
Abstract
Objective:
To evaluate the long-term stability of LeFort I osteotomy followed by distraction osteogenesis with a transcutaneous rigid external device for the treatment of severe maxillary hypoplasia in patients with cleft lip and palate.
Patients and Methods:
Nine patients with cleft lip and palate underwent rigid external distraction after a LeFort I osteotomy for maxillary advancement. Lateral cephalometric films were analyzed for assessment of treatment outcome and stability in 1 month, 6 months, and 1 year after distraction.
Results:
Significant maxillary advancement was observed in the horizontal direction, with the anterior nasal spine (ANS) distance of the maxilla increasing by an average of 20.5 ± 5.1 mm after distraction. The ANS relapse rates in 6 months and 1 year were 8.7% and 12.8%, respectively. The mean inclination of upper incisors to the palatal plane was almost unchanged (before: 109.8° ± 6.6°; after: 108.9° ± 7.5°). The movement ratios at the nasal tip/ANS, soft tissue A point/A point, and the upper vermilion border/upper incisor edge were 0.36:1, 0.72:1, and 0.83:1, respectively.
Conclusion:
Considerable maxillary advancement was achieved with less change of incisors inclination after distraction. Moreover, the relapse rate after 1 year was minimal. The concave facial profile was improved as well as the facial balance and aesthetics.
Keywords
Introduction
Distraction osteogenesis (DO) was first applied by Codivilla in 1905 to lengthen the short femurs with the technique of gradual distraction (Codivilla, 1905). Since then, this technique has been widely utilized to treat uneven extremities. The first application on craniofacial treatment was in 1992 when McCarthy successfully lengthened the mandible by 18 to 24 mm in 4 children with Pierre Robin sequences (McCarthy et al., 1992). Nowadays, this treatment modality is also applied to treat patients having cleft lip and palate with severe maxillary hypoplasia maxilla, which can only be managed by orthognathic surgery, even after primary surgery by experienced cleft surgeons. In 1997, Polley and Figueroa first applied the DO with a rigid external distraction (RED) device to treat patients with cleft lip and palate (Polley & Figueroa, 1997). The combination of the RED device with an intraoral skeletal anchorage was demonstrated by Hierl and Hemprich in 1999 (Hierl & Hemprich, 1999). They carried out a midface DO by utilizing intraoral miniplates and micromesh in treating an edentulous adult patient with cleft lip and palate. Bone-borne RED is an effective alternative method that can be applied at different levels of skeletal fragmentation in various osteotomies including LeFort I, II, and III (Monaghan et al., 2002). In contrast to orthognathic surgery, the greatest advantage of DO is the ability to improve the growth of bony defects along with the simultaneous possibility of expansion of soft tissues (Rachmiel et al., 1998). In the study by Loboa et al. (2004), the neoformation of mesenchymal tissues was triggered by the distraction device in a regular rhythm, which caused little trauma to the tissues and activated new bone formation.
Swennen et al. (2001) reviewed 16 studies that discussed maxillary distraction with tooth-borne anchorage in 121 patients. The results revealed maxillary advancement of 1 to 17 mm, and although a relapse was noted in 65 patients, there was no clear data regarding the degree/rate of relapse. In contrast, the bone-borne group demonstrated an average of 11 mm advancement at the A point with good stabilities in nongrowing patients. Further improvement for better adaptation of the skeletal anchorage was subsequently introduced, including a combination of RED with transcutaneous skeletal anchorage to reduce the patients’ discomfort as well as to gain better control of distraction.
To reduce tooth complications from tooth-borne RED, we used a direct bony attachment for the advancement of the maxilla. This study aimed to evaluate the long-term stability of LeFort I osteotomy followed by DO with skeletal anchorage via transcutaneous RED device for treating patients having cleft lip and palate with severe maxillary hypoplasia.
Materials and Methods
Patients
In this study, all the 9 patients with cleft lip and palate received primary lip/palate repair and alveolar bone graft in Kaohsiung Chung Gung Memorial Hospital. However, they developed a severe class III skeletal pattern with significant midface hypoplasia that required DO. All patients (4 boys, 5 girls; average age: 11.6 ± 0.4 years old; range: 11.2-12.5 years old) underwent LeFort I osteotomy and RED device installation by the same surgeon (Table 1 and Figure 1). Distraction (at a rate of 1 mm/d) was started after a latency period of 7 days after surgery. The DO process lasted for around 1 month and was terminated when the desired skeletal relationship was achieved. The RED devices were removed after an 8-week consolidation period.
Patient Characteristics.
