
Abstract
Objective:
To identify the cultural beliefs about the causes of cleft among parents of patients with nonsyndromic cleft lip and/or palate in a multiethnic society in Malaysia and the difficulties encountered in receiving cleft treatment.
Design:
A descriptive cross-sectional multicenter study based on a study questionnaire was conducted of parents of patients with cleft lip and/or palate.
Setting:
Three centers providing cleft care from different regions in Malaysia: the national capital of Kuala Lumpur, east coast of peninsular Malaysia, and East Malaysia on the island of Borneo.
Participants:
Parents/primary caregivers of patients with cleft lip and/or palate.
Results:
There were 295 respondents from different ethnic groups: Malays (58.3%), indigenous Sabah (30.5%), Chinese (7.1%), Indian (2.4%), and indigenous Peninsular Malaysia and Sarawak (1.7%). Malay participants reported that attributing causes of cleft to God’s will, superstitious beliefs that the child’s father went fishing when the mother was pregnant or inheritance. Sabahans parents reported that clefts are caused by maternal antenatal trauma, fruit picking, or carpentry. The Chinese attribute clefts to cleaning house drains, sewing, or using scissors. Cultural background was reported by 98.3% of participants to pose no barrier in cleft treatment. Those from lower socioeconomic and educational backgrounds were more likely to encounter difficulties while receiving treatment, which included financial constraints and transportation barriers.
Conclusion:
There is a wide range of cultural beliefs in the multiethnic society of Malaysia. These beliefs do not prevent treatment for children with cleft. However, they face challenges while receiving cleft treatment, particularly financial constraints and transportation barriers. Such barriers are more likely experienced by parents from lower income and lower education backgrounds.
Keywords
Introduction
Isolated cleft palate and cleft lip with or without cleft palate are the most common congenital craniofacial anomalies reported worldwide, occurring in approximately 1: 1000 live births (Dixon et al., 2011), with ethnic variation. Generally, populations of Asian descent have the highest prevalence of about 2 per 1000 births, with Caucasians having an intermediate prevalence of 1 per 1000 and African populations having the lowest prevalence (Cooper et al., 2006). In Malaysia, an incidence of cleft lip, cleft palate, and a combination of both has been reported in 1 of 941 births (National Oral Health Survey of School Children, 1998). A 2005 study reported that 11.9% of major birth defects in the Kinta District of the state of Perak, Malaysia, were cleft lip and palate (Thong et al., 2005). Cleft surgery and consultation are mainly offered in plastic and reconstructive surgery units in Malaysia.
Malaysia is a developing country with a population of 28.3 million people from multiracial and multiethnic backgrounds, with Malays, Chinese, and Indians being the major ethnic groups. Minor ethnic groups that contribute to the cultural background of the country include the indigenous people of Sabah and Sarawak, the 2 eastern states on the island of Borneo.
Treatment for a child with cleft starts from the antenatal period during the first detection of cleft until well into adulthood. There is no doubt that many factors could influence the upbringing and treatment of a child with cleft. It starts in the home, mainly by the parents or primary caregivers, and extends among the immediate and extended family members. Furthermore, health-care workers and society also impact the life of a child with cleft. Cultural views and opinions play a key role in people’s belief systems concerning the etiology of medical conditions and illnesses. The Cambridge English Dictionary defines culture as “the way of life, especially the general customs and beliefs, of a particular group of people at a particular time.” Beliefs regarding the etiology of clefts are not always scientifically based. Cultural factors influence the attitudes and behavior toward cleft lip and palate as well as beliefs around the causation and treatment of clefts. A previous study has shown that in diverse multicultural societies, the variety of cultures represents diversification in beliefs about disability and family life (Olasoji et al., 2007).
Currently, plastic surgery units across Malaysia offering cleft services are mainly situated in state capitals. However, not all states have a dedicated resident plastic surgeon and cleft team. As for the states of Sabah and Sarawak, on the island of Borneo, even with allocated plastic surgeons offering cleft surgery, the service is still considered insufficient because of its large geographical area. To reduce the traveling burden for patients, visiting sessions in more rural districts and hospitals are being carried out. Cleft treatment in Malaysia is part of the national health system and is subsidized by the government. There are also nongovernmental organizations helping with cleft families in getting treatment. A multidisciplinary team approach where applicable is practiced to ensure comprehensive cleft care is being carried out. However, access and availability to such care are still somewhat suboptimum and much can improved.
The perceptions about the causes of cleft in the multiethnic and multiracial country of Malaysia have not been well described. In other parts of the world, causal attributions for clefts are influenced by culture and play a vital role in people’s behavior toward seeking medical treatment (Mednick et al., 2013). A previous study in the neighboring Philippines reported that cleft is seen as caused by extreme reactions to food cravings or pagaglilihi, animals, or objects among pregnant women (Bondoc & Ligot, 2015). Chinese participants in one study were reported to believe that putting sharp objects on the bed (such as knives or scissors) when a woman is pregnant results in the baby being born with a cleft lip or palate (Lee et al., 2009). Certain tribes in Nigeria attribute the causes of cleft to witchcraft, evil spirits or the devil, the mother, and occasionally the child (Oginni et al., 2010). Other ethnic groups in Nigeria such as the Yoruba attribute the etiology of cleft to supernatural forces (evil spirits and ancestral spirits), while the Hausa/Fulani attribute it to the “will of God” (Olasoji et al., 2007). A study of a group of South African adult patients with cleft found that some attributed the cause of their clefts to curses or superstitious beliefs that their mothers had handled sharp objects during an eclipse (Patel & Ross, 2003).
