
Abstract
Rare facial clefts are characterized by facial involvement that is not restricted to the lip, palate, and alveolus as in traditional cleft lip and palate. The craniofacial skeleton and the orbital structures are frequently affected in these conditions. Exposure of the eyeball, when not early treated, puts the function and the preservation of the eye at risk. We report the case of a 2-month-old boy admitted to our service with an extensive oral-ocular cleft and exposure of the eyeball with melting corneal ulcer treated with a conjunctival closure with a purse-string suture.
Introduction
Rare facial clefts are characterized by the involvement of facial structures and frequently associated with the orbital and central nervous system extension (Kawamoto, 1976; Tessier, 1976). Exposure of the eyeball, especially of the cornea, resulting from large bone and soft tissue gaps, often leads these patients to permanent loss of vision and/or the eyeball when not treated early (Pereira et al., 2010). A similar situation to that, found in these clefts, is the condition of exposure due to proptosis in patients with syndromic craniosynostosis in which the prompt indication of protection of the eyeball with tarsorrhaphy prevents the cornea from exposure and possible ulceration. In situations such as the one in which the vision was compromised, the preservation of the ocular globe, despite the loss of function, is of extreme importance because it maintains the orbital structure, preserving or interfering less in face growth and development. We report a case of conjunctival closure with a purse-string suture technique in extensive oral-ocular cleft and exposure of the eyeball with progressive corneal stromal dissolution and imminent perforation, called melting corneal ulcer. The study was approved by the human research ethics committee of the author’s institution, and informed consents were assigned by parents and adhered to the ethical principles in the Declaration of Helsinki.
Case Report
A 2-month-old boy was admitted to our hospital presenting a wide cleft compromising the upper lip, maxilla, and left orbital margin. The unusual association among Tessier number 4, 5, 6 in left side could be described beyond the transverse facial cleft (Tessier no. 7) on the contralateral side as well as partial amputation of extremities and constriction rings (Figure 1). The cornea was exposed in spite of the history of attempted protection of the eye through a tarsorrhaphy in the hospital where the child was born when he was 10 days old, and use of ophthalmic antibiotic ointment and lubricating eye drops. The ophthalmologic evaluation revealed an extensive corneal ulcer with apparent herniation of anterior chamber contents—melting ulcer. In the course of genetic evaluation, the mother’s previous medical history, family history, and prenatal history were raised. Oligohydramnios was identified in the third trimester of gestation. The combination of the signs of facial cleft and constriction rings on the fingers and toes was characterized as Amniotic Band Syndrome. Computed tomography (CT) scans showed extensive left maxillary bone defect, pyriform, and ipsilateral orbital floor agenesis with dystopia of the eyeball.

A, Preoperative of wide cleft compromising the upper lip, maxilla, and left orbital margin, and a transverse facial cleft (Tessier no. 7) on the contralateral side. B, After purse-string conjunctival closure. C, Surgical marking the flaps and incisions to facial cleft correction. D, Immediate postoperative left facial clefts correction. E, Postoperative left facial clefts correction. F, Immediate Tessier number 7 cleft surgical correction. G, H, and I, Three-year follow-up first surgical procedure.
Ocular content including extraocular muscle and intraocular fat was segmented and volume calculated by Mimics software (Materialise, version 17.0). The measurement was performed independently for each orbit according the different labels to right and left orbit. The volume of orbital soft tissue on CT image calculated were very similar for both sides. The right volume orbit was 4.013 mm3, and left volume orbit was 4.069 mm3 (Figure 2).