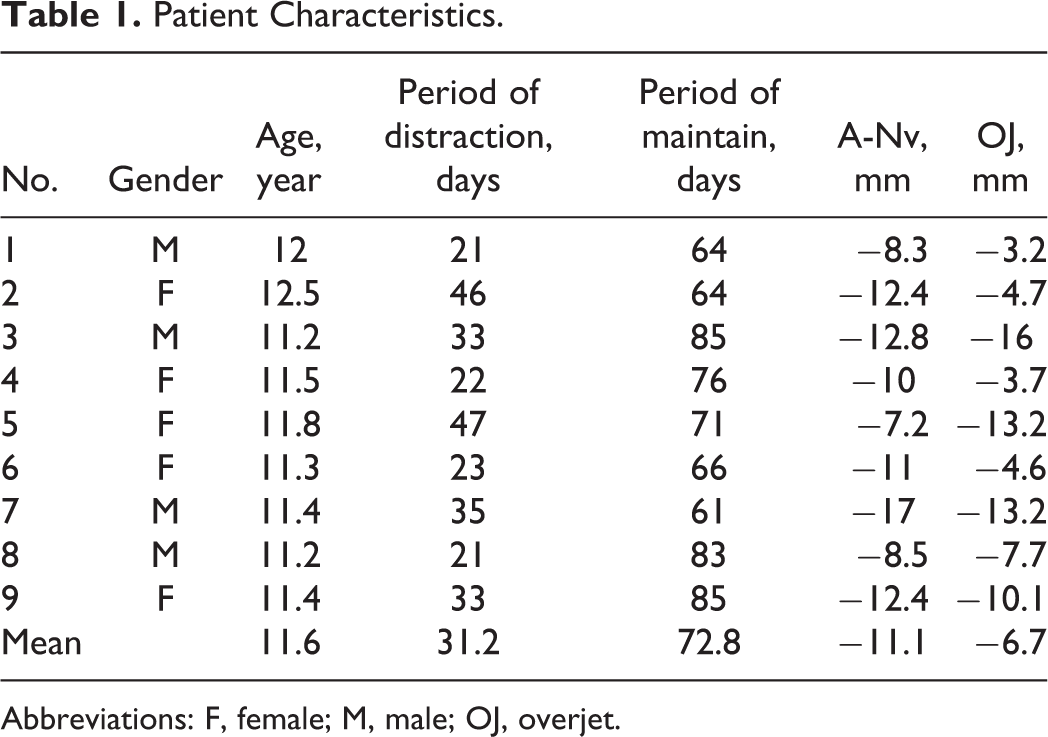
Abbreviations: F, female; M, male; OJ, overjet.
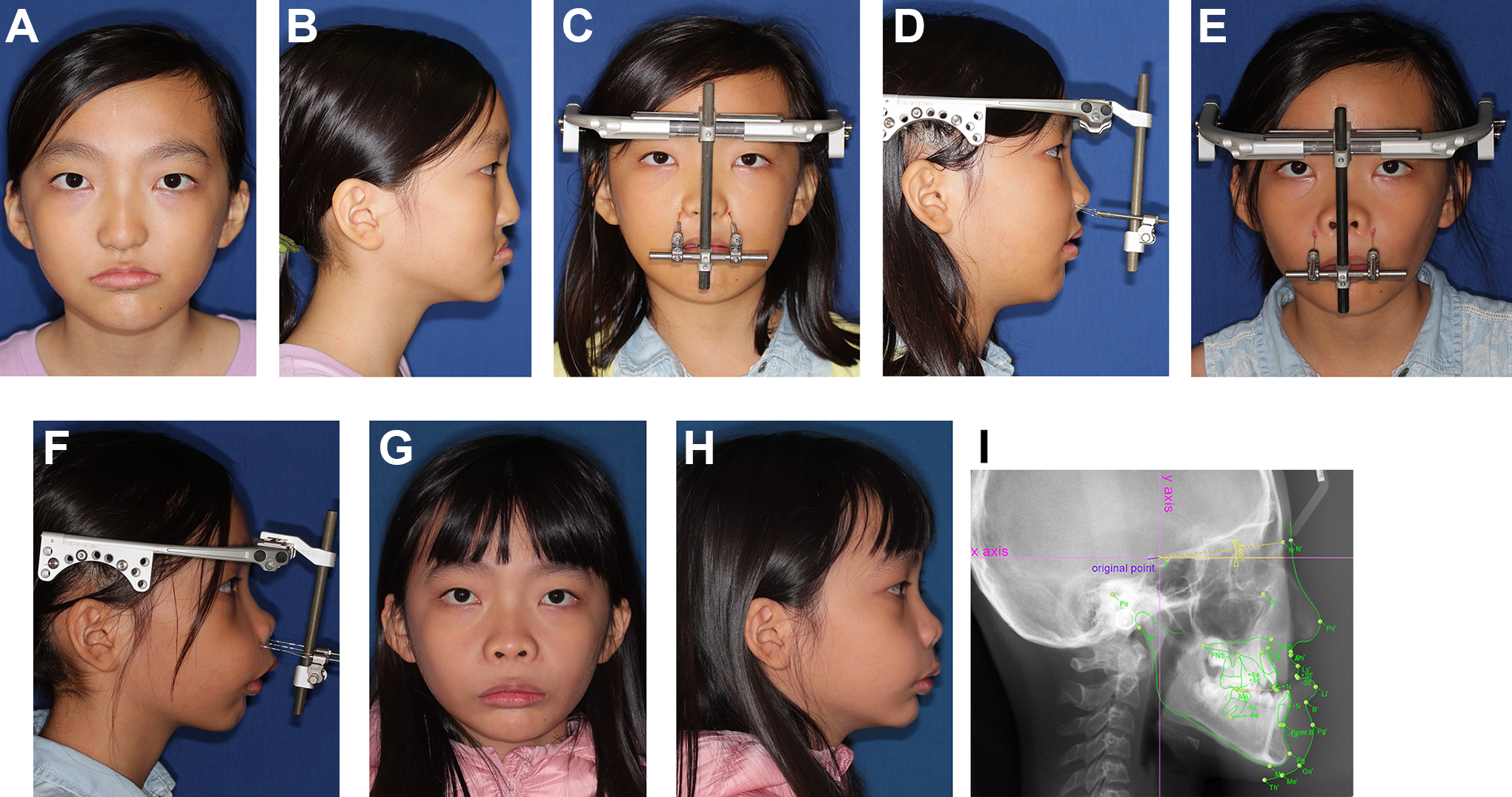
Eleven-year-old girl (case no. 4) with complete bilateral left cleft lip and palate and maxillary deficient facial profile was treated with maxillary lefort I osteotomy and distraction osteogenesis to improve facial profile (A and B) before surgery; (C and D) during distraction; (E and F) immediately after distraction; (G and H) after 1-year review; and (I) cephalometric landmarks and reference lines selected in this study. (The definitions of landmarks are listed in Appendix A).