In another study in a South African setting, traditional healers’ beliefs attributed the causes of cleft to the patients’ ancestors. The traditional healers believed that ancestors would single out a baby with cleft in order to bless the baby with supernatural powers or to punish the child’s mother (Dagher & Ross, 2004). The traditional healers in this study also believed that cleft was caused by curses from jealous people or the result of eating poisoned rabbit meat. The term harelip is associated with cleft lip and/or palate because of the resemblance of the slit-like mouth found on rabbits (Dagher & Ross, 2004). Another study by Ross (2007) found that Muslim and Hindu traditional healers believed that cleft was caused by God or that it was a result of a pregnant woman handling a sharp object during an eclipse.
In Mexico, a solar eclipse was also believed to be the cause of cleft. Pregnant women were believed to be in danger of birthing a baby with a craniofacial cleft if a solar eclipse was to occur (Castro, 1995). In India, some beliefs on the cause of cleft attribute it to sins from a past life (Weatherley-White et al., 2005). Other religious and cultural beliefs regarding the causes of clefts include witchcraft, God’s will, and engaging in a behavior associated with causal power (eg, looking at a child with a facial difference when pregnant; Mednick et al., 2013).
This shows that communities from different parts of the world have different beliefs regarding the causes of cleft. These beliefs may or may not affect the overall treatment and care of cleft in these countries. However, in Malaysia, this has not been explored before. As a melting pot of cultures and ethnicities, the Malaysian context can serve as an example of how different beliefs on the causes of cleft in multiracial and multiethnic communities influence the overall treatment and care for cleft.
Methods
The study was conducted in multiple centers in Malaysia providing cleft services. These include Hospital Kuala Lumpur, Hospital Universiti Sains Malaysia in Kubang Kerian, Kelantan, and Hospital Queen Elizabeth in Kota Kinabalu, Sabah. Malaysia, a country in the Southeast Asian region, is a multiethnic and multicultural society consisting of Malays, Chinese, Indian, Orang Asli (indigenous people of Peninsular Malaysia), and indigenous people of Sabah and Sarawak, 2 states situated on the island of Borneo. The centers chosen were based on their geographical locations in the country representing different population backgrounds. This study was approved by Human Resource Research Ethics Committee of Universiti Sains Malaysia USM/JEPeM/15120557 and Medical Research Ethics Committee (MREC), Ministry of Health Malaysia (NMMR-15-2107-24350).
This was a descriptive cross-sectional study involving parents/primary caregivers of patients with nonsyndromic cleft aged between newborn and 18 years old. The contacts of the patients were collected from various sources including records from specialist clinics, operation books, and admissions to neonatology units. They include patients with scheduled follow-up visits. Clinical diagnostic codes and surgical codes were utilized to identify these patients. The sample size was determined by using single proportion formula: (1.96/Δ)2 (p[1 − p]), where p is a proportion value obtained from a previous study related to cultural beliefs on causes of cleft lip and palate at 20% (Mednick et al., 2013) and Δ is the precision set at 5%, total number of sample calculated was 294 after adding 20% drop out rate. Later, a simple random sampling method was applied to the list of contacts collected.
Parents/caregivers were interviewed based on a questionnaire developed for this study. The questions included sociodemographic data, clinical background, and information on difficulties encountered while receiving cleft care. Parents were also asked open-ended questions in regard to their cultural beliefs about the causes of cleft. Participants’ responses to questions were written on the questionnaire during interviews conducted during outpatient clinic appointments or inpatient hospital admissions. Interviews were conducted by medical officers/doctors in departments of plastic surgery of the involved centers which lasted around 15 to 20 minutes. Responses to open-ended questions were tallied using the categories matching the wording of the participants without further thematic analysis.
Data were entered and analyzed using Statistical Package for the Social Sciences software Version 24.0. Descriptive statistics for the collected variables were computed. For the objective of determining factors associated with encountering difficulties in receiving cleft treatment, binary logistic regression was used. Several categorical variables were recategorized into binary variables, such as the level of education was categorized into lower and higher education levels, income was categorized into RM2000 and less and more than RM2001, ethnicity was categorized into Malay and non-Malay, and type of religion was categorized into Muslim and non-Muslim. Those variables with P value < .25 in the simple logistic regression were included in multiple logistic regression analysis. Forward selection, backward elimination, and manual entry and manual forward methods were utilized to get the best model. All assumptions of multiple logistical regression models were evaluated as well as multicollinearity and interactions; P values of < .05 were considered statistically significant.
