dorsum height appears to create forward-downward rotation in the nasal part of the nasal tip. A possible explanation is that CP treatment inhibits the maxillary growth, which lead to maxillary growth in a forward-downward rotation direction when permanent occlusion is reached at 12 years (Liu et al., 2011a; Liu et al., 2011b). In CLP, forward and downward displacement of the maxilla will promote growth of the nasofrontal suture, resulting in forward and downward growth of nasal part. So based on our research, our research suggests that the growth of nasal bone was disturbed by CLP treatment. As mentioned above, a primary rhinoplasty performed at the time of lip repair may inhibit the nasal cartilage part growth in patients with CLP (Figure 2F).
The characteristic features of the nose for CL, CLP, and control groups in 17 to 18 years are shown in profile view (Figure 3), providing a basis for a specific approach to secondary rhinoplasty. Most of all, our study indicates that the growth of the cartilaginous portion of the nasal dorsum (including nasal tip) was disturbed by treatment in both CL and CLP. Although the nasal bone showed the catchup growth in CLP, the phenomenon seems likely due to maxillary growth in a forward-downward rotation direction because of the poor permanent occlusion observed in 12 to 18 years induced by CLP treatment.
We acknowledge that one of the limitations of the study is that the control group was assumed to have normal skeletal relationships. Given that they were undergoing orthodontic treatment for malocclusion, they presumably had dentoskeletal abnormalities, but no clinically obvious cleft or other craniofacial abnormalities.
Conclusion
In this study, although our results indicated the growth of the nasal dorsum appears to be disturbed by the CLP surgery apart from the intrinsic factors such as midfacial hypoplasia, we still recommend that surgeons treat patients with clefts following the popular management approach according to currently accepted management protocols. Many cleft surgeons, including ourselves, advocate simultaneous tip rhinoplasty at the time of initial lip repair because of the obvious improvement in the unilateral cleft nasal deformity. Normal appearance and good speech with minimal complications is the goal for all patients with clefts, but we need to be aware of which procedures may cause undesirable long-term effects that will need to be addressed at a later date.
Supplemental Material
supplementary_material - Radiologic Evaluation of the Influence of Cleft Treatment on Nasal Dorsum Growth
supplementary_material for Radiologic Evaluation of the Influence of Cleft Treatment on Nasal Dorsum Growth by Lingling Pu, Renkai Liu, Bing Shi, David W. Low and Chenghao Li in The Cleft Palate-Craniofacial Journal
Footnotes
Author’s Note
Samples were collected in accordance with the guidelines of The West China Hospital of Stomatology Institutional Board (WCSHIRB). The experimental protocol was approved by local ethics committee (WCSHIRB, Sichuan University, China). Informed consent was obtained from all subjects or, if subjects were under 18, from a parent and/or legal guardian.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Research and Develop Program, West China College of Stomatology, Sichuan University (LCYJ2919-12).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.