Lateral cephalometric films were collected 1 week before (T0), immediately 1-month after the termination of DO (T1), 6-month after (T2), and 1-year after (T3) distraction. Selected skeletal, dental, and soft tissue landmarks are listed in Appendix A. The definitions of all the landmarks and reference lines (Appendix A; Figure 1) followed those by Lin et al. (2012). The AudaxCeph Empower VER5.2 was used to analyze changes among the above 4 stages. First, we set up an x-y coordinate system on the preoperative cephalogram by fabricating a line 7° below the sella-nasion (S-N) plane as the x-axis, and we used the sella point as the original point. Then we drew a line perpendicular to the x-axis by intersecting the line at the sella for the y-axis. We superimposed the cephalometric films to record the changes between each phases. Changes were assessed by applying linear and angular parameters of skeletal and dental structures. Measurements were taken by 1 examiner (Wei-Ling Gao).
Error Study
A cephalometric tracing and all measurement assessment were taken by 1 researcher. Reproducibility of the reference lines was verified by comparing the angle between the S-N plane and 7° below the S-N plane in all the cephalograms in 2 occasions with a 1-month interval. There was no statistical difference in defining the reference lines among the cephalometric tracing.
The method of evaluating the systematic and random errors in the tracing process followed the study by Houston (1983), and the tested null hypothesis showed that there was no difference between the first and the second measurements.
Results
The average period of distraction was 31.2 ± 10.3 days, and the average maintenance period was 72.8 ± 9.7 days. The mean predistraction overjet was −6.7 ± 4.8 mm, with a range of −13.2 to −3.2 mm. At the end of the distraction, the mean overjet was 4.6 ± 2.6 mm, with a range of 2.1 to 8.4 mm, which increased by an average of 13.5 ± 4.9 mm (Table 1). All skeletal and dental angular/linear changes between T1 and T0 are shown in Table 2.
Cephalometric Measurement of Distraction (T1–T0) Changes.
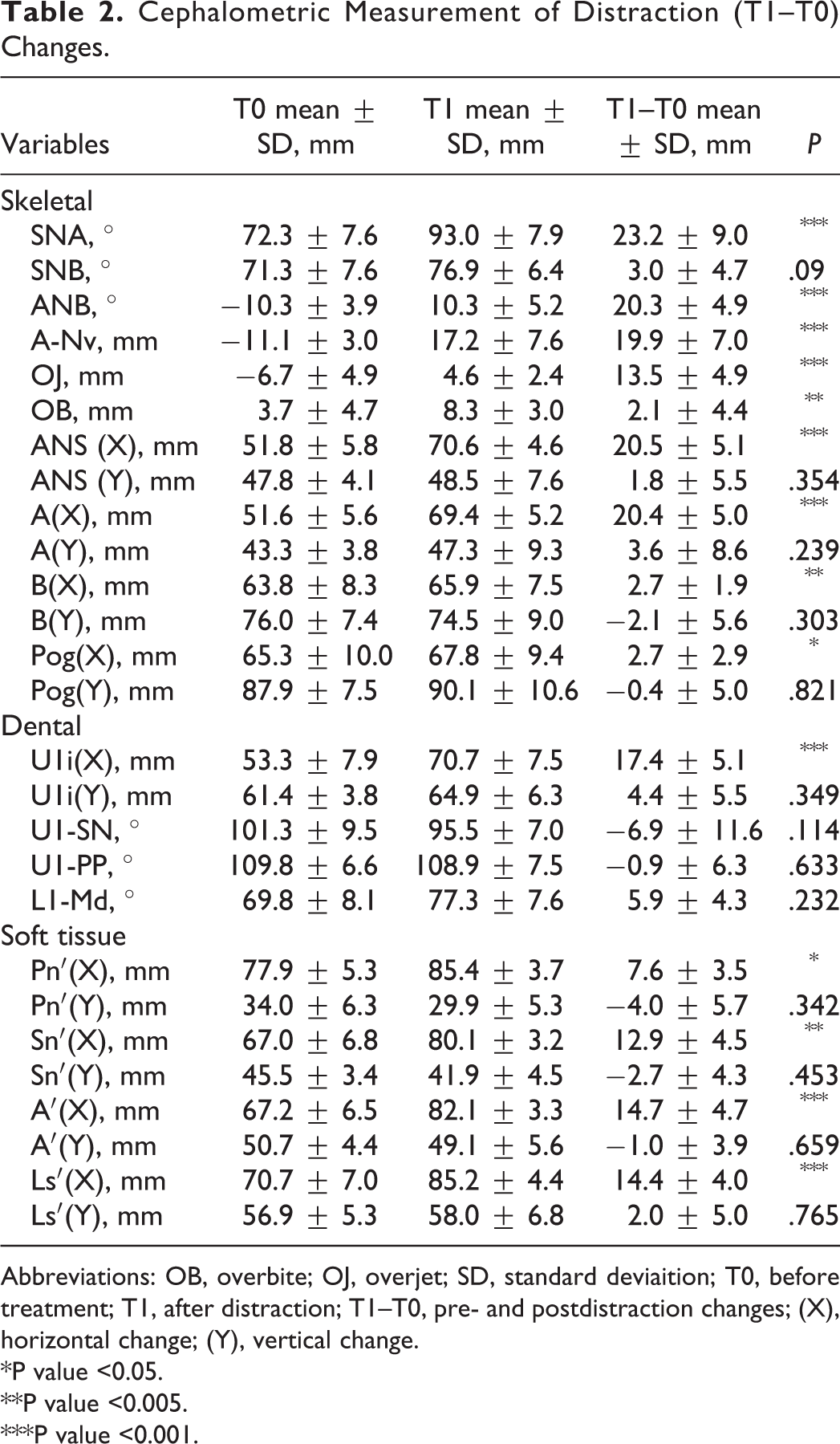
Abbreviations: OB, overbite; OJ, overjet; SD, standard deviaition; T0, before treatment; T1, after distraction; T1–T0, pre- and postdistraction changes; (X), horizontal change; (Y), vertical change.