Results
The Sociodemographic Data of Caregivers
A total of 298 parents and caregivers were approached to participate in the study and 295 respondents were included. Those not included were due to their non-Malaysian citizenship and 2 decided to retract their participation midway the interview. Their socioeconomic demographic data were taken into consideration as shown in Table 1. Estimates of ethnicity and religion from the general population as comparison to the sample size are also included in Table 1. Of the 295 participants, 222 (75.3%) were biological mothers and 62 (21.0%) were biological fathers to patients with cleft.
Socioeconomic Demographic Data of Parents/Caregivers.a
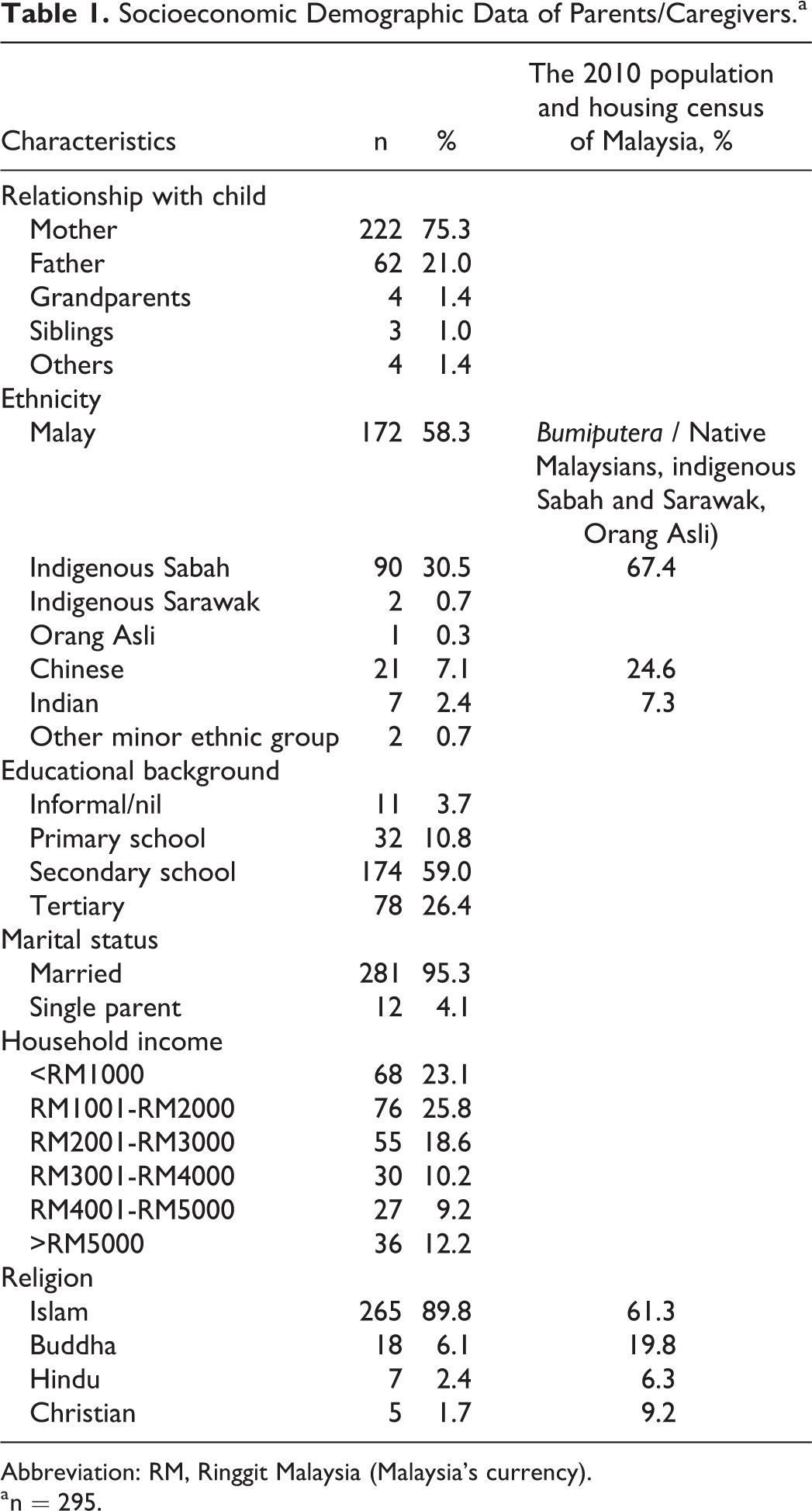
Abbreviation: RM, Ringgit Malaysia (Malaysia’s currency).
a n = 295.
The religious composition of our respondents included 265 (89.8%) Muslims, 18 (6.1%) Buddhists, 7 (2.3%) Hindus, and 5 (1.7%) Christians.
Further information regarding the children was also obtained. The children were all Malaysian citizens with nonsyndromic cleft. There were 165 male (55.9%) and 130 (44.1%) female with 233 (78.9%) of them have had surgical intervention by a plastic surgery team and 62 (21.1%) had not. The children were aged from infancy to adolescence. There were 136 (46.1%) children aged from newborn to 24 months, 111 (37.6%) aged 25 months to 5 years old, and 48 (16.3%) aged 5 years old till 18 years old. Majority of the respondents were Malay and Muslim who represent the majority of the population of Malaysia.
