
Abstract
Objective:
To examine feeding skills of infants with cleft palate with or without cleft lip (CP±L) using infant-driven feeding systems compared to healthy controls on standard bottles.
Design:
Cross-sectional cohort.
Setting:
Large pediatric academic medical center in the Midwestern United States.
Participants:
Infants with CP±L (n = 15) using the Dr. Brown’s Specialty Feeding System and typically developing infants without CP±L (n = 15) using the Dr. Brown’s Natural Flow Original or Options bottles.
Main Outcome Measure(s):
Bottle-feeding proficiency, duration, milk transfer, and signs of feeding difficulty.
Results:
Five-minute feeding proficiency differed significantly between groups with the control group taking 44% of the feed compared to 15% for the CP±L group on level 1 (P < .001) and 21% on level 2 (P < .001) nipples. Proportion of milk transfer was 96% ± 7% for controls and 75% ± 24% for the CP±L group (P = .013). Feeding duration (minutes) differed between the control group (13 ± 3) and the CP±L groups on each nipple level (level 1: 29 ± 16; P = .003; level 2: 32 ± 11; P = .001). Milk transfer rate (mL/min) was 9 ± 3 for control infants compared to 3 ± 1 for infants with CP±L on level 1 (P < .001) and 5 ± 1 on level 2 (P = .007). Coughing occurred in 40% of infants with CP±L and 27% of controls.
Conclusions:
Even when using specialty bottles, infants with CP±L differ from noncleft infants in feeding proficiency, duration, and overall intake.
Introduction
Early feeding success is critical for infants with cleft palate, with or without cleft lip (CP±L), to support normal growth and development and to aid in preparation for surgical intervention. Feeding challenges and poor weight gain are frequent concerns for infants with clefts, particularly for those with cleft palate (Avedian & Ruberg, 1980; Jones, 1988; Marques et al., 2009; Kaye et al., 2017). The presence of a cleft palate does not allow for the creation of negative pressure as the intraoral chamber enlarges during feeding, which impacts the infant’s ability to draw liquids from the breast or standard bottle (Clarren et al., 1987; Mizuno et al., 2002; Reid et al., 2007).
In the past, modifications were made to standard nipples, such enlarging the orifice (Clarren et al., 1987) or poking additional holes (Shaw et al., 1999), to ensure adequate intake for infants with CP±L. More recently, specialized feeding systems have been designed to accommodate for the decreased intraoral suction observed in infants with CP±L. These “cleft-specific” bottles and nipples aid milk extraction and are often the primary tool for feeding management of infants with CP±L. Various feeding systems are available. Some systems rely on the caregiver to compress the bottle or nipple in rhythm with the infant’s sucking pattern to deliver the milk, called “caregiver-assisted” systems (Miller, 2011). Other bottles are infant-driven and include a one-way flow valve that allows the infant to self-pace liquid extraction by independently compressing the nipple. In the absence of comparative effectiveness data, the one chosen should match the infant’s needs and the caregivers’ preference.
Two specialty bottles that are considered caregiver-assisted are the Mead Johnson Cleft Lip/Palate Nurser and Medela SpecialNeeds Feeder. The Mead Johnson Cleft Lip/Palate Nurser includes a long cross-cut nipple and a flexible bottle, which is designed for easy compression by the feeder. The Medela SpecialNeeds Feeder has a Y-Cut silicone nipple that can be squeezed by the feeder to provide fluid to the infant. The bottle also contains a one-way valve to allow extraction by the infant’s own compression efforts. The Pigeon Nipple/Bottle is considered an infant-driven feeding system. A one-way valve is inserted into a nipple that has a firm and soft side. The firm side is positioned toward the roof of the infant’s mouth, while the soft side is placed on the tongue to promote milk flow.
The newest infant-driven bottle available in the United States is the Dr. Brown’s Specialty Feeding System. This bottle has gained popularity with families and craniofacial teams (Madhoun et al., 2020) possibly due to the similarity to the traditional Dr. Brown’s Natural Flow Original and Options bottles. The primary difference between these Dr. Brown’s bottles is the inclusion of an Infant Paced Feeding Valve in the Specialty Feeding System, which allows the infant to independently extract the liquid by compressing the nipple without the need for suction. The nipples used on the Dr. Brown’s bottles range from Ultra-Preemie to Y-Cut and vary by flow rate. Recommendations regarding nipple flow level are provided by Dr. Brown’s and are generally based on the infant’s age, although they suggest that feeding skill should also be considered (Dr. Brown’s, 2018).
While prior studies compared rigid and squeezable bottles (Brine et al., 1994; Shaw et al., 1999), there are no published studies exploring feeding characteristics of infants using infant-driven systems, specifically the Dr. Brown’s Specialty Feeding System. Therefore, it is unknown how this specialized system performs for infants with CP±L in regard to feeding efficiency and safety.
The evaluation of infant feeding skills is challenging due to the subjectivity of assessments, the need for advanced training, and the requirement for specialized equipment (Lau & Smith, 2011). Lau and colleagues developed an objective tool to measure the oral feeding skills of infants born prematurely in the neonatal intensive care unit (NICU) (Lau et al., 1997; Lau & Smith, 2011). By observing the oral feeding performance of the infants in the NICU, the infant’s actual feeding skill and endurance could be determined by examining their feeding proficiency (percentage volume taken during first 5 minutes/total volume prescribed; ≥30% or <30%) and rate of milk transfer (milliliters consumed/minutes of feeding; >1.5 or <1.5 mL/min), respectively (Lau et al., 1997; Lau & Smith, 2011).