*P value <0.05.
**P value <0.005.
***P value <0.001.
Skeletal Change (T1–T0)
The initial skeletal discrepancy (A-Nv) of the maxilla in the horizontal direction was −11.1 ± 3.0 mm, with a range of −7.2 to −17.0 mm. The mean increase was 19.9 ± 7.0 mm at the end of the distraction. The maxilla showed significant advancement in the horizontal direction and moved inferiorly. The position changes of landmark in ANS and A point were significant: ANS (horizontal: 20.5 ± 5.1 mm; vertical: 1.8 ± 5.5 mm) and A point (horizontal: 20.4 ± 5.0 mm; vertical: 3.6 ± 8.6 mm).
The mandible showed mild advancement in the horizontal direction, although the vertical position varied from case to case. The average records of position changes of mandible were: B point (horizontal: 2.7 ± 1.9 mm in absolute value; vertical: 2.1 ± 5.6 mm in absolute value) and Pog (horizontal: 2.7 ± 2.9 mm in absolute value; vertical: 0.4 ± 5.0 mm in absolute value). The distraction moved the maxilla forward, and the direction of distraction induced a clockwise rotation of the mandible (in the downward and backward directions).
Dental Change (T1–T0)
The upper incisor edge showed great anterior advancement (horizontal: 17.4 ± 5.1 mm; vertical: 4.4 ± 5.5 mm). Meanwhile, the upper molar showed similar anterior movement as that of the incisors (horizontal: 13.6 ± 7.5 mm; vertical: 3.5 ± 4.1 mm), indicating a minimal side effect over the dental anchorage. Furthermore, the inclination of the upper incisors to the palatal plane showed little change after distraction (T0: 109.8° ± 6.6°; T1: 108.9° ± 7.5°), which indicates minimal dental side effect over the frontal dentition.
Relapse Rate
After 6 months, ANS showed a horizontal relapse by 1.8 ± 2.4 mm and an inferior change by 0.4 ± 3.2 mm on average. The relapse rate was 8.7% in the horizontal direction and an increase of 24.1% in the vertical direction. A point showed a backward change by 2.3 ± 2.0 mm on average and a superior change by 1.3 ± 3.7 mm. The relapse rate was 11.2% in the horizontal direction and 35.5% in the vertical direction. After 12 months, ANS showed a horizontal relapse by 2.6 ± 2.3 mm and a superior change by 2.2 ± 5.6 mm on average. The relapse rate was 12.8% in the horizontal direction and an increase of 22.2% in the vertical direction. A point showed a backward change by 2.1 ± 3.0 mm on average and a superior change by 0.9 ± 4.1 mm. The relapse rate was 10.1% in the horizontal direction and 23.9% in the vertical direction (Table 3).
Cephalometric Measurement of Treatment Stability.
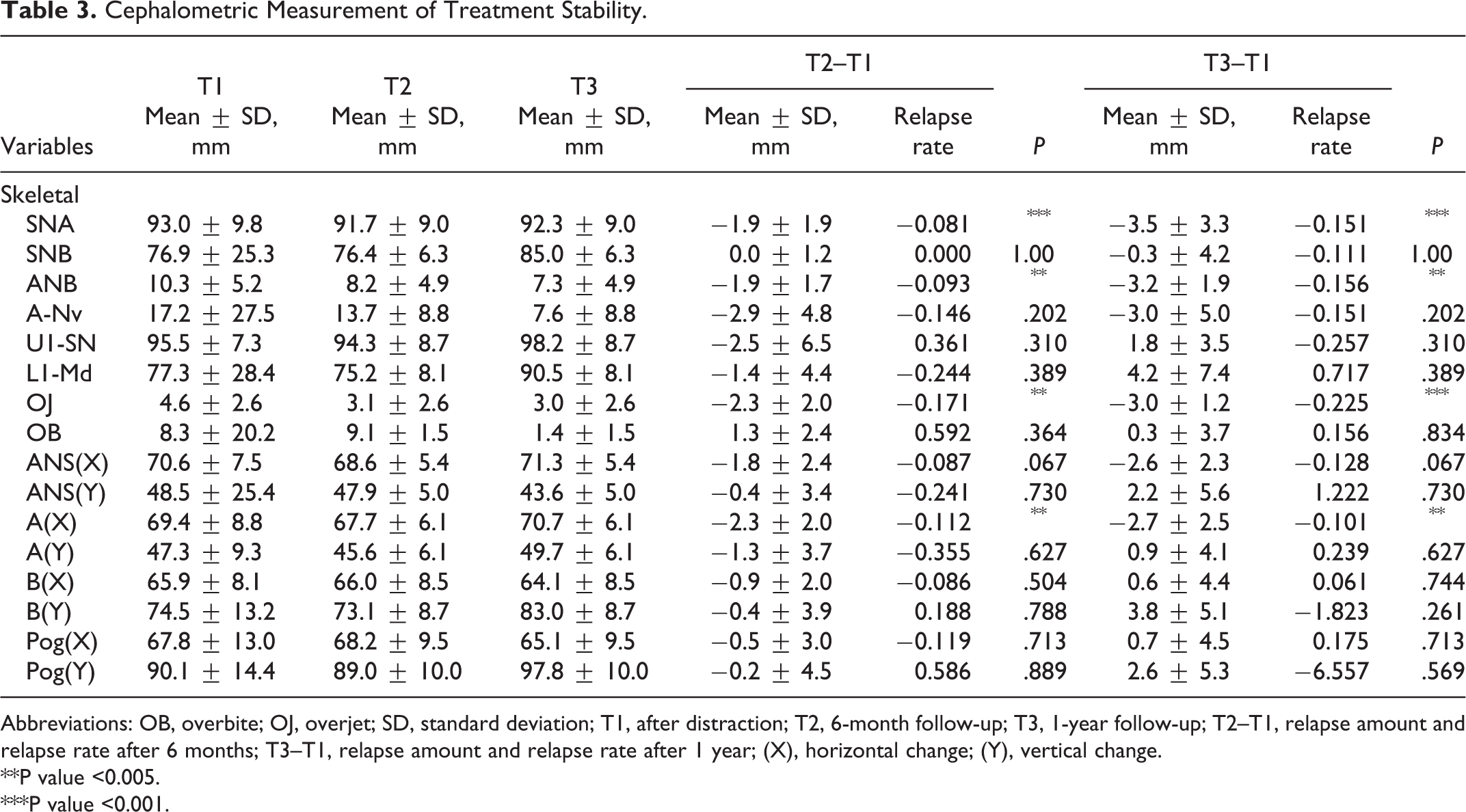
Abbreviations: OB, overbite; OJ, overjet; SD, standard deviation; T1, after distraction; T2, 6-month follow-up; T3, 1-year follow-up; T2–T1, relapse amount and relapse rate after 6 months; T3–T1, relapse amount and relapse rate after 1 year; (X), horizontal change; (Y), vertical change.