Cultural Beliefs on Causes of Cleft
There was a wide range of beliefs regarding the etiology of cleft, as shown in Table 2. The most common cause of cleft was attributed to God’s will, with 53 (18.0%) respondents subscribing to this belief. Other respondents attributed cleft to popular beliefs that the father of the child went fishing during the antenatal period (45 respondents = 15.3%); the cleft was an inherited condition (24 respondents = 8.1%); and physical trauma experienced by the mother during the antenatal period (16 respondents = 5.4%). However, the majority of the respondents (93 = 31.5%) stated that they were unsure of their cultural beliefs regarding the etiology of clefting.
The Beliefs of Parents/Caregivers on the Cause of Cleft Lip and/or Palate.a
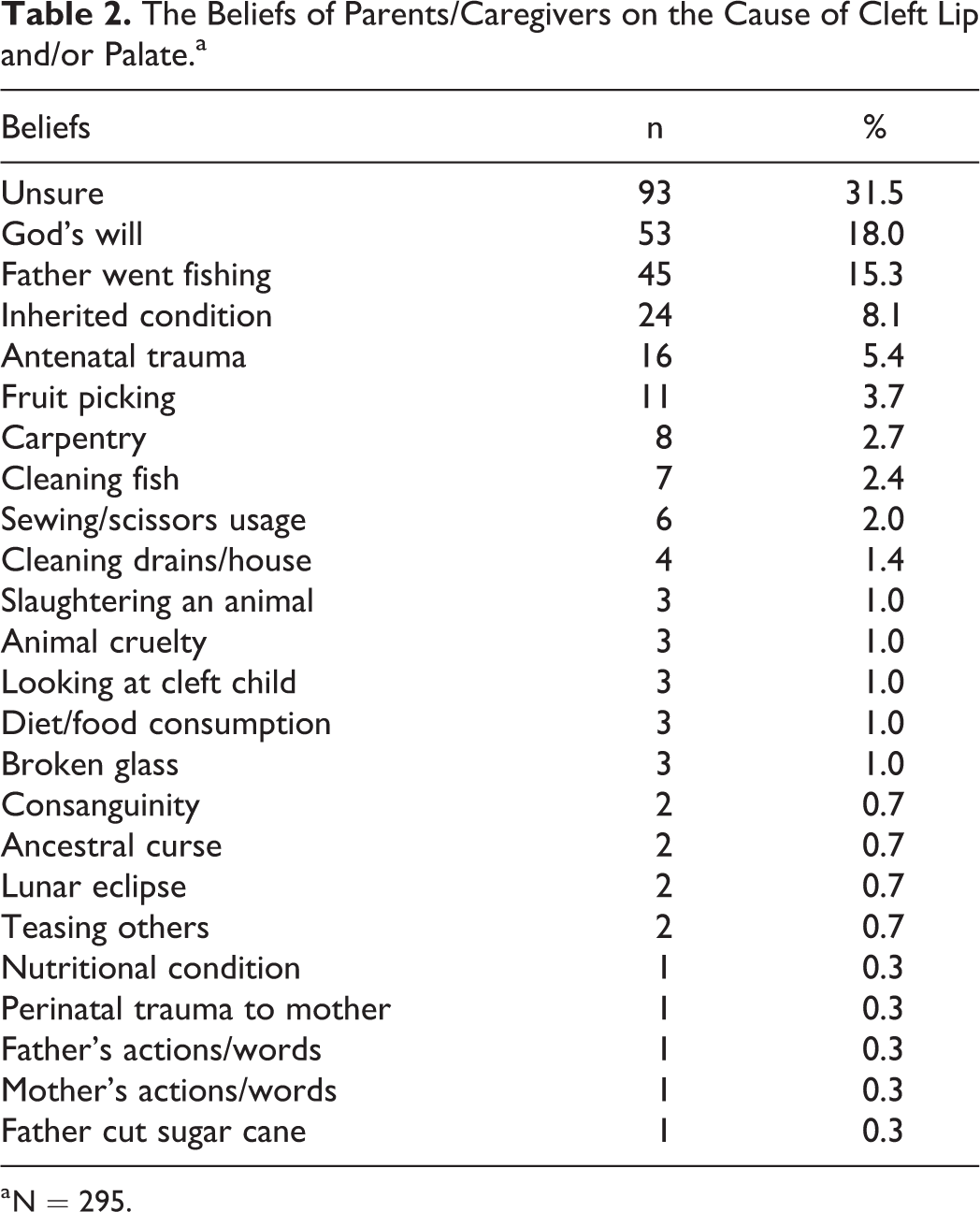
a N = 295.
Of the 172 (58.3%) Malay participants, 50 (29.1%) attributed the cause of cleft to the act of God’s will. About 35 (35%) believed the father of the child went fishing during the antenatal period, and 19 (11.0%) believed that cleft was an inherited condition, while 47 (27.3%) were unsure about the cultural beliefs on the causes of cleft in Malay culture.