The presence of oral feeding difficulties in infants with CP±L has been well described, including inefficient sucking patterns, nasal regurgitation, prolonged feeds, and excessive air intake (Clarren et al., 1987; Jones, 1988; Arvedson & Brodsky, 2002; Masarei et al., 2007). These challenges could result in increased caloric expenditure during feeding. Without adequate intake, infants may struggle to gain weight, potentially resulting in subsequent malnutrition and surgical delays. Whether there is an increased risk of aspiration for infants with nonsydromic CP±L remains unclear, with differing accounts of the presence of coughing and choking and the increased incidence of respiratory infections (Clarren et al., 1987; Shaw et al., 1999; Masarei et al., 2007; de Blacam et al., 2018).
The purpose of this study was to examine the bottle-feeding skills of infants with CP±L using the Dr. Brown’s Specialty Feeding System compared to those of healthy, noncleft infants using standard Dr. Brown’s bottles. It was hypothesized that infants with CP±L would display longer feeding durations with a slower rate and smaller volume of milk consumed. The feeding duration and milk consumption measured during the experimental study session were also compared to home feeding performance, based on parent report.
Methods
Participants
Institutional review board approval was obtained for this prospective study and parents of eligible infants provided written informed consent. Fifteen infants with unrepaired cleft palate with or without lip (CP±L group) and 15 healthy infants without clefts (control group) were enrolled in the study. Infants in both groups were 1 to 12 weeks of age at the time of study visit, born full term (at least 37 weeks gestation), were in generally good health, and had to be using a Dr. Brown’s bottle and the Dr. Brown’s level 1 or level 2 nipple. The level 1 nipple is often used initially for young bottle-feeding infants (0 months+), while the level 2 is typically used secondarily if a faster flow is required as the infant ages (3 months+).
Infants in the CP±L group were recruited from the institution’s Cleft Lip and Palate Center and had to be using the Dr. Brown’s Specialty Feeding System. Exclusion criteria for the CP±L group included complex multianomaly syndromes (with the exception of Stickler syndrome), Pierre Robin sequence, or infants with tracheostomy tubes. Control infants were recruited from the surrounding community. Control infants had to be using the Dr. Brown’s Natural Flow Original or Options bottles. These bottles are functionally the same and include an anti-colic internal vent system, but the Options bottles allow the removal of this internal vent system as the infant matures. Infants had to be using a bottle for at least 25% of feeds, if breastfeeding as well. Exclusion criteria for the control group included the presence of an orofacial cleft, genetic disorder or syndrome, a significant feeding or swallowing disorder, or a chronic medical condition associated with a feeding or swallowing disorder. Children using non-oral feeding methods (eg, gastrostomy or nasogastric tubes) were not eligible for participation in the study in either group.
Infants with CP±L were 65 + 16.49 days of age and controls were 70 + 15.09 days at the study visit, with 4 (33%) females in each group. No statistically significant differences were noted between the groups in regard to infant age or sex. The CP±L group included 3 infants with cleft palate only and 12 with cleft lip and palate. Of the infants with cleft lip and palate, 7 had a unilateral cleft lip and palate (4 left, 3 right) and 5 infants had a bilateral cleft lip and palate. One infant with cleft palate only had a diagnosis of familial Stickler syndrome limited to cleft palate with no other comorbid medical conditions impacting feeding or breathing.
All infants in the control group were using the level 1 nipple with 7 using the Dr. Brown’s Natural Flow Original and 8 using the Dr. Brown’s Options bottles. In the CP±L group, 7 infants were using the level 1 nipple and 8 infants were using the level 2 nipple on the Dr. Brown’s Specialty Feeding System. Although Dr. Brown’s provides general age guidelines regarding nipple flow selection, no association was found between nipple level and age (t(13) = −1.55, P = .145).
Demographic characteristics and medical information were collected from parent report and/or medical records. All infants with cleft lip and/or palate were prenatally diagnosed and 11 (92%) of those families had a prenatal consultation. A family history of clefting was reported for 3 (20%) infants in the cleft group. Two infants in the control group stayed in the NICU for a day and 2 infants with CP±L stayed for 3 and 17 days for feeding and respiratory concerns, respectively. The one infant with CP±L had been admitted to the NICU from a rural (non-pediatric) community hospital due to initial feeding difficulties, but quickly was found to successfully feed once transitioned to a different cleft bottle system.