**P value <0.005.
***P value <0.001.
Correlation Between Soft Tissue and Hard Tissue
In the maxilla, the correlation coefficient ranged from 0.22 to 0.46 on the horizontal plane and 0.12 to 0.34 on the vertical plane. The forward movements of the soft and hard tissues were correlated, but there was no significant correlation (0.12 ≤ r ≤ 0.46). The ratio for the horizontal movement at the level of the nasal tip/ANS, the soft A point/A point, and the upper vermilion border/upper incisor edge was 0.36:1, 0.72:1, and 0.83:1, respectively (Table 4).
Soft Tissue-to-Hard Tissue Ratio After Distraction and Correlation Between Soft Tissue and Hard Tissue Movement.
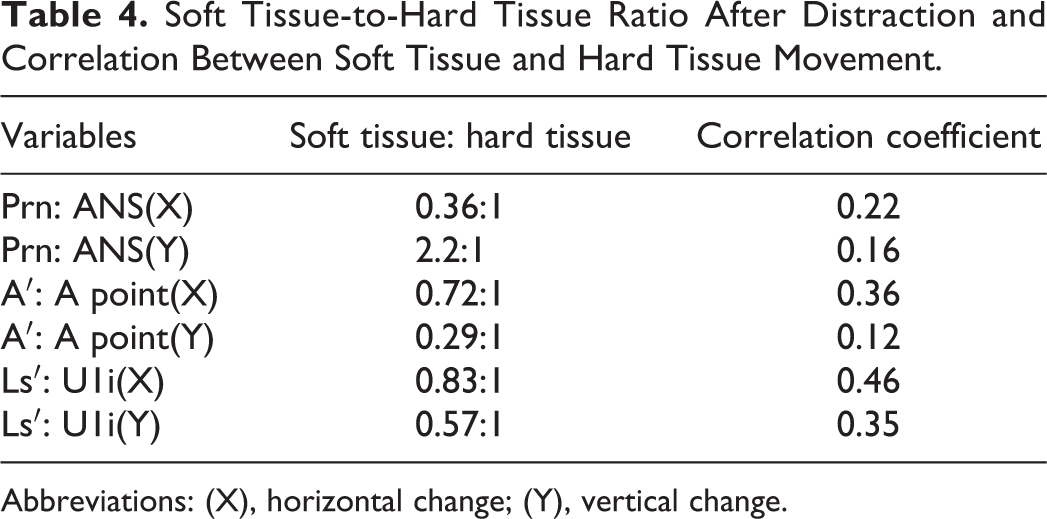
Abbreviations: (X), horizontal change; (Y), vertical change.
Discussion
Distraction osteogenesis is a surgical procedure that is easy to control. It can activate a regeneration process and start a mechanical enhancement of biological responses to the injured tissues and, consequently, lead to new bone formation. Distraction osteogenesis contains 3 phases: latency, distraction, and consolidation (Ai-Aql et al., 2008). The initial trauma brought by surgery requires a latency phase so that the initiation of primary healing can occur. This period generally lasts for 3 to 5 days. If the latency period is longer than 10 to 14 days, a premature bone union tends to make DO difficult. During the distraction phase, tensile forces are applied to the callus base in a rhythm and at a particular rate. When the callus is stretched, a central fibrous zone called the “fibrous interzone” forms, which is a zone full of chondrocyte-like cells, fibroblasts, and oval cells (the intermediate cells between fibroblasts and chondrocytes in morphology; Vauhkonen et al., 1990; Aronson, 1994; Sato et al., 1998; Sultan, 2016). In the distraction phase, the process of distraction activates the transportation of bone fragments, and the formation of a new, immature, woven, and parallel-fibered bone commences. The duration of the distraction phase depends on the degree and severity of the skeletal deformity. However, the rhythm and rate of distraction are more critical compared with the duration. A distraction rate of 1 mm/d is a common standard used in most studies; hence, we used the same criterion in all our patients and obtained good results. The best rhythm for DO is a continuous steady-state separation of the bone fragments (Sultan, 2016). After the distraction bone length is acceptable, the activation of distraction will be terminated. Subsequently, the consolidation phase begins, wherein the bone and extensive amounts of osteoid undergo mineralization and eventual remodeling.