Twenty-one (7.1%) participants were Chinese people. From these respondents, 4 (19.0%) attributed cleft to the act of cleaning their houses, especially the drains during pregnancy; 3 (14.3%) believed that cleft was caused by the usage of scissors and sewing during pregnancy; and another 3 (14.3%) believed cleft was an inherited condition. Eight (38.1%) of these respondents were unsure about their cultural beliefs regarding the etiology of cleft.
Seven (2.4%) of the respondents were Indian. Two (28.3%) of them attributed cleft to the belief that the father of the child went fishing during the antenatal period, 1 (14.3%) attributed cleft to consanguinity between parents of the cleft child, and 2 (28.3%) believed that cleft was caused by a lunar eclipse that occurred during pregnancy. The other 2 (28.3%) Indian respondents were unsure of the cultural beliefs that are believed to cause cleft in Indian culture.
Ninety (30.5%) of the respondents were from the indigenous people of Sabah. There was a wide range of beliefs about the causes of cleft among the Sabahan people; 13 (14.4%) believed cleft was caused by physical trauma experienced by the mother during the antenatal period, 11 (12.2%) attributed cleft to fruit picking during pregnancy, and 8 (8.9%) attributed it to the belief that the child’s father went fishing during the antenatal period. Another 8 people (8.9%) believed that any carpentry activity during the antenatal period caused cleft. Thirty-four (37.8%) of the Sabahan people unsure of their cultural beliefs about the cause of cleft.
We also had respondents from the indigenous Sarawak people, Orang Asli, and other ethnicities. Their beliefs about the cause of cleft were similar to previous racial groups, with an additional belief that cleft was a result of mothers looking at cleft patients during pregnancy.
Despite the different beliefs across different racial and ethnic backgrounds, 290 (98.3%) respondents agreed that their cultural beliefs and background did not prevent them seeking treatment for their cleft child. Only 5 (0.7%) respondents admitted that their cultural background prevented treatment for patients with cleft.
Difficulties Encountered in Receiving Cleft Treatment
We asked our respondents about the challenges they face while seeking or receiving treatment for their child with cleft (Table 3).
Difficulties Encountered by Parents/Caregivers in Seeking or Receiving Cleft Treatment.a
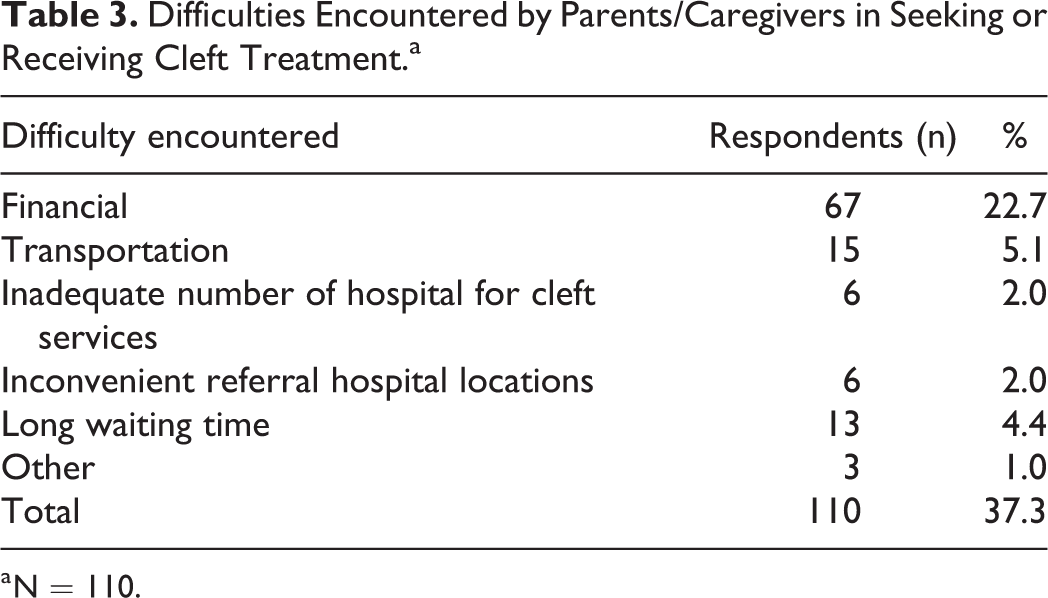
a N = 110.
There were 185 (62.7%) respondents who did not encounter any difficulties, while 110 (37.3%) admitted to facing some difficulties. Sixty-seven (22.7%) people reported that they faced financial constraints, 15 (5.1%) had transportation issues, and 13 (4.4%) experienced a long waiting time for surgery. Six (2.0%) participants identified inconvenient referral hospital (locations) as a challenge, while another 6 (2.0%) felt that there were not enough hospitals providing cleft services.
Simple logistic regression was conducted to explore the factors associated with difficulties encountered in receiving treatment for cleft (Table 4). Only a few factors were proceed into multivariable analysis. They included child’s age, race, and education level of the parents/caregivers. Lower education refers to not receiving any formal education or only receiving formal primary and secondary education. Higher education level refers to further education obtained beyond secondary level, that is, tertiary education.