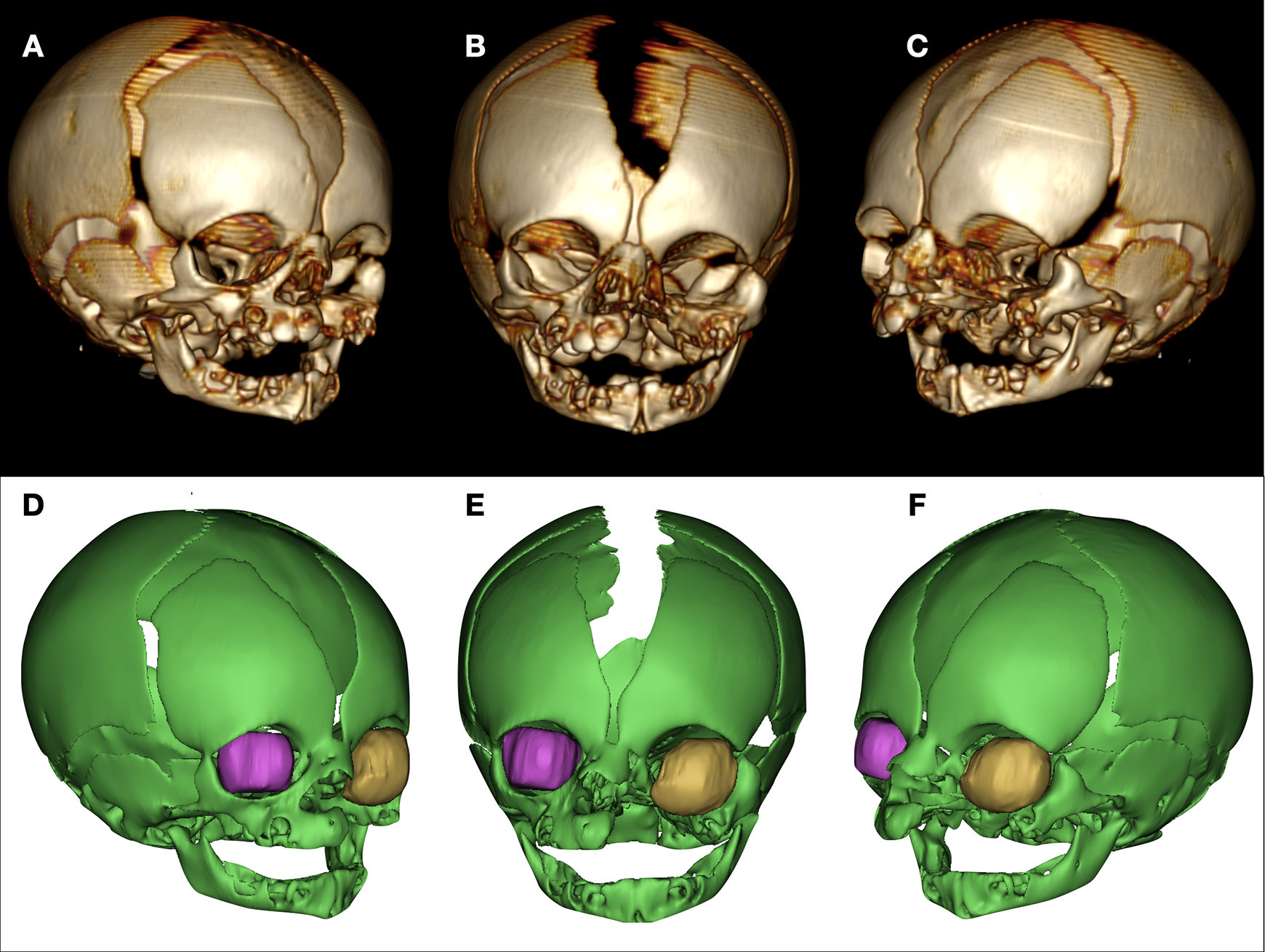
A-C, CT images showed extensive left maxillary bone defect, pyriform, and ipsilateral orbital floor agenesis with dystopia of the eyeball. In D, E, and F, the volume of orbital soft tissue on CT image was calculated for right side: 4.013 mm3 and left volume orbit: 4.069 mm3.