Parent-reported feeding characteristics were collected during the study visit through a parent interview. Table 1 provides a summary of the parent interview data and the corresponding statistical comparisons. Statistically significant group differences were found in the type of milk offered, how the milk was provided, and the parent-reported feeding duration. In terms of nutrition, the majority of infants with CP±L were receiving formula from a bottle. Ten infants in the CP±L group were using standard-calorie milk, while 5 were using increased caloric formulations, ranging from 22 to 27 calories per ounce. Most of the control infants drank breast milk, either provided through breastfeeding, or pumped and offered in a bottle. The most commonly reported feeding duration range for the control group was 10 to 20 minutes, but for infants with CP±L, it was 20 to 30 minutes. Parent-reported milk intake during home feedings was 118.83 ± 30.95 mL for the infants with CP±L and 108.5 ± 25.49 mL for the control group (t(28) = −0.998, P = .327). Parents were also queried about feeding difficulties and could identify multiple feeding problems, if observed. Spitting up was the primary concern for both groups and coughing was reported for twice as many infants with CP±L than controls. No feeding difficulties were reported for 3 and 5 infants in the CP±L and control groups, respectively.
Parent-Reported Feeding Characteristics.
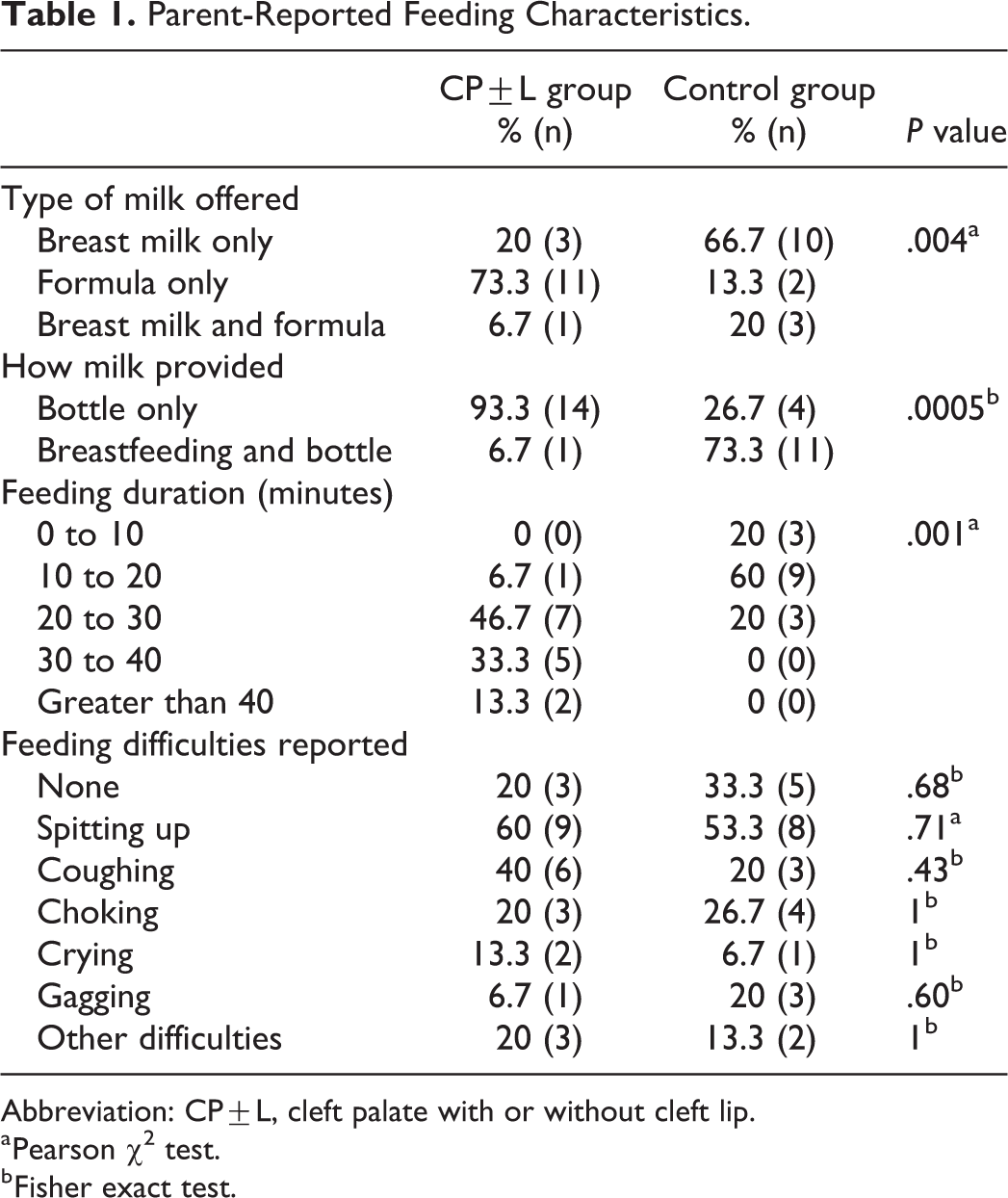
Abbreviation: CP±L, cleft palate with or without cleft lip.
a Pearson χ2 test.
b Fisher exact test.
Procedures
Weight, length, weight-for-length, and head circumference percentiles were obtained from birth and at the study visit. Growth percentiles were determined using the standard World Health Organization (WHO) growth chart for children aged 0 to 2 years (WHO Multicentre Growth Reference Study Group, 2006).