Consolidation is a period after the end of the distraction when the mobile fragments are stabilized in the preplanned position. The distractor is kept to be passive, and it combines with the whole rigid fixation device to act as a “retainer.” This period varies from 8 to 12 weeks to allow mineralization of callus to occur across osseous gap. The consolidation phase is essential in bone healing and should be long enough to ensure the sufficient reunification of the bony fragments. It is logical that the longer phase of consolidation may guarantee the less relapse potential of bony fragments. However, a longer consolidation phase may also lead to some complications, such as mucosal dehiscence, infection, fracture, pin-track ulcers and associated discomfort, and displacement of the transported segment (Natu et al., 2014). To balance the outcome stability and potential complications during the consolidation phase, all of our cases had an 8-week consolidation period. It is also indicated in our study that the amount of bony relapse should be taken into account and applied for overcorrection during distraction period to achieve the desired result. The further relapsed condition of longer follow-up should be investigated in the future.
The first historical use of RED in the skeletal anchorage was performed in an adult female having cleft lip and palate with a 20 mm horizontal advancement and a 13 mm movement inferiorly (Hierl & Hemprich, 1999). However, no long-term follow-up was conducted. The average sagittal advancements in our study were 20.5 mm in ANS and 20.4 mm in A point. Our results were similar to those of previous studies but revealed greater distraction range than those reported in previous studies either with dental anchorage or with skeletal anchorage. Cheung and Chua reviewed 26 papers regarding maxillary distraction in 276 patients with cleft in 2006. Most of the results on maxillary horizontal advancement were only in the range of 5 to 9 mm (Cheung & Chua, 2006).
The direction of the distracted maxilla in our study was managed to gain a backward rotation of the mandible so that their concave class III profile could be simultaneously improved. Our goal for the RED treatment was not only to obtain significant improvement of the maxillary deficiency, which is the main problem in most patients with cleft lip and cleft palate (CLCP), but also by controlling the direction of distraction to achieve the effect of a clockwise rotation of the mandible. The common treatments in patients with skeletal class III malocclusion include growth modification, dentoalveolar compensation (camouflage), and orthognathic surgery (Rabie et al., 2008). The concept of RED includes orthognathic surgery and growth modification. Applying DO in preadolescence children with CLCP may reduce the future need to undergo further surgical procedures. In our study, we will closely review the enrolled patients regarding their growth and the demand for orthognathic surgery.
Aksu et al. (2010) used a dental anchorage for tooth-borne maxillary distraction in adult patients with cleft lip and palate. After the distraction, there was a significant sagittal movement of the upper incisors, revealing a 4.5 mm labial advancement. This result shows that the traction force may cause undesirable labial tipping of the anterior teeth. The inclination of the incisors to the palatal plane in our study showed little or no change immediately after distraction. Hence, skeletal anchorage can help to avoid dentition side effects.
Our study showed that after 6 months, the ANS showed a relapse in the horizontal direction of 1.8 ± 2.4 mm, and this increased to 2.6 ± 2.3 mm after 1 year on average. For the A point, the 6-month relapse was 2.3 ± 2.0 mm, and this increased to 2.7 ± 2.5 mm after 2 years. The 1-year relapse rates in the horizontal direction were 8.7% and 11.2% in ANS and A point, respectively. The 1-year relapse rates were 12.8% and 13.3% in ANS and A point, respectively. These results are similar to those reported by Harada et al. (2001; 12% relapse rate after 6 months; use of skeletal anchorage). The vertical movements by distraction in this study were 1.8 mm in ANS and 3.6 mm in A point (both inferiorly), indicating that the maxilla was moved in a counterclockwise direction. The result showed the greater stability in our study compared to the study by Painatt et al. (2017), which revealed a 38% skeletal relapse in the adults of their study. The patients in our study were all growing children (11.2-12.5 years old) with a better blood supply compared to adults, and an improved ability of tissue repair may be the reason for better postdistraction stability. Hence, we suggest that patients with CLCP should undergo DO in the preadolescent period if possible.
The upper lip advanced significantly with DO, and the soft-to-hard tissue ratio was 0.36:1 in the nasal tip to ANS and 0.73:1 in soft tissue A point to skeletal A point on average. These ratios were considerably lower than those reported in previous studies. Most of these studies have reported that patients with LeFort I advancement showed ratios of soft-to-hard tissue changes between 0.17 and 0.36:1 for nasal tip change to maxillary forward movement and 0.29 to 0.62:1 for the upper lip to upper incisor movement. The results varied due to multiple factors, such as age, patient variation (with clefts or not, unilateral or bilateral), surgical methods, and treatment intervention.