Factors Associated With Difficulties in Receiving Cleft Treatment (Univariable Analysis).
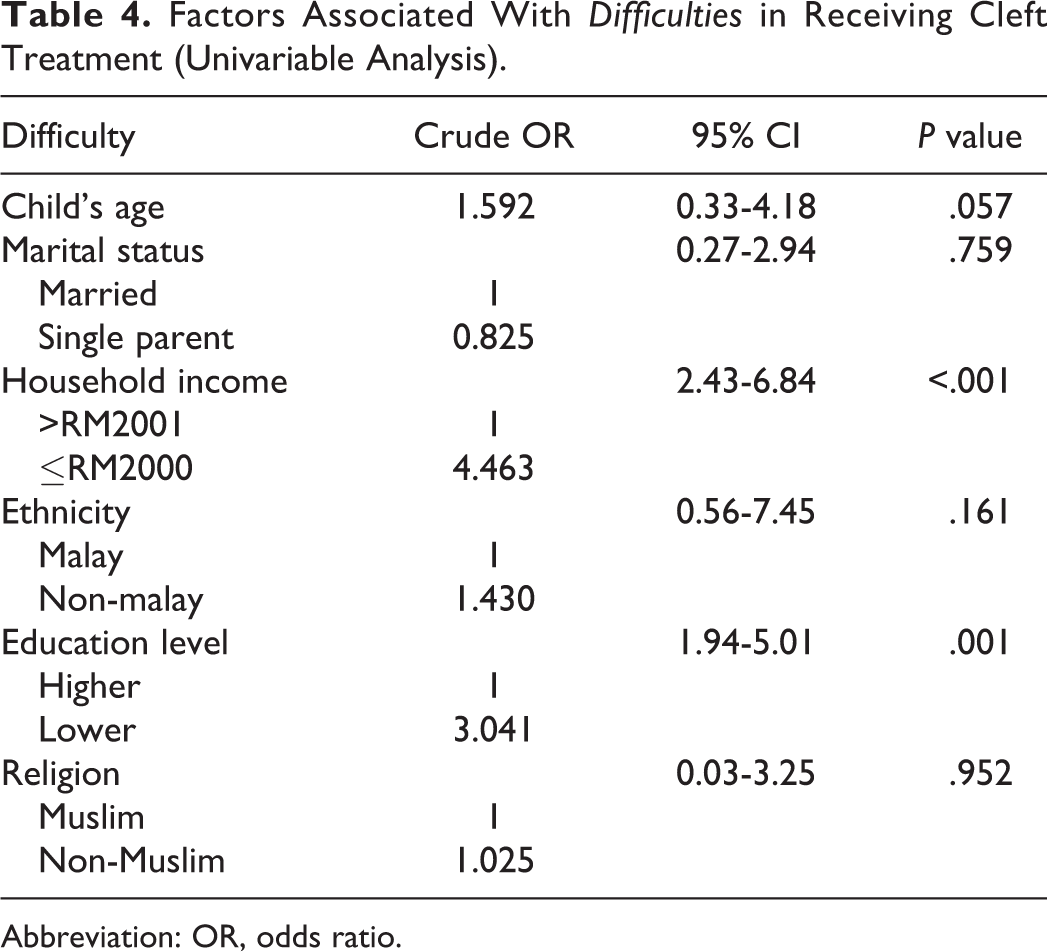
Abbreviation: OR, odds ratio.
As shown in Table 5, significant factors associated with barriers were household income RM2000 and less (adjusted odds ratio [OR]: 4.46; 95% CI: 2.68-7.44; P < .001) and lower education level (adjusted OR: 2.29; 95% CI: 1.13-4.62; P = .021). Other factors significant during simple logistic regression were found to be insignificant.
The final model in Table 5 shows that respondents with a monthly income of RM2000 and less have 4.46 ORs of encountering barriers in receiving cleft treatment, and inferring to the population with similar problems, the ORs fell between 2.68 and 7.44. Respondents with lower education also had 2.29 ORs of encountering barriers in receiving cleft treatment, and inferring to the population with similar problems, the ORs fell between 1.13 and 4.62.