Developmental Screening
All parents completed the 2-month-old form of the Ages & Stages Questionnaires, Third Edition (ASQ-3) to gather information about the infants’ general developmental status and screen for signs of significant global developmental delay. The ASQ-3 is a standardized parent-report questionnaire to screen for developmental delays. The questionnaire includes 5 domains: Communication, Gross Motor, Fine Motor, Problem Solving, and Personal-Social. Each domain consists of 6 questions, with answer options of “Yes,” “Sometimes,” and “Not Yet.” Domain scores are totaled and compared to established cutoffs for interpretation and follow-up recommendations. Infants scoring 2 SDs below the mean require referral for further assessment.
No children scored below the cutoff in all domains of the ASQ-3 in either group. The Gross Motor domain was of particular interest in this study, due to the known improvement of oral sensorimotor skills as posture and muscle tone develop in infancy and childhood (Arvedson & Brodsky, 2002). None of the control infants were below the established cutoff for Gross Motor, but 2 of the infants with CP±L were below the cutoff score on this domain. Since the ASQ-3 is only a screening measure, the infants’ scores were not used as a prerequisite for eligibility in the study.
Bottle-Feeding Evaluation
Infants were fed with their own bottle, nipple, and milk (expressed breast milk or formula) by their parent. The timing of the study visit was based upon the infant’s typical feeding schedule to increase likelihood of the infant completing a feeding at the study visit. Prior to the feeding, the weight of the bottle with and without milk was obtained with a digital scale (Digital Pocket Kitchen Scale; GDEALER). Three measurements, in grams, were collected and an average was calculated. The volume of milk, in milliliters, typically offered during a feeding was measured during the session using the Similac Volu-Feed Nurser (Abbott Nutrition). All feedings were videotaped, focusing the camera on the infant’s face. Five minutes into the feeding, parents were required to take a break from feeding the child so a bottle weight measurement could be obtained. Parents often burped their infants during this break, which was not included in overall feeding time computation. After the weight measurement was obtained, the parents were instructed to resume the feeding without additional interruptions and were encouraged to feed as they would at home. Once the feed was finished, based on parent judgment or milk completion, the bottle’s end weight and the volume of any remaining milk were recorded. Feeding measures included the proficiency of the feeding (% volume taken during the first 5 minutes/total volume offered), rate of transfer (mL/duration of feeding in minutes), and overall transfer (% volume taken/total volume offered) (Lau et al., 1997; Lau & Smith, 2011). Parents were then asked whether the study feeding was typical to feeds at home and any differences were logged.
Measurement validation
The density of the breast milk or formula offered was obtained at the beginning of the visit by dividing the weight of the milk by the volume offered during the feeding. This allowed us to calculate the volume of milk remaining at 5 minutes and at the end of the feed. In order to validate the accuracy of our measurements, a comparison was performed between the final calculated volume, based on each determined density, and the measured remaining volumes obtained using a Similac Volu-Feed Nurser. The overall calculated volume for all infants was 102.99 ± 31.17 mL, while the measured volume was 103.03 ± 31.13 mL. Using a paired-samples t test, no significant differences were found between these values (t(28) = −0.30, P = .765, Cohen d = 0.056). Since the volume for 1 infant with CP±L was not measured with the standard Similac Volu-Feed Nurser at the end of the feed, this participant’s data were not included in this comparison.
Feeding session analysis
Feeding duration was measured based on review of the videotaped feeding session, and time was categorized into “active feeding” and “nonfeeding” periods. Active feeding was defined as the time when the nipple was in the infant’s mouth and nonfeeding included the time spent on other feeding actions (eg, burping, re-alerting, or calming the infant). Active and nonfeeding times were summed to compute complete feeding duration. The 5-minute measurement break was not included as part of this duration.
Two speech-language pathologists (SLPs) reviewed the videos for signs of aspiration, including coughing, wheezing, stridor, throat clearing, gagging, choking, wet voice, and wet/gurgly breathing (Weir et al., 2009). Both SLPs had over 5 years of postgraduate experience and expertise in feeding assessment of infants with cleft lip and palate.
The first SLP rater coded all videotaped feedings, while the second SLP coded 20% of the studies to compute inter-rater agreement. The first rater then re-coded a different set of 20% of the videos over a month after the initial ratings were completed. Raters documented the number of instances and the corresponding time of each aspiration symptom was observed. Following data collection, inter- and intra-rater reliability agreement was calculated.
Parent-reported typical feeding duration and the amount consumed at home were compared to the values collected during the videotaped feeding session.
Statistical Analyses
Parent-reported infant feeding characteristics were analyzed for both groups using descriptive statistics with Pearson χ2 tests or Fisher exact tests performed, with Fisher exact tests being employed for 2 × 2 comparisons when the sample size of one or more cell was less than 5. Independent-samples t tests were used to examine group differences in growth percentiles. One-way analysis of variance was performed to assess differences on feeding measurements with Bonferroni post hoc tests performed, as appropriate. Paired-samples t tests were used to compare parent-reported and observed feeding duration and intake. Cohen d was calculated to determine effect size. Analyses were performed using SPSS (IBM SPSS Statistics 24) and P values of less than .05 were considered statistically significant.
Results
Growth
Comparisons between the CP±L and control group revealed statistically significant differences in weight percentile (t(28) = 2.64, P = .013) and weight-for-length percentile (t(28) = 2.88, P = .008) at the study visit (Table 2). No additional group differences in growth were significant at birth or the study visit.