Our results were lower than those reported by Wen-Ching Ko et al. (2000), which revealed ratios of the nasal tip to ANS to be 0.53:1, 0.96:1 for soft A point to skeletal A point, and 0.8:1 for the upper vermilion border/upper incisor level. The results may be stratified by age. The mean age in our study was 11.6 ± 0.4 years, which was younger than that recorded in the previous study (5.2-25.7 years in the study by Ko et al.). In the study by Ko et al., the results varied for different ages; they speculated that younger patients showed poor correlation between hard and soft tissues. This may result from the less developed soft tissues, with more fat and fewer muscles in children. Moreover, a different soft tissue response in the result may be attributed to the presence of scars and the difference in type and severity of the cleft lip and palate. In our study, the sagittal movement ratio of nasal tip/ANS had a negative correlation. This result was different from that of Ko et al., which revealed a 0.495 correlation coefficient. The skin tension increased after distraction. The more the extent of distraction, the less the expression of the advancement of the nasal tip due to the progressive increasing scarred soft tissue tension.
In the study by Suhr and Kreusch (2004), common challenges in using DO included the choice of different devices, the determination of the vector of distraction, the osteotomy site and area, and the patient’s cooperation. Some studies showed that the probability of complications was 22.8% (Douglas, 2000). In our study, although the direction of distraction was not proper at the initial stage and showed inappropriate skeletal changes in the vertical and horizontal directions in some cases, it was not difficult to control and adjust the desirable direction of distraction because the device is uncomplicated in changing the direction of the tracing wire. However, this can cause scars in the wire exit. In the study by Yu and Woo (2016), although they tried to reduce the size and visibility of the pin site scars in the alar crease, the scars were still prominent and became more distinguished if infection occurred. In our study, the scar is not prominent because of the good resilience in young children. Even if patients care about the dark deposit, laser resurfacing surgery can be applied since it is not an uncommon or complicated treatment.
The use of a transcutaneous device is not rare for distraction in mandibular advancement. Infection is one of the most common complications during distraction. Indeed, one of our patients was infected during the consolidation phase. But after proper medication therapy, the procedure of distraction went well and showed good results. The biggest benefit of a transcutaneous device was the reduction of discomfort for the patient, especially on the lips. In addition, the direction of distraction was easy to operate and maintain than traditional distraction through the mucosa. The previous study (Balaji & Balaji, 2018) did not demonstrate any significant difference between internal and external distraction devices in either the horizontal or vertical amount of distraction in maxilla. However, we found that transcutaneous external distraction device allowed clinicians to better control the directions of distraction in maxilla 3-dimensionally (yaw, roll, and pitch; Pelo et al., 2007). Patients could also easily activate the device according to instruction. Our patients also reported little influence in their chewing function or daily activity during the consolidation phase since they did not wear any tooth-borne or bone-borne devices inside their mouth. External distraction device did tend to increase certain social and physical hardship, which may not be observed in those internal distraction device patients (Yorikatsu et al., 2019). Therefore, our patients were surgically treated during summer vocation so that their physical and psychosocial distress could be minimized. Moreover, the daily intraoral activation of internal distraction device could be more difficult for patients to handle. Another advantage of our transcutaneous external distraction device is much easier for clinicians to monitor the distraction process of distraction during both activation and consolidation phases. Any defects of the external distraction device can be immediately detected.
The imaging tool applied in this study was lateral cephalometric analysis, which revealed the changes of treatment in sagittal and vertical planes. Investigation of potential error during landmarks identification and parameter measurement was carried out according to Houston’s method (Houston, 1983). The result of our error study indicated both the systemic and random errors did not cause any impact to our result. However, this 2-dimensional (2D) imaging tool is limited in explanation of 3-dimensional (3D) changes of surgical result, especially in those patients requiring asymmetrical correction. The patient enrolled in our study did not present any significant asymmetry in their original dentoskeletal discrepancy. Therefore, there was no asymmetric bony positioning applied during the active distraction. Nevertheless, 3D landmarks other than those located in the median plane of the anterior bony contour and soft tissue profile cannot be assessed in 2D cephalometric imaging. The other issues such as 3D airway changes, soft tissue envelope expansion, or growth assessment of craniofacial structures associated with DO can be much more reliable to apply 3D imaging (Durão et al., 2013). Computed tomography or cone-beam computed tomography scan has been utilized in simulation/navigation protocol for orthognathic planning (Chang et al., 2020). This protocol has not been applied in growing patients requiring DO. There are 2 reasons: high radiation exposure and potential image noise caused by radiation scattering due to the metal components of DO device. Both issues require setting up a new relevant protocol in the future, such as application of nonmetallic materials or redesign the fitting position of the retractor. Hence, we believe that our results are of importance in reflecting distraction and postdistraction effects.
Another limitation of our study, however, is the small sample size, which is similar to the previous studies. Patients with CLCP are not common in Taiwan. From 1994 to 2013, the annual incidence rate of CLCP was 1.48 ‰ in Taiwan (Chang et al., 2016). Nevertheless, irrespective of the amount of distraction and the relapse rate, similar results were obtained in all of our patients, indicating the reliability of the method of distraction used.
Conclusions
In this study, distraction using RED devices with skeletal anchorage in children with cleft lip and palate revealed significant maxilla advancement and showed a reasonable relapse rate after 1 year. Further, we recommend that patients with CLCP with severe skeletal discrepancies should undergo distraction using RED devices in the preadolescent period.