Factors Associated With Difficulties in Receiving Cleft Treatment (Multivariable Analysis).a
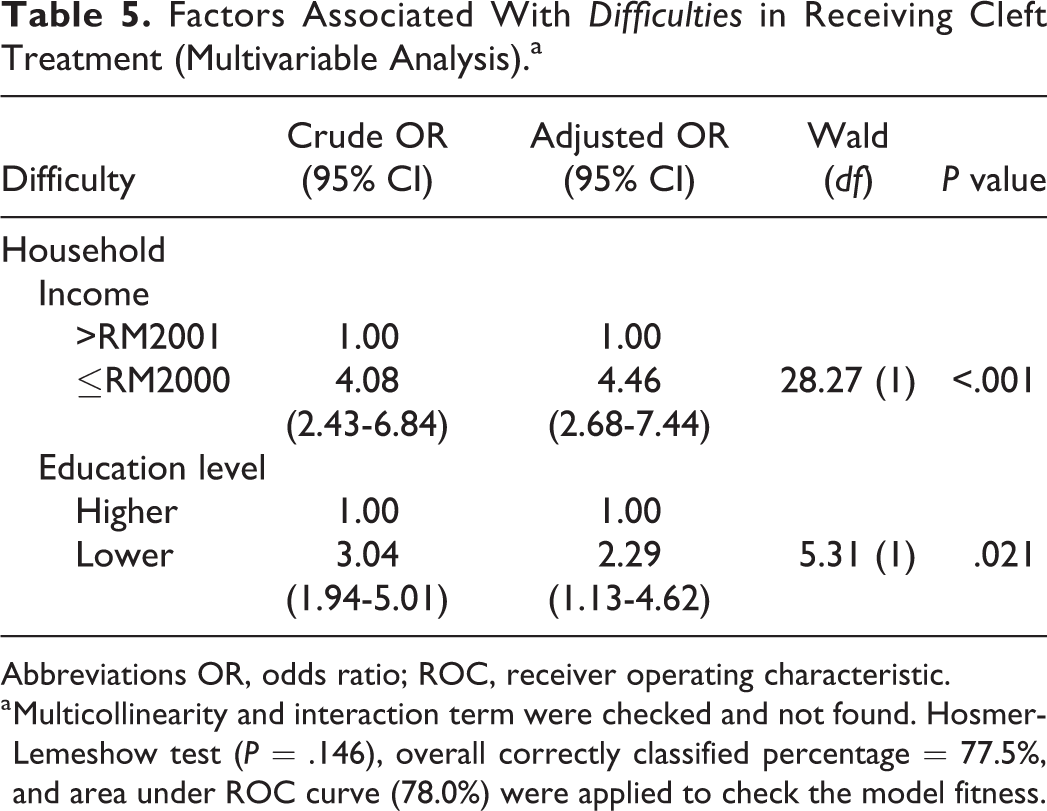
Abbreviations OR, odds ratio; ROC, receiver operating characteristic.
a Multicollinearity and interaction term were checked and not found. Hosmer-Lemeshow test (P = .146), overall correctly classified percentage = 77.5%, and area under ROC curve (78.0%) were applied to check the model fitness.
Discussion
Orofacial clefts remain a crucial component in most plastic and reconstructive services worldwide. An effective delivery of integrated care for patients with cleft has been proven to achieve optimum results. We conducted a study among parents and caregivers of patients with cleft and investigated their demographic background, beliefs about the etiology of cleft based on their cultural background, and difficulties encountered in receiving cleft treatment.
In keeping with previous studies (Olasoji et al., 2007; Oginni et al., 2010; Mednick et al., 2013), a wide range of beliefs was found regarding the etiology of cleft in our local setting. The most common belief attributed cleft to God’s will, stated by 18.0% (n = 53) of the participants. Other popular beliefs attributed cleft to a child’s father fishing during the antenatal period (15.3%, n = 45), a hereditary condition (8.1%, n = 24), and mother’s physical trauma during the antenatal period (5.4%, n = 16). However, a rather significant number of respondents (31.5%, n = 93) stated that they were unsure of their cultural beliefs regarding the causation of cleft lip and/or palate. We speculate this is due to a younger cohort of couples/parents of children with cleft palate. They represent a newer generation of young adults who may not be aware of their cultural beliefs about the cause of cleft. As with many of these beliefs, stories are passed down from generation to generation and tend to fade or even disappear over time. Some may find these beliefs to be irrelevant in the current modern age of technology. However, we believe that these beliefs are integral in the sociocultural epidemiology of cleft lip and/or palate as well as in coping with the disease. In this regard, it is important to point that given the religious background of Malays as Muslims, many of them attribute cleft to Allah’s (God’s) will. Islam, then, encourages people facing such challenges to do so with patience and gratitude, which in turn will earn them Allah’s favor and open the pathway to Paradise (Ross, 2007).
Although Malaysia is predominantly an Islamic and democratic country, other religions can be freely practiced. This is in keeping with most of our respondents being Malay, who are Muslims by default. Other ethnicities from the indigenous Sabahan cohort, such as Bajau and Bugis, commonly practice Islam as well. Other faiths like Buddhism and Christianity are commonly practiced by the Chinese, the Indians, and the Dusun and Kadazan people of Sabah. Hinduism is more common among Indians.
We take note the discrepancy of our data with the national demographics from the Population and Housing Census of Malaysia in 2010 which showed that Malaysia’s population consisted of 24.6% Chinese (vs 7% of sample) and 7.3% Indian population (vs 2% of sample). The distribution of religion also does not match from national rates (Islam 61.3% vs 89.8% in the sample; 19.8% Buddhism vs 6.1% in sample; Christianity 9.2% vs 1.7% in sample; Hinduism 6.3% vs 2.4% in sample). We attribute this to the collection of data involving 3 centers only and foresee this can be overcome in the future by including more centers providing cleft care in various regions of Malaysia. This panoply of different religious backgrounds could explain why a significant percentage of our respondents attributed the cause of cleft to God’s will.