Although the extent of the cleft includes the palate, the child did not present respiratory discomfort. The patient also evolved favorably when an oral diet was introduced, with no indication for enteral catheter feeding. Most likely, the constant crying could be attributed to the corneal exposure. Overall clinical status was good, and no sign suggestive of infectious disease was observed.
Surgical treatment was then carried out to preserve the eyeball. Under general anesthesia, a subconjunctival injection of lidocaine and epinephrine solution (1:100.000) was made. A complete 360-degree peritomy with sharp-tipped Westcott scissors was made following the margins of the ulceration, and then the circumferential detachment of conjunctiva and Tenon’s capsule was performed. A tobacco or tobacco pouch suture was then performed, 1 to 2 mm distant from the peritomy, by passing a silk 4-0 needle thread through all layers of tissue surrounding the ulcer and thereby trailing and obliterating the opening in the cornea. The suture was removed 3 weeks after the surgery (Figures 3 and 4 and Supplemental video).
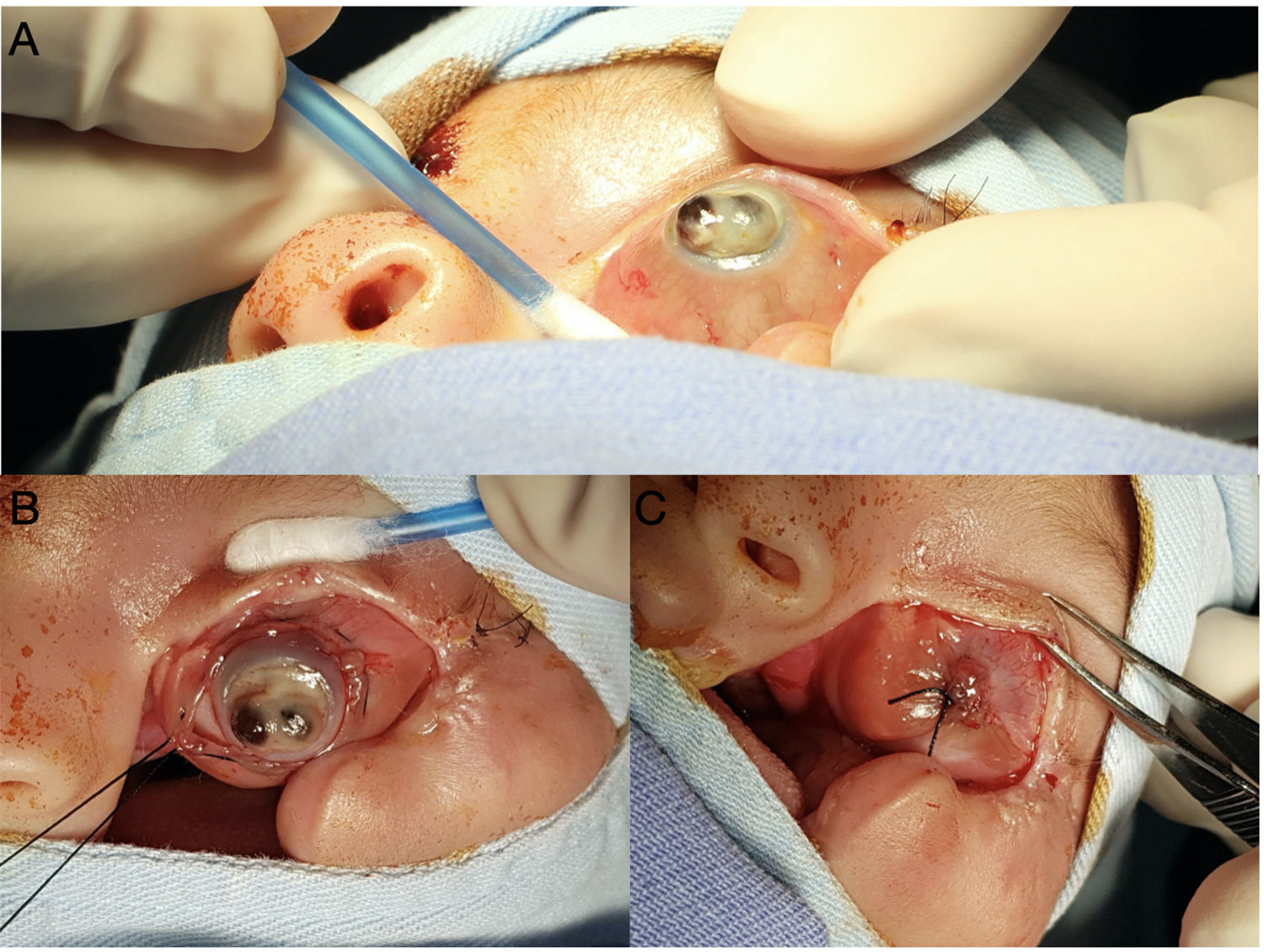
A, Closed view of melting corneal ulcer; (B and C) A tobacco or tobacco pouch suture performed 1-2 mm distant from the peritomy, by passing a silk 4-0 needle thread through all layers of tissue surrounding the ulcer and thereby trailing and obliterating the opening in the cornea.
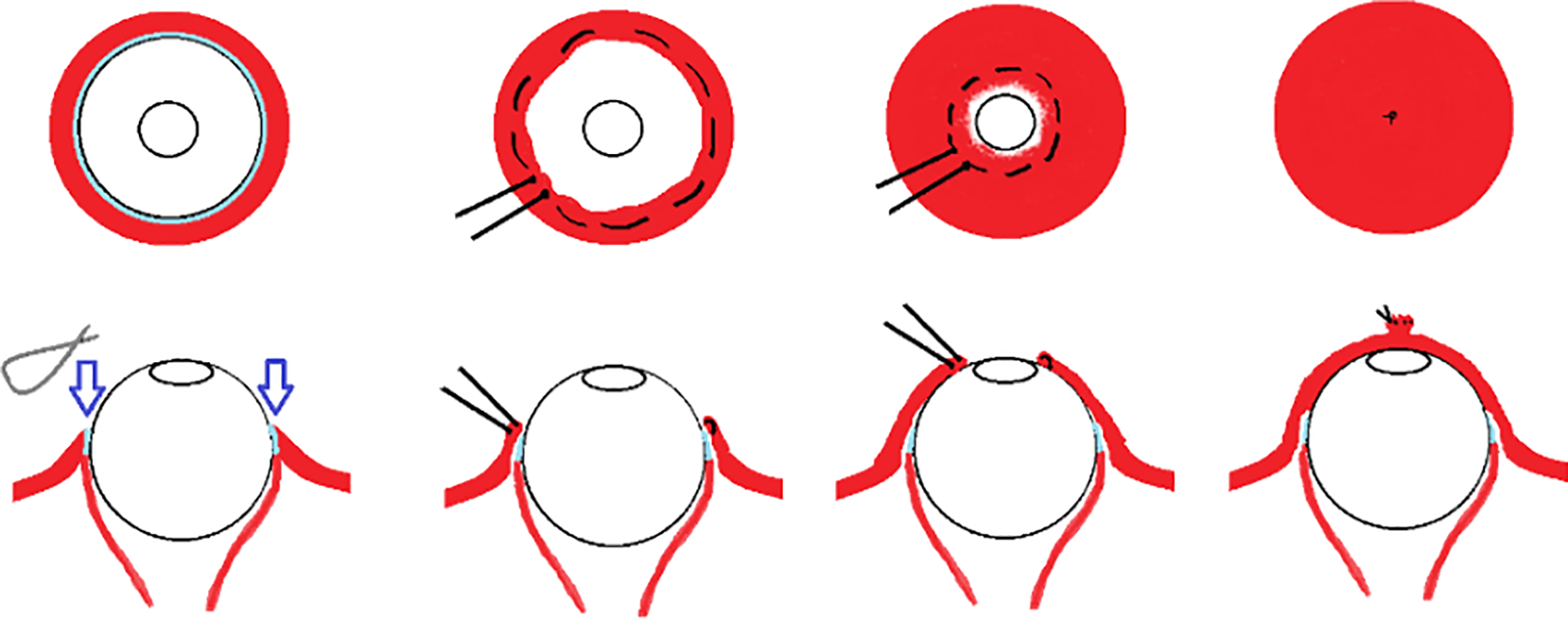
A complete 360-degree peritomy with sharp-tipped Westcott scissors was made following the margins of the ulceration and then the circumferential detachment of conjunctiva and Tenon’s capsule was performed. A tobacco or tobacco pouch suture was then performed, 1-2 mm distant from the peritomy, by passing a silk 4-0 needle thread through all layers of tissue surrounding the ulcer and thereby trailing and obliterating the opening in the cornea.