Growth Measurements for the CP±L and Control Groups.
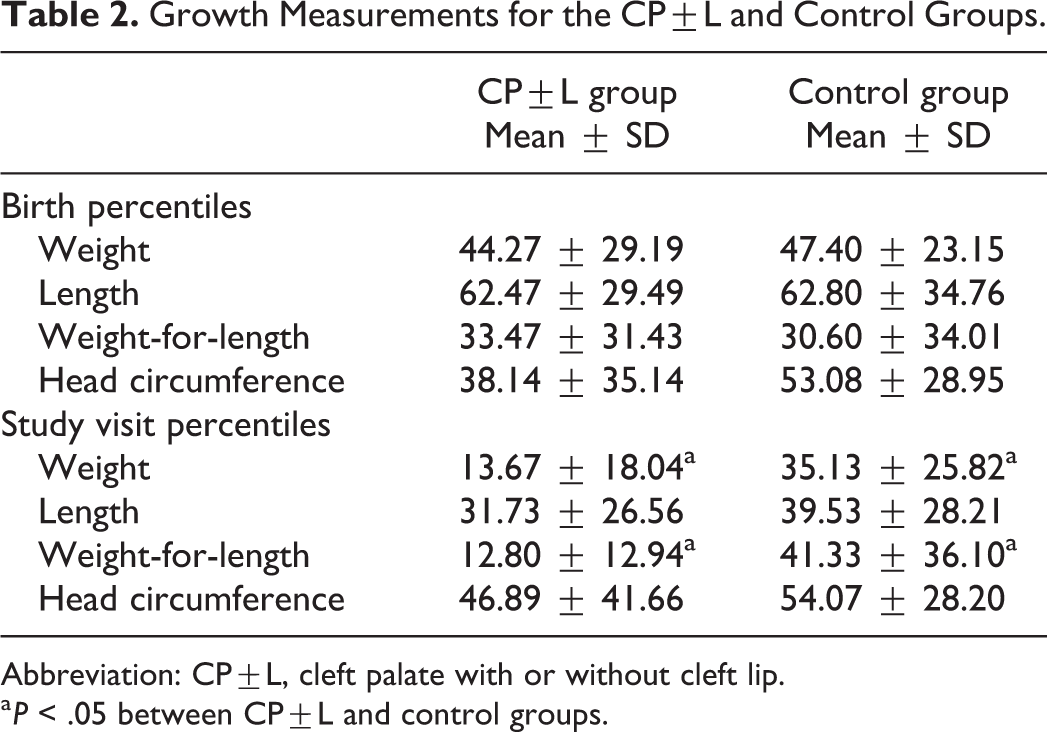
Abbreviation: CP±L, cleft palate with or without cleft lip.
a P < .05 between CP±L and control groups.
Feeding Proficiency and Overall Consumption
Feeding measurements were compared between controls, CP±L infants on the level 1, and CP±L infants on the level 2 nipples (Table 3). The volume offered initially, volume consumed in 5 minutes, and volume consumed during the entire feed were compared. Group differences were found in multiple measures. Feeding proficiency at the 5-minute measurement (F(2,27) = 21.14, P < .001) revealed differences between the control and CP±L subgroups on the level 1 (P < .001) and level 2 nipples (P < .001). Additionally, the percent of volume consumed (F(2,27) = 12.22, P < .001) was significantly different between the control infants and the infants with CP±L on the level 1 nipple (P < .001). Significant differences in milk consumption were also found between the infants with CP±L on the level 1 and level 2 nipples (P = .014).
Measurements Obtained During Bottle-Feeding Sessions.
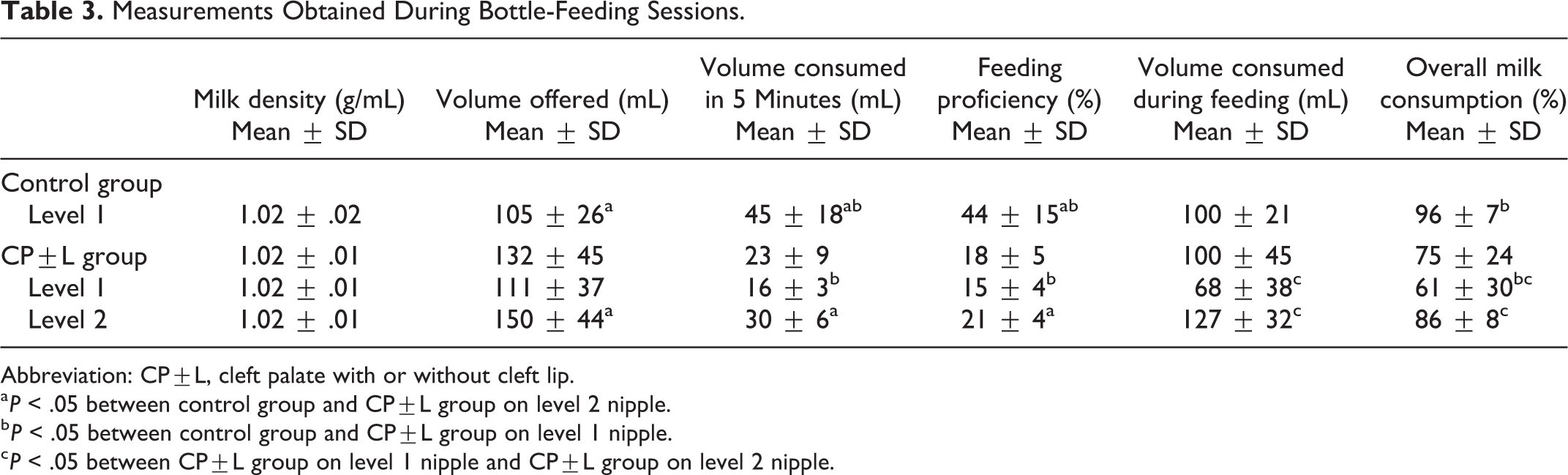
Abbreviation: CP±L, cleft palate with or without cleft lip.