Regarding the belief among the Sabahan people that cleft is caused by fruit picking during pregnancy, it is worth mentioning that most of the edible tropical fruits grow from high trees in Malaysia. To harvest them requires a pole-like instrument commonly called the galah. However, we did not obtain a clear explanation as to how using this apparatus for fruit picking is related to orofacial clefting. Perhaps future studies focusing on Sabahan respondents might provide additional information.
Based on the 21 Chinese participants, cleft was attributed to the act of cleaning houses, especially the drains, or to the usage of scissors and sewing during pregnancy. A previous study of antenatal taboos in Hong Kong revealed that hammering nails, drilling walls, using a needle or scissors in bed, and using broken cups or bowls were thought to cause cleft (Lee et al., 2009). This shows that the Chinese community in Malaysia shares similar beliefs with their Hong Kong counterparts. The belief among the 7 Indian respondents that cleft is a result of a lunar eclipse during pregnancy has also been observed in a Mexican study (Castro, 1995). Similarly, a South African study noted that if a pregnant woman handled a sharp object such as a knife, scissors, or needle during the time of an eclipse, this action could affect her unborn child (Ross, 2007). Based on Hindu beliefs, an eclipse is a “bad time” because during an eclipse “two planets pass each other similar to when two cars pass each other, a lot of dust and pollution is created. The planets have the same effect. This pollution could affect an unborn baby if the mother does not take the necessary precautions” (Ross, 2007).
In spite of all the different beliefs across different racial and ethnic groups, many respondents reported that their cultural beliefs and background did not prevent them from seeking cleft treatment for their child. This is rather reassuring, as it shows that these cultural beliefs do not hinder compliance to surgeries, interventions, and appointments in cleft care. Some of our respondents reported that they encounter challenges when seeking or receiving cleft treatment for their child. Such challenges include financial constraints and transportation issues, and long waiting times for surgery. The challenges faced mainly arise because cleft management is a lifelong integrated process involving frequent visits to clinic sessions with multiple health-care professionals.
Participants who reported difficulties in cleft care were more likely to have lower household incomes and lower education levels. Lower income has been related to a family’s overall financial state, leading to high out-of-pocket expenses and lost time from work due to long-term interdisciplinary follow-ups for patients with cleft (Cassell et al., 2012). Our respondents experienced a similar situation, as they needed to bring their children with cleft for frequent follow-up visits. In certain centers, different specialties involved in cleft care are not allocated at the same center, entailing more time off work and greater expenditure for parents and caregivers.
Parents’ education level may also affect the effective treatment of children with cleft (Noor & Musa, 2007). People with lower health literacy have poorer understanding of health-related information and have been linked with higher hospitalization, overall poorer health conditions, and higher mortality (Berkman et al., 2011). This is particularly true of first-time parents with a child with cleft. Issues regarding feeding, speech impairment, infection, and multiple surgical interventions may be difficult to comprehend. Therefore, rapport and consistent effective communication with these parents is essential. This should continue well into adulthood as the child grows, and other teams in cleft care should participate actively.
Cleft management involves a myriad of medical and nonmedical specialties. Other specialties involved in cleft care should be synchronized with the delivery of effective presurgical counseling. An effort commonly practiced among cleft centers worldwide is organizing combined cleft clinic sessions where patients with cleft and their parents/caregivers attend clinic sessions in the presence of cleft surgeons, dentists, speech therapists, and even counselors. This has been proven to be helpful. However, shortages of personnel from individual specialties remain a problem in our setting. There is much room for improvement in not only increasing the number of trained medical personnel in managing patients with cleft but also improving the delivery of cleft services and overcoming its barriers.
From this study, we acknowledge some limitations encountered. The racial distribution of the respondents may not accurately reflect the demographics of patients with cleft in the country, even though the cohort of respondents was selected from distinct regions of the country. Perhaps future studies can recruit participants from more centers in other regions of the country to eliminate this drawback. The research tool of a study questionnaire to collect data would ideally be augmented by inclusion of standardized and normed measures. In addition, in recruiting primarily from cleft care centers, we did not gather information from those who are not actively receiving cleft treatment nor did we target cultural beliefs about the cause of cleft among the general population of Malaysia. We also acknowledge that by recruiting participants in clinical setting, the sample size is somewhat skewed toward those seeking treatment and follow up and that small numbers in certain ethnic groups precluded further analysis. Despite these limitations, this descriptive analysis provides useful information about cleft care in the country.
Conclusion
A total of 295 respondents from the Malay, Chinese, Indian, and indigenous Sabah and Sarawak people participated in our study. We found that cleft management in Malaysia involves a range of beliefs, with difficulties in cleft care identified among families from lower socioeconomic backgrounds. There is much improvement needed in the future to optimize cleft services in Malaysia.
Footnotes
Acknowledgments
Authors’ Note
This manuscript was presented orally at the 74th Congress of the Korean Society of Plastic & Reconstructive Surgeons and the 19th Scientific Meeting of the Korean Cleft Palate-Craniofacial Association 2016; Seoul, South Korea; November 2016.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.