Ten days after the conjunctival closure procedure, the child underwent to facial clefts surgical correction. Transposition of a myocutaneous flap from the upper eyelid to the medial portion of the orbit was performed. The previous scar area of the tarsorrhaphy was used, which extended laterally to the outer corner of the left eye. Extending soft tissue detachment was performed to medialize the tissues and close the left paranasal region. Identification of the orbicularis muscle was performed, and the closure of the medial and lateral segments of the cleft were closed with the help of an incision in the left nasogenian sulcus. The contralateral macrostomy was corrected at 12 months of age together with the performance of the anterior palate repair and the making of the sac bottom with local flaps. At 3 years of age, the patient returned for posterior palate repair and correction of fistula in the anterior palate. The child is awaiting a new surgical procedure to reconstruct the lower eyelid and adapt the lens. The eyeball shows conjugate movement, and no signal is identified for enucleation indication.
Discussion
Rare facial clefts called Tessier’s clefts number 3 and 4 are characterized by orbital involvement, often associated with dystopia, tear apparatus impairment, and eventually micro- or anophthalmia (Alonso et al., 2008; da Silva Freitas et al., 2010).
The clefts associated with the Amniotic Band Syndrome in turn have a different and often more severe behavior. In fact, amniotic band syndrome consists of a rare congenital anomaly with different clinical manifestations ranging from simple constriction rings to large craniofacial and extremity deformities. Of undetermined etiology, it seems to be a defect in the embryonic matrix that is characterized, in the case of the craniofacial segment, by extensive, complex deformities that compromise multiple structures and do not follow an embryological and developmental pattern (Morovic et al., 2004).
Exposure of the eyeball resulting from large bone and soft tissue gaps observed in rare facial clefts can cause permanent loss of the eyeball. Although in some cases vision is compromised, the preservation of the ocular globe maintains the orbital structure. The orbit grows until approximately 6 years of age and participates in the configuration and development of the face. Enucleation at an early age is extremely harmful to the development of the midface since the absence of the eyeball leads to a progressive loss of the dimensions of the cavity and consequent impact on neighboring structures. In addition, aesthetic rehabilitation through adaptation of lenses is impaired once the eye cavity becomes shallow and with narrower margins (Kish et al., 2011).
The unsuccessful attempt of a tarsorrhaphy and prolonged exposure of the cornea as in the case presented led to complete corneal ulceration and herniation of the structures of the anterior chamber of the eye with visual loss and apparently severe pain. By admitting it and suturing the conjunctiva, the goal was to preserve the eyeball, thereby avoiding further damage to the face growth and better aesthetic rehabilitation in the future. Every time there is corneal damage such as exposure ulcer; we must, as soon as possible, provide mechanic support to heal the wound. The conjunctival graft or flap is a good option. In these cases, it is very important that the conjunctival graft or flap be done preferably in the first 24 hours after birth to protect the eye from excessive exposure. An early intervention is known to increase the chances of preserving the eye, avoiding corneal melting.