a P < .05 between control group and CP±L group on level 2 nipple.
b P < .05 between control group and CP±L group on level 1 nipple.
c P < .05 between CP±L group on level 1 nipple and CP±L group on level 2 nipple.
Feeding Duration
Complete feeding duration, including active and nonfeeding time, was then examined. Significant group differences were noted in active feeding duration (F(2,27) = 13.55, P < .001), with differences found between control infants and infants with CP±L on the level 1 (P = .003) and the level 2 nipple (P < .001; Table 4). No differences were found within infants with CP±L by nipple flow level. Significant group differences were also noted in nonfeeding duration (F(2,27) = 5.14, P = .013) between the control group and the CP±L group on the level 1 (P = .046) and level 2 (P = .040) nipples. Much of the nonfeeding time for infants with CP±L included attempts to wake (n = 5) and calm (n = 2) the infant, while control infants were primarily burped (n = 5) and reengaged to suck as noted by the feeder twisting the bottle (n = 4) during this time. Complete feeding duration, which included active and nonfeeding time, revealed similar results (F(2,27) = 12.26, P < .001) indicating differences between controls and infants with CP±L on the level 1 (P = .003) and level 2 (P = .001) nipples.
Duration of Observed Feedings.
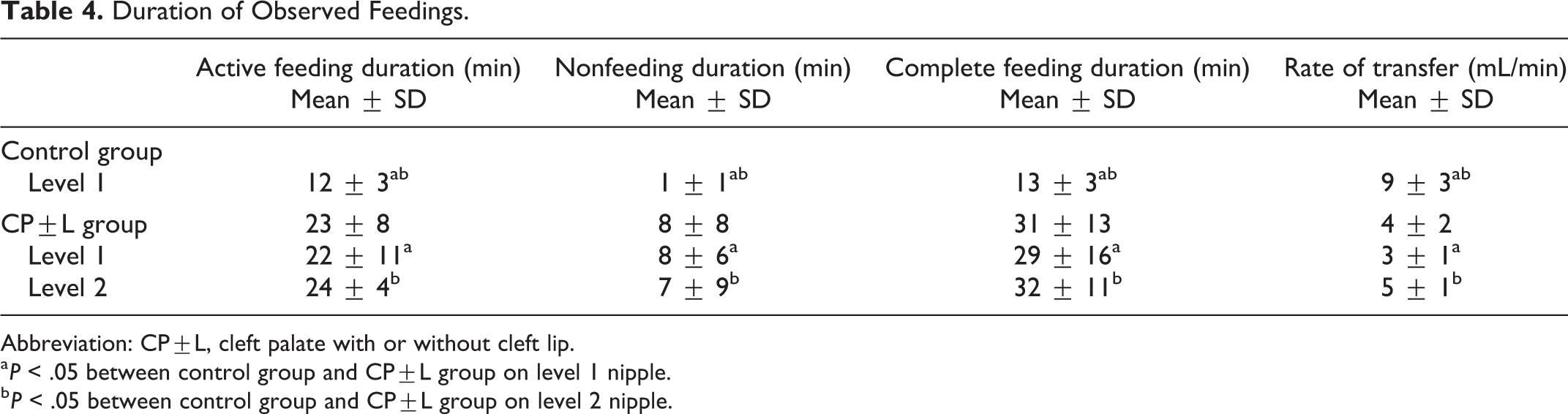
Abbreviation: CP±L, cleft palate with or without cleft lip.
a P < .05 between control group and CP±L group on level 1 nipple.
b P < .05 between control group and CP±L group on level 2 nipple.
Rate of milk intake (mL/min) was examined for the 3 groups revealing significant differences (F(2,27) = 16.49, P < .001). Differences were found between the control infants and the infants with CP±L on the level 1 (P < .001) as well as those on the level 2 (P = .007) nipples.
Feeding Difficulties
While no episodes of choking, wheezing, or wet voice were observed, coughing, stridor, throat clearing, gagging, and wet/gurgly breathing were noted by the SLP raters (Table 5). Five control infants demonstrated at least 1 feeding difficulty during the session, with 2 symptoms observed in 2 of those infants. In the CP±L group, 7 infants displayed feeding difficulties, with multiple challenges noted for 5 of the infants. While more difficulties were observed for the infants with CP±L, particularly those on the level 2 nipple, no statistically significant differences were found. Inter- and intra-rater agreement was 87.5% on the number of feeding difficulties observed.