Footnotes
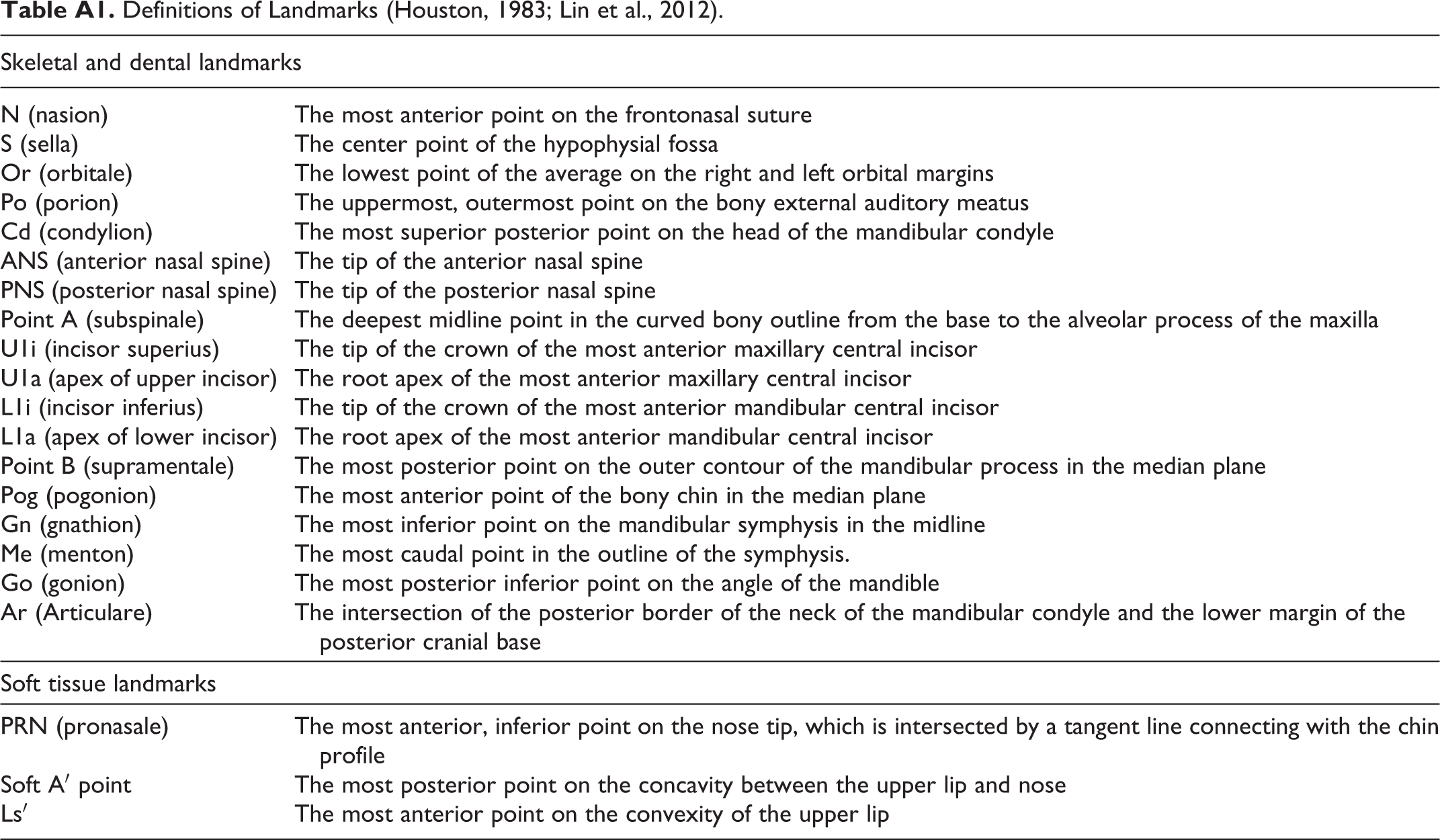
Appendix A
Definitions of Landmarks (Houston, 1983; Lin et al., 2012).
| Skeletal and dental landmarks | |
|---|---|
| N (nasion) | The most anterior point on the frontonasal suture |
| S (sella) | The center point of the hypophysial fossa |
| Or (orbitale) | The lowest point of the average on the right and left orbital margins |
| Po (porion) | The uppermost, outermost point on the bony external auditory meatus |
| Cd (condylion) | The most superior posterior point on the head of the mandibular condyle |
| ANS (anterior nasal spine) | The tip of the anterior nasal spine |
| PNS (posterior nasal spine) | The tip of the posterior nasal spine |
| Point A (subspinale) | The deepest midline point in the curved bony outline from the base to the alveolar process of the maxilla |
| U1i (incisor superius) | The tip of the crown of the most anterior maxillary central incisor |
| U1a (apex of upper incisor) | The root apex of the most anterior maxillary central incisor |
| L1i (incisor inferius) | The tip of the crown of the most anterior mandibular central incisor |
| L1a (apex of lower incisor) | The root apex of the most anterior mandibular central incisor |
| Point B (supramentale) | The most posterior point on the outer contour of the mandibular process in the median plane |
| Pog (pogonion) | The most anterior point of the bony chin in the median plane |
| Gn (gnathion) | The most inferior point on the mandibular symphysis in the midline |
| Me (menton) | The most caudal point in the outline of the symphysis. |
| Go (gonion) | The most posterior inferior point on the angle of the mandible |
| Ar (Articulare) | The intersection of the posterior border of the neck of the mandibular condyle and the lower margin of the posterior cranial base |
| Soft tissue landmarks | |
| PRN (pronasale) | The most anterior, inferior point on the nose tip, which is intersected by a tangent line connecting with the chin profile |
| Soft A′ point | The most posterior point on the concavity between the upper lip and nose |
| Ls′ | The most anterior point on the convexity of the upper lip |
Authors’ Note
The data sets supporting the conclusions of this article are included within the article. Written informed consent was obtained from all the patients before enrollment in the study. This study has been carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) and has been approved by the Institutional Review Board of the Chang Gung Medical Foundation (IRB No: 202000531B0).
Acknowledgments
We would like to thank the Biostatistics Center, Kaohsiung Chang Gung Memorial Hospital, for their assistance with all statistical analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.