The suture in tobacco pouch or smoking bag used in this case is a type of suture consecrated in surgeries of the digestive system, especially gastrostomy, and has as advantages the obliteration of an ulcerated or even open area intentionally, as is the case of gastrostomy (Kantor, 2016). In ophthalmology, the purse-string sutures have been used in the past to treat hyperopic shift following keratotomy (Damiano et al., 1998). It has also been described in penetrating keratoplasty after keratotomy to hold the peripheral incisions closed and stable during penetrating keratoplasty; suturing the keratotomy incisions is known to show incomplete wound healing (McNeill & Wilkins, 1991). The purse-string suture was described by Chawla for managing infectious keratitis with scar dehiscence after radial keratotomy (Chawla et al., 2009). Gundersen et al. (1958) described a 360-degree peritomy like the one performed in our case, but he used a strip 14-mm distant from the peritomy margin to fix over the cornea. As a side effect, this technique can cause ptosis and permanent loss of conjunctiva beyond the retraction of the flap. Conjunctival flaps can be used temporarily and removed after the adequate eyelid reconstruction, and they provide the possibility of a functional eye and normal vision when any other alteration exists. If the eye is viable and a satisfactory palpebral occlusion is achieved, the conjunctiva is opened to ensure visual development and decrease the chance of amblyopia. Therefore, protection of the eyeball through conjunctival flaps for conditions other than rare facial clefts are described in the literature. However, no publication was found by the authors recommending the conjunctival flap as a necessary and urgent procedure in cases of corneal ulcers in rare facial clefts.
The clinical treatment should be initiated by the general doctor with drops, ophthalmic antibiotic ointment, and occlusive dressing because it is very important to these cases that the conjunctival graft or flap be done as soon as possible, preferably in the first 24 hours after birth. Corneal melting is usually painful and visual loss occurs quickly and so early referral to an ophthalmologist is the rule. However, procedures such as tarsorrhaphy mainly and the conjunctival flap as described in this case can be performed by a cleft surgeon with the aim of preserving the eyeball of these patients. The technique described is relatively easy to perform and is within the reach of the cleft surgeon. In other words, a safe approach with great benefit for the child can be achieved even in places with restricted access to specialized professionals.
The procedure of choice at the first moment and ideally soon after birth should be tarsorrhaphy due to the ease of execution and be in the broader domain of the surgeon. In those situations in which tarsorrhaphy is not feasible due to scarcity of tissue and cleft extension, or failure as in the case reported, the conjunctival flap is indicated. The unsuccessful attempt of a tarsorrhaphy or conjunctival covering the prolonged exposure of the cornea can lead to complete corneal ulceration and herniation of the structures of the anterior chamber of the eye. In these cases, when there is no possibility of preserve, the eye evisceration is indicated.
In our case, the detachment of the conjunctiva following the margins of ulceration and the silk-thread suture through all extension of the tissue surrounding the lesion allowed a concentric advancement of the conjunctiva over the ulcerated area and its satisfactory obliteration. The posterior side of facial cleft correction with medial advancement of the soft parts allowed the creation of a bottom of sac and inferior eyelid. Three-year surgical follow-up demonstrates a satisfactory aesthetic result and preserved eyeball. New surgical procedures to repair the inferior eyelid and minimize scars are needed. The long-term follow-up is necessary to evaluate the effects of eyeball preservation in midface growth.
Conclusion
Purse-string suture was an individualized tactic satisfactorily used for protection and maintenance of the eyeball of a complex ocular alteration. The preservation of the orbit structure, even when the function has already been lost, especially in congenital craniofacial anomalies such as atypical facial clefts, has great impact on face growth and development. This technique can be used early, preventing corneal ulceration, and its consequences up until the cleft could be corrected.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.