Observed Feeding Difficulties for the Control and CP±L Groups.

Comparison to Parent Report
Parent-reported typical feeding duration and amount consumed at home were compared to the data obtained during the study visit feeding session. Paired-sample t tests indicated that parent-reported feeding duration for all of the infants (23 ± 12 minutes) was significantly greater than active feeding time at the study visit (18 ± 8 minutes, t(29) = 2.64, P = .013, Cohen d = 0.5) but was not statistically different from the complete study visit feeding duration (22 ± 13 minutes, t(29) = 0.54, P = .595, Cohen d = 0.1). When examining parent report of intake volume, paired-sample t tests indicated that reported intake (114 ± 28 mL) for all infants was significantly greater than the intake consumed at the study visit (100 ± 35 mL, t(29) = 2.19, P = .037, Cohen d = 0.4).
Nine (30%) parents (5 in CP±L group and 4 in control group) indicated subjective differences in the feeding performed during the study and typical feeds. Four parents indicated the feed was slower, 2 reported the infant drank less, and 1 parent stated the infant drank more than anticipated.
Discussion
Infants with CP±L often require the use of cleft-specific bottles to ensure adequate nutritional intake. Infant-driven feeding systems, particularly the Dr. Brown’s Specialty Feeding System (Madhoun et al., 2020), are typically one of the first feeding management strategies offered by craniofacial teams. While commonly utilized, it is unclear whether infants with CP±L using these infant-driven systems feed similarly to infants without clefts. Our results indicate that infants with CP±L using this infant-driven system demonstrate less efficient oral feeding skills than infants without clefts on comparable bottles.
Overall milk density measured during our study was comparable to the reported density of human milk and formula from past studies (Neville et al., 1988; Cichero et al., 2011). The volume of milk offered was greater for infants in the CP±L group on the level 2 nipple when compared to controls. This larger volume may have been due to medical provider recommendations. Specialists at the enrolling institution generally instruct parents to offer additional milk during feedings due to the known risk for growth deficits for infants with CP±L in attempt to increase caloric intake (Kaye et al., 2017).
Five minutes into the feeding, control infants already showed differences from infants with CP±L on both the level 1 and level 2 nipples in the amount they consumed, which influenced their feeding proficiency. Control infants finished almost half of their feed during this time, compared to less than 20% for infants with CP±L. This feeding proficiency represents the infants’ feeding skill, as fatigue should be minimal at this time, based on the oral feeding skill levels (Lau et al., 1997; Lau & Smith, 2011). While the tool describing these levels was developed for preterm infants, it is interesting to note that none of the infants with CP±L met the expected 30% feeding proficiency described, as compared to 87% of control infants that exceeded this feeding proficiency guideline. This indicates generally decreased nutritive feeding skills for infants with CP±L in this study.
The overall percentage consumed differed between controls on the level 1 nipple and infants with CP±L on the same nipple; however, overall volume consumption did not differ. Again, this may have been due to the larger offered volumes for infants with CP±L. Differences were noted between the CP±L subgroups on the 2 different nipple flows for the overall percent and total volume consumed during the feeding. Infants on the level 2 nipple consumed more, which may be a result of the decreased effort required for extraction because of the larger nipple orifice.
Published Dr. Brown’s fluid flow rates differ based on the nipple level, with 9.21 mL/min and 14.96 mL/min found for the level 1 and level 2 nipples, respectively, when tested using a standard breast pump (Pados et al., 2015; Pados et al., 2016). The flow rate for the level 1 nipple was similar to the 9 mL/min found in our study for infants without clefts. However, these expected values differed with our findings for the CP±L group when the Infant Paced Feeding Valve was utilized. This discrepancy was especially noticeable with the level 2 nipple. This may explain why more infants with CP±L began using the level 2 nipple sooner, as they may have struggled with decreased intake and prolonged feeding time (Clarren et al., 1987; Arvedson & Brodsky, 2002; Reid et al., 2007; Miller, 2011).
Maximum feeding duration should be 20 to 30 minutes for infants who have a stable respiratory system without neurological involvement (Arvedson & Brodsky, 2002). Complete feeding duration exceeded 30 minutes for almost half of the infants in the CP±L group, whereas no controls exceeded 20 minutes. This may have contributed to the poorer weight gain observed in the infants with CP±L. Perhaps due to the fear of malnutrition, parents may feel compelled to ensure an infant with cleft palate drinks all the milk offered, even when the recommended feeding time is exceeded. However, the trade-off is that excessive feeding duration can result in increased caloric expenditure and decreased periods of rest between feedings.
Cleft team clinicians frequently ask parents about their child’s feeding duration, but providers should use this information with caution, as this may not always accurately capture true feeding duration. Complete feeding duration (including active and nonfeeding time) appeared to be closer to the duration reported by parents. Differences appeared to exist between parental report and active feeding time, with the reported time exceeding active feeding. This indicates that active feeding time and caloric expenditure may not be accurate when obtained by parent report alone, unless further clarification is obtained.
Reid et al (2006) calculated the rate of milk intake for infants with clefts based on parents’ report of the amount typically consumed and the feeding duration. It was proposed this measurement could be used as a screening tool to identify infants with poor feeding skills, stating that it would be “unrealistic” to perform feeding assessments on all infants. These measurements were compared to the results obtained from a reference test with cutoff scores of <2.2 mL/min at 2 weeks and <3.3 mL/min at 3 months, proposed to identify poor feeders (Reid et al., 2006). While infants in our study fell between these ages, it is interesting to note that all infants in the control group exceeded the proposed 3-month cutoff, even prior to this age, compared to only 11 infants with CP±L. Of the 4 infants with CP±L who did not meet this rate, one was found to fall below the proposed 2-week cutoff of 2.2 mL/min.
Almost half of the infants with CP±L (47%) were observed to demonstrate at least 1 observable sign of feeding difficulty during the study, compared to 33% of infants without clefts. Reid (2006) noted that 65% of parents of infants with clefts who were poor feeders reported findings, such as nasal regurgitation, coughing, choking, gagging, and distress, at 3 months of age. These findings are consistent with the debate about whether pharyngeal swallow function remains intact for nonsyndromic infants with CP±L, with questions arising about the increased risk of aspiration in this population following normal laryngeal descent (de Blacam et al., 2018). However, this could be an indication of other underlying medical conditions not yet diagnosed due to the young age of the infants.
Limitations
Since only 1 infant-driven cleft feeding system was evaluated in this study, it is unclear whether other systems would perform similarly. Evaluation of other feeding systems is warranted to determine which is the most efficient to safely deliver adequate nutrition. The inclusion of more infants using each nipple level would also be useful as well as the use of additional nipple flow levels.
Since the feeding session was conducted in a clinical space, the study feed may have been less representative of typical feeds at home. There also may have been innate variability in infants’ feeding skills, which may not have been captured with the observation of a single feed. The use of home feeding journals or the examination of more than 1 feed may be useful in future studies to ensure feeding sessions are as representative as possible. Furthermore, the use of a comprehensive standardized developmental assessment (eg, Bayley Scales of Infant and Toddler Development), in addition to the feeding assessment, may more accurately describe the developmental and feeding skills of infants with clefts in future studies.
Video recordings did not include an external microphone on the infant, which may have limited the ability to listen for more subtle evidence of feeding disturbance (eg, wet/gurgly breathing). Video review was also not blinded to the infants’ group, potentially causing unintended bias in feeding ratings. Since the majority of infants in the CP±L group had a visual deformity due to the presence of a cleft lip, blinding to group would have been difficult without modification to the recorded images.
Clinical Implications and Future Directions
The bottle-feeding skills of infants with CP±L appear to be less efficient than those observed in healthy, noncleft infants, even with the use of a cleft-specific feeding system. The results of this study support the need for close clinical monitoring of feeding and growth for infants with CP±L in early infancy to promote success. Due to the risk of malnutrition from prolonged feedings with decreased intake, cleft teams should adopt a low threshold for other interventions, such as milk fortification, offering increased volumes of milk, or the use of faster flowing nipples. Specialized providers, such as feeding therapists and dietitians, should monitor these modifications closely with a team approach. While these providers are not required members of craniofacial teams (ACPA, 2018), their presence and involvement is essential to the care of infants with clefts. A dedicated multidisciplinary cleft feeding team could provide further caregiver and infant supports to promote improved feeding and growth outcomes for infants with CP±L (Baylis et al., 2018).
Teams should consider periodically observing complete feeding sessions during appointments to determine feed duration, intake amount, and the presence of feeding difficulties. Parents should be asked how representative the observed feeding was compared to home feeds. Such observation should particularly be conducted on infants with a history of prolonged feeds, signs of feeding challenges, and those with poor weight gain.
If infants with CP±L are able to tolerate the flow of the level 2 nipple, it may be advantageous for feeding providers to promote its use. This may result in increased intake and/or shorter feeding duration. However, due to the potential of pharyngeal swallow dysfunction from the increased flow rate, close monitoring should be performed during craniofacial appointments and at home.
Lastly, the refinement or development of improved feeding systems for infants with CP±L may be necessary to “normalize” feeding skills. Reduced extraction rate may be a primary cause of decreased proficiency and increased feeding duration. Modified valves to improve milk flow or specialized nipples to improve compression flow rate to allow for additional extraction should be explored.
Conclusion
Even with the use of specialty bottle systems, infants with CP±L differ from their noncleft peers in feeding proficiency, rate of milk transfer, and feed duration. Due to these results, additional feeding strategies may be needed for infants with CP±L in early infancy to support adequate growth and development and to prepare for required surgical interventions. These strategies may include the use of feeding interventions, such as milk/formula fortification or faster flowing nipples, if tolerated. Specially trained feeding providers on cleft teams should initiate the use of these modifications, with close monitoring, to care for these high-risk infants. Future research studies should explore the feeding skills of infants with CP±L as well as the development or modification of current cleft feeding systems to safely maximize feeding outcomes.
Footnotes
Authors’ Note
Results from this project were presented on April 12, 2019, at the 2019 Annual Meeting of the American Cleft Palate-Craniofacial Association in Tucson, Arizona.
Acknowledgments
Special thanks to Drs. Eric Healy and Youkyung Bae for their mentorship and to Mrs. Caitlin Cummings for her assistance with video review.
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from the Ohio Speech-Language-Hearing Association.